
Socioeconomic, Eating- and Health-Related Limitations of Food Consumption among Polish Women 60+ Years: The ‘ABC of Healthy Eating’ Project

 ,
,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
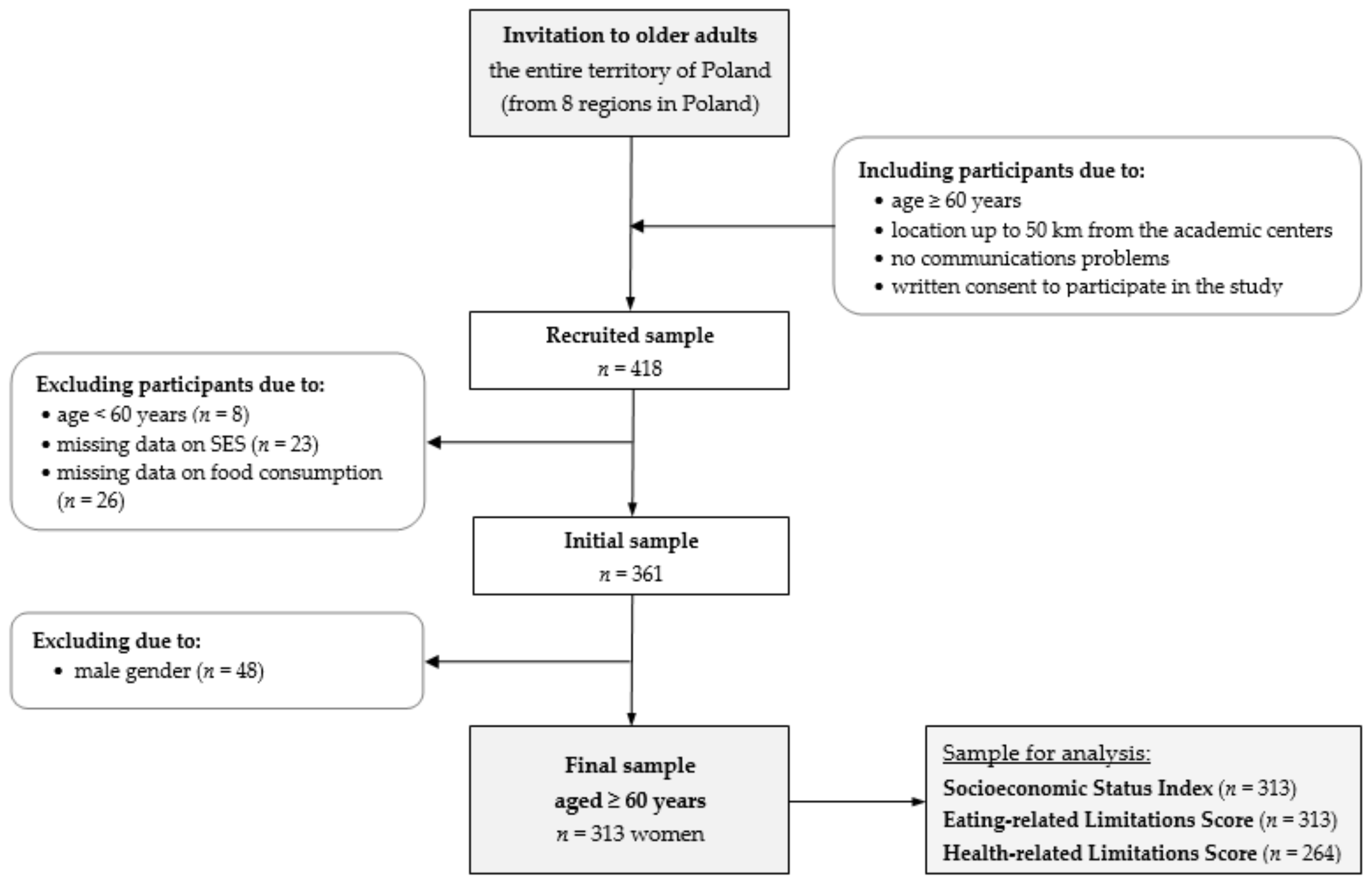
2.2. Study Design and Participants
2.3. Dietary Data
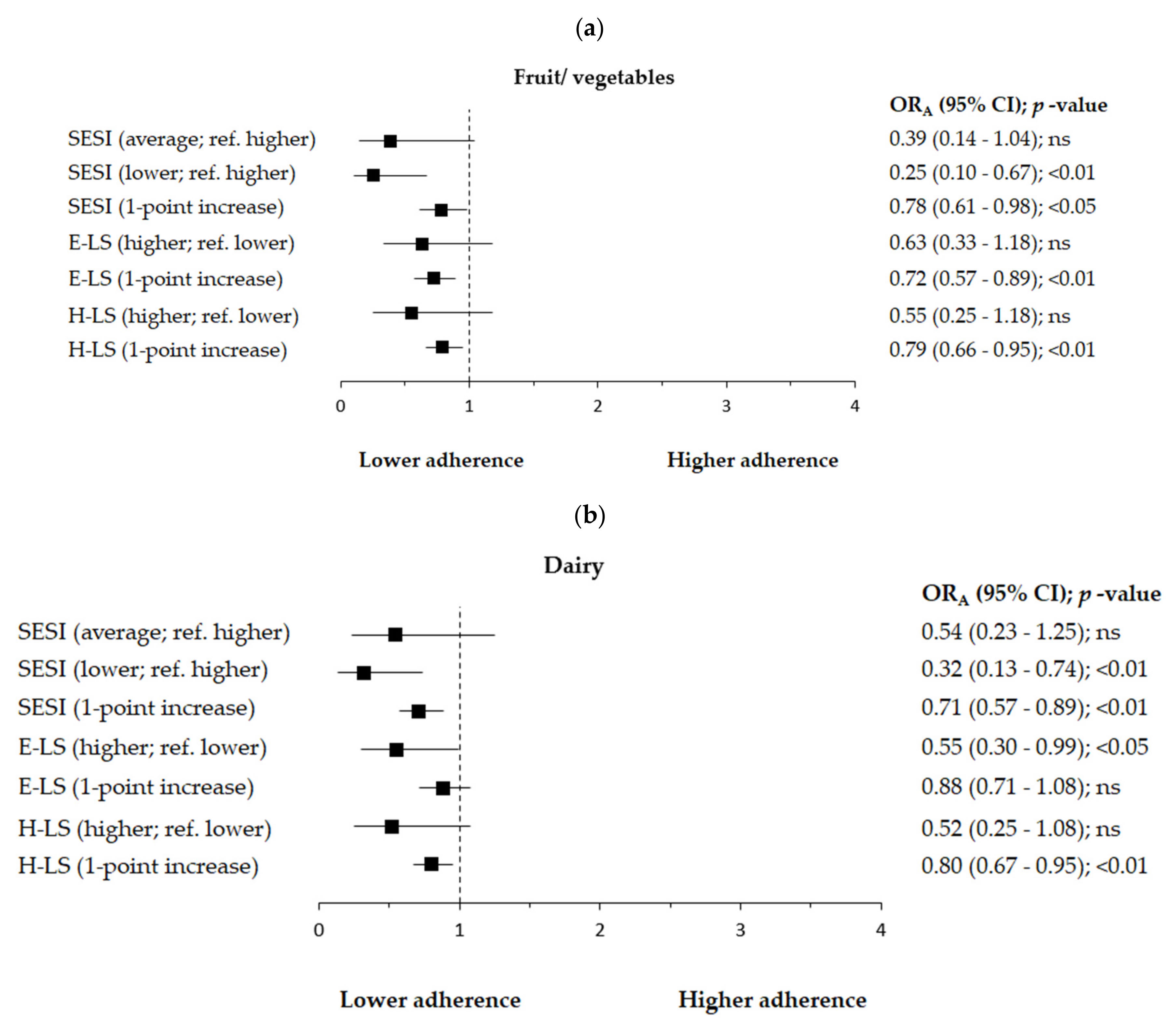
- fruit or vegetables <2, ≥2 servings/day (serving size: 80–100 g, e.g., medium-sized tomato or apple, 1 cup of raw leafy greens, ½ cup of cut-up fruit or vegetables, 1 cup of 100% fruit or vegetable juice);
- dairy (milk, fermented milk drinks, cheese, etc.) <1, ≥1 serving/day (serving size: e.g., a cup of milk, buttermilk, kefir or yoghurt, 100 g of cottage cheese, 2 slices of cheese);
