
The COVID-19 Infodemic: Mechanism, Impact, and Counter-Measures—A Review of Reviews


1
Pediatric Neurology and Metabolic Medicine, Center for Pediatrics and Adolescent Medicine, University Hospital Heidelberg, INF 430, 69120 Heidelberg, Germany
2
Center for Virtual Patients, Medical Faculty, University of Heidelberg, INF 430, 69120 Heidelberg, Germany
Sustainability 2022, 14(5), 2605; https://doi.org/10.3390/su14052605
Submission received: 23 January 2022
/
Revised: 21 February 2022
/
Accepted: 21 February 2022
/
Published: 23 February 2022
(This article belongs to the Topic Impact of COVID-19 Global Crisis on the Sustainable Development Goals)
Abstract
:The acceptability of appropriate SARS-CoV-2 pandemic measures including vaccinations is currently being hampered due to significant misinformation all over the globe, also known as the “infodemic” within the pandemic. We asked the following two research questions: (1) What is the current extent of the global infodemic preventing populations from receiving adequate healthcare including COVID-vaccinations? (2) Which are appropriate countermeasures to manage the infodemic in order to guarantee adequate healthcare in the SARS-CoV-2 pandemic? Pubmed and Cochrane Library were accessed on 29 October 2021 and searched for reviews and systematic reviews on “COVID-19” and “infodemic”. The literature identified was analyzed with methods of qualitative research focusing on (1) mechanism, (2) impact, and (3) countermeasures to confront the infodemic. The world-wide infodemic is being recognized as a multifaceted problem beyond health and human rights, extending into global political spheres such as societal cohesion and security. The mechanism of the COVID-19 infodemic involves specific factors related to the situation, sender, instrument, and recipient. Although freedom of expression and the right to seek, receive, and impart information through any media is a fundamental human right, the infodemic has a substantial impact on health, another fundamental human right, by causing stress, deception, violence, and harm. Mixed-synergistic pre-impact, trans-impact, and post-impact countermeasures can be taken; the most important is building and maintaining trust.
1. Introduction
1.1. Background and Rationale for This Work
COVID-19 (coronavirus disease 2019) is due to an infection from the novel coronavirus known as SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2). By 16 April 2021, 282,912,372 cases and 5,417,212 deaths were reported globally [1]. Vaccination is expected to reduce the further spread of SARS-CoV-2, and by 29 December 2021, 9,035,158,893 vaccine doses were administered globally [1,2]. Access to vaccinations for both adults and children is an important preventive health care instrument to overcome the current SARS-CoV-2 pandemic [3]. Acceptability of appropriate pandemic measures including vaccinations is currently being hampered due to significant misinformation all over the globe, also known as the “infodemic” within the pandemic [4].
Health is a human right. Specifically, according to Article 25 of the Universal Declaration of Human Rights, “Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control” [5]. Health is also a child’s right: article 24 of the United Nations Convention on the Rights of the Child states that children have the right to enjoy “the highest attainable standard of health” [6]. In addition, health is an important aspect of sustainability. “Ensure healthy lives and promote well-being for all at all ages” is a sustainable development goal defined by the United Nations member states [7]. Of note, targets 3.3 (“by 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases”), 3.8 (“achieve universal health coverage, including financial risk protection, access to quality essential health-care services and access to safe, effective, quality and affordable essential medicines and vaccines for all”), 3b (“support the research and development of vaccines and medicines for the communicable and non-communicable diseases that primarily affect developing countries, provide access to affordable essential medicines and vaccines, in accordance with the Doha Declaration on the TRIPS Agreement and Public Health, which affirms the right of developing countries to use to the full the provisions in the Agreement on Trade-Related Aspects of Intellectual Property Rights regarding flexibilities to protect public health, and, in particular, provide access to medicines for all”), and 3d (“strengthen the capacity of all countries, in particular developing countries, for early warning, risk reduction and management of national and global health risks”) of this sustainable development goal cover issues encountered in the COVID-19 pandemic [8]. At the same time, freedom of opinion and speech is another fundamental human right that has to be balanced appropriately in this context. As such, Article 19 of the Universal Declaration of Human Rights states that “Everyone has the right to freedom of opinion and expression; this right includes freedom to hold opinions without interference and to seek, receive and impart information and ideas through any media and regardless of frontiers” [5].
1.2. Definitions
The term “infodemic” was coined by Rothkopf in 2003 in the wider context of a SARS outbreak. Specifically, Rothkopf defined an infodemic as “a few facts, mixed, with fear, speculation and rumor, amplified and relayed swiftly worldwide by modern information technologies [that] have affected national and international economies, politics and even security in ways that are utterly disproportionate with the root realities” [9]. Likewise, the WHO defines an infodemic as: “too much information including false or misleading information in digital and physical environments during a disease outbreak” [4].
1.3. Research Questions
We directed our efforts in researching the current global spectrum of COVID-19 related infodemic in order to identify common themes and proposed countermeasures. We asked the following two research questions: (1) What is the current extent of the global infodemic preventing populations from receiving adequate healthcare including COVID-vaccinations? (2) Which are appropriate countermeasures to manage the infodemic in order to guarantee adequate healthcare in the SARS-CoV-2 pandemic? As such, this review of reviews is focusing on (1) mechanism, (2) impact, and (3) countermeasures to confront the infodemic. It provides a temporo-spatial mapping of the literature as well as a contextual integration of the COVID-19 infodemic in examples of previous, similar phenomena in other infectious diseases.
2. Previous Literature
The COVID-19 infodemic is a rapidly evolving situation. The current picture within the original literature and reviews is in part fragmented and mostly focuses on single aspects of the issue. Therefore, there is a need for a review of reviews in order to render the available evidence visible and transparent from a holistic overarching perspective.
