
The Prevalence and Risk Factors Associated with Iodine Deficiency in Canadian Adults

 , , ,
, , ,
Abstract
:1. Introduction
2. Experimental
2.1. Study Design, Participant Eligibility, and 24 h Urine Sampling
2.2. PURE Participants and Self-Reported Dietary Intake
2.3. Iodide, Thiocyanate, Nitrate and Sodium Determination in 24 h Urine Samples
2.4. Statistical Analysis
3. Results
3.1. PURE Cohort Characteristics and CE Method Performance
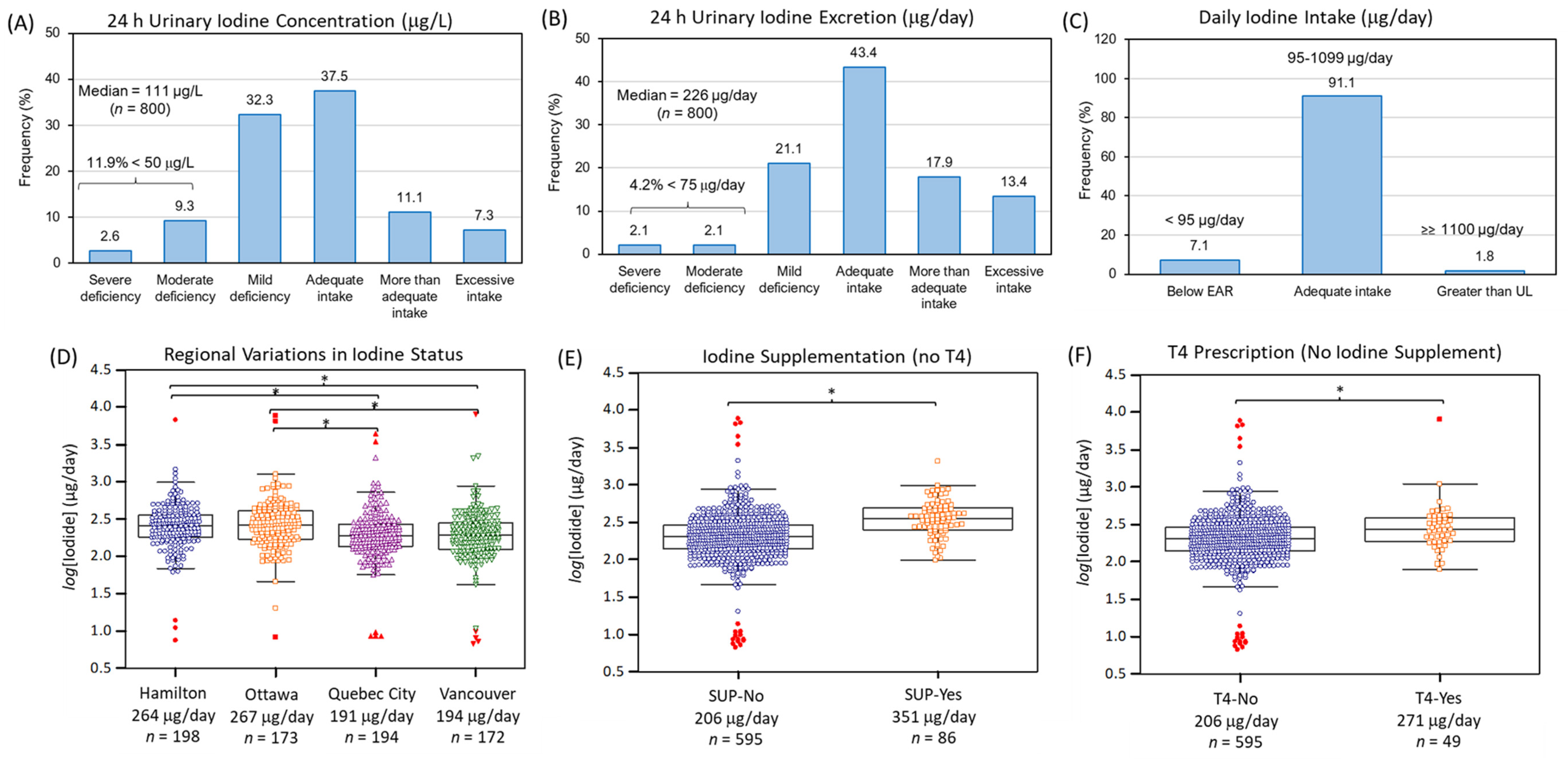
3.2. Iodine Nutritional Status of Canadian Adults from PURE-24USE
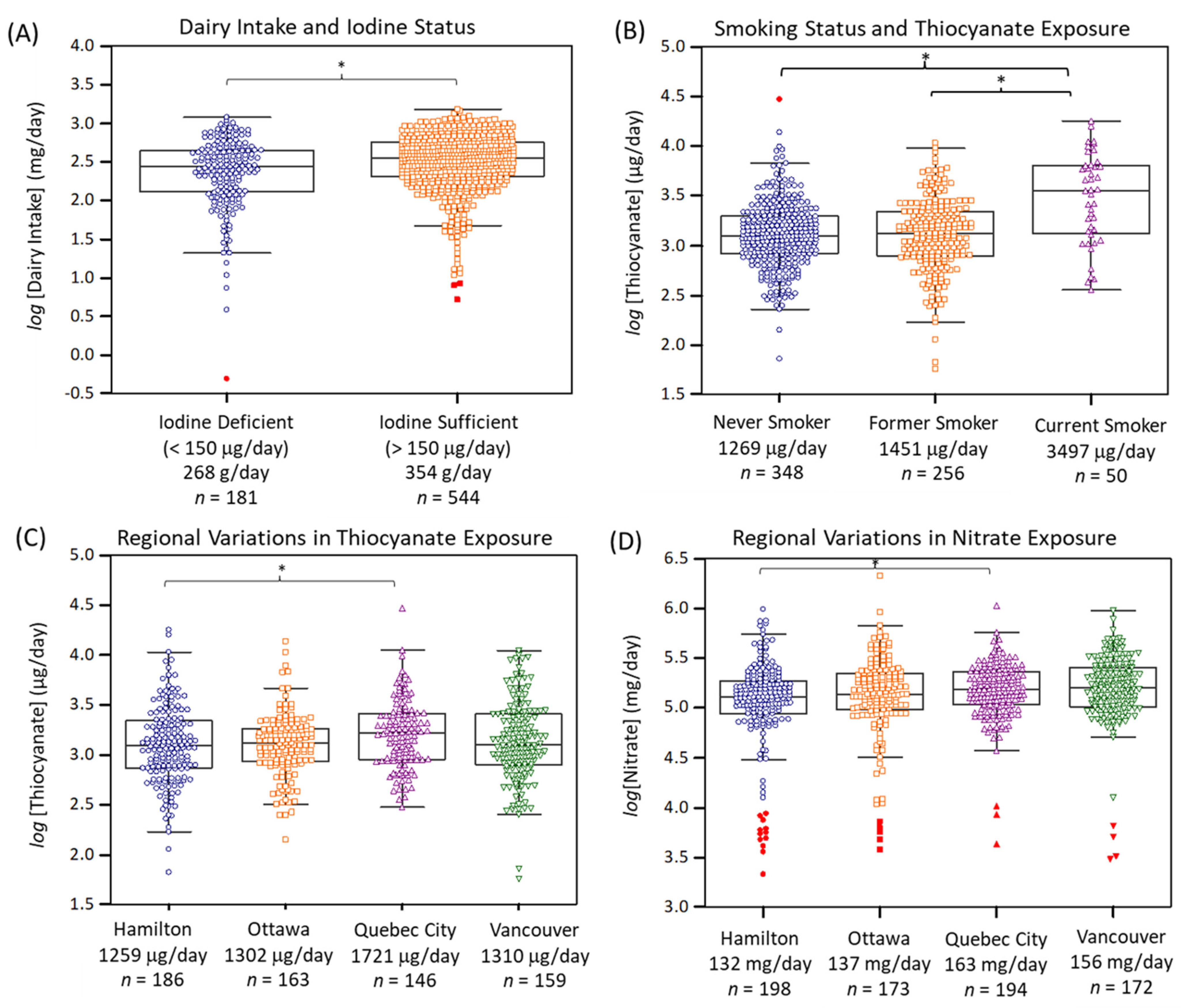
3.3. Factors Contributing to Iodine Deficiency in Canada
3.4. Risk Assessment of Iodine Deficiency from Exposure to Environmental Iodine Uptake Inhibitors
4. Discussion
4.1. Iodine Nutritional Status of Canadian Adults
4.2. Major Dietary Sources of Iodine Nutrition in Canada
4.3. Regional Variations in Iodine Deficiency across Canada Modulated by Exposure to Iodine Uptake Inhibitors
4.4. Study Strengths, Limitations and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chung, H.R. Iodine and thyroid function. Ann. Pediatr. Endocrinol. Metab. 2014, 19, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, P.R.; Zavacki, A.M. The role of the iodothyronine deiodinases in the physiology and pathophysiology of thyroid hormone action. Eur. Thyroid J. 2012, 1, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Andersson, M. Assessment of iodine nutrition in populations: Past, present, and future. Nutr. Rev. 2012, 70, 553–570. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Steer, C.D.; Golding, J.; Emmett, P.; Rayman, M.P. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Nazeri, P.; Mirmiran, P.; Shiva, N.; Mehrabi, Y.; Mojarrad, M.; Azizi, F. Iodine nutrition status in lactating mothers residing in countries with mandatory and voluntary iodine fortification programs: An updated systematic review. Thyroid 2015, 25, 611–620. [Google Scholar] [CrossRef] [Green Version]