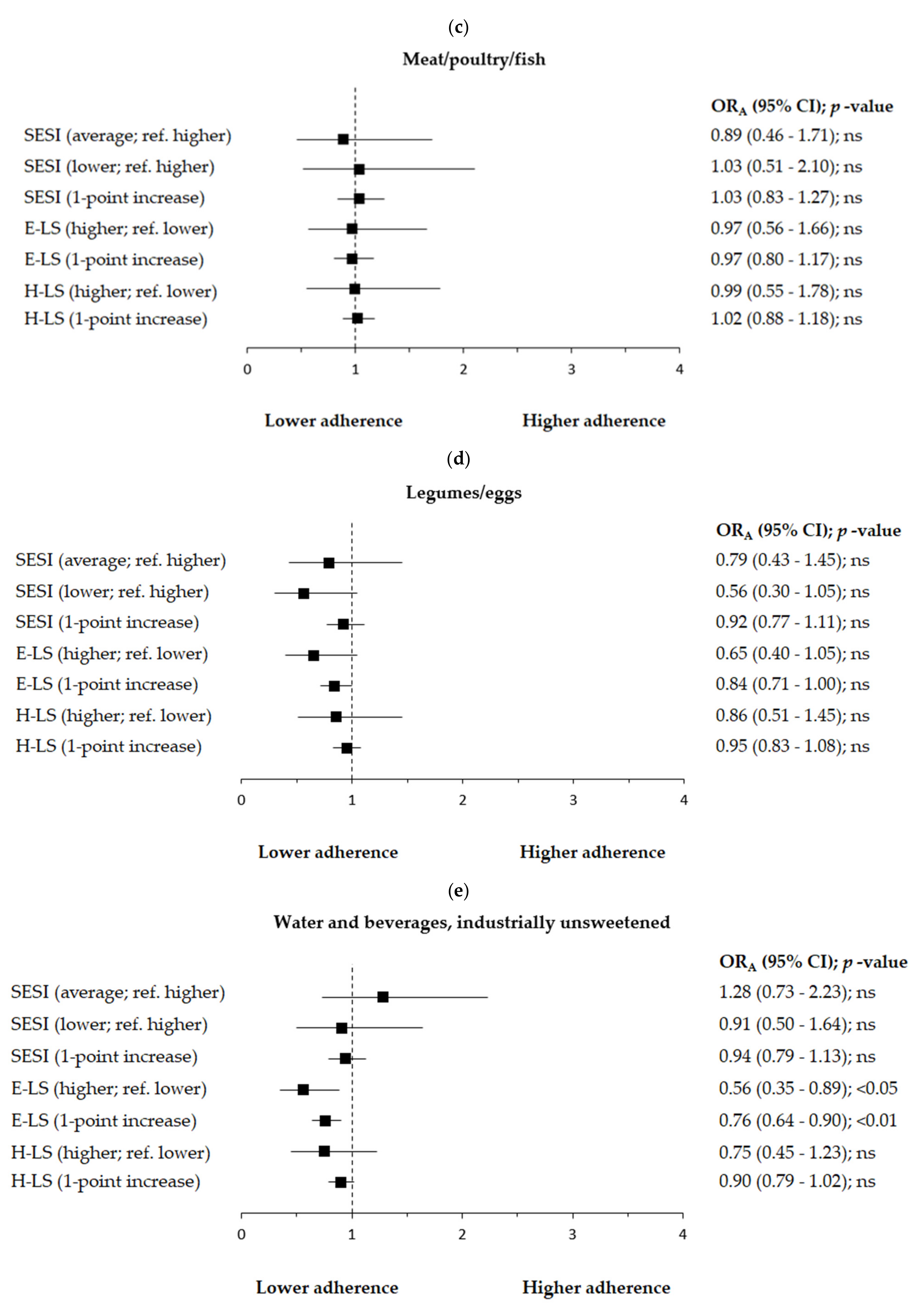
- meat or poultry or fish <1, ≥1 serving/day (serving size: 100–200 g, e.g., 100 g of meat, 2 slices of ham, 84 g of cooked fish or seafood);
- legumes (bean soup, pea soup, cooked beans etc.) or eggs <2, ≥2 servings/week (serving size: e.g., ¼ cup of cooked beans or peas, 1 egg or 2 egg whites);
- water and beverages industrially unsweetened (water, juice, coffee, tea, etc., excluding sweetened beverages coca-cola type) <6, ≥6 cups/day. Such categories were created due to the distribution and the average consumption of water and beverages industrially unsweetened in this study (approx. 1400 mL/day).