3. Methods
3.1. Review Scope
3.2. Literature Search
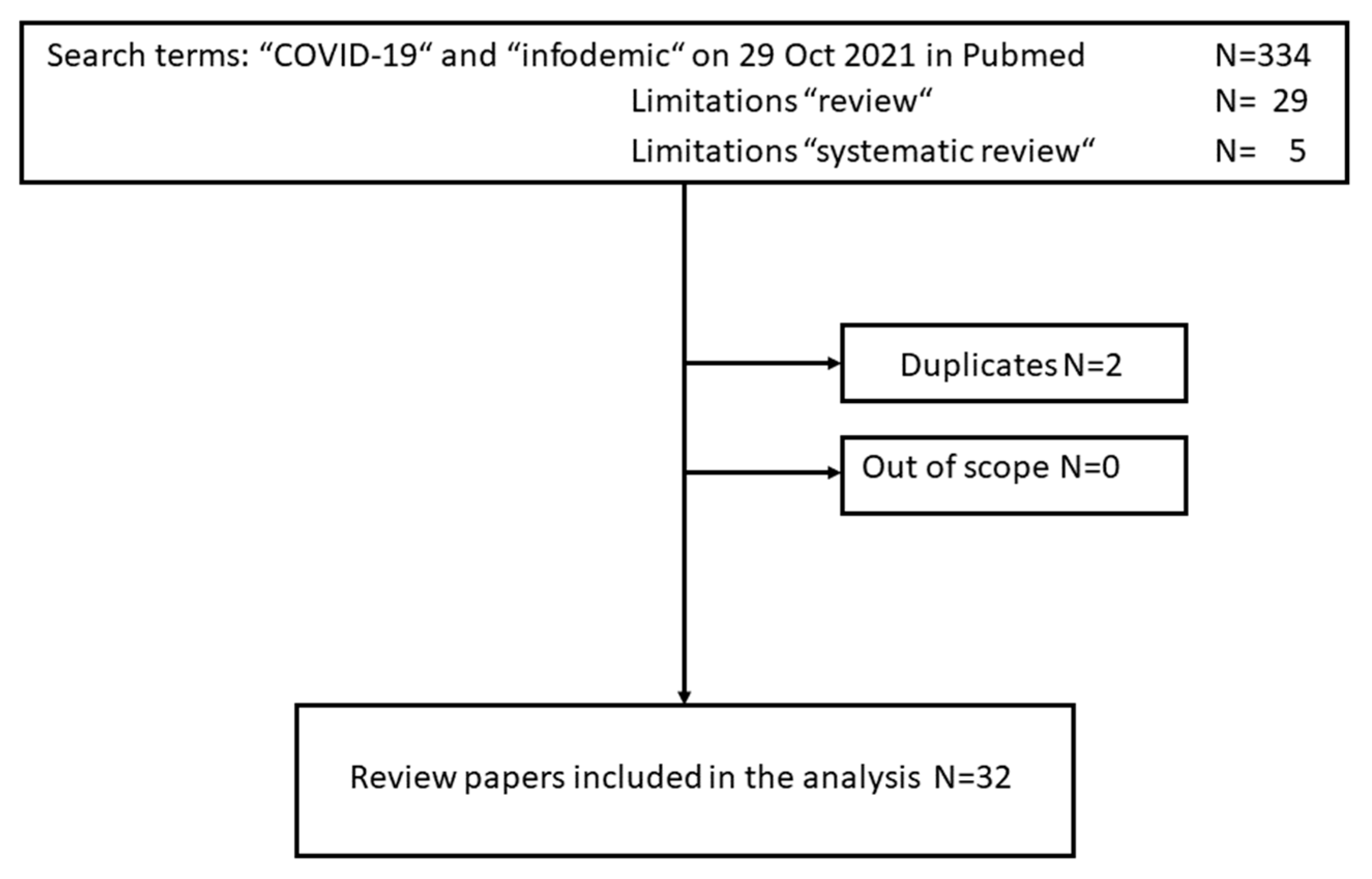
We searched two literature databases. Pubmed was accessed over the internet and searched on 29 October 2021 with keywords “COVID-19” and “infodemic”. Search limitations included “reviews” and “systematic reviews”. In addition, a search in the Cochrane Library was conducted with the same search terms, parameters, and dates at https://www.cochranelibrary.com/advanced-search (accessed on 29 October 2021), and no review was identified.
Results were downloaded in Libre Office Calc format (https://www.libreoffice.org/discover/calc/ (accessed on 14 November 2021)) and duplicates were removed manually.
3.3. Qualitative Literature Analysis
The geographic distribution of the identified literature was assessed by mapping in order to gain insight into the literature’s global distribution. The reports’ first authors’ countries of affiliations were mapped online with www.mapchart.net (accessed on 22 November 2021). The map was then downloaded over the internet and saved as .png file.
Identified reviews were analyzed through a qualitative, mixed narrative-phenomenological approach as proposed by Creswell [11,12]. Specifically, narrative-phenomenological qualitative information in the articles was identified by transcribing articles into plain text format which was then assessed for significant statements as narrow unit of analysis. These significant statements were then horizontalized and grouped into clusters of meaning (Table 1). The coding was conducted with the open source qualitative data analysis package RQDA (http://rqda.r-forge.r-project.org/, accessed 14 November 2021) in R (https://www.r-project.org/ (accessed on 14 November 2021)) on a Linux computer operated with Linux Mint (https://linuxmint.com/ (accessed on 14 November 2021)).
4. Presentation and Interpretation of Results
4.1. Global Geographical Distribution of Reviews Included Assessed as Countries of First Authors’ Affiliation
The first authors’ affiliations of the literature identified represented a broad spectrum of diverse countries in terms of economic development and care systems as well as geographic distribution over the globe, ranging from North and South America, Europe, Africa, and Asia (Figure 2).
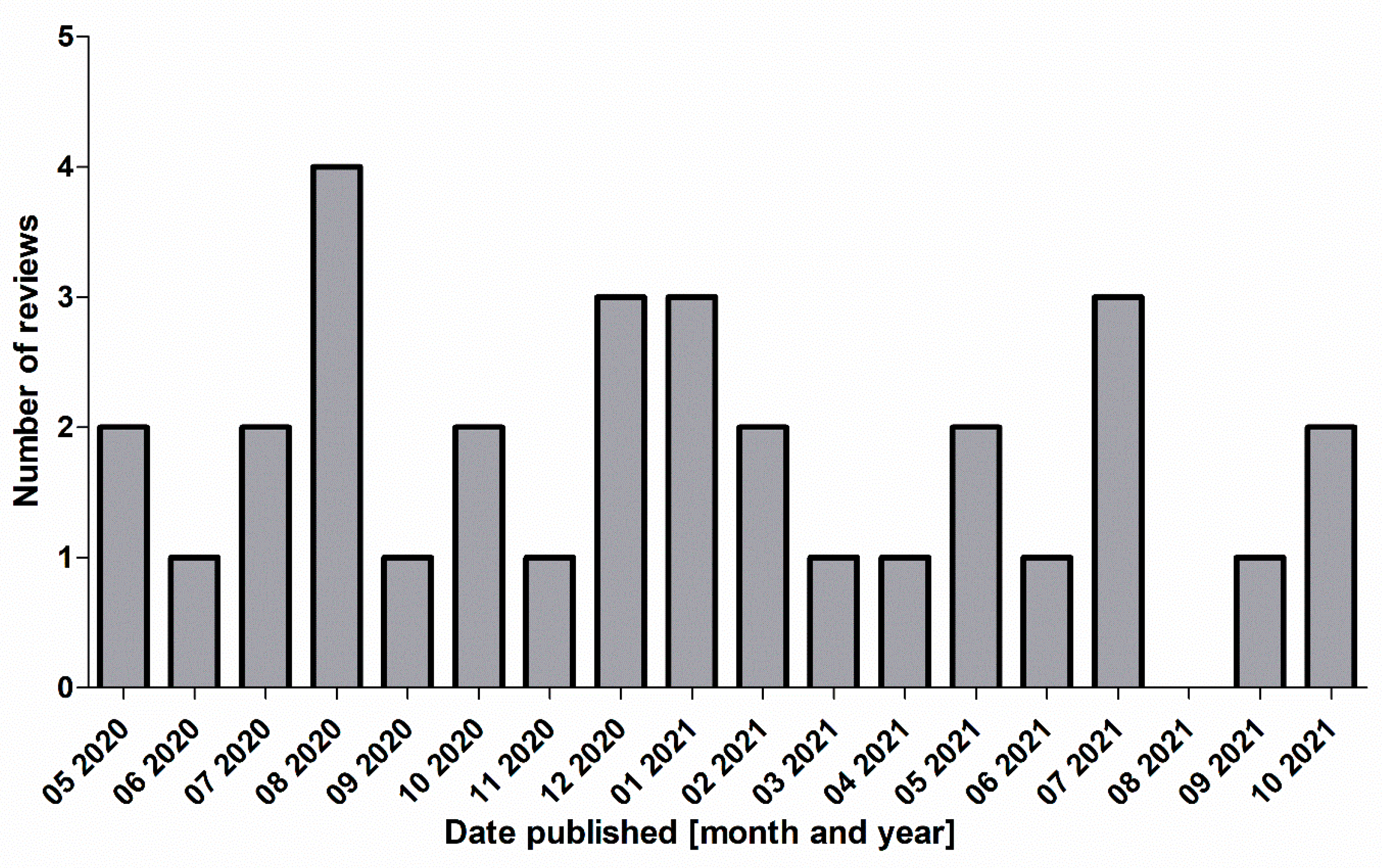
This suggests that the observations described and synthesized in the reports are rather universal and can be generalized. All review articles were published between May 2020 and October 2021 (close of database was 29 October 2021).