- Laurberg, P.; Nøhr, S.B.; Pedersen, K.M.; Hreidarsson, A.B.; Andersen, S.; Bülow Pedersen, I.; Knudsen, N.; Perrild, H.; Jørgensen, T.; Ovesen, L. Thyroid disorders in mild iodine deficiency. Thyroid 2000, 10, 951–963. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Boelaert, K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015, 3, 286–295. [Google Scholar] [CrossRef]
- Bilal, M.Y.; Dambaeva, S.; Kwak-Kim, J.; Gilman-Sachs, A.; Beaman, K.D. A Role for iodide and thyroglobulin in modulating the function of human immune cells. Front. Immunol. 2017, 8, 1573. [Google Scholar] [CrossRef] [Green Version]
- Pearce, E.N.; Andersson, M.; Zimmermann, M.B. Global iodine nutrition: Where do we stand in 2013? Thyroid 2013, 23, 523–528. [Google Scholar] [CrossRef]
- Li, Y.; Teng, D.; Ba, J.; Chen, B.; Du, J.; He, L.; Lai, X.; Teng, X.; Shi, X.; Li, Y.; et al. Efficacy and safety of long-term universal salt iodization on thyroid disorders: Epidemiological evidence from 31 provinces of mainland China. Thyroid 2020, 30, 568–579. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Andersson, M. Global Endocrinology: Global perspectives in endocrinology: Coverage of iodized salt programs and iodine status in 2020. Eur. J. Endocrinol. 2021, 185, R13–R21. [Google Scholar] [CrossRef] [PubMed]
- Farebrother, J.; Zimmermann, M.B.; Andersson, M. Excess iodine intake: Sources, assessment, and effects on thyroid function. Ann. N. Y. Acad. Sci. 2019, 1446, 44–65. [Google Scholar] [CrossRef] [PubMed]
- Krela-Kazmierczak, I.; Czarnywojtek, A.; Skoracka, K.; Rychter, A.M.; Ratajczak, A.E.; Szymczak-Tomczak, A.; Ruchała, M.; Dobrowolska, A. Is there an ideal diet to protect against iodine deficiency? Nutrients 2021, 13, 513. [Google Scholar] [CrossRef] [PubMed]
- Nista, F.; Bagnasco, M.; Gatto, F.; Albertelli, M.; Vera, L.; Boschetti, M.; Musso, N.; Ferone, D. The effect of sodium restriction on iodine prophylaxis: A review. J. Endocrinol. Investig. 2022, 45, 1121–1138. [Google Scholar] [CrossRef]