2.4. Anthropometric Measurements
2.5. Socioeconomic Status Index (SESI)
2.6. Eating-Related Limitations Score (E-LS)
2.7. Health-Related Limitations Score (H-LS)
2.8. Statistical Analysis
3. Results
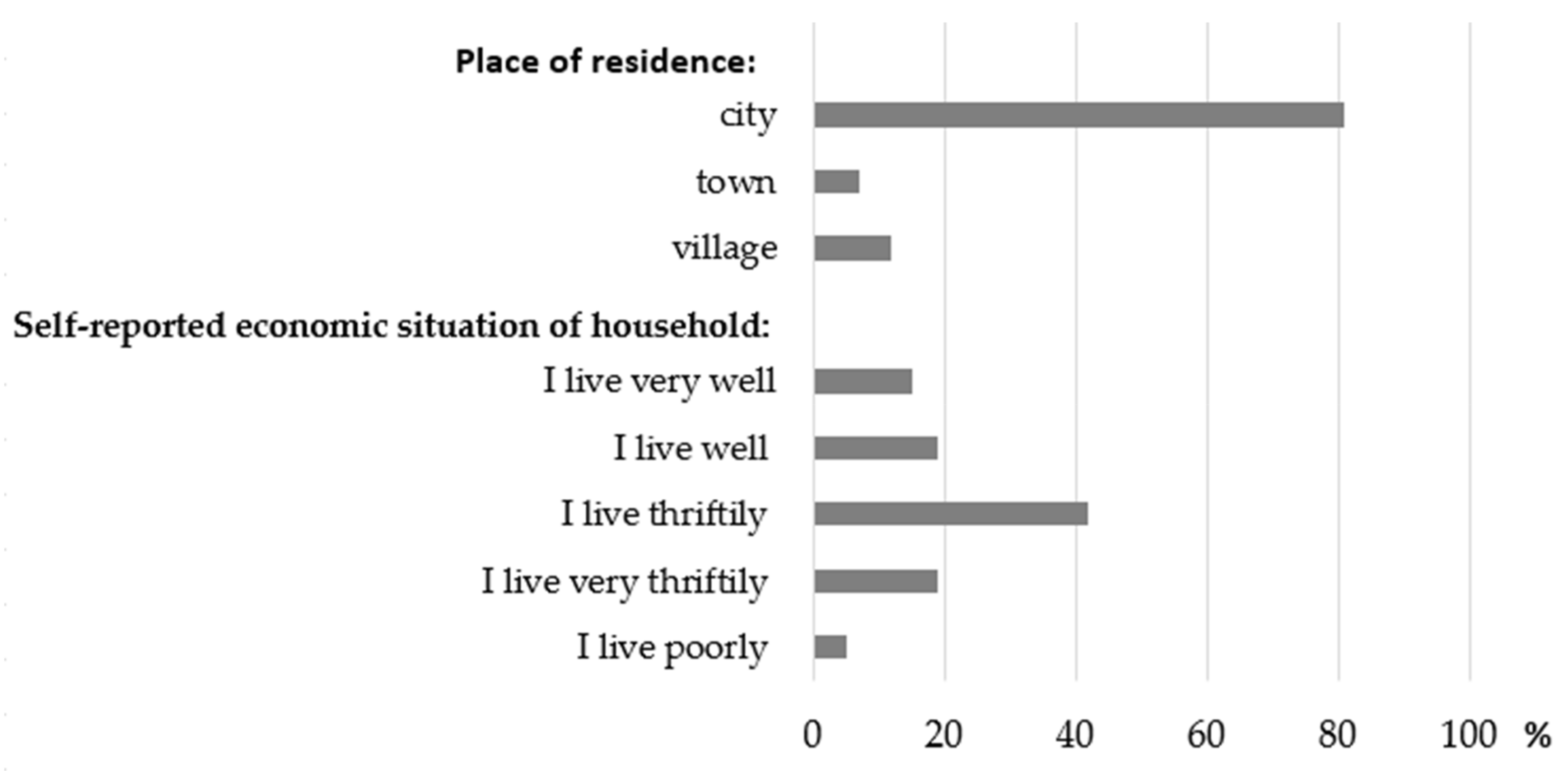
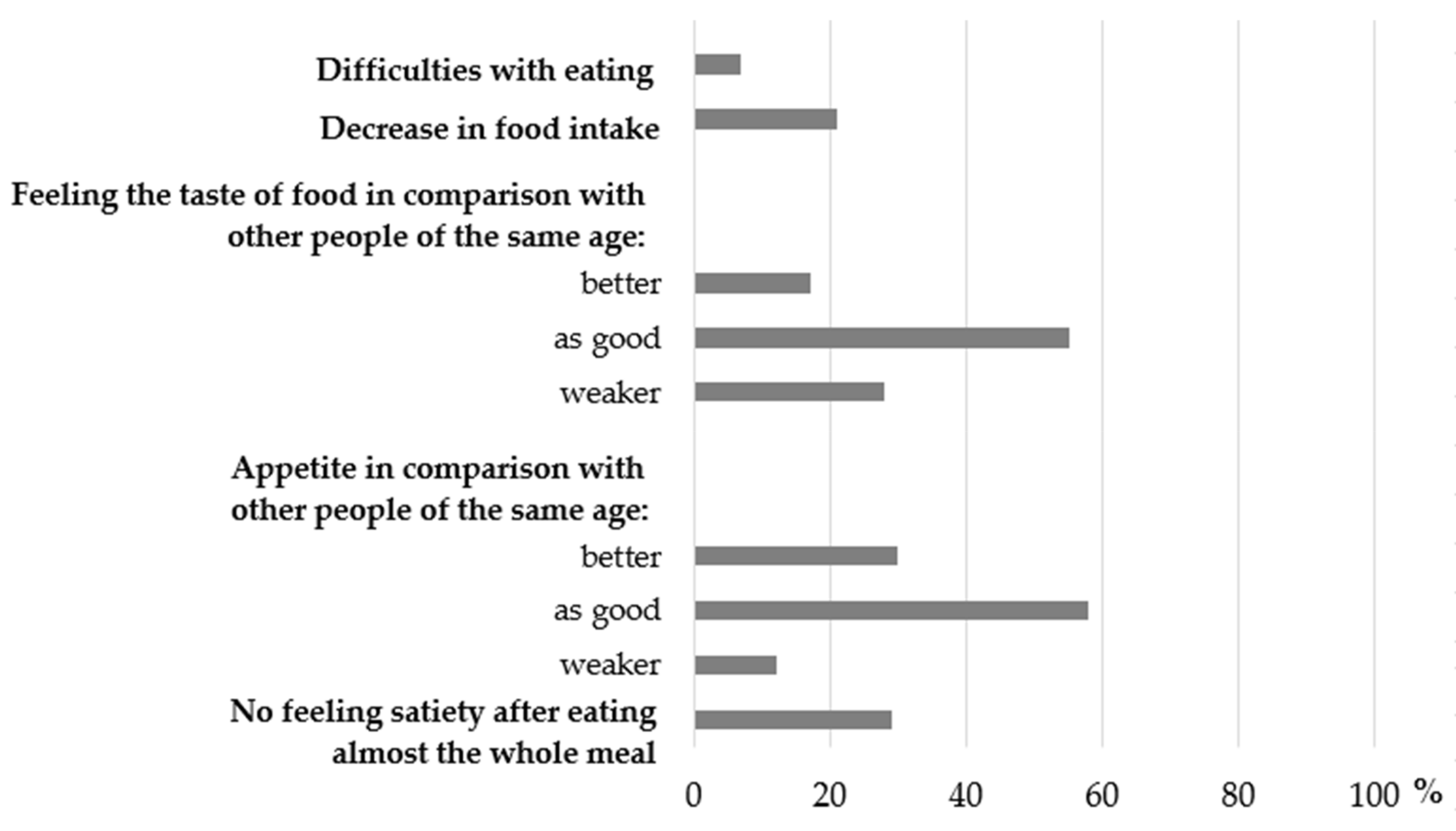
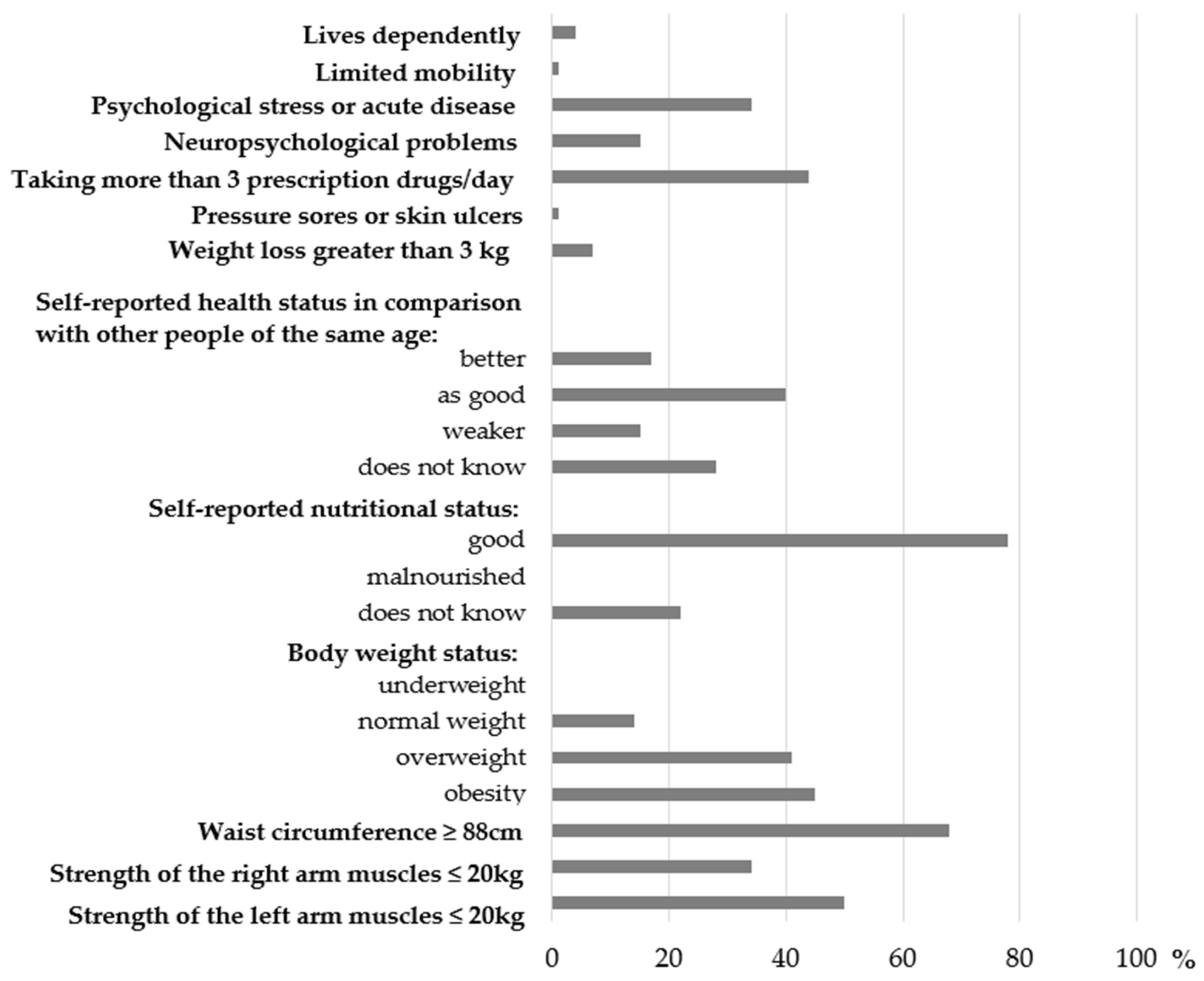
3.1. Distribution of the Components of Socioeconomic, Eating- and Health-Related Limitations Scores
3.2. Associations of Socioeconomic Status, Eating- and Health-Related Limitations with Food Consumption
4. Discussion
4.1. Socioeconomic Status and Food Consumption
4.2. Eating-Related Limitations of Food Consumption
4.3. Health-Related Limitations of Food Consumption
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.-W.; et al. Forecasting life expectancy, years of life lost, and all-Cause and cause-Specific mortality for 250 causes of death: Reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [Green Version]
- European Commission. Report on the Impact of Demographic Changes; Publications Office of the European Union: Luxembourg, 2020; Available online: https://ec.europa.eu/info/files/report-impact-demographic-change-reader-friendly-version-0_en (accessed on 29 March 2021).
- Central Statistical Office. Statistic Population in Poland. 2019. Available online: https://stat.gov.pl/obszary-tematyczne/ludnosc/ludnosc/ (accessed on 12 September 2020).
