

What Do We Know about the Use of the Walk-along Method to Identify the Perceived Neighborhood Environment Correlates of Walking Activity in Healthy Older Adults: Methodological Considerations Related to Data Collection—A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Data Sources and Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction
3. Results
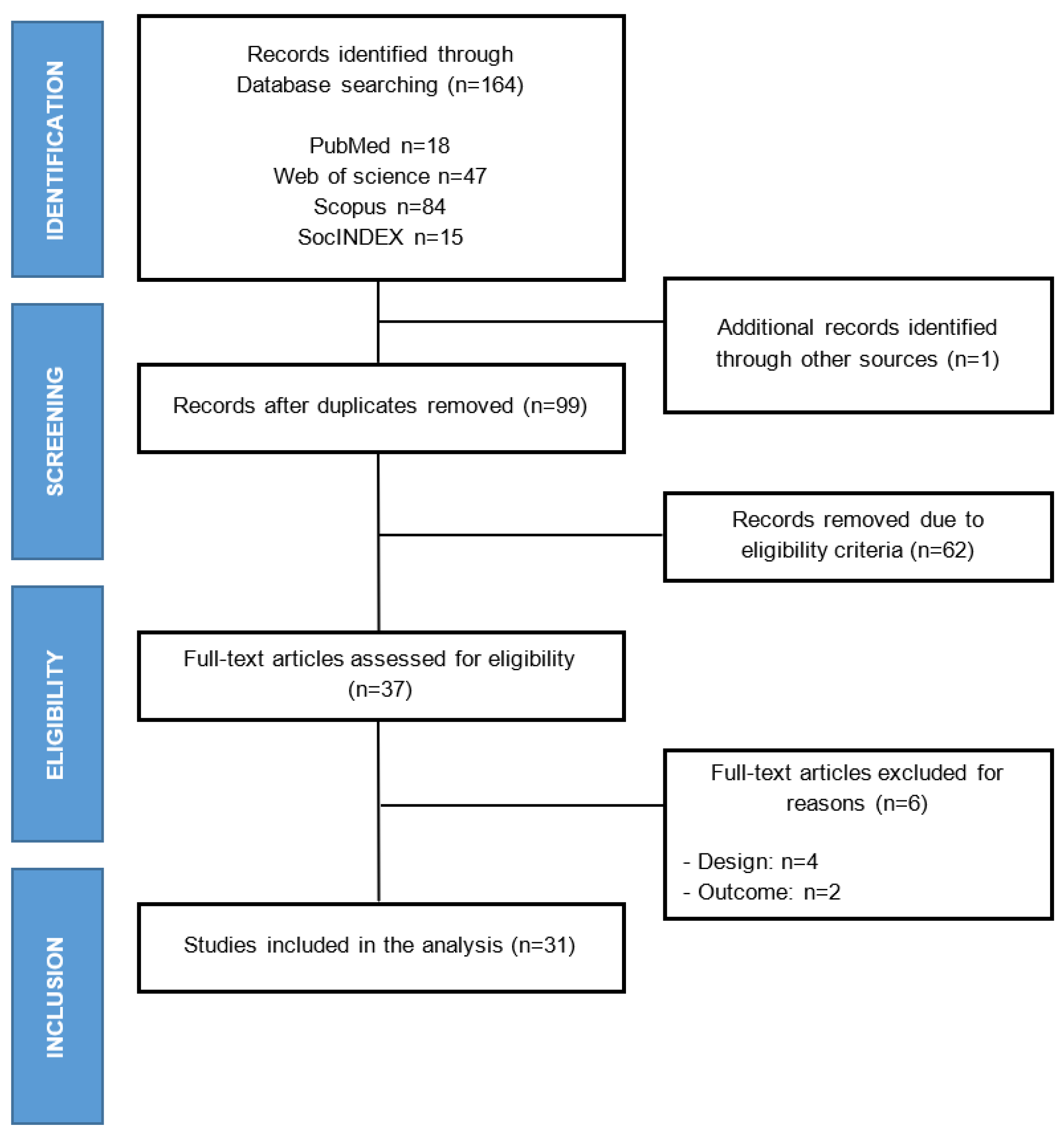
3.1. Study Selection
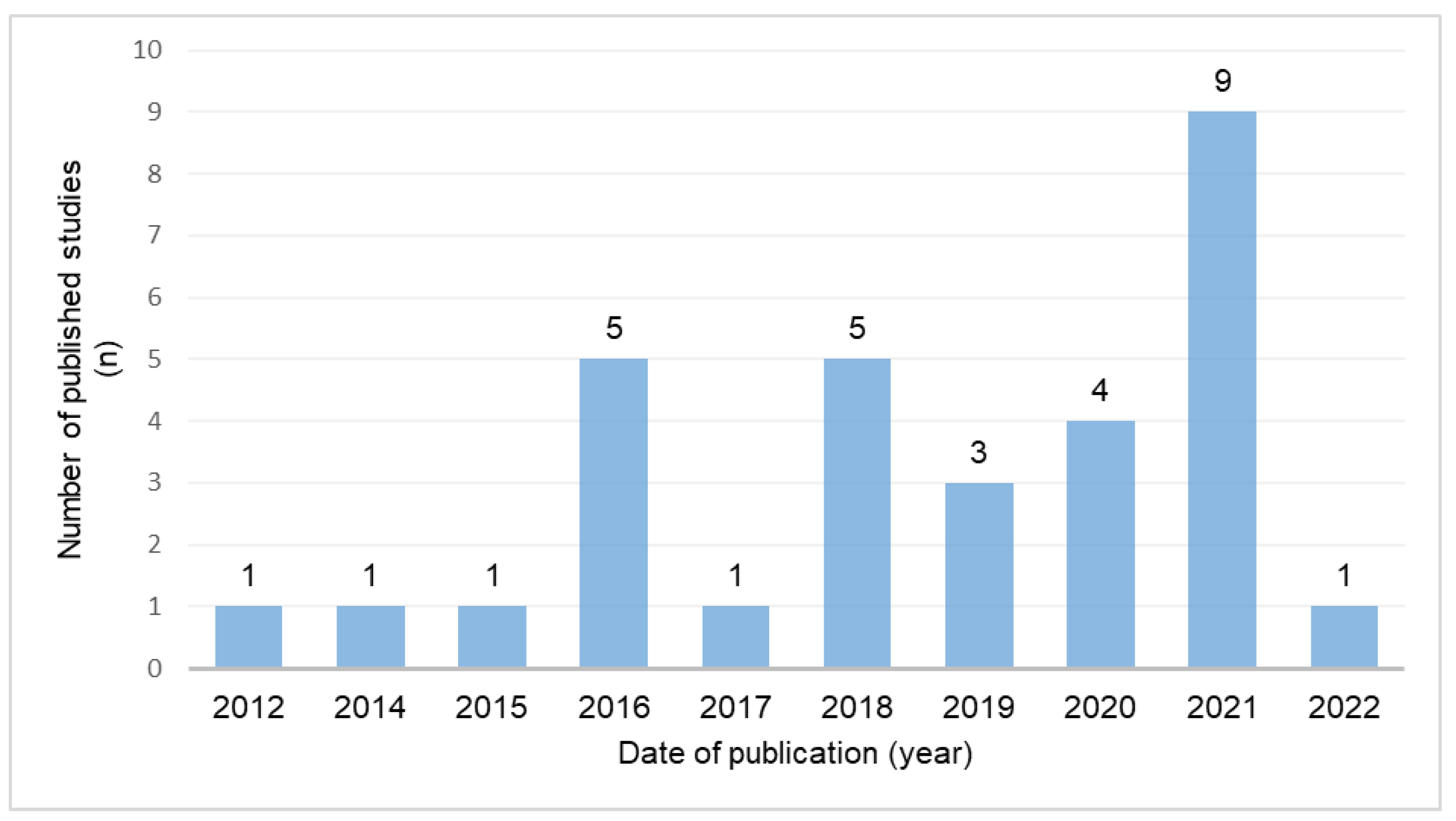
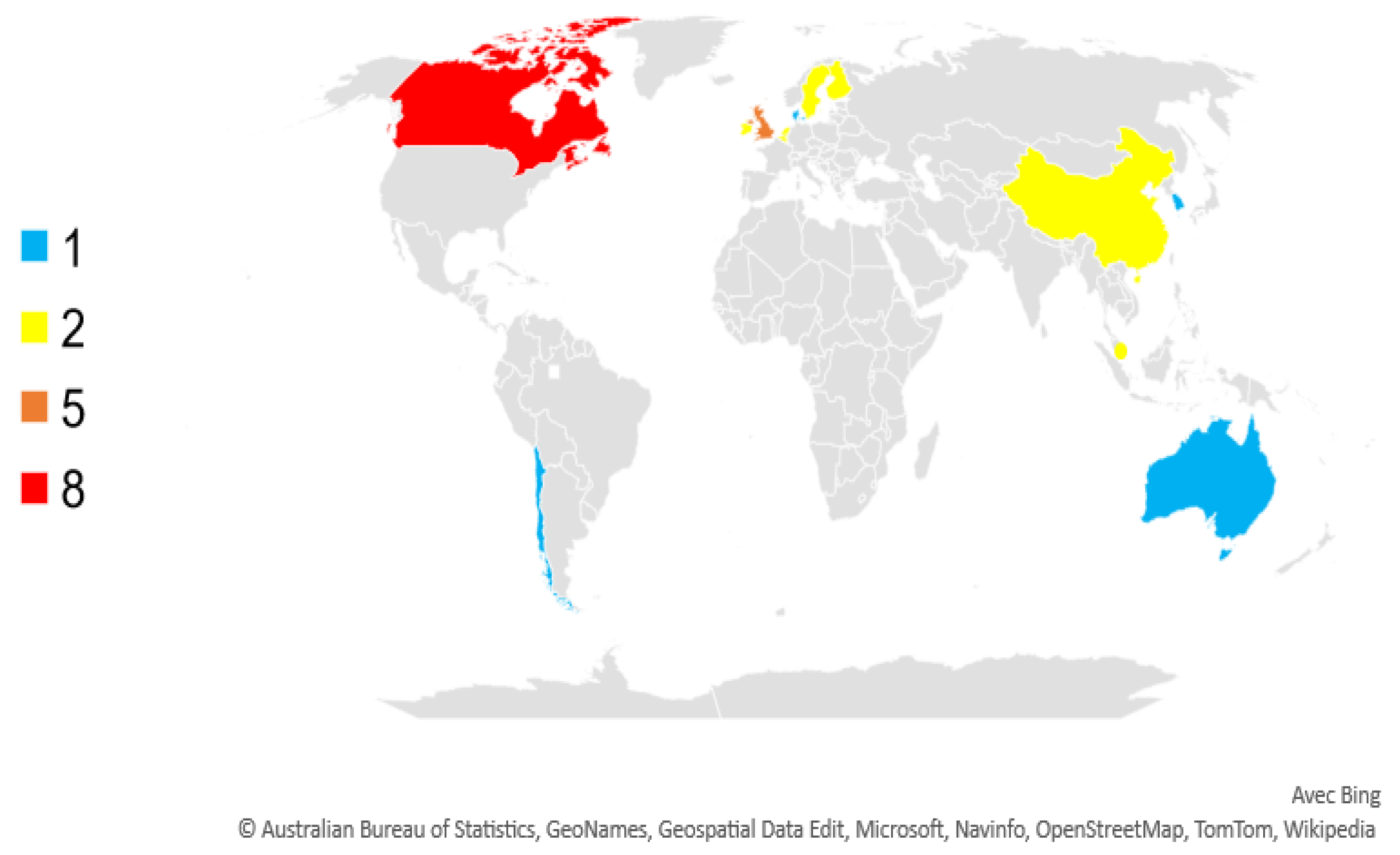
3.2. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Publication Year | Country | Title | Journal | Funding |
|---|---|---|---|---|---|
| Močnik et al. [9] | 2022 | Singapore | Exploring facilitators and barriers of older adults’ outdoor mobility: A walk-along study in Singapore. | Journal of Transport & Health | This research is supported by Singapore’s Ministry of National Development and National Research Foundation under the L2NIC Award No L2NICTDF1-2017-2. Any opinions, findings and conclusions or recommendations expressed in this material are those of the authors and do not reflect the views of Singapore’s Ministry of National Development and National Research Foundation. |
| Lauwers et al. [59] | 2021 | Belgium | Exploring how the urban neighborhood environment influences mental well-being using walking interviews. | Health and Place | This work was supported by the Belgian Federal Science Policy Office (BELSPO) [grant number BR/175/A3/NAMED]. |
| Herrmann-Lunecke et al. [60] | 2021 | Chile | Perception of the built environment and walking in pericentral neighbourhoods in Santiago, Chile. | Journal of Aging and Physical Activity | This work was supported by ANID under grant Fondecyt Regular No. 1200527 and by CONICYT under grant Fondecyt Regular No. 1170292. |
| Grove [61] | 2021 | Ireland | Ageing as Well as You Can in Place: Applying a Geographical Lens to the Capability Approach. | Social Science & Medicine | This research was funded by the Health Research Board in Ireland (SPHeRE/2013/1). |
| Sun and Lau [62] | 2021 | China | Go-along with older people to public transport in high-density cities: Understanding the concerns and walking barriers through their lens. | Journal of Transport & Health | This research is supported by Research Grants Council (RGC) of Hong Kong No. 17600818. |
| Lager et al. [35] | 2021 | The Netherlands | Neighbourhood walks as place-making in later life. | Social & Cultural Geography | Not mentioned. |
| Kou et al. [36] | 2021 | China | Physical environmental factors influencing older adults’ park use: A qualitative study. | Urban Forestry & Urban Greening | This work was supported by the Economic & Social Research Council as part of the wider Healthy Urban Living and Ageing in Place (HULAP) Project [ES/N013336/1, 2016]. Ruibing Kou was supported by the Chinese Scholarship Council No. 201606370019. |