- Knowles, J.; van der Haar, F.; Shehata, M.; Gerasimov, G.; Bimo, B.; Cavenagh, B.; Maramag, C.C.; Otico, E.; Izwardy, D.; Spohrer, R.; et al. Iodine intake through processed food: Case studies from Egypt, Indonesia, the Philippines, the Russian Federation and Ukraine, 2010–2015. Nutrients 2017, 9, 797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlton, K.; Probst, Y.; Kiene, G. Dietary iodine intake of the Australian population after introduction of a mandatory iodine fortification programme. Nutrients 2016, 8, 701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pehrsson, P.R.; Patterson, K.Y.; Spungen, J.H.; Wirtz, M.S.; Andrews, K.W.; Dwyer, J.T.; Swanson, C.A. Iodine in food- and dietary supplement composition databases. Am. J. Clin. Nutr. 2016, 104, 868S–876S. [Google Scholar] [CrossRef] [Green Version]
- Roseland, J.M.; Phillips, K.M.; Patterson, K.Y.; Pehrsson, P.R.; Bahadur, R.; Ershow, A.G.; Somanchi, M. Large variability of iodine content in retail cow’s milk in the U.S. Nutrients 2020, 12, 1246. [Google Scholar] [CrossRef]
- Zhao, W.; Han, C.; Shi, X.; Xiong, C.; Sun, J.; Shan, Z.; Teng, W. Prevalence of goiter and thyroid nodules before and after implementation of the universal salt iodization program in mainland China from 1985 to 2014: A systematic review and meta-analysis. PLoS ONE 2014, 9, e109549. [Google Scholar] [CrossRef]
- König, F.; Andersson, M.; Hotz, K.; Aeberli, I.; Zimmermann, M.B. Ten repeat collections for urinary iodine from spot samples or 24-hour samples are needed to reliably estimate individual iodine status in women. J. Nutr. 2011, 141, 2049–2054. [Google Scholar] [CrossRef]
- WHO. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; World Health Organization and Food and Agriculture Organization of the United Nations: Geneva, Switzerland, 2004; pp. 303–314.