- Frackiewicz, J.; Włodarek, D.; Brzozowska, A.; Wierzbicka, E.; Słowińska, M.; Wądołowska, L.; Kaluza, J. Hematological parameters and all-cause mortality: A prospective study of older people. Aging Clin. Exp. Res. 2017, 30, 517–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, M.H.; González, M.P.; Colombo, P.B.; Calvo-Gallego, J. Mortality and use of healthcare resources in elderly patients in Seville: Differences between institutionalised patients and those included in a home care program. Semergen 2020, 47, 106–113. [Google Scholar] [CrossRef]
- Rizzuto, D.; Melis, R.J.F.; Angleman, S.; Qiu, C.; Marengoni, A. Effect of Chronic Diseases and Multimorbidity on Survival and Functioning in Elderly Adults. J. Am. Geriatr. Soc. 2017, 65, 1056–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perna, L.; Mielck, A.; Lacruz, M.E.; Emeny, R.T.; Holle, R.; Breitfelder, A.; Ladwig, K.H. Socioeconomic position, resilience, and health behaviour among elderly people. Int. J. Public Health 2011, 57, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Rosano, A.; Di Lazzaro, L.; Lubrano, C.; Carbonelli, M.; Pinto, A.; Giusti, A.M.; Lenzi, A.; Siervo, M. Impact of Disability, Psychological Status, and Comorbidity on Health-Related Quality of Life Perceived by Subjects with Obesity. Obes. Facts 2020, 13, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Zielińska, M.A.; Białecka, A.; Pietruszka, B.; Hamułka, J. Vegetables and fruit, as a source of bioactive substances, and impact on memory and cognitive function of elderly. Postepy Hig. Med. Dosw. 2017, 71, 267–280. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gómez, M.E.; Zapico, S.C. Frailty, Cognitive Decline, Neurodegenerative Diseases and Nutrition Interventions. Int. J. Mol. Sci. 2019, 20, 2842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verlaan, S.; Aspray, T.J.; Bauer, J.M.; Cederholm, T.; Hemsworth, J.; Hill, T.R.; McPhee, J.; Piasecki, M.; Seal, C.; Sieber, C.C.; et al. Nutritional status, body composition, and quality of life in community-dwelling sarcopenic and non-sarcopenic older adults: A case-control study. Clin. Nutr. 2015, 36, 267–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Ros, P.; Vila-Candel, R.; López-Hernández, L.; Martínez-Arnau, F.M. Nutritional Status and Risk Factors for Frailty in Community-Dwelling Older People: A Cross-Sectional Study. Nutrients 2020, 12, 1041. [Google Scholar] [CrossRef]
- Affret, A.; Severi, G.; Dow, C.; Rey, G.; Delpierre, C.; Boutron-Ruault, M.-C.; Clavel-Chapelon, F.; Fagherazzi, G. Socio-economic factors associated with a healthy diet: Results from the E3N study. Public Health Nutr. 2017, 20, 1574–1583. [Google Scholar] [CrossRef] [Green Version]
- Wadolowska, L.; Ulewicz, N.; Sobas, K.; Wuenstel, J.W.; Slowinska, M.A.; Niedzwiedzka, E.; Czlapka-Matyasik, M. Dairy-Related Dietary Patterns, Dietary Calcium, Body Weight and Composition: A Study of Obesity in Polish Mothers and Daughters, the MODAF Project. Nutrients 2018, 10, 90. [Google Scholar] [CrossRef] [Green Version]
- Nicklett, E.J.; Kadell, A.R. Fruit and vegetable intake among older adults: A scoping review. Maturitas 2013, 75, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Vandenberghe-Descamps, M.; Sulmont-Rossé, C.; Septier, C.; Feron, G.; Labouré, H. Using food comfortability to compare food’s sensory characteristics expectations of elderly people with or without oral health problems. J. Texture Stud. 2017, 48, 280–287. [Google Scholar] [CrossRef]
- Sergi, G.; Bano, G.; Pizzato, S.; Veronese, N.; Manzato, E. Taste loss in the elderly: Possible implications for dietary habits. Crit. Rev. Food Sci. Nutr. 2017, 57, 3684–3689. [Google Scholar] [CrossRef]
- Okamoto, N.; Amano, N.; Nakamura, T.; Yanagi, M. Relationship between tooth loss, low masticatory ability, and nutritional indices in the elderly: A cross-sectional study. BMC Oral Health 2019, 19, 110. [Google Scholar] [CrossRef] [Green Version]
- Picetti, D.; Foster, S.; Pangle, A.K.; Schrader, A.; George, M.; Wei, J.Y.; Azhar, G. Hydration health literacy in the elderly. Nutr. Health Aging 2017, 4, 227–237. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo, I.; Serra-Prat, M.; Yébenes, J.C. The Role of Water Homeostasis in Muscle Function and Frailty: A Review. Nutrients 2019, 11, 1857. [Google Scholar] [CrossRef] [Green Version]
- Gandy, J. Water intake: Validity of population assessment and recommendations. Eur. J. Nutr. 2015, 54, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Marseglia, A.; Xu, W.; Fratiglioni, L.; Fabbri, C.; Berendsen, A.A.M.; Bialecka-Debek, A.; Jennings, A.; Gillings, R.; Meunier, N.; Caumon, E.; et al. Effect of the NU-AGE Diet on Cognitive Functioning in Older Adults: A Randomized Controlled Trial. Front. Physiol. 2018, 9, 349. [Google Scholar] [CrossRef]
- Govindaraju, T.; Sahle, B.W.; McCaffrey, T.A.; McNeil, J.J.; Owen, A.J. Dietary Patterns and Quality of Life in Older Adults: A Systematic Review. Nutrients 2018, 10, 971. [Google Scholar] [CrossRef] [Green Version]
- Fabiani, R.; Naldini, G.; Chiavarini, M. Dietary Patterns in Relation to Low Bone Mineral Density and Fracture Risk: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 219–236. [Google Scholar] [CrossRef]
- Gu, Q.; Sable, C.M.; Brooks-Wilson, A.; Murphy, R.A. Dietary patterns in the healthy oldest old in the healthy aging study and the Canadian longitudinal study of aging: A cohort study. BMC Geriatr. 2020, 20, 106. [Google Scholar] [CrossRef] [Green Version]
- The Situation of Older People in Poland in 2019. Statistics Poland, Statistical Office in Białystok, Warsaw, Białystok 2021. Available online: https://stat.gov.pl/download/gfx/portalinformacyjny/en/defaultaktualnosci/3618/1/2/1/the_situation_of_older_people_in_poland_in_2019.pdf (accessed on 16 December 2021).
- Leblanc, V.; Hudon, A.-M.; Royer, M.-M.; Corneau, L.; Dodin, S.; Bégin, C.; Lemieux, S. Differences between men and women in dietary intakes and metabolic profile in response to a 12-week nutritional intervention promoting the Mediterranean diet. J. Nutr. Sci. 2015, 4, e13. [Google Scholar] [CrossRef] [Green Version]
- Peters, S.A.E.; Hyxley, R.R.; Woodward, M. Sex differences in body anthropometry and composition in individuals with and without diabetes in the UK Biobank. BMJ Open 2016, 6, e010007. [Google Scholar] [CrossRef] [Green Version]
- Guigoz, Y. The Mini-Nutritional Assessment (MNA®) Review of the Literature—What does it tell us? J. Nutr. Health Aging 2006, 10, 466–487. [Google Scholar]
- Söderhamn, U.; Dale, B.; Sundsli, K.; Söderhamn, O. Nutritional screening of older home-dwelling Norwegians: A comparison between two instruments. Clin. Interv. Aging 2012, 7, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Kowalkowska, J.; Wadolowska, L.; Czarnocinska, J.; Czlapka-Matyasik, M.; Galinski, G.; Jezewska-Zychowicz, M.; Bronkowska, M.; Dlugosz, A.; Loboda, D.; Wyka, J. Reproducibility of a Questionnaire for Dietary Habits, Lifestyle and Nutrition Knowledge Assessment (KomPAN) in Polish Adolescents and Adults. Nutrients 2018, 10, 1845. [Google Scholar] [CrossRef] [Green Version]
- Kwestionariusz do Badania Poglądów i Zwyczajów Zywieniowych oraz Procedura Opracowania Danych (KomPAN®): Wersja Polskojezyczna [Dietary Habits and Nutrition Beliefs Questionnaire and the Manual for Developing of Nutritional Data (Kom-PAN®). Committee of Human Nutrition Science Polish Academy of Science. Warsaw. 2014. Available online: http://www.knozc.pan.pl/ (accessed on 29 March 2020).