| Hand et al. [10] | 2021 | Canada | Applying the Go-along Method to Enhance Understandings of Occupation in Context. | Journal of Occupational Science | This work was supported by the Social Science and Humanities Research Council of Canada under No. 435-2018-1440. |
| Saint-Onge et al. [8] | 2021 | Canada | Older Public Housing Tenants’ Capabilities for Physical Activity Described Using Walk-along Interviews in Montreal, Canada. | International Journal of Environmental Research and Public Health | The main author received a doctoral research scholarship from the FRQ-SC during this study. |
| Li and Woolrych. [58] | 2021 | U.K. | Experiences of Older People and Social Inclusion in Relation to Smart “Age-Friendly” Cities: A Case Study of Chongqing, China. | Frontiers in Public Health | This study was supported by The School of Energy, Geoscience, Infrastructure and Society (EGIS) at Heriot-Watt University. |
| Veitch et al. [7] | 2020 | Australia | Designing parks for older adults: A qualitative study using walk-along interviews. | Urban Forestry & Urban Greening | This research was funded by an Australian Research Council Discovery Project (No. DP170100188). JV is supported by a Future Leader Fellowship from the National Heart Foundation of Australia (ID 101928). |
| Carroll et al. [55] | 2020 | Denmark | Going along with older people: exploring age-friendly neighbourhood design through their lens. | Journal of Housing and the Built Environment | This research was supported by Områdefornyelsen Sydhavnen, The Danish Foundation for Culture and Sports Facilities, The Velux Foundations, and TrygFonden. |
| Hand. [56] | 2020 | Canada | Older Women’s Engagement in Community Occupations: Considerations of Lifespan and Place. | Scandinavian Journal of Occupational Therapy | The author gratefully acknowledges funding from the Social Sciences and Humanities Research Council of Canada. |
| Sundevall and Jansson [57] | 2020 | Sweden | Inclusive Parks across Ages: Multifunction and Urban Open Space Management for Children, Adolescents, and the Elderly. | International Journal of Environmental Research and Public Health | This research was funded by Stiftelsen Carl-Fredrik von Horns fond and Stiftelsen Fonden för markvård till minne av Sanders Alburg through The Royal Swedish Academy of Agriculture and Forestry (KSLA). |
| Cao et al. [6] | 2019 | Singapore | Using Walk-Along Interviews to Identify Environmental Factors Influencing Older Adults’ Out-of-Home Behaviors in a High-Rise, High-Density Neighborhood. | International Journal of Environmental Research and Public Health | This research received no external funding. |
