
The Development of a Life-Cycle-Based Sustainability Index That Incorporates Patient-Centredness for Assessing and Reporting the Sustainability of Healthcare Buildings in Saudi Arabia

Abstract
:1. Introduction
2. Measuring Sustainability in Healthcare Buildings
3. Measuring Patient-Centred Care in Healthcare Buildings
4. Methodology
5. Research Methods
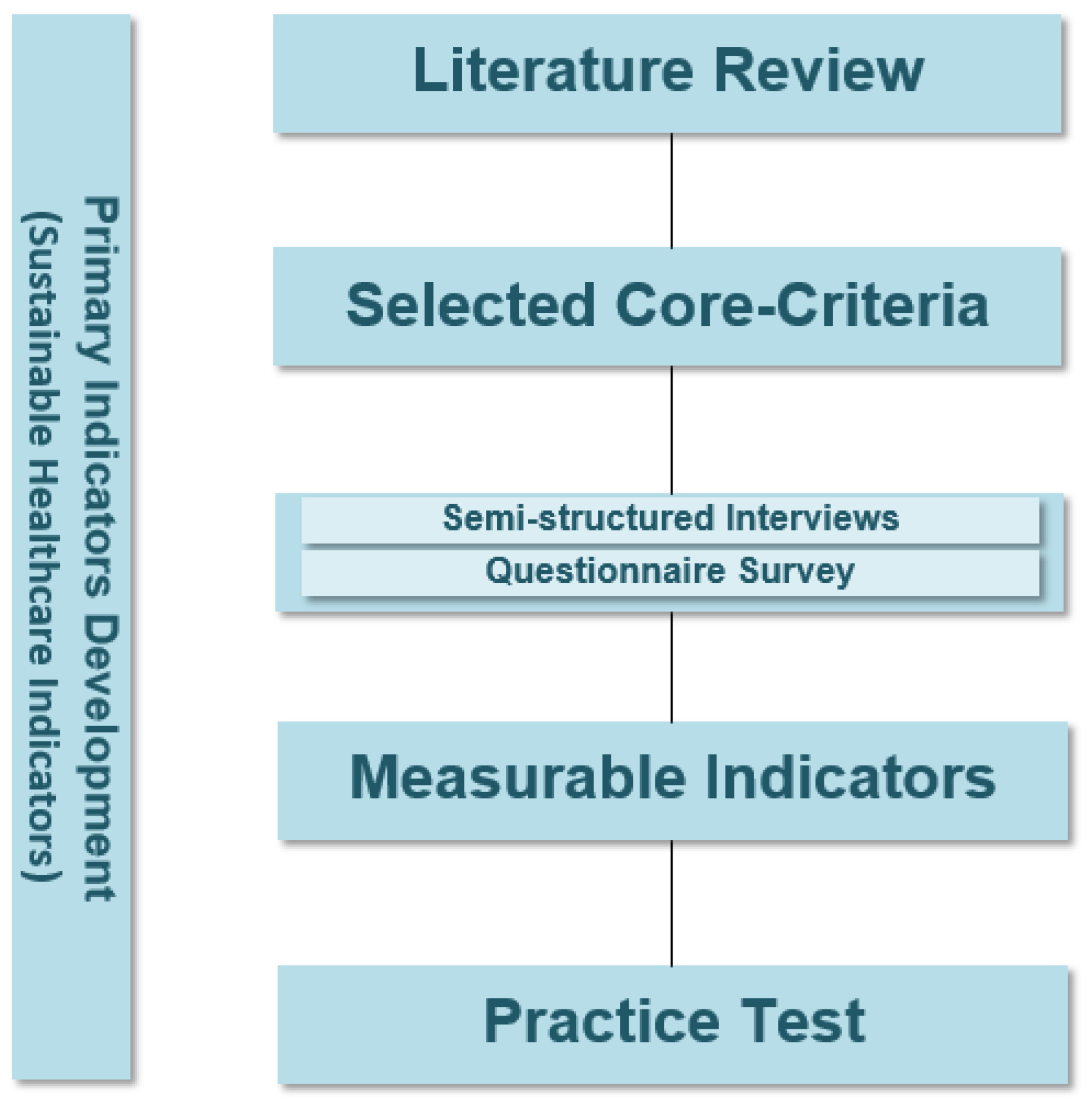
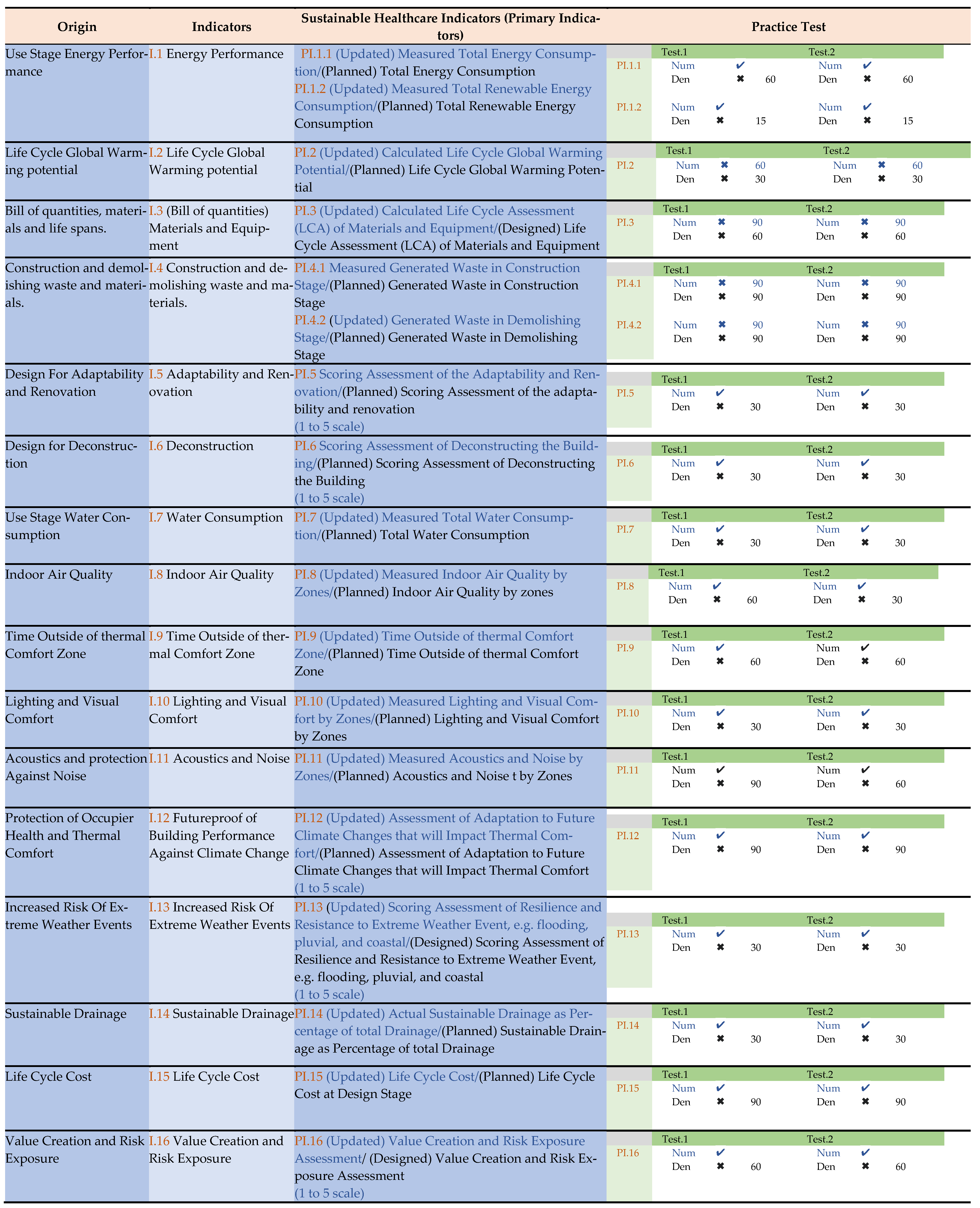
5.1. Development of Sustainable Healthcare Indicators (Primary Indicators)
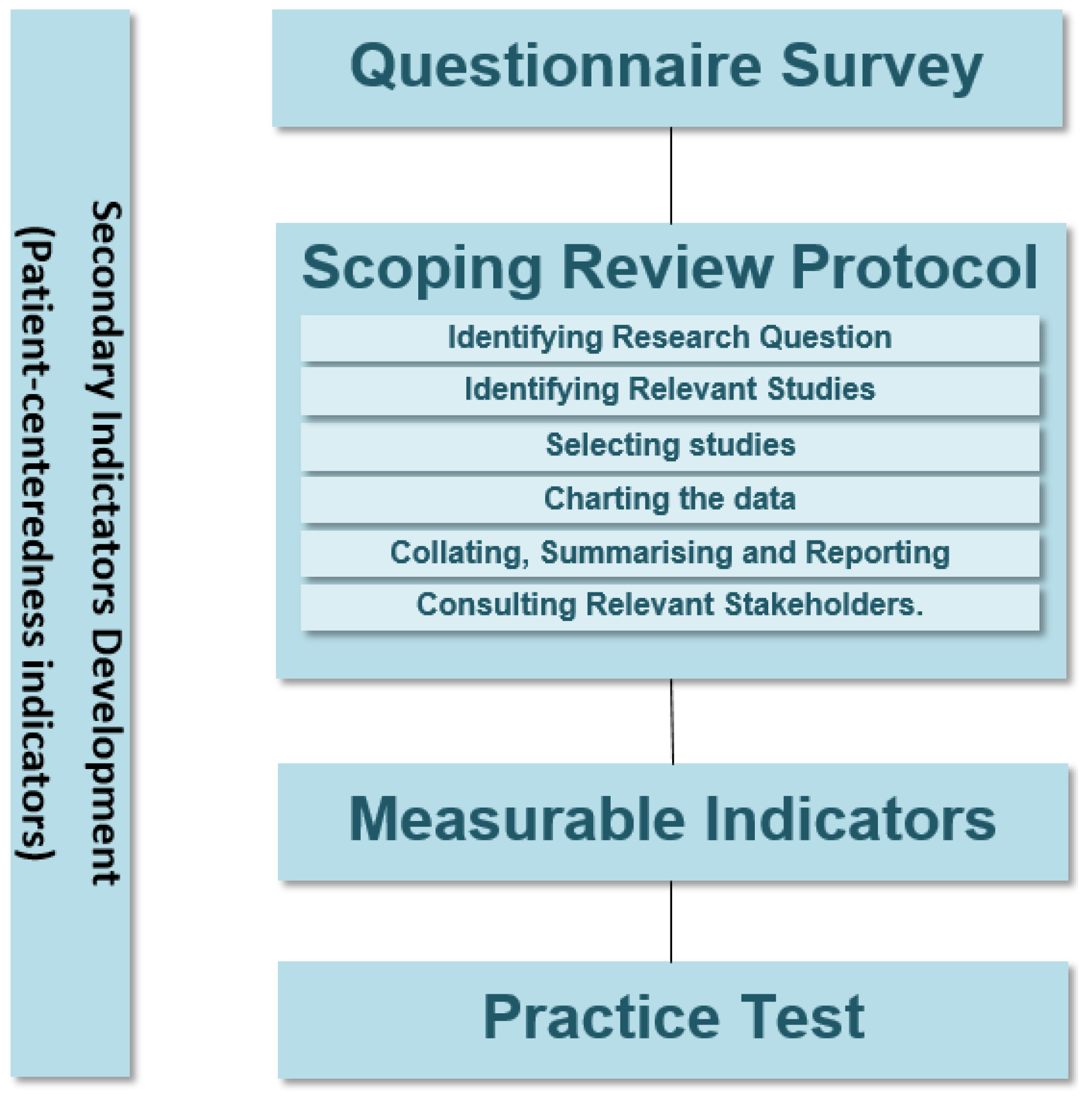
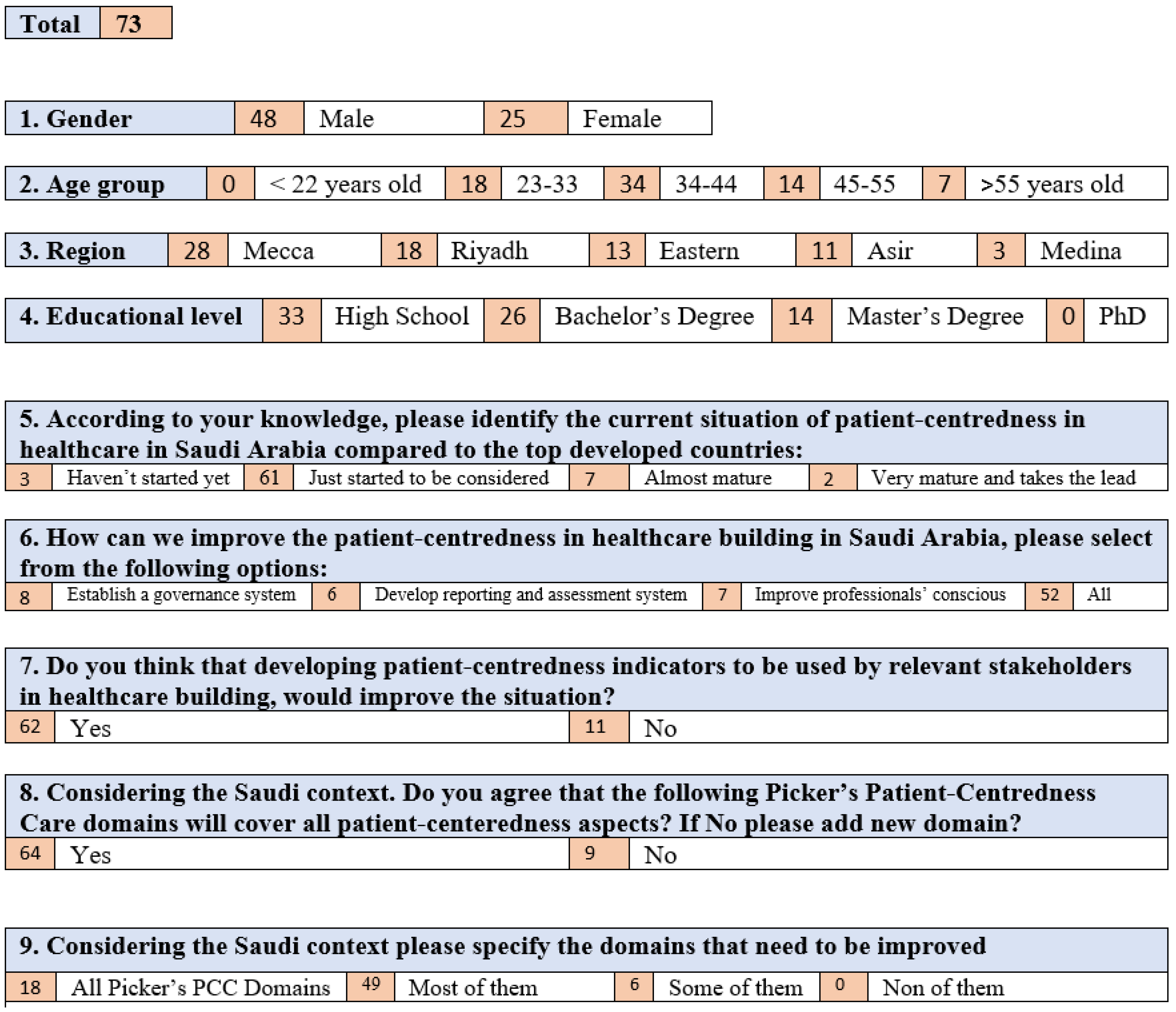
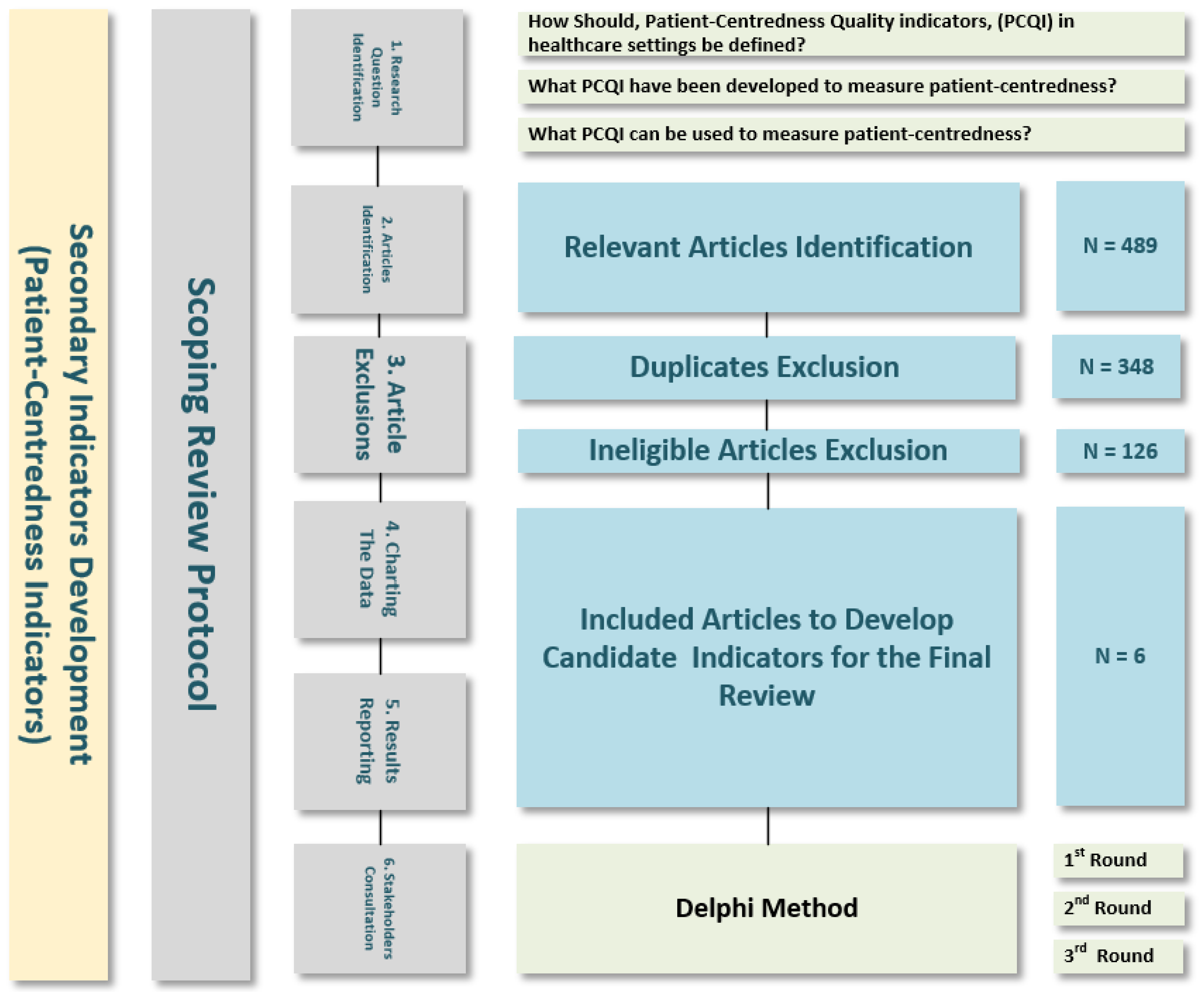
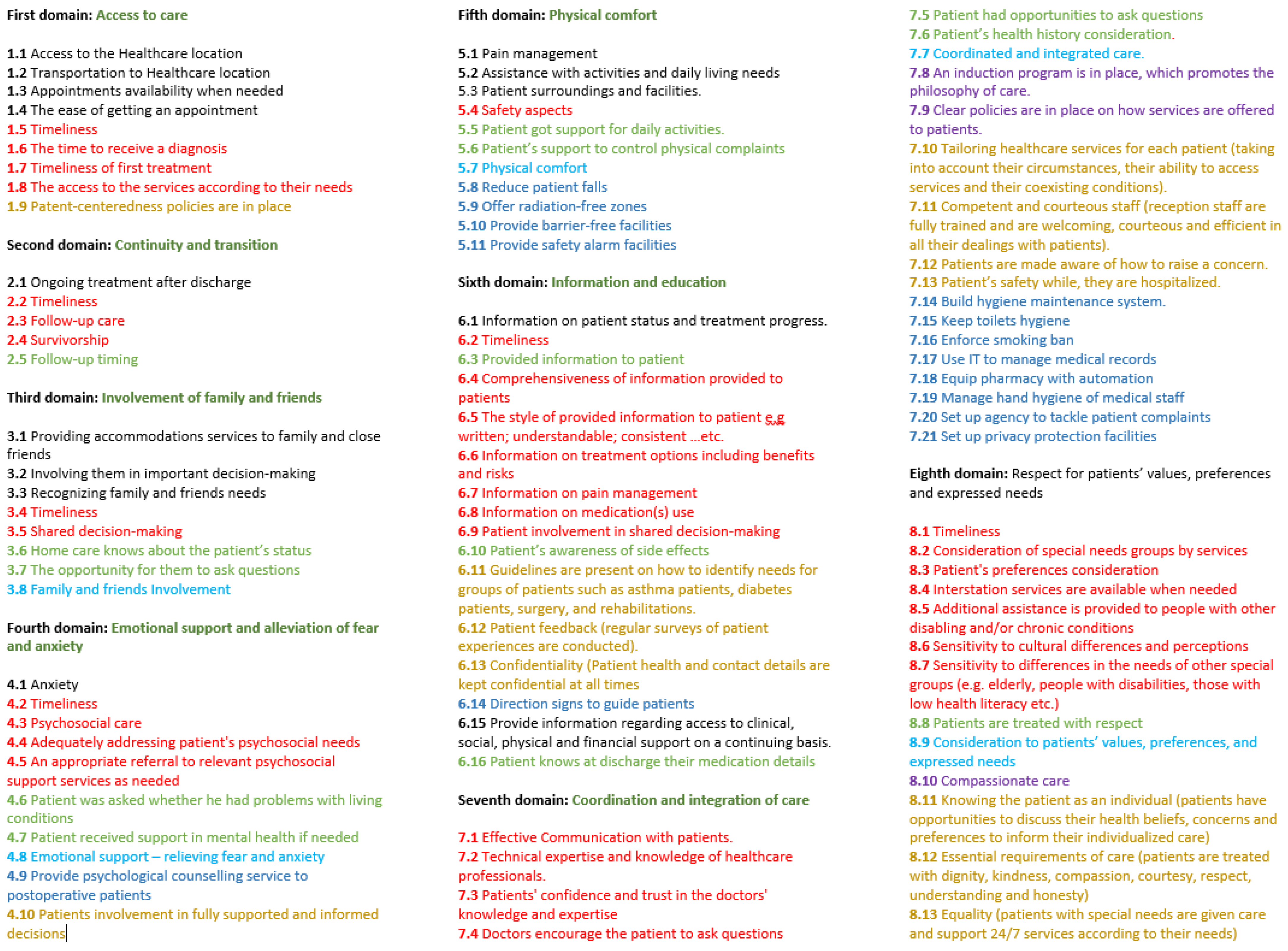
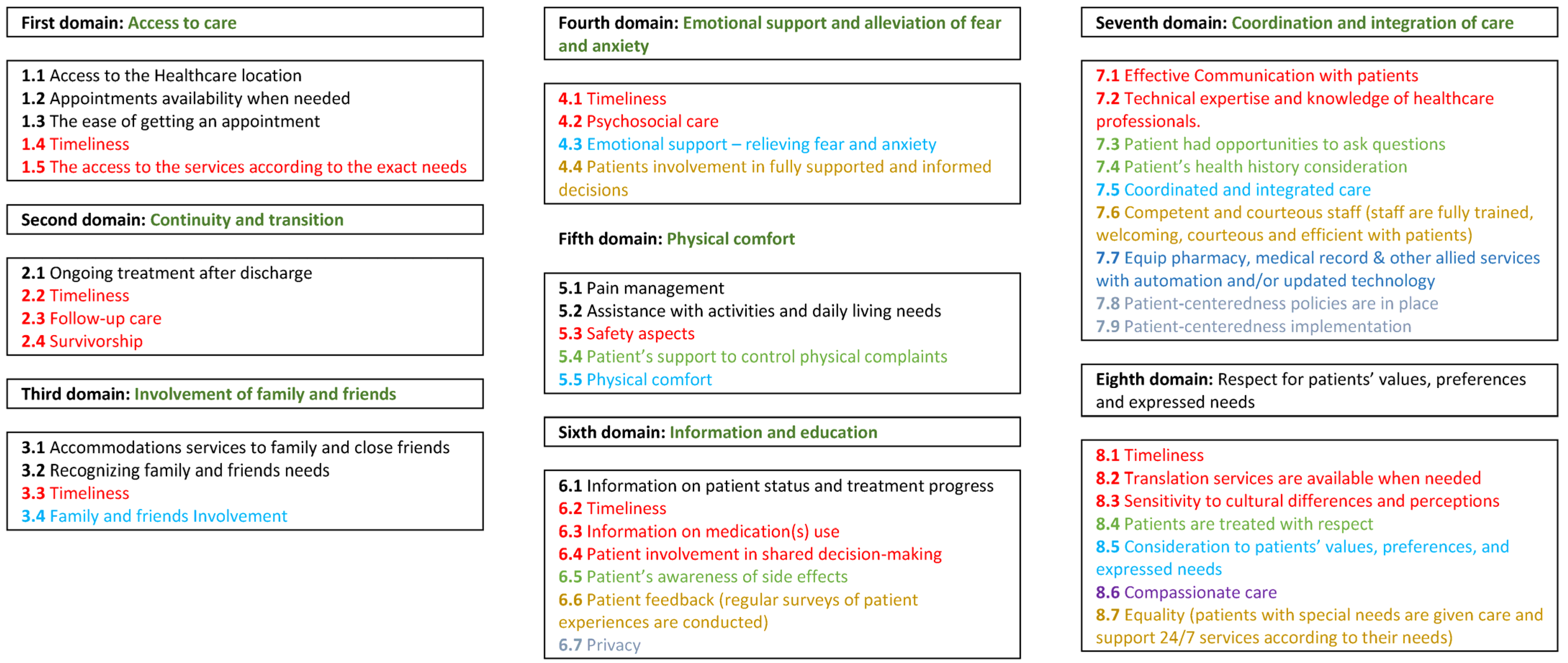
