2. Background
Mobile applications are very useful tools for the promotion of health [
1]. Their use in primary prevention contributes to improvements in nutrition and physical activity [
2,
3,
4]. Apps can also help to reduce the consumption of alcohol [
5]. Sousa et al. [
6] found a significant effect on positive life perspectives and global lifestyle, among other aspects.
The strategy for health promotion and prevention in the Spanish National Health System [
7] proposes the progressive development of interventions aimed at increasing health. Health interventions based on digital technologies, including mobile applications, are optimal for complementing existing sanitary tools [
8], and therefore the World Health Organization [
9] has recently published a guide for their design, development and implementation. Some eHealth apps for adolescents have been designed [
10,
11], and interventions with apps such as that of Benavides et al. have been documented [
12]. However, the potential of digital technologies and applications for the promotion of health and for risk prevention in young people has not yet been thoroughly addressed [
13]. This is an incipient line of research.
Although there are numerous applications available, especially for adults [
14], there are very few applications for the child–adolescent population that consider physical, mental and social well-being jointly. According to Schoeppe et al. [
15], the overall quality of the apps available for improving diet and physical activity and preventing sedentary behaviours in children and adolescents is moderate. While functionality is the best-rated aspect, content quality is the worst. There is also a widely shared perception that apps are boring [
16]. This led to the development of Healthy Jeart. This free application, designed to be used by people aged 8–16 years, was evaluated, before its dissemination, as a “healthy app” by the Andalusian Agency for Healthcare Quality [
17]. This distinction recognises the quality and safety of mobile health applications.
The design of Healthy Jeart began with an exploratory qualitative and interdisciplinary study. Through nominal groups of children and adolescents, the content that potential end users considered should be addressed in the app was identified [
18]. This content was organised, after analysis, into seven areas of health: physical activity, nutrition, physical and psychological well-being, toxic substances and addictions, affection–sexuality and new technologies.
Healthy Jeart contains practical advice and suggestions using brief and simple messages (tips) related to these health areas. See
Figure 1. Children and adolescents can obtain further information by checking the recommended additional resources. Experts in these areas at the national level reviewed the tips to ensure their suitability and adequacy. The language is adapted to the target population.