| Macintyre et al. [25] | 2019 | England | I Would Never Come Here Because I’ve Got My Own Garden”: Older Adults’ Perceptions of Small Urban Green Spaces. | International Journal of Environmental Research and Public Health | This research was funded as part of the GHIA project by the Natural Environment Research Council, the Arts and Humanities Research Council and the Economic and Social Research Council under the Valuing Nature Programme, grant number NE/N013530/1. J.S.B. |
| Cassarino et al. [54] | 2019 | Ireland | Cognitive and Sensory Dimensions of Older People’s Preferences of Outdoor Spaces for Walking: A Survey Study in Ireland. | International Journal of Environmental Research and Public Health | This research received no external funding. This work was partially supported by Seed Award funding granted by the School of Applied Psychology, University College Cork, Ireland. |
| Thandi et al. [38] | 2018 | Canada | Engaging Older Men in Physical Activity: Implications for Health Promotion Practice. | American Journal of Men’s Health | The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research (Ref. Number 138295). Writing up of this work was partly funded by Movember Canada (No. 11R18455). |
| Lee and Dean. [30] | 2018 | Canada | Perceptions of Walkability and Determinants of Walking Behaviour among Urban Seniors in Toronto, Canada. | Journal of Transport & Health | Not mentioned. |
| Hand et al. [23] | 2018 | Canada | Toward Understanding Person-Place Transactions in Neighborhoods: A Qualitative-Participatory Geospatial Approach. | Gerontologist | This study was supported by the Social Science and Humanities Research Council (No. 430-2015-00618). |
| Suopajärvi [37] | 2018 | Finland | From Tar City to Smart City Living with the Smart City Ideology as a Senior City Dweller. | Ethnologia Fennica | This article is based on research projects that were funded by the Academy of Finland No. 258570 and No. 132847. |
| Nordin et al. [53] | 2018 | Sweden | The physical environment, activity and interaction in residential care facilities for older people: a comparative case study. | Scandinavian Journal of Caring Sciences | The School of Education, Health and Social Studies at Dalarna University supported this study. |
| Zandieh et al. [52] | 2017 | The Netherlands | Do Inequalities in Neighborhood Walkability Drive Disparities in Older Adults’ Outdoor Walking? | International Journal of Environmental Research and Public Health | This research was financially supported by Erasmus Mundus scholarship supplied by the European Union. |
| Luusua et al. [32] | 2016 | Finland | Northern Urban Lights: Emplaced Experiences of Urban Lighting as Digital Augmentation. | Architecture and interaction: Human computer interaction | We would like to thank our participants, the Academy of Finland for their support of the UBI Metrics and the Adaptive Urban Lighting projects, as well as the Nokia Foundation for their support. |
