

Association between Sugar Intake and an ECG Parameter: A Case Study on Young Athletes
Abstract
:1. Introduction and Background
1.1. Risks of Sugar
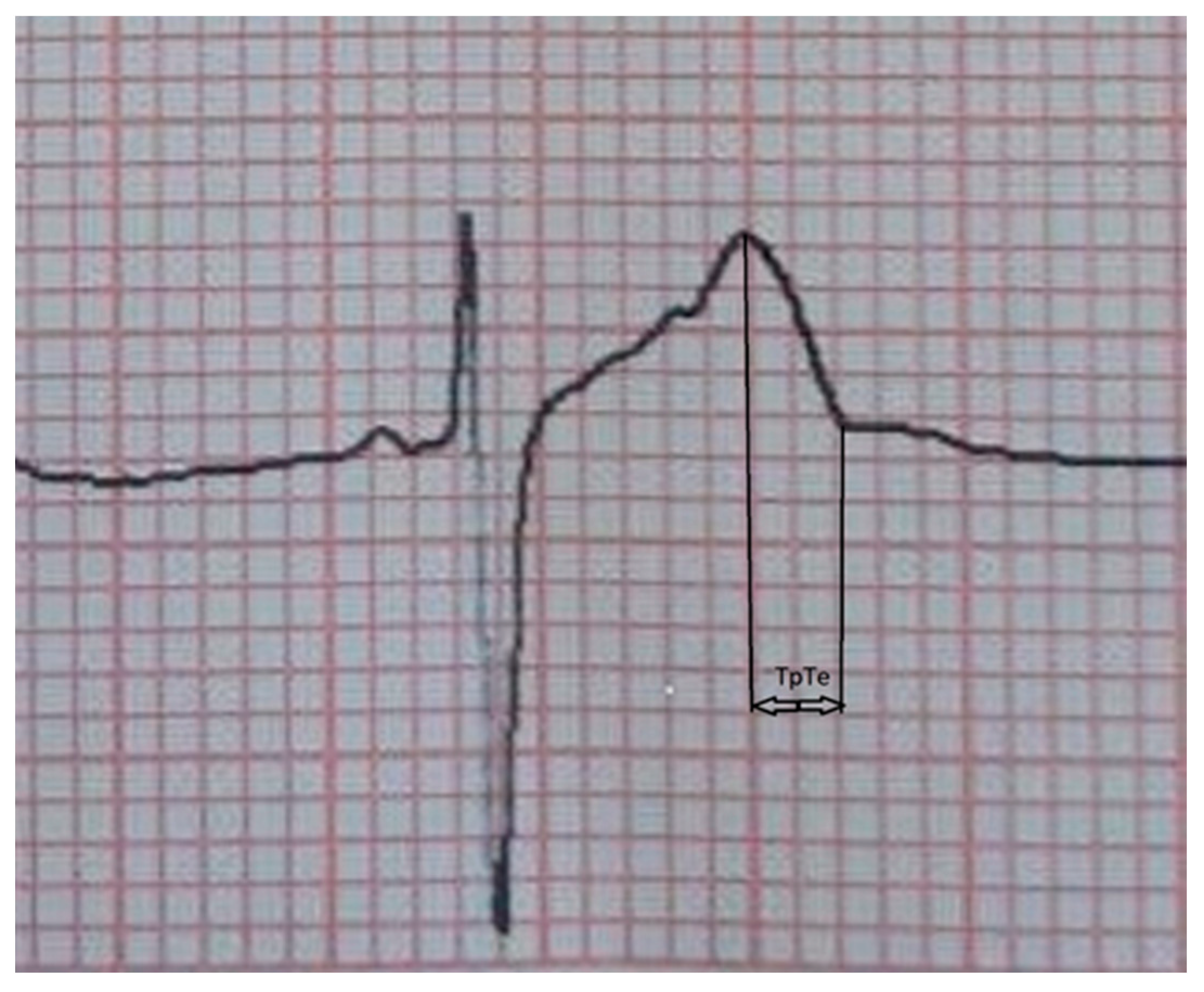
1.2. Tp-Te Duration, an ECG Parameter
1.3. Aims of the Study
2. Materials and Methods
2.1. Participants of the Study
2.2. Description of Procedures
2.3. Statistical Procedures
3. Results
4. Discussion
4.1. Implemented Measures to Reduce Sugar Intake, Primarily in the EU Countries
4.2. Public Policies in Serbia
4.3. Limitations of the Study
5. Recommendations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Di Nicolantonio, J.J.; Lucan, S.C. The wrong white crystals: Not salt but sugar as aetiological in hypertension and cardiometabolic disease. Open Heart 2014, 1, e000167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Q.; Zhang, Z.; Gregg, E.W.; Flanders, W.D.; Merritt, R.; Hu, F.B. Added sugar intake and cardiovascular diseases mortality among US adults. JAMA Intern. Med. 2014, 174, 516–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; Van Horn, L.V.; Feig, D.I.; Anderson, C.A.M.; Patel, M.J.; Cruz Munos, J.; Krebs, N.F.; Xanthakos, S.A.; et al. Added Sugars and Cardiovascular Disease Risk in Children: A Scientific Statement FROM the American Heart Association. Circulation 2017, 135, e1017–e1034. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Diani, L.; Forchielli, M.L. Sugar Intake: Are All Children Made of Sugar? Life 2021, 11, 444. [Google Scholar] [CrossRef]
- Cheng, W.L.; Li, S.J.; Lee, T.I.; Lee, T.W.; Chung, C.C.; Kao, Y.H.; Chen, Y.J. Sugar Fructose Triggers Gut Dysbiosis and Metabolic Inflammation with Cardiac Arrhythmogenesis. Biomedicines 2021, 9, 728. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, L.; Imamura, F.; Brage, S.; Griffin, S.J.; Wareham, N.J.; Forouhi, N.G. Intakes and sources of dietary sugars and their association with metabolic and inflammatory markers. Clin. Nutr. 2018, 37, 1313–1322. [Google Scholar] [CrossRef] [Green Version]