- Li, M.; Eastman, C.J. The changing epidemiology of iodine deficiency. Nat. Rev. Endocrinol. 2012, 8, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Vejbjerg, P.; Knudsen, N.; Perrild, H.; Laurberg, P.; Andersen, S.; Rasmussen, L.B.; Ovesen, L.; Jørgensen, T. Estimation of iodine intake from various urinary iodine measurements in population studies. Thyroid 2009, 19, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Perrine, C.G.; Cogswell, M.E.; Swanson, C.A.; Sullivan, K.M.; Chen, T.C.; Carriquiry, A.L.; Dodd, K.E.; Caldwell, K.L.; Wang, C. Comparison of population iodine estimates from 24-hour urine and timed-spot urine samples. Thyroid 2014, 24, 748–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montenegro-Bethancourt, G.; Johner, S.A.; Stehle, P.; Neubert, A.; Remer, T. Iodine status assessment in children: Spot urine iodine concentration reasonably reflects true twenty-four-hour iodine excretion only when scaled to creatinine. Thyroid 2015, 25, 688–697. [Google Scholar] [CrossRef]
- Doggui, R.; El Ati-Hellal, M.; Traissac, P.; El Ati, J. Pre-analytical factors influence accuracy of urine spot iodine assessment in epidemiological surveys. Biol. Trace Elem. Res. 2018, 186, 337–345. [Google Scholar] [CrossRef]
- Chen, W.; Wu, Y.; Lin, L.; Tan, L.; Shen, J.; Pearce, E.N.; Guo, X.; Wang, W.; Bian, J.; Jiang, W.; et al. 24-hour urine samples are more reproducible than spot urine samples for evaluation of iodine status in school-age children. J. Nutr. 2016, 146, 142–146. [Google Scholar] [CrossRef] [Green Version]
- Niwattisaiwong, S.; Burman, K.D.; Li-Ng, M. Iodine deficiency: Clinical implications. Clev. Clin. J. Med. 2017, 84, 236–244. [Google Scholar] [CrossRef]
- Government of Canada. Iodine Status of Canadians, 2009 to 2011. Statistics Canada. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2012001/article/11733-eng.htm (accessed on 1 May 2022).