| Ottoni et al. [49] | 2016 | Canada | Benches become like porches”: The built and social environment’s influence on older adults experiences’ of mobility and well-being. | Social Science & Medicine | Not mentioned. |
| Curl et al. [50] | 2016 | U.K. | Developing an Audit Checklist to Assess Outdoor Falls Risk. | Proceedings of the Institution of Civil Engineers: Urban Design and Planning | This research was funded through the Medical Research Council (grant reference G1002782/1) as part of the Lifelong Health and Well-being (LLHW) Cross-Council Programme. The LLHW Funding Partners are: Arts and Humanities Research Council, Biotechnology and Biological Sciences Research Council, Engineering and Physical Sciences Research Council, Economic and Social Research Council, Medical Research Council, Chief Scientist Office of the Scottish Government Health Directorates, National Institute for Health Research/The Department of Health, The Health and Social Care Research and Development of the Public Health Agency (Northern Ireland), Wales Office of Research and Development for Health and Social Care, and the Welsh Assembly Government. The LLHW programme and funding partners had no role in the design, collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to submit the manuscript for publication. |
| Yoo and Kim [46] | 2016 | Republic of Korea | Perceived urban neighborhood environment for physical activity of older adults in Seoul, Korea: A multimethod qualitative study. | Preventive Medicine | This work was supported by the 2014 SNU Brain Fusion Program of the Seoul National University (SNU Project No. 0434-20140016) and the Korea Health Promotion Foundation Research Grant (15-08). |
| Zandieh et al. [51] | 2016 | England | Older Adults’ Outdoor Walking: Inequalities in Neighbourhood Safety, Pedestrian Infrastructure and Aesthetics. | International Journal of Environmental Research and Public Health | This research was financially supported by Erasmus Mundus scholarship supplied by the European Union. |
| Lager et al. [48] | 2015 | The Netherlands | Understanding older adults’ social capital in place: Obstacles to and opportunities for social contacts in the neighbourhood. | Geoforum | This research would not have been possible without the financial support of the Ubbo Emmius Fund. |
| Gardner [47] | 2014 | Canada | The role of social engagement and identity in community mobility among older adults aging in place. | Disability and Rehabilitation | Not mentioned. |
| Van Cauwenberg et al. [5] | 2012 | Belgium | Environmental factors influencing older adults’ walking for transportation: a study using walk-along interviews. | International Journal of Behavioral Nutrition and Physical Activity | Not mentioned. |