5.2. Development of Patient-Centredness Indicators (Secondary Indicators)
5.3. Practice Test
6. The Development of the Indicators and Results Interpretation
7. Practice Test
8. Research Contribution
9. Research Limitations
10. Further Research
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gilson, L.; World Health Organization. Health Policy and System Research: A Methodology Reader: The Abridged Version; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Hensher, M. Incorporating environmental impacts into the economic evaluation of health care systems: Perspectives from ecological economics. Resour. Conserv. Recycl. 2020, 154, 104623. [Google Scholar] [CrossRef]
- World Health Organization. Special Report on Climate Change and Health, the Health Argument for Climate Action; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- COP26 Health Programme. Available online: https://cdn.who.int/media/docs/default-source/climate-change/cop26-health-programme.pdf (accessed on 22 February 2023).
- Balbus, J. Observations from COP27: Health Care Is Becoming a Bigger Part of the Climate Change Solution. Environ. Health Perspect. 2022, 130, 121001. [Google Scholar] [CrossRef] [PubMed]
- Prüss, A.; Emmanuel, J.; Stringer, R.; Pieper, U.; Townend, W.; Wilburn, S.; Chantier, Y.; World Health Organization. Safe Management of Wastes from Health-care Activities; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Lenzen, M.; Malik, A.; Li, M.; Fry, J.; Weisz, H.; Pichler, P.