- Bertinato, J.; Qiao, C.; L’Abbé, M.R. Iodine status of Canadian children, adolescents, and women of childbearing age. J. Nutr. 2021, 151, 3710–3717. [Google Scholar] [CrossRef]
- Eisenbrand, G.; Gelbke, H.P. Assessing the potential impact on the thyroid axis of environmentally relevant food constituents/contaminants in humans. Arch. Toxicol. 2016, 90, 1841–1857. [Google Scholar] [CrossRef]
- Ozpinar, A.; Kelestimur, F.; Songur, Y.; Can, O.; Valentin, L.; Caldwell, K.; Arikan, E.; Unsal, I.; Serteser, M.; Inal, T.; et al. Iodine status in Turkish populations and exposure to iodide uptake inhibitors. PLoS ONE 2014, 9, e88206. [Google Scholar] [CrossRef]
- Mente, A.; Dagenais, G.; Wielgosz, A.; Lear, S.A.; McQueen, M.J.; Zeidler, J.; Fu, L.; DeJesus, J.; Rangarajan, S.; Bourlaud, A.S.; et al. Assessment of dietary sodium and potassium in Canadians using 24-hour urinary collection. Can. J. Cardiol. 2016, 32, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Nori de Macedo, A.; Teo, K.; Mente, A.; McQueen, M.J.; Zeidler, J.; Poirier, P.; Lear, S.A.; Wielgosz, A.; Britz-McKibbin, P. A robust method for iodine status determination in epidemiological studies by capillary electrophoresis. Anal. Chem. 2014, 86, 10010–10015. [Google Scholar] [CrossRef] [PubMed]
- Nori de Macedo, A.; Macri, J.; Hudecki, P.L.; Saoi, M.; McQueen, M.J.; Britz-McKibbin, P. Validation of a capillary electrophoresis assay for monitoring iodine nutrition in populations for prevention of iodine deficiency: An interlaboratory method comparison. J. Appl. Lab. Med. 2017, 1, 649–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakobsen, J.; Ovesen, L.; Fagt, S.; Pedersen, A.N. Para-aminobenzoic acid used as a marker for completeness of 24 hour urine: Assessment of control limits for a specific HPLC method. Eur. J. Clin. Nutr. 1997, 51, 514–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teo, K.; Chow, C.K.; Vaz, M.; Rangarajan, S.; Yusuf, S.; PURE Investigators-Writing Group. The Prospective Urban Rural Epidemiology (PURE) study: Examining the impact of societal influences on chronic noncommunicable diseases in low-, middle-, and high-income countries. Am. Heart J. 2009, 158, 1–7.e1. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Shin, D.; Cho, M.S.; Song, W.O. Food group intakes as determinants of iodine status among US adult population. Nutrients 2016, 8, 325. [Google Scholar] [CrossRef] [Green Version]
- Bajaj, J.K.; Salwan, P.; Salwan, S. Various possible toxicants involved in thyroid dysfunction: A review. J. Clin. Diagn. Res. 2016, 10, FE01-3. [Google Scholar] [CrossRef]
- Mendy, A. Association of urinary nitrate with lower prevalence of hypertension and stroke and with reduced risk of cardiovascular mortality. Circulation 2018, 137, 2295–2297. [Google Scholar] [CrossRef]
- Health Canada. Dietary Sources. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-nutrition-surveillance/health-nutrition-surveys/canadian-health-measures-survey/iodine-nutrition-biomarkers-cycle-1-canadian-health-measures-survey-food-nutrition-surveillance-health-canada.html (accessed on 1 May 2022).
- Dold, S.; Zimmermann, M.B.; Jukic, T.; Kusic, Z.; Jia, Q.; Sang, Z.; Quirino, A.; San Luis, T.O.L.; Fingerhut, R.; Kupka, R.; et al. Universal salt iodization provides sufficient dietary iodine to achieve adequate iodine nutrition during the first 1000 Days: A cross-sectional multicenter study. J. Nutr. 2018, 148, 587–598. [Google Scholar] [CrossRef]
- Mente, A.; O’Donnell, M.; Rangarajan, S.; McQueen, M.; Dagenais, G.; Wielgosz, A.; Lear, S.; Ah, S.T.L.; Wei, L.; Diaz, R.; et al. Urinary sodium excretion, blood pressure, cardiovascular disease, and mortality: A community-level prospective epidemiological cohort study. Lancet 2018, 392, 496–506. [Google Scholar] [CrossRef]
- Graudal, N. Population data on blood pressure and dietary sodium and potassium do not support public health strategy to reduce salt intake in Canadians. Can. J. Cardiol. 2016, 32, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Groufh-Jacobsen, S.; Hess, S.Y.; Aakre, I.; Folven Gjengedal, E.L.; Blandhoel Pettersen, K.; Henjum, S. Vegans vegetarians and pescatarians are at risk of iodine deficiency in Norway. Nutrients 2020, 12, 3555. [Google Scholar] [CrossRef] [PubMed]
- Fallon, N.; Dillon, S.A. Low intakes of iodine and selenium amongst vegan and vegetarian women highlight a potential nutritional vulnerability. Front. Nutr. 2020, 7, 72. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.B.; Ovesen, L.; Christiansen, E. Day-to-day and within-day variation in urinary iodine excretion. Eur. J. Clin. Nutr. 1999, 53, 401–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Als, C.; Helbling, A.; Peter, K.; Haldimann, M.; Zimmerli, B.; Gerber, H. Urinary iodine concentration follows a circadian rhythm: A study with 3023 spot urine samples in adults and children. J. Clin. Endocrinol. Metab. 2000, 85, 1367–1369. [Google Scholar] [CrossRef]
- Valentín-Blasini, L.; Blount, B.C.; Delinsky, A. Quantification of iodide and sodium-iodide symporter inhibitors in human urine using ion chromatography tandem mass spectrometry. J. Chromatogr. A 2007, 1155, 40–46. [Google Scholar] [CrossRef]
- Cheuvront, S.N. Urinalysis for hydration assessment: An age-old problem. Am. J. Clin. Nutr. 2016, 104, 3–4. [Google Scholar] [CrossRef] [Green Version]
- Health Canada. Dietary Reference Intakes, Updated November 2010. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/healthy-eating/dietary-reference-intakes/tables.html (accessed on 1 May 2022).