3.3. Participant Characteristics
3.4. Walk-along Interview: Data Collection Method
3.4.1. Where?
3.4.2. When?
| Author | Number of Group (n) | Number of Participants (n) | Gender (F: Female; M: Male) (n) | Age, Mean (SD) (Range), Years | Health Status | Education | Ethnicity/Birthplace | Income |
|---|---|---|---|---|---|---|---|---|
| Močnik et al., 2022 [9] | 1 | 90 | F: 70; M: 20 | 70.48 | More than half of the participants self-rated their health as moderate, and almost a third rated it as good. | Not mentioned. | Chinese: 76; Malay: 6; Indian 7; Other state: 1. | All participants’ incomes were provided by a government social assistance program. |
| Lauwers et al., 2021 [59] | 3 (–50) years old (50–70) years old (70+) | 50 years old: 9 (50–70): 9 (70+): 10 | No specific information about older adults. All participants: F:17; M: 11 | (50–70): 9 (70+): 10 | Not mentioned. | No specific information: The recruitment strategy intended to reach a varied sample in terms of age, gender, education level, employment status, and cultural background. | Not mentioned. | Not mentioned. |
| Herrmann-Lunecke et al., 2021 [60] | 3 Young adults Middle-aged adults Older adults | No specific information for older adults: 120 participants (20 participants per neighborhood). | No specific information about older adults. Half of each neighborhood group was composed of women. | Older adults were above 60 years old. | Not mentioned. | Not mentioned. | Not mentioned. | Not mentioned. |
| Grove 2021 [61] | 1 | 15 (10 in WAI) | No specific information about WAI participants. All participants: F: 12; M: 3 | No specific information about WAI participants. All participants:(65–69): 1 (70–74): 9 (75–79): 1 (80–84): 0 (85–89): 1 Age not identified during interview: 3 | Chronic Obstructive Pulmonary Disease: 3. Alzheimer’s Disease: 2. Parkinson’s Disease: 1. Digestive Conditions: 2. Macular degeneration: 1. Non-specific limitations: 2. None identified: 4 | Not mentioned. | Not mentioned. | Not mentioned. |
| Sun and Lau 2021 [62] | 1 | 72 | F: 44; M: 28 | (65–69): 27 (70–74): 17 (75–79): 20 (80+): 8 | Not mentioned. | Not educated: 8 Primary school: 36 School: 24 Tertiary school: 4 | Not mentioned. | No income: 51 Less than HKD 5000: 10 HKD 5–9.999,000: 9 HKD +10,000: 5 |
| Lager et al., 2021 [35] | 1 | 12 | F:10; M: 2 | 74.58 (8.07) [C] (65–87) | Not mentioned. | No specific information. | White: 12 | Not mentioned. |
| Kou et al., 2021 [36] | 1 | 20 (15 in WAI) | No specific information about WAI participants: F:8; M:12 | No specific information about WAI participants: 73.89 (8.23) | Advanced lower extremity functioning: 86.5 (11.9) | No specific information about WAI participants. Primary level of education: 2 Secondary level of education: 9 Tertiary level of education: 9 | White: 20 | Not mentioned. |
| Hand et al., 2021 [10] | 1 | The original study involved 38 participants but results from 2 women only were presented | F:2 | 75 and 77 | Nancy [P]: significant health challenges/Eleanor [P]: no information | Not mentioned. | Not mentioned. | Not mentioned. |
| Saint-Onge et al., 2021 [8] | 1 | 26 | F:18; M:8 | 71.96 (8.0) | Self-reported Very good: 11 Good: 10 Average: 4 Bad: 1 Very bad: 0 | Secondary or less: 17 College diploma: 2 University diploma: 7 | Not mentioned. | USD 9999 or less: 2 USD 10,000–19,999: 17 USD 20,000–39,999: 5 |
| Li and Woolrych 2021 [58] | 3: Living in different district: Dahuanglu Community (DC) Shiyoulu Community (SC) Huualongqiao Community (HC) | 64 (WAI: 21): DC: 22 (6) SC: 21 (7) HC: 21 (8) | No specific information about WAI participants. All participants— DC: F: 13; M: 9 SC: F:16; M: 5HC: F10; M:11 | No specific information about WAI participants. All participants— DC: 74.91 (60–90 med: 75) SC: 72.9 (60–86 med: 73) HC: 70.0 (62–84 med: 69) | Participants ranged in terms of gender, ages, socio-economic background (low, medium, and high levels of income), health status, education, living status, and household composition. | No specific information about WAI participants. All participants— DC: No qualification: 5 Elementary education: 2 Secondary education: 5 College, university education, and scientific education: 5 SC: No qualification: 3 Elementary education: 0 Secondary education: 15 College, university education, and scientific education: 3 HC: No qualification: 0 Elementary education: 2 Secondary education: 13 College, university education, and scientific education: 6 | Not mentioned. | GBP (March 2020: GPB 1 = CNY 9): No specific information about participants of WAI. All participants— DC: 308.89 (308.89–555.56 med: 333.33) SC: 356.08 (111.11–1111.11 med: 333.33) HC: 407.41 (222.22–666.67 med: 333.33) |