-P.; Chaves, L.S.M.; Capon, A.; Pencheon, D. The environmental footprint of health care: A global assessment. Lancet Planet. Health 2020, 4, e271–e279. [Google Scholar] [CrossRef] [PubMed]
- Karliner, J.; Slotterback, S.; Boyd, R.; Ashby, B.; Steele, K.; Wang, J. Health care’s climate footprint: The health sector contribution and opportunities for action. Eur. J. Public Health 2020, 30, ckaa165.843. [Google Scholar] [CrossRef]
- Stevanovic, M.; Allacker, K.; Vermeulen, S. Development of an approach to assess the life cycle environmental impacts and costs of general hospitals through the analysis of a Belgian case. Sustainability 2019, 11, 856. [Google Scholar] [CrossRef] [Green Version]
- NHS England. Delivering a ‘Net Zero’ National Health Service; NHS England: London, UK, 2020. [Google Scholar]
- Hu, H.; Cohen, G.; Sharma, B.; Yin, H.; McConnell, R. Sustainability in Health Care. Annu. Rev. Environ. Resour. 2022, 47, 173–196. [Google Scholar] [CrossRef]
- Alasiri, A.A.; Mohammed, V. Healthcare Transformation in Saudi Arabia: An Overview Since the Launch of Vision 2030. Health Serv. Insights 2022, 15, 11786329221121214. [Google Scholar] [CrossRef]
- Saudi Arabia MoH- Health Sector: Transformation Strategy. Available online: https://www.moh.gov.sa/en/Ministry/vro/Documents/Healthcare-Transformation-Strategy.pdf (accessed on 22 February 2023).