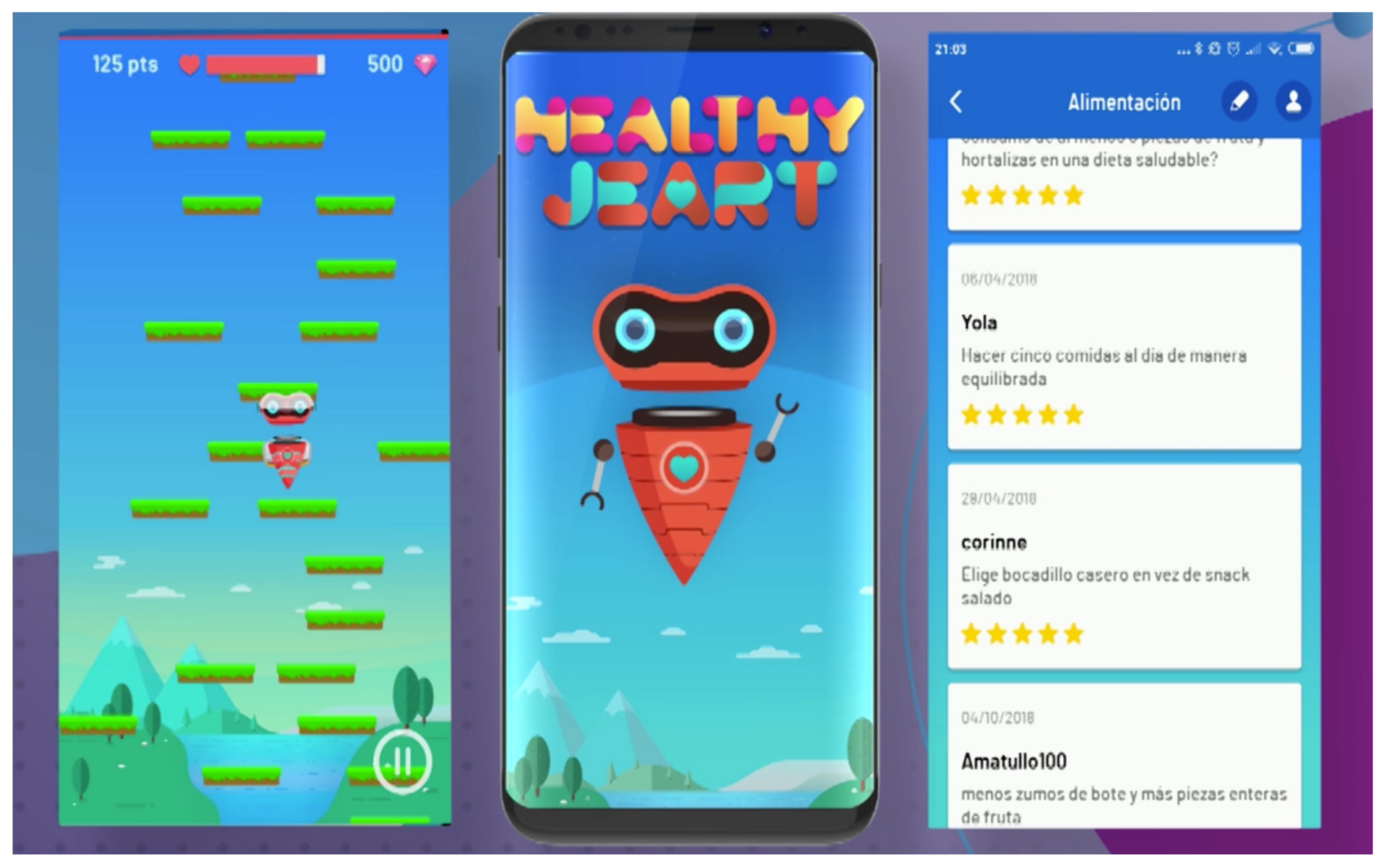
In addition to the tips, there is a game through which the users can recognise the different elements that benefit health and consolidate the knowledge acquired about healthy habits. Healthy Jeart also includes a forum for sharing healthy ideas, which are evaluated by the administrators. Based on the evaluation, the user can obtain rewards for the game. The evaluation is manifested in stars, which the users can exchange for gems for the game. The gems allow the avatar in Healthy Jeart to be changed. The main character in the game is Jeart, a likable, heart-shaped alien. See
Figure 2.
Moreover, Healthy Jeart offers educational activities that teachers can use in their lessons, as well as monthly health challenges, where students can participate and compete with other educational centres. The challenges refer to activities that must be developed in the classroom for at least 21 days, for instance, carrying out a breathing exercise after the break. Of all the centres participating in each challenge, one will be the winner and will be awarded a certificate, which will be automatically issued by the app [
19]. Thus, Healthy Jeart implements various behaviour-change strategies, transcending the application itself [
20]. Specifically, the instructions on how to engage in a behaviour, the feedback on that behaviour and the modelling of behaviours are promoted through challenges and activities, which must be implemented in the classroom under the guidance of the teacher. The challenges and activities are also based on the strategy of social support, as their purpose is to stimulate the interactions, collaboration, etc., which take place within groups of peers.
This study derives from the conviction that adolescence is a key stage for the promotion of a healthy life, during which it is fundamental to correct unhealthy habits that may have been acquired in childhood [
21]. In Spain, various studies have warned that young people are not following balanced diets [
22,
23]; thus, it is necessary to intervene in order to improve eating habits as a preventive measure for adolescents, with therapeutic actions in cases of obesity depending on their excess body weight and their comorbidities [
24]. Furthermore, on average, Spanish children and adolescents do not achieve the recommended levels of physical activity, especially girls [
25,
26]. Thus, educational interventions are needed to reduce sedentary behaviour in the young population [
27], for psychological vulnerability reasons as well as sanitary reasons [
28]. Adolescents do not have healthy lifestyles [
29], and they develop significantly less-healthy practices during the transition to young adulthood [
30]. It is an urgent matter to help them improve their habits and sensitize them to the importance of avoiding risks to their present and future state of health [
31].