4.2. Mechanism of the Infodemic
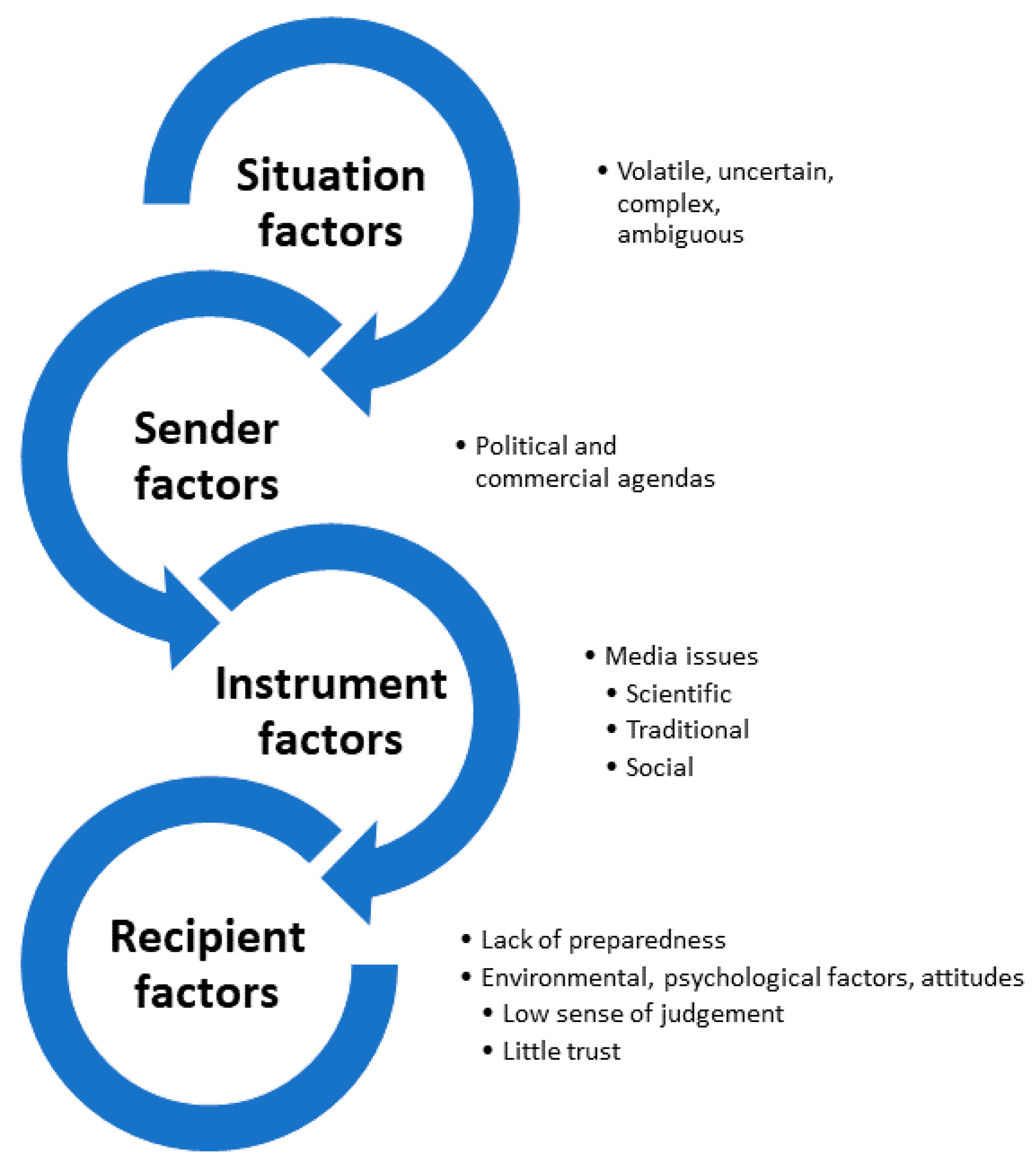
The mechanism of the infodemic implies factors that are related to (1) the situation, (2) the sender of the message, (3) the communication instrument used, and (4) the recipient of the message (Figure 3).
4.2.1. Situation Factors
Situation factors are issues inherent to the situation itself that subsequently fuel an infodemic. COVID-19 evolved as a rapidly changing, dynamic situation with volatile, uncertain, complex, and ambiguous elements [2]. There was an exponential increase of publications on the subject COVID-19 with biased peer-review and editorial processes [14,15]. Scientific information was produced fast at standards below best practice, disseminated at high visibility, and the captured interest did not correlate with quality [16]. The situation changed fast, messages disseminated were mixed, incomplete, conflicting, and sometimes incorrect [17,18]. Scientific information was exchanged fast and preliminary as non-peer reviewed preprints; in addition, an exceptionally high number of articles was later retracted [19]. There were many unknowns about the disease, such as transmission, manifestation, long-term sequelae, and immunity; at the same time the communication of these issues occurred in a complex scientific and mathematical-statistical language or by means of data-intense dashboards [20,21].