- Della Corte, K.W.; Perrar, I.; Penczynski, K.J.; Schwingshackl, L.; Herder, C.; Buyken, A.E. Effect of Dietary Sugar Intake on Biomarkers of Subclinical Inflammation: A Systematic Review and Meta-Analysis of Intervention Studies. Nutrients 2018, 10, 606. [Google Scholar] [CrossRef] [Green Version]
- Cao, M.; Zhu, Y.; Chen, Y.; Jing, J. Sugar-Sweetened Beverages and Symptom Complaints among School-Aged Children: A National Longitudinal Study. Nutrients 2022, 14, 406. [Google Scholar] [CrossRef]
- Lang, T.; Schoen, V.; Hashem, K.; McDonald, L.; Parker, J.; Savelyeva, A. Chapter Five—The Environmental, Social, and Market Sustainability of Sugar. In Advances in Food Security and Sustainability; David, B., Ed.; Elsevier: Amsterdam, The Netherlands, 2017; Volume 2, pp. 115–136. [Google Scholar]
- Antzelevitch, C. Role of spatial dispersion of repolarization in inherited and acquired sudden cardiac death syndromes. American Journal of Physiology. Heart Circ. Physiol. 2007, 293, H2024–H2038. [Google Scholar] [CrossRef] [Green Version]
- Bieganowska, K.; Sawicka-Parobczyk, M.; Bieganowski, M.; Piskorski, J. T peak-t end interval in 12-lead electrocardiogram of healthy children and adolescents t-peak -t-end interval in childhood. Ann. Noninvasive Electrocardiol. 2013, 18, 344–351. [Google Scholar] [CrossRef]
- Jaromin, J.; Markiewicz-Łoskot, G.; Szydłowski, L.; Kulawik, A. Diagnostic Value of the TpTe Interval in Children with Ventricular Arrhythmias. Int. J. Env. Res. Public Health 2021, 18, 12194. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.cdc.gov/growthcharts/data/set1clinical/cj41l023.pdf (accessed on 7 June 2022).