The aim of this study was to analyse the changes in nutrition and physical activity habits, as well as in indicators of psychological well-being, in a group of adolescents after an educational intervention, differentiating between an experimental group that used the mobile application designed by the research team, i.e., Healthy Jeart, and a control group.
3. Materials and Methods
An empirical intervention study was conducted. This was the first evaluation of adolescents’ healthy habits, in a pilot study with a single intervention using Healthy Jeart. A total of 4 class groups from an educational centre in Huelva city (Spain) participated in the study. Randomly, the ‘A’ class groups in the third and fourth year of secondary education were selected to organise the control group, and the ‘B’ class groups in the same years were assigned to the experimental group. The educational centre has two class groups per year.
3.1. Instrument
The data were gathered through a questionnaire of closed questions based on the validated HBSC (Health Behaviour in School-aged Children) instrument, which can be found at
https://www.hbsc.es/ (accessed on 7 March 2022). Neither translation nor cross-cultural adjustment of the instrument was necessary. A Spanish version of the instrument is available. The first seven questions were related to the sociodemographic dimension (sex, year and class group, month of birth, age, education level of the parents and economic position of the family). The rest of the questions explored the habits of the participants regarding:
- (1).
Nutrition (3 items): the frequency with which the respondent has breakfast on weekdays and at weekends, and the frequency with which certain foods and drinks are consumed (fruit, sweets, energy drinks, etc.).
- (2).
Body weight control (5 items): weight, height, perception of one’s own body, feelings toward one’s body and whether the respondent is on a diet.
- (3).
Physical activity (2 items): the frequency with which the respondent feels they are active in the week and frequency with which he/she engages in physical activity in his/her leisure time.
- (4).
Dental hygiene (1 item): the frequency with which the respondent brushes his/her teeth.
- (5).
Assumption of risk (8 items): the frequency with which the respondent smokes, drinks alcohol or takes drugs, as well as the type of the latter, if applicable.
- (6).
Violence (2 items): the frequency with which the respondent suffers injuries and becomes involved in physical fights.
- (7).
Positive health (12 items): subjective perception of health and diverse aspects of life.
The questionnaire was digitalised using Survey Monkey and made available to the participants on the first day of contact and on the last day of the intervention. In the initial version, a last question was added at the end, which asked the participants to indicate the areas of Healthy Jeart for which they believed they should improve their habits. The participants received precise instructions on how they should access and answer the questionnaire (indications about what was asked in each part, not about the type of answer). The students answered the questionnaire in class. Their teachers knew the instrument well and were able to assist them.
3.2. Programme
The intervention focused on the three areas that scored the highest on the last question of the questionnaire after the first round of data collection, which were nutrition, physical activity and positive health. It was conducted by a trained person, who did not belong to the research team, in a weekly one-hour session considered as part of the tutorial action plan of the third trimester. The informed consent of the participants’ parents or legal guardians had previously been obtained. Moreover, the Research Ethics Committee of the province of Huelva approved the study. The committee is constituted and acts according to the regulations in force and the guidelines of the International Conference on Good Clinical Practice.
The control group followed the class-based intervention. Different activities were developed in the classroom: looking for information about the properties (vitamins, nutrients, benefits, etc.) of certain foods, designing posters to raise awareness of the benefits of each food group, reflecting on scenes from a short film, etc. One activity was developed per session, and the programme was made up of 12 activities in total. The activities were designed and revised by experts in the areas within the framework of the app creation project and are available both on Healthy Jeart and on the Web at
https://www.healthyjeart.com/actividades-didacticas/ (accessed on 7 March 2022) as suggestions for teachers. These activities did not involve the use of the app. Therefore, this group did not interact with Healthy Jeart.
The dynamics of the sessions with the experimental group adhered to the following scheme, considering that the participants had access to Healthy Jeart:
- (1).
Play the game, challenging the students to beat their own scores.
- (2).
Visualise the tips for healthy habits.
- (3).
Participate in the forum of ideas.
- (4).
Develop the same didactic activity to consolidate healthy habits as in the control group.
This pilot study was conducted after presentation of the tool to the management team and the teachers in a specific seminar.