4.2.2. Sender Factors
Sender factors relate to originators of misinformation in the infodemic. Some senders had their own commercial or political agenda, i.e., misinformation can be disseminated with the intent to “trick people into believing something for financial gain or political advantage” [22]. The virus was indeed politicized [14]. Irrational beliefs including prejudice, paranoia, extremism, racism, conspiracy theories, and faith in magical cures played a role [23,24,25]. An example of inappropriate marketing was the direct-to-consumer targeted online advertisement of unproven and unauthorized stem-cell-based interventions in China [26]. Senders of misinformation can include individuals who deny scientific consensus on health issues [22]. Examples of misinformation tactics applied are the presentation of unqualified “experts”, misleading the public through logical fallacies, creating impossible expectations for scientific research, cherry-picking data or selected anecdotes, and spreading conspiracy theories [22,27].
4.2.3. Instrument Factors
Instrument factors relate to issues with media that disseminate information leading to an infodemic. These issues were reported in scientific and general media, for traditional outlets (e.g., television channels, newspapers, and radio channels), as well as for online and social media formats [14,15,16,18,19,21,25,28,29,30,31,32]. Specifically, medical journals published low-quality non-transparent articles without the usual standard of academic and editorial rigor [16]. Most of the thousands of articles published on COVID-19 were not original research but reviews and editorials with evident absence of evidence-based guidelines [19]. Social media, usually operating in an unregulated environment, contributed to disseminating both accurate information conveyed by experts, but also misinformation and speculation [20,31,33]. False information and unsourced recommendations on health were spread by various outlets including digital media [15]. Widespread availability of information on the internet and low-barrier access to electronic media facilitated sharing and amplifying genuine and fake messages [25,28,32]. Bots (i.e., software applications that automatically conduct tasks on the internet and social media without human interaction) contributed to the infodemic [30].
4.2.4. Recipient Factors
Recipient factors relate to the individual or the group that is opposed to the infodemic. A lack of adequate preparedness for the pandemic was identified as an issue, in addition to a widespread low digital health literacy [24,30]. A lack of trust in the government and a lack of scientific knowledge can lead to the increased consumption of misinformation [33]. Magarini et al. identified specific socio-environmental conditions, psychological processes and attitudes in addition to contextual factors that can render individuals vulnerable to irrational and adverse beliefs in the infodemic [23]. In particular, these factors included low educational level, younger age, low level of epistemic trust, avoidance of uncertainty, extraversion, collective narcissism, a conspiracy-prone mindset, high level of self-perceived risk, and anxiety [23]. Possible reasons for susceptibility for vaccine hesitancy are mistrust of doctors, health services, the government, the pharmaceutical industry, safety concerns, complacency over low perceived personal risks, misinformation, religious beliefs, dietary restrictions, historical concerns, a particular lifestyle (“natural medicine”), or COVID-19 denial [34].
4.3. Impact of the Infodemic on Health
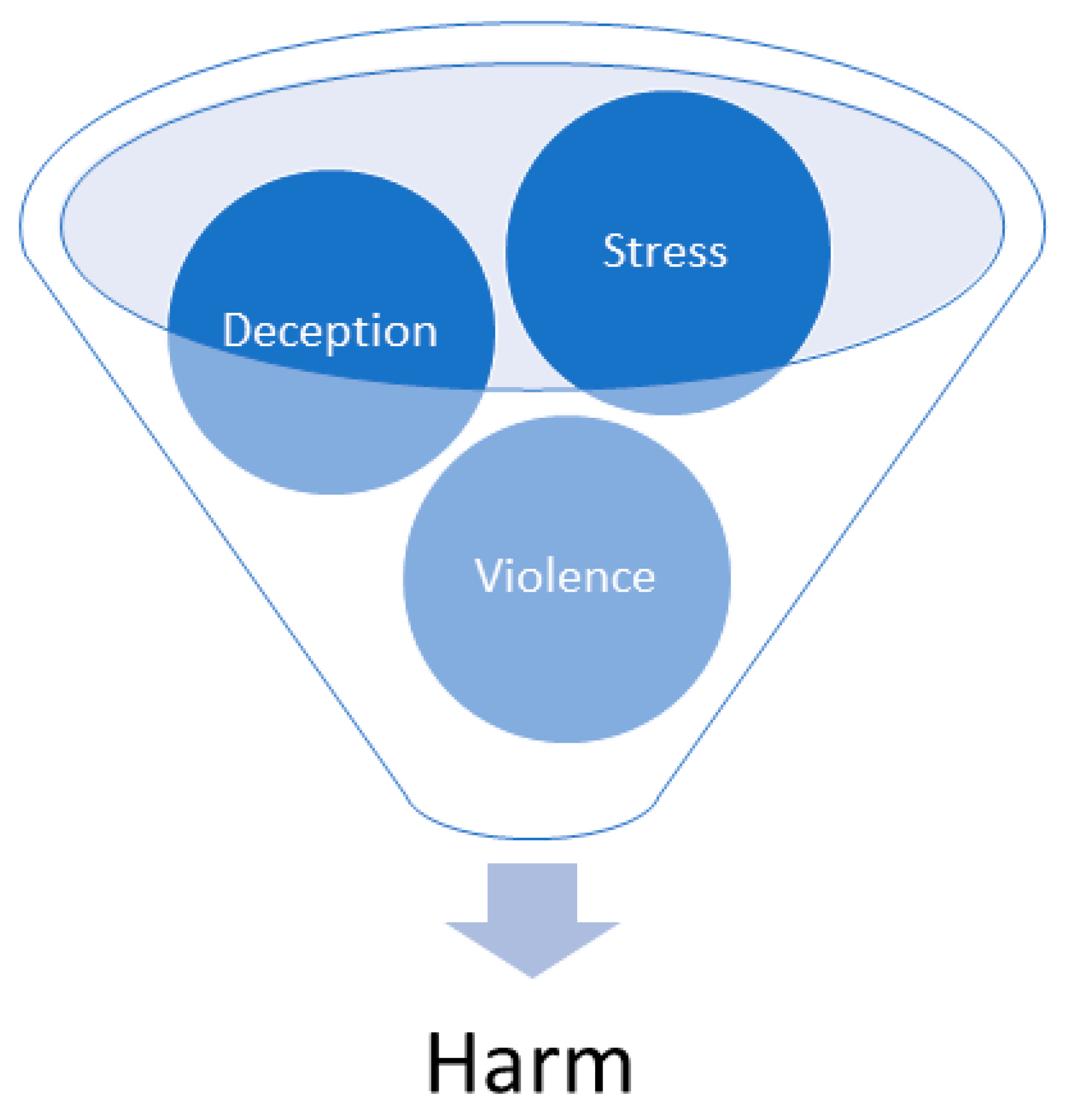
The impact of the infodemic on the individual or the population could be categorized into four clusters: (1) stress, (2) deception, (3) violence, leading to (4) harm (Figure 4).