- World Economic Forum. Sustainable Health Systems—Visions, Strategies, Critical Uncertainties and Scenarios; A Report from the World Economic Forum Prepared in Collaboration with McKinsey & Company; World Economic Forum: Cologny, Switzerland, 2013. [Google Scholar]
- Hensher, M.; McGain, F. Health Care Sustainability Metrics: Building A Safer, Low-Carbon Health System: Commentary examines how to build a safer, low-carbon health system. Health Affairs 2020, 39, 2080–2087. [Google Scholar] [CrossRef]
- Chui, K.T.; Alhalabi, W.; Pang, S.S.H.; Pablos, P.O.d.; Liu, R.W.; Zhao, M. Disease diagnosis in smart healthcare: Innovation, technologies and applications. Sustainability 2017, 9, 2309. [Google Scholar] [CrossRef] [Green Version]
- Khosravi, F.; Izbirak, G.; Adewale Adesina, K. An exponentially distributed stochastic model for sustainability measurement of a healthcare system. Sustainability 2019, 11, 1285. [Google Scholar] [CrossRef] [Green Version]
- Buffoli, M.; Capolongo, S.; di Noia, M.; Gherardi, G.; Gola, M. Healthcare sustainability evaluation systems. In Improving Sustainability during Hospital Design and Operation; Springer: Cham, Switzerland, 2015; pp. 23–29. [Google Scholar]
- Kajikawa, Y.; Inoue, T.; Goh, T.N. Analysis of building environment assessment frameworks and their implications for sustainability indicators. Sustain. Sci. 2011, 6, 233–246. [Google Scholar] [CrossRef]
- Alshamrani, O. Evaluation of School Buildings Using Sustainability Measures and Life-Cycle Costing Technique. Ph.D. Thesis, Concordia University, Montreal, QC, Canada, 2012. [Google Scholar]
- Guerrero, J.I.; Miró-Amarante, G.; Martín, A. Decision support system in health care building design based on case-based reasoning and reinforcement learning. Expert Syst. Appl. 2022, 187, 116037. [Google Scholar] [CrossRef]
- Castro, M.d.F.M.d.A.; Mateus, R.; Bragança, L. Proposal for a Healthcare Building Sustainability Assessment (HBSA) Method. 2014. Available online: http://wsb14barcelona.org/programme/pdf_poster/P-143.pdf (accessed on 22 February 2023).
- Shepley, M.M.; Baum, M.; Ginsberg, R.; Rostenberg, B. Eco-effective design and evidence-based design: Perceived synergy and conflict. Herd 2009, 2, 56–70. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.d.F.; Mateus, R.; Bragança, L. Healthcare Building Sustainability Assessment tool—Sustainable Effective Design criteria in the Portuguese context. Environ. Impact Assess. Rev. 2017, 67, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Baum, M.S.M.; Rostenberg, B.; Ginsberg, R. Eco-Effective Design and Evidence-Based Design: Removing Barriers to Integration; Final Report for AIA Board Knowledge Committee; The American Institute of Architects: Washington, DC, USA, 2009. [Google Scholar]
- Mortimer, F.; Isherwood, J.; Wilkinson, A.; Vaux, E. Sustainability in quality improvement: Redefining value. Future Healthc. J. 2018, 5, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Mehra, R.; Sharma, M.K. Measures of Sustainability in Healthcare. Sustain. Anal. Model. 2021, 1, 100001. [Google Scholar] [CrossRef]
- Renedo, A.; Marston, C. Developing patient-centred care: An ethnographic study of patient perceptions and influence on quality improvement. BMC Health Serv. Res. 2015, 15, 122. [Google Scholar] [CrossRef] [Green Version]
- Marchi, L.; Antonini, E.; Politi, S. Green building rating systems (GBRSs). Encyclopedia 2021, 1, 998–1009. [Google Scholar] [CrossRef]
- Ding, G.K. Sustainable construction—The role of environmental assessment tools. J. Environ. Manag. 2008, 86, 451–464. [Google Scholar] [CrossRef] [Green Version]
- AlJaberi, O.; Hussain, M.; Drake, P. A framework for measuring sustainability in healthcare systems. Int. J. Healthc. Manag. 2017, 13, 1–10. [Google Scholar] [CrossRef]
- Hussain, M.; Khan, M.; Al-Aomar, R. A framework for supply chain sustainability in service industry with Confirmatory Factor Analysis. Renew. Sustain. Energy Rev. 2016, 55, 1301–1312. [Google Scholar] [CrossRef]
- Stylos, N.; Vassiliadis, C. Differences in Sustainable Management Between Four- and Five-Star Hotels Regarding the Perceptions of Three-Pillar-Sustainability. J. Hosp. Mark. Manag. 2015, 24, 791–825. [Google Scholar] [CrossRef] [Green Version]
- Saudi Vision 2030. Saudi Arabia. Available online: https://www.vision2030.gov.sa/media/rc0b5oy1/saudi_vision203.pdf (accessed on 22 February 2023).
- Directorate-General for Environment (European Commission). Level(s), What’s in It for Cities? Publications Office of the European Union: Luxembourg, 2022. [Google Scholar]
- Directorate-General for Environment (European Commission). Level(s) and the New European Bauhaus; Publications Office of the European Union: Luxembourg, 2022. [Google Scholar]
- Russo, G.; Moretta Tartaglione, A.; Cavacece, Y. Empowering Patients to Co-Create a Sustainable Healthcare Value. Sustainability 2019, 11, 1315. [Google Scholar] [CrossRef] [Green Version]
- WHO Global Strategy on People-Centred and Integrated Health Services. Available online: https://apps.who.int/iris/bitstream/handle/10665/155002/WHO_HIS_SDS_2015.6_eng.pdf?sequence=1&isAllowed=y (accessed on 22 February 2023).