- Dahl, L.; Wik Markhus, M.; Sanchez, P.V.R.; Moe, V.; Smith, L.; Meltzer, H.M.; Kjellevold, M. Iodine deficiency in a study population of Norwegian pregnant women-Results from the Little in Norway Study (LiN). Nutrients 2018, 10, 513. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.; Lee, S.Y.; Stagnaro-Green, A.; MacKay, D.; Wong, A.W.; Pearce, E.N. Iodine content of the best-selling United States adult and prenatal multivitamin preparations. Thyroid 2019, 29, 124–127. [Google Scholar] [CrossRef]
- Leung, A.M.; Pearce, E.N.; Braverman, L.E. Iodine content of prenatal multivitamins in the United States. N. Engl. J. Med. 2009, 360, 939–940. [Google Scholar] [CrossRef] [Green Version]
- Parle, J.V.; Franklyn, J.A.; Cross, K.W.; Jones, S.R.; Sheppard, M.C. Thyroxine prescription in the community: Serum thyroid stimulating hormone level assays as an indicator of undertreatment or overtreatment. Br. J. Gen. Pract. 1993, 43, 107–109. [Google Scholar] [PubMed]
- Shimoda, S.I.; Kasai, K.; Kikuchi, T.; Ieiri, T. Preferential renal excretion of iodide derived from thyroxine and triiodothyronine deiodination in man. J. Clin. Endocrinol. Metab. 1977, 44, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Bouga, M.; Lean, M.E.J.; Combet, E. Contemporary challenges to iodine status and nutrition: The role of foods, dietary recommendations, fortification and supplementation. Proc. Nutr. Soc. 2018, 77, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Watutantrige-Fernando, S.; Barollo, S.; Bertazza, L.; Sensi, F.; Cavedon, E.; Censi, S.; Veronese, N.; Ceccato, F.; Vianello, F.; Boscaro, M.; et al. Iodine status in the elderly: Association with milk intake and other dietary habits. J. Nutr. Health Food Sci. 2017, 5, 1–5. [Google Scholar] [CrossRef]
- Borucki Castro, S.I.; Berthiaume, R.; Laffey, P.; Fouquet, A.; Beraldin, F.; Robichaud, A.; Lacasse, P. Iodine concentration in milk sampled from Canadian farms. J. Food Prot. 2010, 73, 1658–1663. [Google Scholar] [CrossRef]
- Flachowsky, G.; Franke, K.; Meyer, U.; Leiterer, M.; Schöne, F. Influencing factors on iodine content of cow milk. Eur. J. Nutr. 2014, 53, 351–365. [Google Scholar] [CrossRef]
- Phillips, D.I. Iodine, milk, and the elimination of endemic goitre in Britain: The story of an accidental public health triumph. J. Epidemiol. Community Health 1997, 51, 391–393. [Google Scholar] [CrossRef] [Green Version]
- van der Reijden, O.L.; Galetti, V.; Bürki SZeder, C.; Krzystek, A.; Haldimann, M.; Berard, M.B.; Zimmermann, J.; Herter-Aeberli, I. Iodine bioavailability from cow milk: A randomized, crossover balance study in healthy iodine-replete adults. Am. J. Clin. Nutr. 2019, 110, 102–110. [Google Scholar] [CrossRef]
- Bath, S.C.; Hill, S.; Infante, H.G.; Elghul, S.; Nezianya, C.J.; Rayman, M.P. Iodine concentration of milk-alternative drinks available in the UK in comparison with cows’ milk. Br. J. Nutr. 2017, 118, 525–532. [Google Scholar] [CrossRef] [Green Version]
- Government of Canada. Available online: https://food-guide.canada.ca/en/healthy-eating-recommendations (accessed on 1 May 2022).