4.3.1. Stress
Much of the COVID-19 associated socio-economic damage and impacted flow of life was not only attributed to the disease itself but to the misinformation around it (Chowdhury, 2021). Infodemics can lead to stress [32]. Stress-related psychological issues and mental health impacts manifested with a broad spectrum. Misinformation led to fear and panic [31]. The rapid spread of information led to uncertainty; misinformation caused anxiety or psychological distress, fear, uncertainty, panic, depression, and fatigue [29]. Abrams et al. and Anwar reported confusion, public worry, panic, fear and psychological stress [21,35]. Mass hysteria and mass fear also known as “coronaphobia” across different strata of the society were observed [36]. Panic, anxiety, obsessive behaviors, hoarding, paranoia, depression, and post-traumatic stress disorder (PTSD) associated with quarantine measures were fueled by the infodemic on social media [36,37,38]. Healthcare workers were concerned about safe and responsible functioning [39].
4.3.2. Deception
The infodemic can lead to deception resulting in poor and erroneous decision making. The overabundance of factual and misinformation contributed to vaccine hesitancy [34]. Rapidly disseminated, low-quality scientific output such as systematic reviews not properly conducted, but labeled as such, which may not immediately be visible to the reader, can lead to inaccurate representation of scientific evidence, inaccurate estimates of the treatment effectiveness, misleading conclusions, and reduced applicability [16]. This can result in promotion of false information and biased health policies [15]. Unscientific cures and unverified medicines promoted by politicians and fake doctors received substantial attention [21]. The promotion of unauthorized and unproven indications for stem-cell administrations in China attracted patients from within the country and abroad [26]. The infodemic interfered with communication channels to the public and affected appropriate adherence of the population to meaningful pandemic countermeasures [40]. In a clinical context, uncertainty affected shared decision making with patients, and decisions on safely reinitiating services [35]. Misleading communication practices can hamper the uptake of scientific information in an environment of poor public awareness of dangers of the infodemic itself [14].
4.3.3. Violence
Various degrees of subtle up to physically manifested violence were observed in the infodemic. There are concerns that semi-automated decision making in the digital response to the pandemic may increase existing discrimination and inequalities [41]. Racial prejudices tied to the origin of the virus impeded scientific collaborations, and there was an increase in domestic and elderly abuse [21]. Likewise, the infodemic triggered discrimination, stigmatization, and xenophobia against particular communities [24,36]. Misinformation, rumors, and conspiracy theories led to physical harassment and attacks against healthcare workers and people of Asian origin [29].
4.3.4. Harm
The infodemic worsened the impact of the pandemic and led to damage and harm [33,42]. Fake news, conspiracy theories, and racist news might even lead to loss of life [32,42]. Likewise, unscientific and unproven cures were harmful [21]. An important example was vaccine hesitancy which left non-vaccinated individuals unprotected and was fueled though uncertainty due to the infodemic and misinformation [34]. Misinformation could induce hazardous behavior; the distrust in scientific and public institutions as well as the confidence crisis triggered by the infodemic resulted in harmful health behavior and also had an impact on mental health. [14,23]. Dubey et al., (2020) suggest that the infodemic increased substance dependence [36].
4.4. Measures to Confront the Infodemic by Phase of Disaster Cycle
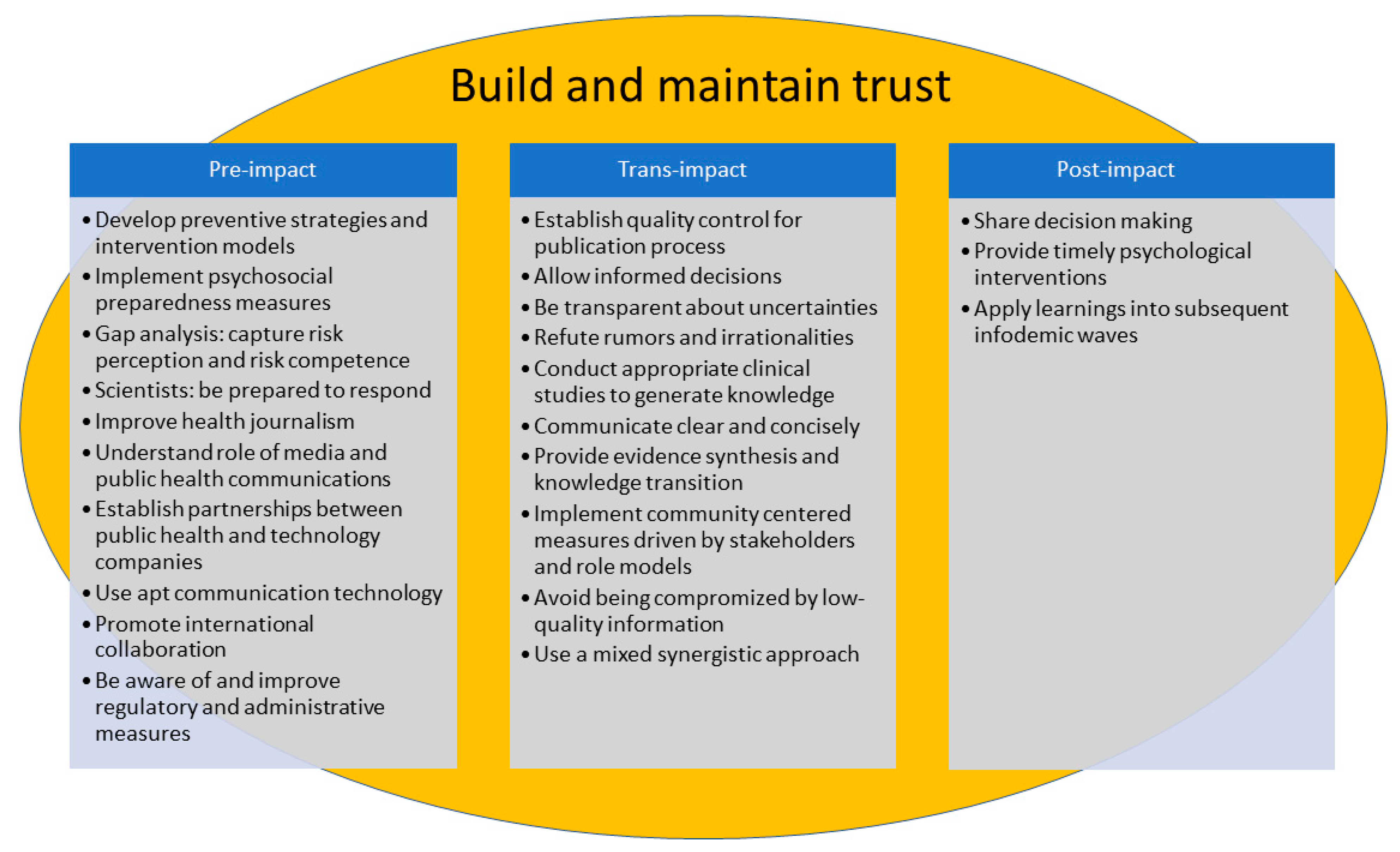
A disaster cycle distinguishes, in general, three phases of a crisis in function of time: (1) pre-impact, i.e., before the disaster strikes, (2) trans-impact, i.e., during the impact of the disaster, and (3) post-impact, the phase after the disaster [13].