- Marfell-Jones, M.J.; Stewart, A.D.; de Ridder, J.H. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Wellington, New Zealand, 2012. [Google Scholar]
- Batsis, J.A.; Mackenzie, T.A.; Bartels, S.J.; Sahakyan, K.R.; Somers, V.K.; Lopez-Jimenez, F. Diagnostic accuracy of body mass index to identify obesity in older adults: NHANES 1999–2004. Int. J. Obes. 2015, 40, 761–767. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Serrano-Alarcón, M.; Perelman, J. Ageing under unequal circumstances: A cross-sectional analysis of the gender and socioeconomic patterning of functional limitations among the Southern European elderly. Int. J. Equity Health 2017, 16, 175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Styszynski, A.; Mossakowska, M.; Chudek, J.; Puzianowska-Kuznicka, M.; Klich-Raczka, A.; Neumann-Podczaska, A.; Szybalska, A.; Wieczorowska-Tobis, K. Prevalence of anemia in relation to socio-economic factors in elderly Polish population: The results of PolSenior study. J. Physiol. Pharmacol. 2018, 69, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Lallo, C.; Raitano, M. Life expectancy inequalities in the elderly by socioeconomic status: Evidence from Italy. Popul. Health Metr. 2018, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Van Der Meij, B.S.; Wijnhoven, H.; Lee, J.S.; Houston, D.K.; Hue, T.; Harris, T.B.; Kritchevsky, S.B.; Newman, A.B.; Visser, M. Poor Appetite and Dietary Intake in Community-Dwelling Older Adults. J. Am. Geriatr. Soc. 2017, 65, 2190–2197. [Google Scholar] [CrossRef] [Green Version]
- Hung, Y.; Wijnhoven, H.A.H.; Visser, M.; Verbeke, W. Appetite and Protein Intake Strata of Older Adults in the European Union: Socio-Demographic and Health Characteristics, Diet-Related and Physical Activity Behaviours. Nutrients 2019, 11, 777. [Google Scholar] [CrossRef] [Green Version]
- Wilson, M.-M.G.; Thomas, D.R.; Rubenstein, L.; Chibnall, J.T.; Anderson, S.; Baxi, A.; Diebold, M.R.; Morley, J.E. Appetite assessment: Simple appetite questionnaire predicts weight loss in community-dwelling adults and nursing home residents. Am. J. Clin. Nutr. 2005, 82, 1074–1081. [Google Scholar] [CrossRef]
- Siviero, P.; Zambon, S.; Limongi, F.; Castell, M.V.; Cooper, C.; Deeg, R.J.H.; Denkinger, M.; Dennison, E.M.; Edwards, M.H.; Gesmundo, A.; et al. How Hand Osteoarthritis, Comorbidity, and Pain Interact to Determine Functional Limitation in Older People: Observations from the European Project on OSteoArthritis Study. Arthritis Rheumatol. 2016, 68, 2662–2670. [Google Scholar] [CrossRef] [Green Version]
- Kondo, K.; Jingushi, S.; Ohfuji, S.; Sofue, M.; Itoman, M.; Matsumoto, T.; Hamada, Y.; Shindo, H.; Takatori, Y.; Yamada, H.; et al. Factors associated with functional limitations in the daily living activities of Japanese hip osteoarthritis patients. Int. J. Rheum. Dis. 2016, 20, 1372–1382. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhao, A. Dietary Diversity and Healthy Aging: A Prospective Study. Nutrients 2021, 13, 1787. [Google Scholar] [CrossRef]
- Lee, W.-J.; Liu, L.-K.; Peng, L.-N.; Lin, M.-H.; Chen, L.-K. Comparisons of Sarcopenia Defined by IWGS and EWGSOP Criteria Among Older People: Results From the I-Lan Longitudinal Aging Study. J. Am. Med Dir. Assoc. 2013, 14, 528.e1–528.e7. [Google Scholar] [CrossRef]
- World Health Organization. Waist Circumference and Waist–Hip Ratio: Report of a WHO Expert Consultation Geneva; World Health Organization: Geneva, Switzerland, 8—11 December 2008. [Google Scholar]
- Armitage, P.; Berry, G.; Matthews, J.N.S. Statistical Methods in Medical Research, 4th ed.; Blackwell Science: Oxford, UK, 2001. [Google Scholar]
- Middaugh, A.L.; Fisk, P.S.; Brunt, A.; Rhee, Y.S. Few Associations between Income and Fruit and Vegetable Consumption. J. Nutr. Educ. Behav. 2012, 44, 196–203. [Google Scholar] [CrossRef]
- Affret, A.; Severi, G.; Dow, C.; Mancini, F.R.; Rey, G.; Delpierre, C.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C.; Fagherazzi, G. Socio-economic factors associated with an increase in fruit and vegetable consumption: A 12-year study in women from the E3N-EPIC study. Public Health Nutr. 2017, 21, 740–755. [Google Scholar] [CrossRef] [Green Version]
- Krusinska, B.; Kowalkowska, J.; Wadolowska, L.; Wuenstel, J.W.; Slowinska, M.A.; Niedzwiedzka, E. Fibre-Related Dietary Patterns: Socioeconomic Barriers to Adequate Fibre Intake in Polish Adolescents. A Short Report. Nutrients 2017, 9, 590. [Google Scholar] [CrossRef] [Green Version]
- Atkins, J.L.; Ramsay, S.E.; Whincup, P.H.; Morris, R.W.; Lennon, L.T.; Wannamethee, S.G. Diet quality in older age: The influence of childhood and adult socio-economic circumstances. Br. J. Nutr. 2015, 113, 1441–1452. [Google Scholar] [CrossRef] [Green Version]
- Shahar, S.; Vanoh, D.; Ludin, A.F.M.; Singh, D.K.A.; Hamid, T.A. Factors associated with poor socioeconomic status among Malaysian older adults: An analysis according to urban and rural settings. BMC Public Health 2019, 19, 549. [Google Scholar] [CrossRef] [Green Version]
- Salehi, L.; Eftekhar, H.; Mohammad, K.; Tavafian, S.S.; Jazayery, A.; Montazeri, A. Consumption of fruit and vegetables among elderly people: A cross sectional study from Iran. Nutr. J. 2010, 9, 2. [Google Scholar] [CrossRef] [Green Version]
- Dean, W.R.; Sharkey, J.R. Rural and Urban Differences in the Associations between Characteristics of the Community Food Environment and Fruit and Vegetable Intake. J. Nutr. Educ. Behav. 2011, 43, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Possa, G.; De Castro, M.A.; Marchioni, D.M.L.; Fisberg, R.M.; Fisberg, M. Probability and amounts of yogurt intake are differently affected by sociodemographic, economic, and lifestyle factors in adults and the elderly—Results from a population-based study. Nutr. Res. 2015, 35, 700–706. [Google Scholar] [CrossRef] [Green Version]
- Deshmukh-Taskar, P.; Nicklas, T.A.; Yang, S.-J.; Berenson, G.S. Does Food Group Consumption Vary by Differences in Socioeconomic, Demographic, and Lifestyle Factors in Young Adults? The Bogalusa Heart Study. J. Am. Diet. Assoc. 2007, 107, 223–234. [Google Scholar] [CrossRef] [Green Version]
- Kapaj, A.; Deci, E. World Milk Production and Socio-Economic Factors Effecting Its Consumption. In Dairy in Human Health and Disease across the Lifespan; Watson, R.R., Robert Collier, J., Preedy, V.R., Eds.; Academic Press: Cambridge, MA, USA, 2017; pp. 107–115. [Google Scholar] [CrossRef]
- Central Statistical Office. Prices of Agricultural Products. Available online: http://stat.gov.pl/ceny_produktow_rolnych_w_pazdzierniku_2016_r.pdf.2016 (accessed on 29 March 2021).