- Rasmussen, L.B.; Jørgensen, T.; Perrild, H.; Knudsen, N.; Krejbjerg, A.; Laurberg, P.; Pedersen, I.B.; Bjergved, L.; Ovesen, L. Mandatory iodine fortification of bread and salt increases iodine excretion in adults in Denmark—A 11-year follow-up study. Clin. Nutr. 2014, 33, 1033–1040. [Google Scholar] [CrossRef]
- Yu, S.; Wang, D.; Cheng, X.; Zhang, Q.; Wang, M.; Guo, H.; Yu, B.; Zhang, X.; Xia, L.; Sun, D.; et al. Establishing reference intervals for urine and serum iodine levels: A nationwide multicenter study of a euthyroid Chinese population. Clin. Chim. Acta 2020, 502, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, N.; Bülow, I.; Laurberg, P.; Perrild, H.; Ovesen, L.; Jørgensen, T. Alcohol consumption is associated with reduced prevalence of goitre and solitary thyroid nodules. Clin. Endocrinol. 2001, 55, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Carlé, A.; Pedersen, I.B.; Knudsen, N.; Perrild, H.; Ovesen, L.; Rasmussen, L.B.; Jørgensen, T.; Laurberg, P. Moderate alcohol consumption may protect against overt autoimmune hypothyroidism: A population-based case-control study. Eur. J. Endocrinol. 2012, 167, 483–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.L.; Lam, L.T.; Zeng, Q.; Han, S.Q.; Fu, G.; Hou, C.C. Effects of drinking water with high iodine concentration on the intelligence of children in Tianjin, China. J. Public Health 2009, 31, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Leung, A.M.; Katz, P.M.; He, X.; Feig, D.S.; Pearce, E.N.; Braverman, L.E. Urinary perchlorate and thiocyanate concentrations in pregnant women from Toronto, Canada. Thyroid 2014, 24, 175–176. [Google Scholar] [CrossRef] [Green Version]
- Tonacchera, M.; Pinchera, A.; Dimida, A.; Ferrarini, E.; Agretti, P.; Vitti, P.; Santini, F.; Crump, K.; Gibbs, J. Relative potencies and additivity of perchlorate, thiocyanate, nitrate, and iodide on the inhibition of radioactive iodide uptake by the human sodium iodide symporter. Thyroid 2004, 14, 1012–1019. [Google Scholar] [CrossRef] [Green Version]
- Mortensen, M.E.; Birch, R.; Wong, L.Y.; Valentin-Blasini, L.; Boyle, E.B.; Caldwell, K.L.; Merrill, L.S.; Moye, J., Jr.; Blount, B.C. Thyroid antagonists and thyroid indicators in U.S. pregnant women in the Vanguard Study of the National Children’s Study. Environ. Res. 2016, 149, 179–188. [Google Scholar] [CrossRef] [Green Version]
- Buratti, M.; Xaiz, D.; Caravelliand, G.; Colombi, A. Validation of urinary thiocyanate as a biomarker of tobacco smoking. Biomarkers 1997, 2, 81–85. [Google Scholar] [CrossRef]
- Jain, R. Trends and variability in the levels of urinary thiocyanate, perchlorate, and nitrate by age, gender, race/ethnicity, smoking status, and exposure to environmental tobacco smoke over 2005–2012. Sci. Total Environ. 2016, 557–558, 221–230. [Google Scholar] [CrossRef]
- Vanderver, G.B.; Engel, A.; Lamm, S. Cigarette smoking and iodine as hypothyroxinemic stressors in U.S. women of childbearing age: A NHANES III analysis. Thyroid 2007, 17, 741–746. [Google Scholar] [CrossRef] [Green Version]
- Blount, B.C.; Alwis, K.U.; Jain, R.B.; Solomon, B.L.; Morrow, J.C.; Jackson, W.A. Perchlorate, nitrate, and iodide intake through tap water. Environ. Sci. Technol. 2010, 44, 9564–9570. [Google Scholar] [CrossRef] [PubMed]