Various measures were proposed or discussed in the literature reviewed and are summarized in Figure 5. The attribution of a given measure to a specific temporal phase in the cycle is not absolutely categorical, and some measures can extend over two or more phases. Some observations reported relate to both the pandemic and the infodemic as both related phenomena cannot be regarded in strict isolation from each other. The most important one across all phases of the disaster cycle is building and maintaining trust.
4.4.1. Pre-Impact Measures
Pre-impact measures should be considered as a timely preparation ahead of the curve before an infodemic strikes in order to reduce vulnerabilities, and in order to plan how to respond to minimize its hazardous effects. This includes building a network of trust and alliances as well as identifying gaps. The development of strategies and models to prepare for crisis prevention and intervention is important [24,36,37]. Establishing mental health organizations with international branches for research, mental healthcare delivery, and awareness programs at personal and community levels have been proposed for future pandemics [36]. Capturing the risk perception and risk competence can identify gaps in the population and support crisis preparation [20]. A good understanding of health information seeking behavior of the population can help mitigating and preparing for an infodemic [42]. Scientists play a significant role in the context of an infodemic because of their expertise and their societal standing; they should be conscious about this and be prepared to respond to families, friends, and the community [17]. Improving quality of health journalism increases credibility which is particularly important in mass-media environments where health literacy is low [28].
Editors and peer reviewers of scientific publications should ensure academic rigor and methodological robustness [16]. Journalists and editors should be sensitized how to recognize misinformation, how to deal with preliminary data, be cognizant of reliability and credibility of their sources, communicate balanced context preferring informative rather than shocking headlines [22]. A good understanding of the role of media and technology companies and public health communications can support the mitigation of an infodemic [41]. Apt use of the internet, technology, and social media can mitigate the impact of both the pandemic and the infodemic [36]. Partnerships between the public health sector and technology companies, ideally before the occurrence of a crisis, can be beneficial [41]. The awareness of regulatory and administrative measures provides orientation, it might be necessary to close gaps within this domain if deficiencies are being identified [26]. As an infodemic can be a global phenomenon, international collaboration among researches and regulators is warranted [26].
4.4.2. Trans-Impact Measures
The goals of trans-impact measures are to minimize the impact of the infodemic with an immediate action plan once it commences. When the infodemic strikes, building trust by credibility is important. One aspect is that scientific publications be conducted according to robust and rigorous standards [16]. Risk communication allowing informed decision making, promoting appropriate protective behavior, and maintaining trust is key [20,22]. Transparency about uncertainties should be clearly communicated [20,40]. Refuting rumors and irrationalities is important [20,22]. Fact-checkers, health literacy guidelines, myth busters, checklists, and artificial intelligence can be useful tools to approach this goal [15,30]. Designing and conducting appropriate clinical studies to generate useful knowledge will support evidence-based decision making and contribute to flatten the infodemic curve [19,43]. Clear, concise communication and messaging allows decision-makers to take action based on correct interpretation of the data and avoids being misled, e.g., by low-quality data [14]. In addition, evidence synthesis and knowledge translation can be useful tools to communicate accurate scientific information to decision-makers [14,38]. Implementing community centered measures driven by stakeholders and role models can help producing orientation, reducing uncertainties, and building as well as maintaining trust [18,22,34].
Stakeholders encompass a wide range of groups which include a. individuals, families, and communities, b. educators and educational institutions, c. health professionals and health organizations, d. journalists and media organizations, e. technology platforms, f. researchers and research institutions, g. funders and foundations, and h. governments [22]. Avoiding information overload and preventing misleading information from being disseminated widely is another important consideration [15,25,32]. Low barrier access to virus testing can reduce uncertainty and fear of the unknown [39]. Cooperation, participation, proportionality, and a good understanding of risk perception and risk competency are additionally important elements to confront the infodemic [20,40]. Awareness of both behavior as well as attitudes is important to understand the affected population [42]. Due to the complexity of an infodemic, the overall approach does not focus on a single item, but rather a synergistic mix of various tactical elements [30].
4.4.3. Post Impact Measures
Post impact measures should support the way back to normalcy. Shared decision making, e.g., with colleagues and patients, can help to build bridges, facilitate transition, and support change management [35]. Timely intervention and long-term psychological follow-up should be considered for vulnerable groups or groups at high risk for psychosocial issues [36]. Lessons-learned and lessons-identified should be implemented into improved management of subsequent infodemic waves or even future pandemics [31].
4.5. Examples for Infodemics in the Past Other Than COVID-19
The infodemic during COVID-19 is not an isolated phenomenon in the history of infectious disease outbreaks; there are predecessors. In general, viral epidemics and pandemics have been associated with anxiety and stress [37]. Vaccine hesitancy itself has been observed in Europe since the 18th century, and had even led to violent riots [34]. Infodemics have been observed during SARS, H1N1, and MERS pandemics [21]. The spread of misinformation with regard to prevention, treatment, risk factors, transmission mode, complications, and vaccines was observed in large-scale outbreaks of infectious diseases since the year 2000 including Ebola, and conspiracy theories particularly involved vaccines [33]. With regard to stem cell research, both researchers and regulators have been fighting against misleading advertising of unproven interventions for decades [26].
4.6. Limitations and Directions for Future Research
This report has important limitations that have to be taken into account for appropriate interpretation. Firstly, the information presented is based on qualitative information extracted from reviews, the original reviews themselves being conducted with heterogeneous methodologies ranging from narrative to systematic. A formal assessment of review quality based on pre-specified criteria such as PRISMA was not undertaken. Secondly, many phenomena presented in the reviews were based on observations and not necessarily controlled experiments; therefore, the inference of causality rather than association should be undertaken with caution. Third, this review of reviews was based on two mainly medical databases because the pandemic is mainly a medical issue. A literature search in more than two databases may have contributed further aspects and perspectives that were not captured here. Nevertheless, this work is informative and generalizable in the context of these limitations. This report is of interest as a baseline for future pandemics in order to ascertain whether learnings from the present COVID-19 infodemic were helpful to avoid or at least mitigate another infodemic. In addition, future research about infodemics should consider perspectives on sustainable development goals including their short- and long-term targets and indicators.
5. Conclusions
This review of reviews provides an overview of the significance, mechanism, impact, and countermeasures to confront the COVID-19 infodemic.
An infodemic is significant, because it is recognized as a multifaceted problem beyond health and human rights, extending into global political spheres such as societal cohesion and security [4,44].