- Van der Zanden, L.D.; van Kleef, E.; de Wijk, R.A.; van Trijp, H.C. Knowledge, perceptions and preferences of elderly regarding protein-enriched functional food. Appetite 2014, 80, 16–22. [Google Scholar] [CrossRef]
- Jeruszka-Bielak, M.; Kollajtis-Dolowy, A.; Santoro, A.; Ostan, R.; Berendsen, A.A.M.; Jennings, A.; Meunier, N.; Marseglia, A.; Caumon, E.; Gillings, R.; et al. Are Nutrition-Related Knowledge and Attitudes Reflected in Lifestyle and Health Among Elderly People? A Study Across Five European Countries. Front. Physiol. 2018, 9, 994. [Google Scholar] [CrossRef]
- Shatenstein, B.; Gauvin, L.; Keller, H.; Richard, L.; Gaudreau, P.; Giroux, F.; Gray-Donald, K.; Jabbour, M.; Morais, J.A.; Payette, H. Baseline determinants of global diet quality in older men and women from the NuAge cohort. J. Nutr. Health Aging 2013, 17, 419–425. [Google Scholar] [CrossRef]
- Sanchez, M.-A.; Armaingaud, D.; Messaoudi, Y.; Letty, A.; Mahmoudi, R.; Sanchez, S. Multiple factor analysis of eating patterns to detect groups at risk of malnutrition among home-dwelling older subjects in 2015. BMJ Open 2019, 9, e023548. [Google Scholar] [CrossRef] [Green Version]
- Södergren, M.; McNaughton, S.A.; Salmon, J.; Ball, K.; Crawford, D.A. Associations between fruit and vegetable intake, leisure-time physical activity, sitting time and self-rated health among older adults: Cross-sectional data from the WELL study. BMC Public Health 2012, 12, 551. [Google Scholar] [CrossRef] [Green Version]
- Oyebode, O.; Gordon-Dseagu, V.; Walker, A.; Mindell, J. Fruit and vegetable consumption and all-cause, cancer and CVD mortality: Analysis of Health Survey for England data. J. Epidemiol. Community Health 2014, 68, 856–862. [Google Scholar] [CrossRef]
- PREDIMED Investigators; Babio, N.; Becerra-Tomás, N.; Martínez-González, M.; Corella, D.; Estruch, R.; Ros, E.; Sayón-Orea, C.; Fitó, M.; Serra-Majem, L.; et al. Consumption of Yogurt, Low-Fat Milk, and Other Low-Fat Dairy Products Is Associated with Lower Risk of Metabolic Syndrome Incidence in an Elderly Mediterranean Population. J. Nutr. 2015, 145, 2308–2316. [Google Scholar] [CrossRef] [Green Version]
- Díaz-López, A.; Bulló, M.; Martínez-González, M.A.; Corella, D.; Estruch, R.; Fitó, M.; Gómez-Gracia, E.; Fiol, M.; De La Corte, F.J.G.; Ros, E.; et al. Dairy product consumption and risk of type 2 diabetes in an elderly Spanish Mediterranean population at high cardiovascular risk. Eur. J. Nutr. 2015, 55, 349–360. [Google Scholar] [CrossRef] [Green Version]
- Rozenberg, S.; Body, J.-J.; Bruyere, O.; Bergmann, P.; Brandi, M.L.; Cooper, C.; Devogelaer, J.-P.; Gielen, E.; Goemaere, S.; Kaufman, J.-M.; et al. Effects of Dairy Products Consumption on Health: Benefits and Beliefs—A Commentary from the Belgian Bone Club and the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases. Calcif. Tissue Int. 2015, 98, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Hess, J.M.; Jonnalagadda, S.S.; Slavin, J.L. Dairy Foods: Current Evidence of their Effects on Bone, Cardiometabolic, Cognitive, and Digestive Health. Compr. Rev. Food Sci. Food Saf. 2015, 15, 251–268. [Google Scholar] [CrossRef]
- Bimbo, F.; Bonanno, A.; Nocella, G.; Viscecchia, R.; Nardone, G.; De Devitiis, B.; Carlucci, D. Consumers’ acceptance and preferences for nutrition-modified and functional dairy products: A systematic review. Appetite 2017, 113, 141–154. [Google Scholar] [CrossRef] [Green Version]
- National Center for Nutrition Education Recommendations for Healthy Eating. 2020. Available online: https://ncez.pl/abc-zywienia-/zasady-zdrowego-zywienia/talerz-zdrowego-zywienia (accessed on 21 May 2021).