- Santana, M.J.; Ahmed, S.; Lorenzetti, D.; Jolley, R.J.; Manalili, K.; Zelinsky, S.; Quan, H.; Lu, M. Measuring patient-centred system performance: A scoping review of patient-centred care quality indicators. BMJ Open 2019, 9, e023596. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.A. Patient Experience: A return to purpose. Patient Exp. J. 2017, 4, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Handley, M.D.; Ingrid, M. Measuring patient-centered care for specific populations: A necessity for improvement. Patient Exp. J. 2020, 7, 10–12. [Google Scholar] [CrossRef]
- Modigh, A.; Sampaio, F.; Moberg, L.; Fredriksson, M. The impact of patient and public involvement in health research versus healthcare: A scoping review of reviews. Health Policy 2021, 125, 1208–1221. [Google Scholar] [CrossRef]
- Arif, M.; Bendi, D.; Toma-Sabbagh, T.; Sutrisna, M. Construction waste management in India: An exploratory study. Constr. Innov. 2012, 12, 133–155. [Google Scholar] [CrossRef]
- Directorate-General for Environment (European Commission). Level(s), A Common Language for Building Assessment; Office des Publications de l’Union Européenne: Luxembourg, 2021. [Google Scholar]
- Jamoussi, B.; Abu-Rizaiza, A.; AL-Haij, A. Sustainable Building Standards, Codes and Certification Systems: The Status Quo and Future Directions in Saudi Arabia. Sustainability 2022, 14, 10314. [Google Scholar] [CrossRef]
- Sánchez Cordero, A.; Gómez Melgar, S.; Andújar Márquez, J.M. Green building rating systems and the new framework level (s): A critical review of sustainability certification within Europe. Energies 2019, 13, 66. [Google Scholar] [CrossRef] [Green Version]
- European Commission. LEVEL(S) Taking Action on the Total Impact of the Construction Sector; Publications Office of the European Union: Luxembourg, 2019. [Google Scholar]
- Mes, M.A.; Chan, A.H.Y.; Wileman, V.; Katzer, C.B.; Goodbourn, M.; Towndrow, S.; Taylor, S.J.C.; Horne, R. Patient involvement in questionnaire design: Tackling response error and burden. J. Pharm. Policy Pract. 2019, 12, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijma, A.J.; Bletterman, A.N.; Clark, J.R.; Vervoort, S.C.J.M.; Beetsma, A.; Keizer, D.; Nijs, J.; Van Wilgen, C.P. Patient-centeredness in physiotherapy: What does it entail? A systematic review of qualitative studies. Physiother. Theory Pract. 2017, 33, 825–840. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.E.; Sansoni, J.; Morris, D.; Thompson, C. A Delphi study to develop indicators of cancer patient experience for quality improvement. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2018, 26, 129–138. [Google Scholar] [CrossRef]
- Ouwens, M.; Hermens, R.; Hulscher, M.; Vonk-Okhuijsen, S.; Tjan-Heijnen, V.; Termeer, A.; Marres, H.; Wollersheim, H.; Grol, R. Development of indicators for patient-centred cancer care. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2009, 18, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Tzelepis, F.; Sanson-Fisher, R.W.; Zucca, A.C.; Fradgley, E.A. Measuring the quality of patient-centered care: Why patient-reported measures are critical to reliable assessment. Patient Prefer. Adherence 2015, 9, 831–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patient-Centred Healthcare Indicators Review; International Alliance of Patients Organization: London, UK, 2012.
- Zhou, H.; Bai, G.; Gao, J.; Zhou, Y.; Ma, E.; Hu, L.; Hu, G.; Zhao, P.; Jiang, F.; Luo, L.; et al. The development of indicator measure for monitoring the quality of patient-centered care in China’s tertiary hospitals. PLoS ONE 2018, 13, e0205489. [Google Scholar] [CrossRef]
- Sehulster, L.M.; Chinn, R.Y.W.; Arduino, M.J.; Carpenter, J.; Donlan, R.; Ashford, D.; Besser, R.; Fields, B.; McNeil, M.M.; Whitney, C.; et al. Guidelines for Environmental Infection Control in Health-Care Facilities; Recommendations from CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC); American Society for Healthcare Engineering/American Hospital Association: Chicago IL, USA, 2004. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Core Criteria | Associated Objectives |
|---|---|
| Use Stage Energy Performance | Greenhouse Gas Emissions during Building’s Life Cycle |
| Life Cycle Global Warming Potential | Greenhouse Gas Emissions during Building’s Life Cycle |
| Bill of Quantities, Materials and Life Spans | Resource Efficient and Circular Material Life Cycles |
| Construction and Demolishing Waste and Materials | Resource Efficient and Circular Material Life Cycles |
| Design For Adaptability and Renovation | Resource Efficient and Circular Material Life Cycles |
| Design for Deconstruction | Resource Efficient and Circular Material Life Cycles |
| Use Stage Water Consumption | Efficient Use of Water Resources |
| Indoor Air Quality | Healthy and Comfortable Spaces |
| Time Outside of thermal Comfort Zone | Healthy and Comfortable Spaces |
| Lighting and Visual Comfort | Healthy and Comfortable Spaces |
| Acoustics and Protection Against Noise | Healthy and Comfortable Spaces |
| Protection of Occupier Health and Thermal Comfort | Adaptation and Resilience to Climate Change |
| Increased Risk Of Extreme Weather Events | Adaptation and Resilience to Climate Change |
| Sustainable Drainage | Adaptation and Resilience to Climate Change |
| Life Cycle Cost | Optimised Life Cycle Cost and Value |
| Value Creation and Risk Exposure | Optimised Life Cycle Cost and Value |
| Origin | Indicators | Sustainable Healthcare Indicators (Primary Indicators) |