The mechanism of the COVID-19 infodemic involves specific factors related to the situation, sender, instrument, and recipient. Although freedom of expression and the right to seek, receive, and impart information through any media is a fundamental human right, the infodemic has a substantial impact on health, another fundamental human right, by causing stress, deception, violence, and harm. Mixed-synergistic pre-impact, trans-impact, and post-impact countermeasures can be taken; the most important is building and maintaining trust.
Funding
For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding program “Open Access Publikationskosten” as well as by Heidelberg University.
Institutional Review Board Statement
Not applicable, because this review did not directly involve humans or animals.
Informed Consent Statement
Not applicable, because this review did not directly involve humans.
Data Availability Statement
All relevant data are in the manuscript.
Acknowledgments
I am indebted to Joachim A. Koops, Institute of Security and Global Affairs, Leiden University, The Netherlands, for the inspiring discussions about International Human Rights. I thank Sophie Ries for proofreading the manuscript.
Conflicts of Interest
The author declares no conflict of interest.
References
- Johns Hopkins University. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 29 December 2021).
- Schulze, C.; Welker, A.; Kuhn, A.; Schwertz, R.; Otto, B.; Moraldo, L.; Dentz, U.; Arends, A.; Welk, E.; Wendorff, J.J.; et al. Public Health Leadership in a VUCA World Environment: Lessons Learned during the Regional Emergency Rollout of SARS-CoV-2 Vaccinations in Heidelberg, Germany, during the COVID-19 Pandemic. Vaccines 2021, 9, 887. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Vaccines. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines (accessed on 29 December 2021).
- World Health Organization. Health Topics/Infodemic. Available online: https://www.who.int/health-topics/infodemic#tab=tab_1 (accessed on 12 January 2021).
- United Nations. Universal Declaration of Human Rights. Available online: https://www.un.org/en/about-us/universal-declaration-of-human-rights (accessed on 29 December 2021).
- United Nations. Convention on the Rights of the Child. Available online: https://www.ohchr.org/en/professionalinterest/pages/crc.aspx (accessed on 29 December 2021).
- United Nations. Sustainable Development. Goal 3: Good Health and Well Being. Ensure Healthy Lifes and Promote Well-Being for All at All Ages (Overview). Available online: https://sdgs.un.org/goals/goal3 (accessed on 4 January 2022).
- United Nations. Sustainable Development. Goal 3: Good Health and Well Being. Ensure Healthy Lifes and Promote Well-Being for All at all Ages (Targets and Indicators). Available online: https://sdgs.un.org/goals/goal3 (accessed on 4 January 2022).
- Rothkopf, D.J. When the Buzz Bites Back. Available online: https://www.washingtonpost.com/archive/opinions/2003/05/11/when-the-buzz-bites-back/bc8cd84f-cab6-4648-bf58-0277261af6cd/ (accessed on 12 January 2022).
- Pautasso, M. Ten simple rules for writing a literature review. PLoS Comput. Biol. 2013, 9, e1003149. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W. Narrative Research. In Qualitative Inquiry & Research Design: Choosing among Five Approaches; Sage: Washington, DC, USA, 2021; pp. 70–76. [Google Scholar]
- Creswell, J.W. Phenomenological Research. In Qualitative Inquiry & Research Design: Choosing among Five Approaches; Sage: Washington, DC, USA, 2021; pp. 76–83. [Google Scholar]
- Kano, M.; Wood, M.M.; Siegel, J.M.; Bourque, L.B. Disaster Research and Epidemiology. In Koenig’s and Schultz’s Disaster Medicine: Principles and Practice; Koenig, K.L., Schultz, C.H., Eds.; Cambridge University Press: New York, NY, USA, 2010; pp. 3–20. [Google Scholar]
- La Bella, E.; Allen, C.; Lirussi, F. Communication vs evidence: What hinders the outreach of science during an infodemic? A narrative review. Integr. Med. Res. 2021, 10, 100731. [Google Scholar] [CrossRef] [PubMed]
- Mheidly, N.; Fares, J. Leveraging media and health communication strategies to overcome the COVID-19 infodemic. J. Public Health Policy 2020, 41, 410–420. [Google Scholar] [CrossRef]
- Abbott, R.; Bethel, A.; Rogers, M.; Whear, R.; Orr, N.; Shaw, L.; Stein, K.; Coon, J.T. Characteristics, quality and volume of the first 5 months of the COVID-19 evidence synthesis infodemic: A meta-research study. BMJ Evid.-Based Med. 2021. [Google Scholar] [CrossRef]
- Larson, H.J. A call to arms: Helping family, friends and communities navigate the COVID-19 infodemic. Nat. Rev. Immunol. 2020, 20, 449–450. [Google Scholar] [CrossRef]
- Topf, J.M.; Williams, P.N. COVID-19, Social Media, and the Role of the Public Physician. Blood Purif. 2021, 50, 595–601. [Google Scholar] [CrossRef]
- Tentolouris, A.; Ntanasis-Stathopoulos, I.; Vlachakis, P.K.; Tsilimigras, D.I.; Gavriatopoulou, M.; Dimopoulos, M.A. COVID-19: Time to flatten the infodemic curve. Clin. Exp. Med. 2021, 21, 161–165. [Google Scholar] [CrossRef]
- Loss, J.; Boklage, E.; Jordan, S.; Jenny, M.A.; Weishaar, H.; El Bcheraoui, C. Risk communication in the containment of the COVID-19 pandemic: Challenges and promising approaches. Bundesgesundh. Gesundh. Gesundh. 2021, 64, 294–303. [Google Scholar] [CrossRef]
- Anwar, A.; Malik, M.; Raees, V.; Anwar, A. Role of Mass Media and Public Health Communications in the COVID-19 Pandemic. Cureus 2020, 12, e10453. [Google Scholar] [CrossRef]
- U.S. Surgeon General. Confronting Health Misinformation: The U.S. Surgeon General’s Advisory on Building a Healthy Information Environment. Available online: https://www.ncbi.nlm.nih.gov/books/NBK572169/ (accessed on 7 January 2022).