3.3. Participants
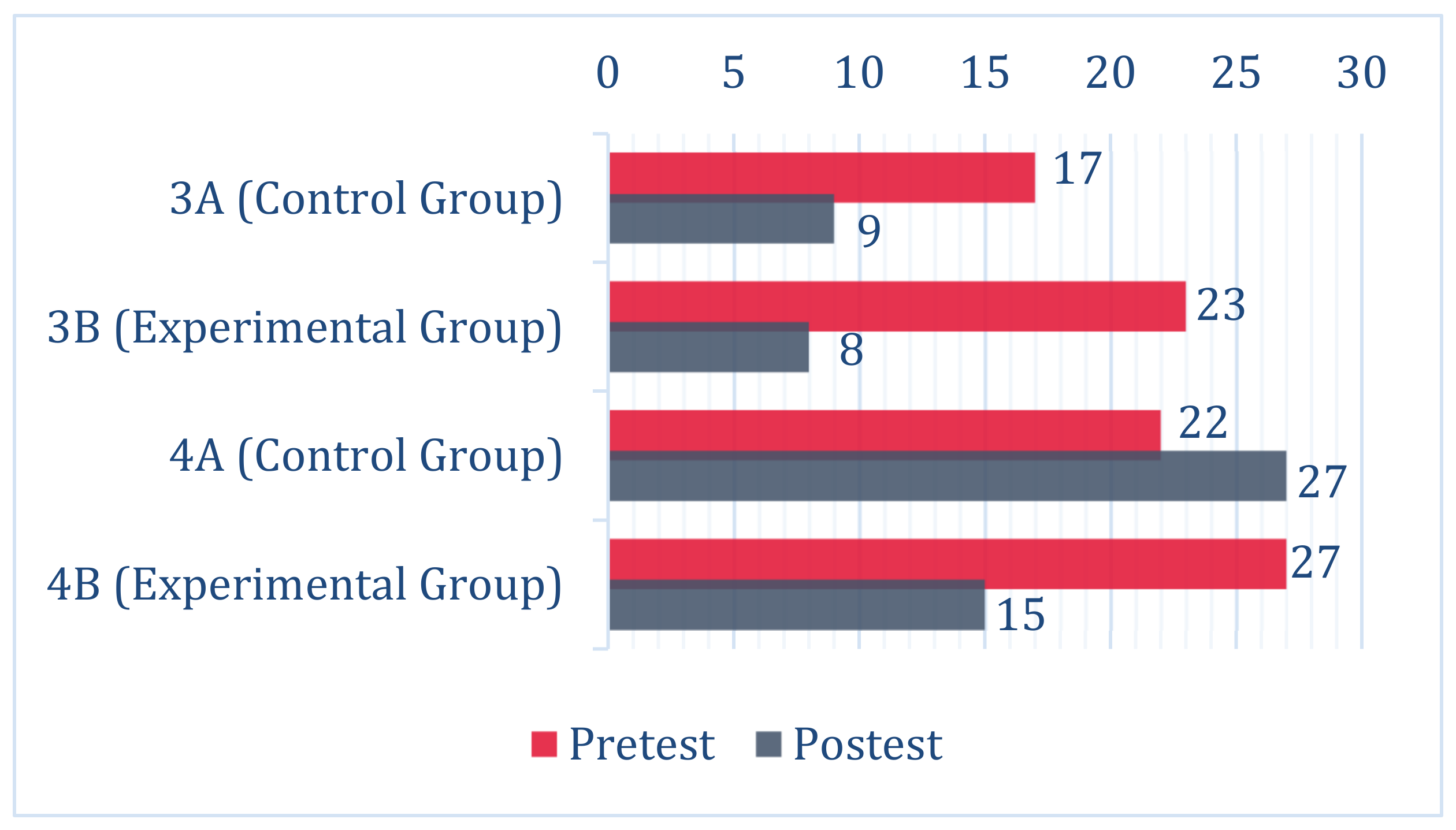
A total of 89 students completed the questionnaire before the intervention (39 in the control group and 50 in the experimental group). Of these, 59 completed the questionnaire after the intervention (36 in the control group and 23 in the experimental group). Thirty students were lost to follow-up as a result of not completing the final evaluation, since participation was voluntary. There were 44 girls (49.4%) and 45 boys (50.5%) in the first round of data collection (pre-test), and 24 girls (40.7%) and 35 boys (59.3%) in the second round of data collection (post-test). The numbers of students per year and per class group at each of the time points are shown in
Figure 3.