- Boraita, A.; Heras, M.E.; Morales, F.; Marina-Breysse, M.; Canda, A.; Rabadan, M.; Barriopedro, M.I.; Varela, A.; de la Rosa, A.; Tuñón, J. Reference Values of Aortic Root in Male and Female White Elite Athletes According to Sport. Circ. Cardiovasc. Imaging 2016, 9, e005292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inanir, M.; Sincer, I.; Erdal, E.; Gunes, Y.; Cosgun, M.; Mansiroglu, A.K. Evaluation of electrocardiographic ventricular repolarization parameters in extreme obesity. J. Electrocardiol. 2019, 53, 36–39. [Google Scholar] [CrossRef]
- Turgay Yıldırım, Ö.; Kaya, Ş.; Baloğlu Kaya, F. Evaluation of the Tp-e interval and Tp-e/QTc ratio in patients with benign paroxysmal positional vertigo in the emergency department compared with the normal population. J. Electrocardiol. 2020, 58, 51–55. [Google Scholar] [CrossRef]
- Yilmaz, E.; Aydin, E. The effect of low iron storage without Anaemia on electrocardiography. J. Electrocardiol. 2021, 64, 76–79. [Google Scholar] [CrossRef]
- Cordeiro, R.; Karimian, N.; Park, Y. Hyperglycemia Identification Using ECG in Deep Learning Era. Sensors 2021, 21, 6263. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.L.; Su, S.; Nguyen, H.T. Neural network approach for non-invasive detection of hyperglycemia using electrocardiographic signals. In Proceedings of the 36th Annual International Conference of the IEEE Engineering in Medicine and BiologySociety, Chicago, IL, USA, 26–30 August 2014; pp. 4475–4478. [Google Scholar]
- Vézina-Im, L.-A.; Beaulieu, D.; Bélanger-Gravel, A.; Boucher, D.; Sirois, C.; Dugas, M.; Provencher, V. Efficacy of school-based interventions aimed at decreasing sugar-sweetened beverage consumption among adolescents: A systematic review. Public Health Nutr. 2017, 20, 2416–2431. [Google Scholar] [CrossRef] [Green Version]
- Hawkes, C.; Jewell, J.; Allen, K. A Food Policy Package for Healthy Diets and the Prevention of Obesity and Diet-Related Non-communicable Diseases: The NOURISHING Framework. Obes. Rev. 2013, 14 (Suppl. S2), 159–168. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund. World Cancer Research Fund International NOURISHING and MOVING Policy Database. 2022. Available online: https://policydatabase.wcrf.org/ (accessed on 21 April 2022).