- Magarini, F.M.; Pinelli, M.; Sinisi, A.; Ferrari, S.; De Fazio, G.L.; Galeazzi, G.M. Irrational Beliefs about COVID-19: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 9839. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.P.; Kute, V.B.; Agarwal, S.K. “Infodemic” COVID 19: More Pandemic than the Virus. Indian J. Nephrol. 2020, 30, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Sasidharan, S.; Singh, D.H.; Vijay, S.; Manalikuzhiyil, B. COVID-19: Pan(info)demic. Turk. J. Anaesthesiol. Reanim. 2020, 48, 438–442. [Google Scholar] [CrossRef]
- Lv, J.; Su, Y.; Song, L.; Gong, X.; Peng, Y. Stem cell ‘therapy’ advertisements in China: Infodemic, regulations and recommendations. Cell Prolif. 2020, 53, e12937. [Google Scholar] [CrossRef] [PubMed]
- Diethelm, P.; McKee, M. Denialism: What is it and how should scientists respond? Eur. J. Public Health 2009, 19, 2–4. [Google Scholar] [CrossRef] [Green Version]
- Sharma, D.C.; Pathak, A.; Chaurasia, R.N.; Joshi, D.; Singh, R.K.; Mishra, V.N. Fighting infodemic: Need for robust health journalism in India. Diabetes Metab. Syndr. 2020, 14, 1445–1447. [Google Scholar] [CrossRef]
- Rocha, Y.M.; de Moura, G.A.; Desidério, G.A.; de Oliveira, C.H.; Lourenço, F.D.; de Figueiredo Nicolete, L.D. The impact of fake news on social media and its influence on health during the COVID-19 pandemic: A systematic review. Z. Gesundh. Wiss. 2021. [Google Scholar] [CrossRef]
- Bin Naeem, S.; Kamel Boulos, M.N. COVID-19 Misinformation Online and Health Literacy: A Brief Overview. Int. J. Environ. Res. Public Health 2021, 18, 8091. [Google Scholar] [CrossRef]
- Gabarron, E.; Oyeyemi, S.O.; Wynn, R. COVID-19-related misinformation on social media: A systematic review. Bull. World Health Organ. 2021, 99, 455–463a. [Google Scholar] [CrossRef]
- Rathore, F.A.; Farooq, F. Information Overload and Infodemic in the COVID-19 Pandemic. JPMA J. Pak. Med. Assoc. 2020, 70 (Suppl. 3), S162–S165. [Google Scholar] [CrossRef]
- Chowdhury, N.; Khalid, A.; Turin, T.C. Understanding misinformation infodemic during public health emergencies due to large-scale disease outbreaks: A rapid review. Z. Gesundh. Wiss. 2021. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.J.; Larson, H.; Dubé, È.; Fisher, A. Vaccine Hesitancy: Drivers and How the Allergy Community Can Help. J. Allergy Clin. Immunol. Pract. 2021, 9, 3568–3574. [Google Scholar] [CrossRef] [PubMed]
- Abrams, E.M.; Shaker, M.; Oppenheimer, J.; Davis, R.S.; Bukstein, D.A.; Greenhawt, M. The Challenges and Opportunities for Shared Decision Making Highlighted by COVID-19. J. Allergy Clin. Immunol. Pract. 2020, 8, 2474–2480. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- Khan, S.; Siddique, R.; Wang, X.; Zhang, R.; Nabi, G.; Sohail Afzal, M.; Liu, J.; Xue, M. Mental health consequences of infections by coronaviruses including severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Brain Behav. 2021, 11, e01901. [Google Scholar] [CrossRef]
- Zhu, Z.; Lian, X.; Su, X.; Wu, W.; Marraro, G.A.; Zeng, Y. From SARS and MERS to COVID-19: A brief summary and comparison of severe acute respiratory infections caused by three highly pathogenic human coronaviruses. Respir. Res. 2020, 21, 224. [Google Scholar] [CrossRef]
- Mahajan, A.; Manchikanti, L. Value and Validity of Coronavirus Antibody Testing. Pain Physician 2020, 23, S381–S390. [Google Scholar] [CrossRef]
- Bórquez, P.B.; Luengo-Charath, M.X.; Anguita, M.V.; Bascuñán, R.M.; Pacheco, M.I.; Michaud Ch, P.; Vacarezza, Y.R. The responsible use and dissemination of information in a pandemic: An ethical imperative. Rev. Chil. Pediatr. 2020, 91, 794–799. [Google Scholar] [CrossRef]
- Storeng, K.T.; de Bengy Puyvallée, A. The Smartphone Pandemic: How Big Tech and public health authorities partner in the digital response to COVID-19. Glob. Public Health 2021, 16, 1482–1498. [Google Scholar] [CrossRef]
- Choi, H.; Jeong, G. Characteristics of the Measurement Tools for Assessing Health Information-Seeking Behaviors in Nationally Representative Surveys: Systematic Review. J. Med. Internet Res. 2021, 23, e27539. [Google Scholar] [CrossRef]
- Chow, N.; Hogg-Johnson, S.; Mior, S.; Cancelliere, C.; Injeyan, S.; Teodorczyk-Injeyan, J.; Cassidy, J.D.; Taylor-Vaisey, A.; Côté, P. Assessment of Studies Evaluating Spinal Manipulative Therapy and Infectious Disease and Immune System Outcomes: A Systematic Review. JAMA Netw. Open 2021, 4, e215493. [Google Scholar] [CrossRef] [PubMed]
- Vériter, S.L.; Bjola, C.; Koops, J.A. Tackling COVID-19 Disinformation: Internal and External Challenges for the European Union. Hague J. Dipl. 2020, 15, 569–582. [Google Scholar] [CrossRef]
Figure 1.
Literature search strategy flow chart. Two databases (Pubmed and Cochrane Library) were considered. The search in the Cochrane Library revealed no results.
Figure 1.
Literature search strategy flow chart. Two databases (Pubmed and Cochrane Library) were considered. The search in the Cochrane Library revealed no results.

Figure 2.
Spatio-temporal mapping of scientific review publications on infodemic in the COVID-19 pandemic (N = 32, close of database: 29 October 2021). Top: first authors’ countries of affiliation; bottom: publication dates of reviews.
Figure 2.
Spatio-temporal mapping of scientific review publications on infodemic in the COVID-19 pandemic (N = 32, close of database: 29 October 2021). Top: first authors’ countries of affiliation; bottom: publication dates of reviews.


Figure 3.
Mechanistic factors, described in reviews, of the infodemic during the COVID-19 pandemic.

Figure 4.
Impact of the COVID-19 infodemic.

Figure 5.
Measures to confront the infodemic by phase of disaster cycle.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Cluster matrix of literature analysis.
| Mechanisms of the Infodemic | Situation factors |
| Sender factors | |
| Instrument factors | |
| Recipient factors | |
| Impact of the Infodemic | Stress |
| Deception | |
| Violence | |
| Harm | |
| Measures to Confront the Infodemic by Phase of Disaster Cycle # | Pre-impact |
| Trans-impact | |
| Post-impact |
# The three-phase disaster cycle was defined as in [13]. In bold: main clusters; in regular font: subclusters
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ries, M. The COVID-19 Infodemic: Mechanism, Impact, and Counter-Measures—A Review of Reviews. Sustainability 2022, 14, 2605. https://doi.org/10.3390/su14052605
AMA Style
Ries M. The COVID-19 Infodemic: Mechanism, Impact, and Counter-Measures—A Review of Reviews. Sustainability. 2022; 14(5):2605. https://doi.org/10.3390/su14052605
Chicago/Turabian StyleRies, Markus. 2022. "The COVID-19 Infodemic: Mechanism, Impact, and Counter-Measures—A Review of Reviews" Sustainability 14, no. 5: 2605. https://doi.org/10.3390/su14052605
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.