| Veitch et al., 2020 [7] | 1 | 30 | F:15; M:15 | 74.9 (5.4) | Not mentioned. | Low (did not complete high school): 3 Medium (year 12/trade/certificate): 4 High (university or tertiary qualification): 23 | Not mentioned. | Not mentioned. |
| Carroll et al., 2020 [55] | 1 | 16 | F:8; M:8 | 73.38 (10.06) (59–90) | Not mentioned. | Not mentioned. | Not mentioned. | Not mentioned. |
| Hand 2020 [56] | 1 | 14 (3 in the current study results) | F:3 | Above 65 years old (no other information). | Not mentioned. | Not mentioned. | Not mentioned. | Not mentioned. |
| Sundevall and Jansson 2020 [57] | 3: Children Adolescent Elderly | Elderly: 6 | F:3; M:3 | F: 70.33 (4.51) [C] M: 73.67 (4.04) [C] | Not mentioned. | Not mentioned. | Lived in Landskrona all life: 3 Born in Landskrona and has also moved back: 1 Born in the region and lives in Landskrona for 25 years: 1 Born in other part of Sweden and has lived in Landskrona for several years: 1 | Not mentioned. |
| Cao et al., 2019 [6] | 1 | 12 | F:6; M:6 | (55–64): 2 (65–74): 6 (75–84): 4 | Not mentioned. | Not mentioned. | Chinese: 10 Indian: 1 Other: 1 | Not mentioned. |
| Macintyre et al., 2019 [25] | 1 | 10 | F:8; M:2 | (60+) | Not mentioned. | Not mentioned. | Not mentioned. | Not mentioned. |
| Cassarino et al., 2019 [54] | 1 | 112 (7 in WAI) | No specific information | No specific information. | Not mentioned. | Not mentioned. | Not mentioned. | Not mentioned. |
| Thandi et al., 2018 [38] | 1 | 4 | M:4 | (70–86) | Functionally capable of completing daily activities. Self-reported— Multiple chronic health conditions: 1 Generally healthy; history of back pain and some shortness of breath: 1 Previous stroke: mild cognitive decline: 1 Generally healthy; history of leg pain following biking accident as a pedestrian: 1 | Secondary school: 2 Graduate degree: 1 University degree: 1 | White, of European background | Satisfied with their financial status. |
| Lee and Dean 2018 [30] | 2: Wychwood and Edenbrigde-Humber valley habitants | 28 (3 in WAI) | No specific information about WAI participants. All participants: Wychwood: F:14; M:0 Edenbrigde-Humber valley: F:11; M:3 | No specific information about WAI participants. All participants: Wychwood: (65–69):1 (70–74):0 (75–79):4 (80–84):3 (85–89):4 [90+]:3 Edenbrigde-Humber valley: (65–69):0 (70–74):0 (75–79):2 (80–84):1 (85–89):4 (90+): 6 | The population sample of seniors ranged in terms of socio-economic status as well as overall physical and mental health levels | Not mentioned. | No specific information about WAI participants. All participants birthplaces— Wychwood: Canada: 11 Ireland:1 Jamaica: 2 Edenbrigde-Humber valley: Canada:12 Scotland:1 Slovenia:1 | Not mentioned. |
| Hand et al., 2018 [23] | 1 | 14 (13 in WAI) | No specific information about WAI participants. All participants: F:11; M:3 | No specific information about WAI participants. All participants: 75.92 (8.29)[C] | Self-reported: experiencing very good or excellent health | Completed high school or higher education. | Caucasian | Not mentioned. |
| Suopajärvi 2018 [37] | 1 | 16 (10 in WAI) | Not mentioned | (61–87) (2011) | All lived independently. | No specific information about WAI participants. All participants— Basic education: 2 Intermediate education level: 10 University education: 4 | No specific information about WAI participants. All participants: All except two of them had lived for most of their lives in Oulu | Financially capable of using computers and the internet |
| Nordin et al., 2018 [53] | 2 RCF A RCF B | The staff and relatives who were at the RCFs during data collection received information and were invited to participate in the unstructured observations and walk-along interviews. In total, there were 83 people included; Residents: 54 Staff members: 25 Relatives: 4 Older adults: 58 | Older adults: 52 RCF A: F:20; M: 6 RCF B: F:17; M:9 | RCF A: 87 (74–96) RCF B: 88 (71–100) | RCF A Communication, poor: 3.85%; good: 96.15 Orientation, poor: 19.24%; good: 80.76% Mobility, poor: 26.93%; good: 73.07% Emotion, poor: 26.93%; good: 73.07% Socialization, poor: 11.54%; good: 88.46% RCF B Communication, poor: 15.9%; good: 84.61% Orientation, poor: 11.54%; good: 88.46% Mobility, poor: 23.08%; good: 76.92% Emotion, poor: 34.62%; good: 65.38% Socialization, poor: 19.24%; good: 80.76% | Not mentioned. | Not mentioned. | Not mentioned. |
| Zandieh et al., 2017 [52] | 2: Low- and high-deprivation areas | 173 (19 in WAI) Low-deprivation area: 93 (9 in WAI) High-deprivation area: 80 (10 in WAI) | Low-deprivation area: F: 7; M: 2 High-deprivation area: F: 6; M:4 | Low-deprivation area: (65–74): 4 (75+): 5 High-deprivation area: (65–74): 5 (75+): 5 | Able to walk, independent in daily life activities, and mentally healthy. Self-reported Low-deprivation area Good: 9 Poor: 0 High-deprivation area Good: 9 Poor: 1 | Low-deprivation area— GCSE and higher: 9 Sub-GCSE: 0 High-deprivation area— GCSE and higher: 2 Sub-GCSE: 8 | Low-deprivation area— White British: 8 BME groups: 1 High-deprivation area: White British :5 BME groups: 5 | Not mentioned. |