- De Groef, B.; Decallonne, B.R.; Van der Geyten, S.; Darras, V.M.; Bouillon, R. Perchlorate versus other environmental sodium/iodide symporter inhibitors: Potential thyroid-related health effects. Eur. J. Endocrinol. 2006, 155, 17–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manousou, S.; Stål, M.; Larsson, C.; Mellberg, C.; Lindahl, B.; Eggertsen, R.; Hulthén, L.; Olsson, T.; Ryberg, M.; Sandberg, S.; et al. A Paleolithic-type diet results in iodine deficiency: A 2-year randomized trial in postmenopausal obese women. Eur. J. Clin. Nutr. 2018, 72, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.V.; Erskine, N.A.; Kiefe, C.I.; Barton, B.A.; Lapane, K.L.; Do, V.T.H.; Goldberg, R.J. Is low iodine a risk factor for cardiovascular disease in Americans without thyroid dysfunction? Findings from NHANES. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 651–656. [Google Scholar] [CrossRef]
- Herter-Aeberli, I.; Cherkaoui, M.; El Ansari, N.; Rohner, R.; Stinca, S.; Chabaa, L.; von Eckardstein, A.; Aboussad, A.; Zimmermann, M.B. Iodine supplementation decreases hypercholesterolemia in iodine-deficient, overweight women: A randomized controlled trial. J. Nutr. 2015, 145, 2067–2075. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | 24 h UIE (µg/day) | 24 h UIC (µg/L) | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age | 0.99 (0.99–1.01) | 0.257 | 0.98 (0.97–1.00) | 0.0516 |
| Male sex | 0.80 (0.56–1.14) | 0.215 | 0.76 (0.56–1.03) | 0.0754 |
| BMI (>27 kg/m2) | 0.66 (0.47–0.92) | 0.0153 | 0.99 (0.96–1.02) | 0.515 |
| 24 h Urine volume (L) | 0.69 (0.56–0.85) | 4.07 × 10−4 | 2.31 (1.91–2.81) | 5.87 × 10−17 |
| Current smoker | 0.85 (0.43–1.67) | 0.635 | 1.13 (0.64–1.99) | 0.671 |
| Current alcohol consumer | 1.59 (0.98–2.47) | 0.059 | 1.48 (1.00–2.20) | 0.0505 |
| Study site: | ||||
| Hamilton | 1.00 (ref.) | -- | 1.00 (ref.) | -- |
| Vancouver | 2.54 (1.52–4.23) | 3.57 × 10−4 | 1.83 (1.20–2.81) | 5.31 × 10−3 |
| Quebec City | 2.58 (1.57–4.22) | 1.74 × 10−4 | 1.89 (1.25–2.84) | 2.41 × 10−3 |
| Ottawa | 1.19 (0.69–2.05) | 0.531 | 1.28 (0.85–1.93) | 0.839 |
| Rural location | 0.99 (0.69–1.60) | 0.953 | 1.28 (0.85–1.93) | 0.246 |
| Iodine supplementation | 0.18 (0.08–0.41) | 6.30 × 10−5 | 0.31 (0.19–0.52) | 8.77 × 10−6 |
| T4 prescription | 0.33 (0.14–0.78) | 1.20 × 10−2 | 0.43 (0.23–0.79) | 6.76 × 10−3 |
| Dairy intake (g/day) | 0.999 (0.998–0.999) | 3.94 × 10−4 | 0.999 (0.998–1.00) | 4.41 × 10−4 |
| Starch intake (g/day) | 0.999 (0.997–1.00) | 0.105 | 0.999 (0.997–1.00) | 0.0470 |
| Sodium excretion (g/day) | 0.71 (0.61–0.84) | 3.03 × 10−5 | 0.93 (0.83–1.05) | 0.265 |
| Salty food intake (g/day) | 1.00 (1.00–1.01) | 0.108 | 1.00 (0.97–1.00) | 0.856 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathiaparanam, S.; Nori de Macedo, A.; Mente, A.; Poirier, P.; Lear, S.A.; Wielgosz, A.; Teo, K.K.; Yusuf, S.; Britz-Mckibbin, P. The Prevalence and Risk Factors Associated with Iodine Deficiency in Canadian Adults. Nutrients 2022, 14, 2570. https://doi.org/10.3390/nu14132570
Mathiaparanam S, Nori de Macedo A, Mente A, Poirier P, Lear SA, Wielgosz A, Teo KK, Yusuf S, Britz-Mckibbin P. The Prevalence and Risk Factors Associated with Iodine Deficiency in Canadian Adults. Nutrients. 2022; 14(13):2570. https://doi.org/10.3390/nu14132570
Chicago/Turabian StyleMathiaparanam, Stellena, Adriana Nori de Macedo, Andrew Mente, Paul Poirier, Scott A. Lear, Andreas Wielgosz, Koon K. Teo, Salim Yusuf, and Philip Britz-Mckibbin. 2022. "The Prevalence and Risk Factors Associated with Iodine Deficiency in Canadian Adults" Nutrients 14, no. 13: 2570. https://doi.org/10.3390/nu14132570