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Chen, J.; Fewtrell, M.; Kennedy, G.; Naska, A.; Riediger, K.; Roos, N.; Sanders, T.; Tuohy, K.M.; Valtueña-Martínez, S. Nutrition challenges ahead. EFSA J. 2016, 14, e00504. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Components | Scoring (Points) |
|---|---|
| Place of residence: | |
| city (>100,000 inhabitants) | 0 |
| town (<100,000 inhabitants) | 1 |
| village | 2 |
| Self-reported economic situation of household: | |
| I live very well—I have enough resources for everything, and I put off savings | 0 |
| I live well—I have enough resources for everything, but I don’t put off savings | 1 |
| I live thriftily—I have enough resources for everything | 2 |
| I live very thriftily—I have enough resources only for basic needs (food/clothing/housing fees) | 3 |
| I live poorly—I don’t have enough resources even for basic needs (food/clothing/housing fees) | 4 |
| Components | Scoring (Points) |
|---|---|
| Difficulties with self-feeding (self-fed with some difficulty or unable to eat without assistance) | |
| no | 0 |
| yes | 1 |
| Decrease in food intake in the last 3 months (due to loss of appetite, digestive problems, chewing or swallowing difficulties) | |
| no | 0 |
| yes | 1 |
| Feeling the taste of food in comparison with other people of the same age | |
| better | 0 |
| as good | 1 |
| weaker | 2 |
| Appetite in comparison with other people of the same age | |
| better | 0 |
| as good | 1 |
| weaker | 2 |
| Feeling satiety after eating almost the whole meal | |
| yes | 0 |
| no | 1 |
| Components | Cut-Offs for Scoring (Points) | |
|---|---|---|
| 0 | 1 | |
| Lives dependently (i.e., in nursing home or hospital) | no | yes |
| Limited mobility (i.e., able to get out of bed/chair but does not go out vs. goes out) | no | yes |
| Psychological stress or acute disease in the last 3 months | no | yes |
| Neuropsychological problems | no | yes |
| Taking more than 3 prescription medications/day | no | yes |
| Pressure sores or skin ulcers | no | yes |
| Weight loss greater than 3 kg in the last 3 months | no | yes |
| Self-reported health status in comparison with other people of the same age (i.e., weaker/does not know vs. as good/better) | no | yes |
| Self-reported nutritional status (malnourished/does not know vs. good) | no | yes |
| BMI (kg/m2) | 18.5–29.9 | <18.5 or ≥30 |
| Waist circumference (cm) | <88 | ≥88 |
| Strength of the right arm muscles (kg) | >20 | ≤20 |
| Strength of the left arm muscles (kg) | >20 | ≤20 |
| Variables | Sample Percentage (%) or Mean ± SD |
|---|---|
| Sample size | 313 |
| Age, years | 69.5 ± 5.6 |
| 60–69 | 63 |
| 70–89 | 37 |
| BMI (kg/m2) | 29.8 ± 4.8 |
| Waist circumference (cm) | 94.0 ± 11.2 |
| Strength of the right arm muscles (kg) | 22.5 ± 6.0 |
| Strength of the left arm muscles (kg) | 20.5 ± 5.5 |
| Socioeconomic Status Index (SESI) a, points | 2.1 ± 1.3 |
| higher, 0–1 | 27 |
| average, 2 | 42 |
| lower, 3–6 | 31 |
| Eating-related Limitations Score (E-LS) b, points | 2.5 ± 1.4 |
| lower, ≤2 | 57 |
| higher, 3–7 | 43 |
| Health-related Limitations Score (H-LS) c, points | 3.6 ± 2.0 |
| lower, <4 | 49 |
| higher, 4–13 | 51 |
| Consumption of: | |
| Fruit/vegetables, servings/day | |
| lower, <2 | 15 |
| higher, ≥2 | 85 |
| Dairy, servings/day | |
| lower, <1 | 18 |
| higher, ≥1 | 82 |
| Meat/poultry/fish, servings/day | |
| lower, <1 | 23 |
| higher, ≥1 | 77 |
| Legumes/eggs, servings/week | |
| lower, <2 | 34 |
| higher, ≥2 | 66 |
| Water and beverages industrially unsweetened d, cups/day | |
| lower, <6 | 53 |
| higher, ≥6 | 47 |
| Variables | Consumption of | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fruit/Vegetables (Servings/Day) | Dairy (Servings/Day) | Meat/Poultry/Fish (Servings/Day) | Legumes/Eggs (Servings/Week) | Water and Beverages Industrially Unsweetened d (Cups/Day) | |||||||||||
| <2 | ≥2 | p | <1 | ≥1 | p | <1 | ≥1 | p | <2 | ≥2 | p | <6 | ≥6 | p | |
| Sample size | 47/34 # | 266/230 # | 57/41 # | 256/223 # | 72/60 # | 241/204 # | 105/90 # | 208/174 # | 167/134 # | 146/130 # | |||||
| Socioeconomic Status Index (SESI) a, points | 2.5 ± 1.1 | 2.0 ± 1.3 | <0.01 | 2.6 ± 1.4 | 2.0 ± 1.2 | <0.01 | 2.1 ± 1.2 | 2.1 ± 1.3 | ns | 2.2 ± 1.2 | 2.1 ± 1.3 | ns | 2.2 ± 1.4 | 2.1 ± 1.2 | ns |
| higher, 0–1 | 13 | 30 | 16 | 30 | 26 | 28 | 23 | 30 | 29 | 26 | |||||
| average, 2 | 40 | 42 | <0.05 | 40 | 42 | <0.05 | 44 | 41 | ns | 40 | 42 | ns | 38 | 46 | ns |
| lower, 3–6 | 47 | 28 | 44 | 28 | 29 | 32 | 37 | 28 | 34 | 28 | |||||
| Eating-related Limitations Score (E-LS) b, points lower, ≤2 higher, 3–7 | 3.1 ± 1.4 | 2.4 ± 1.4 | <0.01 | 2.8 ± 1.4 | 2.4 ± 1.4 | <0.05 | 2.5 ± 1.4 | 2.5 ± 1.4 | ns | 2.7 ± 1.3 | 2.4 ± 1.4 | <0.05 | 2.7 ± 1.4 | 2.2 ± 1.4 | <0.001 |
| 47 | 59 | ns | 44 | 60 | <0.05 | 57 | 57 | ns | 50 | 61 | ns | 50 | 65 | <0.01 | |
| 53 | 41 | 56 | 40 | 43 | 43 | 50 | 39 | 50 | 35 | ||||||
| Health-related Limitations Score (H-LS) c, points lower, <4 higher, 4–13 | 4.6 ± 2.1 | 3.5 ± 2.0 | <0.01 | 4.6 ± 2.4 | 3.4 ± 1.9 | <0.01 | 3.5 ± 2.0 | 3.7 ± 2.1 | ns | 3.9 ± 2.2 | 3.5 ± 2.0 | ns | 3.9 ± 2.1 | 3.4 ± 2.0 | <0.05 |
| 35 | 51 | ns | 34 | 52 | <0.05 | 50 | 49 | ns | 46 | 51 | ns | 45 | 54 | ns | |
| 65 | 49 | 66 | 48 | 50 | 51 | 54 | 49 | 55 | 46 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamulka, J.; Frackiewicz, J.; Stasiewicz, B.; Jeruszka-Bielak, M.; Piotrowska, A.; Leszczynska, T.; Niedzwiedzka, E.; Brzozowska, A.; Wadolowska, L. Socioeconomic, Eating- and Health-Related Limitations of Food Consumption among Polish Women 60+ Years: The ‘ABC of Healthy Eating’ Project. Nutrients 2022, 14, 51. https://doi.org/10.3390/nu14010051
Hamulka J, Frackiewicz J, Stasiewicz B, Jeruszka-Bielak M, Piotrowska A, Leszczynska T, Niedzwiedzka E, Brzozowska A, Wadolowska L. Socioeconomic, Eating- and Health-Related Limitations of Food Consumption among Polish Women 60+ Years: The ‘ABC of Healthy Eating’ Project. Nutrients. 2022; 14(1):51. https://doi.org/10.3390/nu14010051
Chicago/Turabian StyleHamulka, Jadwiga, Joanna Frackiewicz, Beata Stasiewicz, Marta Jeruszka-Bielak, Anna Piotrowska, Teresa Leszczynska, Ewa Niedzwiedzka, Anna Brzozowska, and Lidia Wadolowska. 2022. "Socioeconomic, Eating- and Health-Related Limitations of Food Consumption among Polish Women 60+ Years: The ‘ABC of Healthy Eating’ Project" Nutrients 14, no. 1: 51. https://doi.org/10.3390/nu14010051