| Luusua et al., 2016 [32] | 2: Young adults, older adults | 16 (5 older adults) | F:3; M:2 | (65+) | Not mentioned. | Different educational, personal, and employment backgrounds. | Not mentioned. | Not mentioned. |
| Ottoni et al., 2016 [49] | 2 2012: T1 2014: T2 | 50. T1: 28 T2: 22 | T1— F:17; M: 11 T2— F:12; M:10 | T1— (–75): 21 (75+): 7 T2— (–75): 14 (75+): 8 | Not mentioned. | T1— Secondary school or less: 2 Trade school: 8 University or graduate school: 18 T2— Secondary school or less: 3 Trade school: 6 University or graduate school: 12 No response: 1 | T1— European Descent 26 First nation: 1 West Indian: 1 T2— European: 21 West Indian: 1 | T1— Low (less than USD 25,000): 7 Medium (USD 25,000–74,999): 12 High (USD +75,000): 5 No response: 4 T2— Low: 2 Medium: 12 High: 3 No response: 5 |
| Curl et al., 2016 [50] | 1 | 20 | F:17; M: 3 | 77 (6.71) | Fallers | Not mentioned. | Not mentioned. | Not mentioned. |
| Yoo and Kim 2016 [46] | 2: Older adults Service providers | Older adults: 46 (19 in WAI) | No specific information about WAI participants. All participants: F:28, M: 18 | 75.4 (6.4) | Good: 13 Average: 21 Bad: 12 | Not mentioned. | Not mentioned. | Not mentioned. |
| Zandieh et al., 2016 [51] | 2: Low- and high-deprivation areas | 173 (19 in WAI) Low-deprivation area: 93 (9 in WAI) High-deprivation area: 80 (10 in WAI) | Low-deprivation area— F: 7; M: 2 High-deprivation area— F: 6; M:4 | Low-deprivation area— (65–74): 4 (75+): 5 High-deprivation area— (65–74): 5 (75+): 5 | Able to walk, independent in daily life activities, and mentally healthy. Self-reported Low-deprivation area Good: 9 Poor: 0 High-deprivation area Good: 9 Poor: 1 | Low-deprivation area— GCSE and higher: 9 Sub-GCSE: 0 High-deprivation area— GCSE and higher: 2 Sub-GCSE: 8 | Low-deprivation area— White British: 8 BME groups: 1 High-deprivation area— White British: 5 BME groups: 5 | Not mentioned. |
| Lager et al., 2015 [48] | 1 | 7 | F:7 | (65–70): 2 (70–75): 1 (75–80): 1 (85–90): 3 | Not mentioned. | Not mentioned. | White: 7 | Not mentioned. |
| Gardner 2014 [47] | 1 | 6 | F:3; M:3 | 82.5 (4.32) | Participants varied in their levels of education and income, lived in a variety of housing types, reflected a range of functional abilities, and used various forms of mobility within their neighborhoods. | Highschool: 2 Some highschool: 3 PhD: 1 | White Canadian: 3 White Austrian: 1 White Irish: 1 | USD 10–20,000: 2 USD 20–30,-000: 3 USD 30–40,000: 1 |
| Van Cauwenberg et al., 2012 [5] | 1 | 57 | F: 27; M:30 | 73.4 (5.4) | Not mentioned. | Higher education: 27 | Not mentioned. | Not mentioned. |
| Author | Exclusion/Inclusion Criteria |
|---|---|
| Močnik et al., 2022 [9] | Not mentioned. |
| Lauwers et al., 2021 [59] | The recruitment strategy intended to reach a varied sample in terms of age, gender, education level, employment status, and cultural background. However, the large geographical scale and time limitation of the study led to convenience sampling, based on the willingness of the people we met in the organizations. Knowing the mixed use of language in the Brussels Capital Region (most spoken: French, English, and Dutch), only participants skilled in Dutch, French, or English with a minimum age of 18 years were included. |
| Herrmann-Lunecke et al., 2021 [60] | Participants were required to speak Spanish and to have lived in the neighborhood for at least the last two years. |
| Grove 2021 [61] | Not mentioned. |
| Sun and Lau 2021 [62] | Living in the study areas and familiar with the designated routes, aged 65 or above, and can walk and use public transport without aids. |
| Lager et al., 2021 [35] | The Dutch retirement age of the time (65) was chosen as the threshold. |
| Kou et al., 2021 [36] | Not mentioned. |
| Hand et al., 2021 [10] | Residents were eligible to participate in the larger study if they: (a) had lived in one of the neighborhoods for at least 1 year, (b) were not working or were engaged in part-time paid employment, (c) were able to converse in English, and (d) were able to access the community, either alone or with assistance. |
| Saint-Onge et al., 2021 [8] | Individuals were eligible to participate if they were (1) tenants of one of the three study sites; (2) able to walk four 10 min sessions, and (3) able to communicate in either French, English, or Spanish. They were excluded if they reported having an intellectual, visual, or auditory impairment that could significantly impact walking safety and ability. |