- Kirkpatrick, S.I.; Raffoul, A.; Maynard, M.; Lee, K.M.; Stapleton, J. Gaps in the Evidence on Population Interventions to Reduce Consumption of Sugars: A Review of Reviews. Nutrients 2018, 10, 1036. [Google Scholar] [CrossRef] [Green Version]
- Bucher Della Torre, S.; Moullet, C.; Jotterand Chaparro, C. Impact of Measures Aiming to Reduce Sugars Intake in the General Population and Their Implementation in Europe: A Scoping Review. Int. J. Public Health 2022, 66, 1604108. [Google Scholar] [CrossRef]
- Djordjic, V.; Radisavljevic, S.; Milanovic, I.; Bozic, P.; Grbic, M.; Jorga, J.; Ostojic, S.M. WHO European Childhood Obesity Surveillance Initiative in Serbia: A prevalence of overweight and obesity among 6–9-year-old school children. J. Pediatr. Endocrinol. Metab. 2016, 29, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Bozic, P.; Djordjic, V.; Markovic, L.; Cvejic, D.; Trajkovic, N.; Halasi, S.; Ostojic, S. Dietary Patterns and Weight Status of Primary School Children in Serbia. Front. Public Health 2021, 15, 678346. [Google Scholar] [CrossRef]
- Nittari, G.; Scuri, S.; Petrelli, F.; Pirillo, I.; di Luca, N.M.; Grappasonni, I. Fighting obesity in children from European World Health Organization member states. Epidemiological data, medical-social aspects, and prevention programs. Clin. Ter. 2019, 170, e223–e230. [Google Scholar]
- Rule book on closer conditions for organizing, achieving, and monitoring the nutrition of students in primary school. Off. Gazette RS 2018, 68, 28. (In Serbian)
- Rulebook on closer conditions and manner of achieving children’s nutrition in a preschool institution. Off. Gazette RS 2018, 39, 24. (In Serbian)
- #STRENGTH2FOOD: Food Quality for Sustainability and Health. Available online: https://www.strength2food.eu/ (accessed on 21 April 2022).


{kind=link}
| The Group with Sugar Intake | The Group without Sugar Intake | t-Test, Mann–Whitney Test, or Chi-Squared Test p-Value | |
|---|---|---|---|
| Sex | 0.06 | ||
| Male: 62 (65%) | 32 (52%) | 30 (48%) | |
| Female: 34 (35%) | 12 (35%) | 22 (65%) | |
| Age, years | 10.68 ± 2.11 | 10.17 ± 1.97 | 0.63 |
| Training hours per week | 3.55 ± 1.02 | 3.21 ± 0.69 | 0.18 |
| Years of training (years) | 3.43 ± 1.61 | 3.29 ± 1.64 | 0.60 |
| Height (cm) | 152.25 ± 15.24 | 146.08 ± 14.62 | 0.07 |
| Weight (kg) | 47.45 ± 16.88 | 39.44 ± 10.92 | 0.02 * |
| Weight status 0.06 | |||
| Normal weight 25 (39%) 39 (61%) | |||
| 64 (67%) | |||
| Overweight or obese 19 (59%) 13 (41%) | |||
| 32 (33%) | |||
| Type of sport 0.46 | |||
| IB 15 (16%) 4 (27%) 11 (73%) | |||
| IC 17 (18%) 9 (53%) 8 (47%) | |||
| IIC 36 (37%) 17 (47%) 19 (53%) | |||
| IIIA 22 (23%) 10 (45%) 12 (55%) | |||
| IIIC 6 (6%) 4 (66%) 2 (33%) | |||
| TpTe (ms) | 73 ± 8 ms | 60 ± 8 ms | p < 0.001 ** |
| TpTe | |
|---|---|
| Age, years | r = 0.16 |
| Sex | r = 0.19 |
| Height (cm) | r = 0.20 |
| Weight (kg) | r = 0.29 |
| Weight status | r = 0.13 |
| Training hours per week | r = 0.08 |
| Years of training (years) | r = 0.07 |
| Sugar intake | r = 0.63 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šarčević, Z.; Lužanin, Z.; Tepavčević, A. Association between Sugar Intake and an ECG Parameter: A Case Study on Young Athletes. Sustainability 2022, 14, 14916. https://doi.org/10.3390/su142214916
Šarčević Z, Lužanin Z, Tepavčević A. Association between Sugar Intake and an ECG Parameter: A Case Study on Young Athletes. Sustainability. 2022; 14(22):14916. https://doi.org/10.3390/su142214916
Chicago/Turabian StyleŠarčević, Zoran, Zorana Lužanin, and Andreja Tepavčević. 2022. "Association between Sugar Intake and an ECG Parameter: A Case Study on Young Athletes" Sustainability 14, no. 22: 14916. https://doi.org/10.3390/su142214916