3.4. Data Analysis
To identify changes in behaviour for the variables related to the priority intervention areas (dependent variables) after the educational intervention (independent variable), hypotheses testing was used. Using these statistical tests, applied to the data for the experimental and control groups, the aim was to determine whether statistically significant differences occurred in the nutritional, physical activity and positive healthy habits of the participants, before and after the experience. Therefore, the null hypothesis (H0) was the absence of significant differences in the results before and after the educational intervention. The alternative hypothesis (H1) was the existence of differences between the results obtained at the two time points.
The Mann–Whitney U-test for independent samples was applied. For the analysis of the data, the statistical package IBM SPSS Statistics V.25.0. (IBM Spain S.A., Madrid, Spain) was used. It is important to highlight the fact that, since the selected samples were not representative of the population from which they came and the study variables did not show a normal distribution, a non-parametric contrast was used (the Kolmogorov–Smirnov test was applied to verify the normality of the data, obtaining significance levels below 0.05 in all cases).
5. Discussion
The habits of the sample of participants in this study were in line with the results of the study entitled “Health Behaviour in School-aged Children” (HBSC 2018), conducted in Andalusia [
32], although it warns, to a slightly greater extent, of lacks/problems in their lifestyles due to a worsening of behaviours among some of the students.
After the class-based intervention, the results demonstrated a partial effect in the nutritional area, which did not occur after the intervention implemented with Healthy Jeart. It is worth clarifying that, in Healthy Jeart, health is approached globally, and consequently nutrition is one of the seven areas tackled. In the first moments of the sessions dedicated to nutrition, the students did not focus exclusively on eating habits through the tips, the game and the forum. This occurred in every session. These students did not focus only on the content tackled in the didactic activities in each session, unlike the control group. We believe that the activities worked well in both groups, although the interaction with the app in the sessions on nutrition counteracted the effects for this reason. The content of this area and the work proposals in the app should therefore be reviewed.
The results show the need for the updates that have been planned for the application, which are aimed at extending the functionality with a new system about eating. These enable young people to search for nutritional information: (1) manually, (2) through the direct scanning of a bar code, (3) by providing the bar code manually or (4) through image recognition. In this way, the users are offered an attractive way of checking the ingredients of a product, the level of processing of a food product through the NOVA group to which it belongs and the meaning of these groups, the nutritional information provided and the allergens the product contains. This functionality, which allows users to obtain correct information while selecting foods for consumption, ignoring the influence of marketing and fashion, is already found in other applications [
11].
We cannot confirm that the mHealth intervention was more effective than the class-based intervention in the promotion of healthy behaviours [
6], or that it was less successful. The educational intervention carried out, whether it took place with or without the support of Healthy Jeart, did not result in substantial changes in healthy life habits in the sample of participants. The results did not show a general positive improvement. Therefore, among the limitations of the study, firstly, it is important to point out the use of a measurement instrument that is widely used internationally but which was not adjusted to the content of the application or to the activities. For this reason, we worked on the writing and validation of a scale that increased the effectiveness of the evaluation. This evaluation instrument can be found at
https://www.healthyjeart.com/ (accessed on 7 March 2022). Secondly, it is also important to admit that the last round of data collection coincided with the termination of the intervention, although changes in habits are shown in the medium or long term, according to the existing scientific evidence. Thirdly, the sample size was small. Lastly, the intervention duration was short, which conditioned its effect. The low reach and exposure of the intervention could explain its low impact, as was the case in other experiences and studies [
33].
We agree that technology can be a good ally in promoting healthy habits [
34,
35]. We should highlight the effect detected in the group that worked with Healthy Jeart on feeling good and in shape. The global perspective on health of the app would explain this change. Advice and suggestions help adolescents become aware of different lifestyle domains.


 ,
, 



{kind=link}
{kind=link}
{kind=link}