|---|---|---|
| Use Stage Energy Performance | Energy Performance | (Updated) Measured Total Energy Consumption/(Planned) Total Energy Consumption (Updated) Measured Total Renewable Energy Consumption/(Designed) Total Renewable Energy Consumption |
| Life Cycle (LC) Global Warming Potential | Life Cycle Global Warming Potential | (Updated) Life Cycle (LC) Global Warming Potential/(Planned) Life Cycle Global Warming Potential |
| Bill of Quantities, Materials and Life Spans | Bill of Quantities, Materials and Equipment | (Updated) Calculated Life Cycle Assessment (LCA) of Materials and Equipment/(Planned) Life Cycle Assessment (LCA) of Materials and Equipment |
| Construction and Demolishing Waste and Materials | Construction and Demolishing Waste and materials | Measured Generated Waste in Construction Stage/(Planned) Generated Waste in Construction Stage Generated Waste in Demolishing Stage/(Planned) Generated Waste in Demolishing Stage |
| Design For Adaptability and Renovation | Adaptability and Renovation | (Updated) Scoring Assessment of the adaptability and renovation for the whole building/(Planned) Scoring Assessment of the adaptability and renovation for the whole building (1 to 5 scale) |
| Design for Deconstruction | Deconstruction | (Updated) Scoring Assessment of Deconstructing the Building/(Planned) Scoring Assessment of Deconstructing the Building (1 to 5 scale) |
| Use Stage Water Consumption | Water Consumption | (Updated) Measured Total Water Consumption/(Planned) Total Water Consumption |
| Indoor Air Quality | Indoor Air Quality | (Updated) Measured Indoor Air Quality by Zones/(Planned) Indoor Air Quality by Zones |
| Time Outside of Thermal Comfort Zone | Time Outside of thermal Comfort Zone | (Updated) Measured Time Outside of thermal Comfort Zone/(Designed) Time Outside of Thermal Comfort Zone |
| Lighting and Visual Comfort | Lighting and Visual Comfort | (Updated) Measured Lighting and Visual Comfort by Zones/(Planned) Lighting and Visual Comfort Assessment by Zones |
| Acoustics and Protection Against Noise | Acoustics and Noise | (Updated) Measured Acoustics and Noise by Zones/(Planned) Acoustics and Noise Assessment by Zones |
| Protection of Occupier Health and Thermal Comfort | Futureproof of Building Performance Against Climate Change | (Updated) Scoring Assessment of Adaptation to Future Climate Change that will Impact Thermal Comfort/(Planned Scoring Assessment of Adaptation to Future Climate Change that will Impact Thermal Comfort (1 to 5 scale) |
| Increased Risk Of Extreme Weather Events | Increased Risk Of Extreme Weather Events | (Updated) Scoring Assessment of resilience and Resistance to Extreme Weather Event, e.g., flooding, pluvial, and coastal/(Planned) Scoring Assessment of resilience and Resistance to Extreme Weather Event, e.g., flooding, pluvial, and coastal (1 to 5 scale) |
| Sustainable Drainage | Sustainable Drainage | (Updated) Actual Sustainable Drainage as Percentage of total Drainage System/(Planned) Sustainable Drainage as Percentage of total Drainage System |
| Life Cycle Cost | Life Cycle Cost | (Updated) Life Cycle Cost/(Planned) Life Cycle Cost at Design Stage |
| Value Creation and Risk Exposure | Value Creation and Risk Exposure | (Updated) Value Creation and Risk Exposure Assessment/(Planned) Value Creation and Risk Exposure Assessment at Design Stage (1 to 5 scale) |
| Participants | Experience (Years) | Title | Academic Qualification |
|---|---|---|---|
| Participant 1 | 25 | General Manager/Contractor | Master’s Degree |
| Participant 2 | 20 | Executive Manager/Contractor | Master’s Degree |
| Participant 3 | 28 | Managing Director/Consultant | Bachelor’s Degree |
| Participant 4 | 6 | HSE Executive/Governmental Authority | Bachelor’s Degree |
| Participant 5 | 10 | Senior Facilities Engineer | Bachelor’s Degree |
| Participant 6 | 27 | HSE Consultant/Consultant | Bachelor’s Degree |
| Participant 7 | 5 | Graduate Research Assistant/Researcher | PhD Candidate |
| Participant 8 | 12 | Director/Contractor | Bachelor’s Degree |
| Participant 9 | 11 | Senior Engineer/Designer | Bachelor’s Degree |
| Participant 10 | 20 | Business Manager/Consultant | Bachelor’s Degree |
| Participant 11 | 18 | Executive Officer/Consultant | Bachelor’s Degree |
| Participant 12 | 34 | Directors/Contractor | Bachelor’s Degree |
| Participant 13 | 16 | Executive Officer/Consultant | Bachelor’s Degree |
| Participant 14 | 15 | Dept. Head of Tech Services/Designer | Bachelor’s Degree |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhaij, A.; Jamoussi, B.; Abu-Rizaiza, A. The Development of a Life-Cycle-Based Sustainability Index That Incorporates Patient-Centredness for Assessing and Reporting the Sustainability of Healthcare Buildings in Saudi Arabia. Sustainability 2023, 15, 5784. https://doi.org/10.3390/su15075784
Alhaij A, Jamoussi B, Abu-Rizaiza A. The Development of a Life-Cycle-Based Sustainability Index That Incorporates Patient-Centredness for Assessing and Reporting the Sustainability of Healthcare Buildings in Saudi Arabia. Sustainability. 2023; 15(7):5784. https://doi.org/10.3390/su15075784
Chicago/Turabian StyleAlhaij, Ali, Bassem Jamoussi, and Asad Abu-Rizaiza. 2023. "The Development of a Life-Cycle-Based Sustainability Index That Incorporates Patient-Centredness for Assessing and Reporting the Sustainability of Healthcare Buildings in Saudi Arabia" Sustainability 15, no. 7: 5784. https://doi.org/10.3390/su15075784