| Li and Woolrych 2021 [58] | Not mentioned. |
| Veitch et al., 2020 [7] | Required to be English-speaking. |
| Carroll et al., 2020 [55] | Irrespective of their physical ability or potential impairment. |
| Hand 2020 [56] | Selection criteria were age 65 years or more, able to participate in an interview in English, not working full-time, and able to move about the community in some way. |
| Sundevall and Jansson 2020 [57] | Not mentioned. |
| Cao et al., 2019 [6] | This study included those aged 55–64 because Singapore is aging rapidly, and this age group’s opinions are valuable for future developments. To be recruited, participants needed to be able to speak either English or Mandarin Chinese and be living in Yuhua East, or living in a nearby neighborhood but walking to the facilities in Yuhua East on a daily or weekly basis. |
| Macintyre et al., 2019 [25] | Any adults aged 60 or over in 2018 were considered eligible to participate if they lived or spent a large amount of time (i.e., a minimum of one or more hours every two weeks) in Old Moat when the study occurred. Participants were excluded from the study if they had a diagnosis of dementia, since this could affect their ability to participate in the interviews. Participants who were able to complete walk-along interviews were prioritized for recruitment, although participants who preferred to participate in a sitting down photo elicitation interview were also recruited. |
| Cassarino et al., 2019 [54] | Not mentioned. |
| Thandi et al., 2018 [38] | Inclusion criteria were broad—they had to self-identify as men aged 65 or older, be able to communicate in English, live in the community, and be able to move about within and outside their homes. |
| Lee and Dean 2018 [30] | The only selection criteria were that participants had to live in the chosen neighborhoods, Wychwood and Edenbridge-Humber Valley, and be over the age of 65 years. |
| Hand et al., 2018 [23] | We recruited 14 residents age 65 years or more living in two neighborhoods with diverse characteristics in a mid-sized Canadian city. Individuals were eligible to participate if they had lived in one of the target neighborhoods for at least 1 year, could participate in an interview in English, were not working full-time, and were able to venture into their community. |
| Suopajärvi 2018 [37] | All except two of them had lived for most of their lives in Oulu; however, this was not a criterion for selecting study participants. |
| Nordin et al., 2018 [53] | Not mentioned. |
| Zandieh et al., 2017 [52] | Inclusion criteria were being aged 65 or over, residing in of one of the selected wards, being able to walk, being independent in daily life activities, and being mentally healthy. |
| Luusua et al., 2016 [32] | Not mentioned. |
| Ottoni et al., 2016 [49] | We include participants who reside in one of three adjacent neighborhoods: Vancouver’s West End, Yaletown, and Downtown. |
| Curl et al., 2016 [50] | Older adults (aged 65 years and over) who had experienced a fall in the previous 12 months. We defined “older people” as those aged 65 or older. We used the Scottish Walkability Assessment Tool (SWAT) as a starting point for our audit checklist. We used a convenience sample, recruited from those who had already participated in a focus group about falling outdoors, and based on having experienced a fall during the previous year and their willingness to participate in further research. |
| Yoo and Kim 2016 [46] | Not mentioned. |
| Zandieh et al., 2016 [51] | Older adults (65 years and upward), residents of a low- or high-deprivation area, those able to walk, those independent in their daily life activities, and the mentally healthy were eligible to participate in this research. Ability to speak English was not an eligibility criteria. |
| Lager et al., 2015 [48] | Not mentioned. |
| Gardner 2014 [47] | Over the age of 75, living alone (as most older adults in this age category live alone) and having resided in the study neighborhood for a minimum of three years. |
| Van Cauwenberg et al., 2012 [5] | To be included, participants had to be over 65 years old, dwelling in the community, and able to walk independently for at least 30 min. |
| Author | Number of Participants | Data Collection Duration | WAI Duration per Participant | Total Duration of the WAI (Number of Participants × Duration per Participant) | ||
|---|---|---|---|---|---|---|
| Range | Mean | Range | Mean | |||
| Močnik et al., 2022 [9] | 90 | From 1 December 2017 to 21 February 2018 (3 months) | Not mentioned | Not mentioned. | ||
| Lauwers et al., 2021 [59] | Total: 28 50 years old: 9 (50–70): 9 (70+): 10 | From March 2019 to June 2019 (4 months) | Not mentioned | 90 min (1 h 30 min) | 2520 min (42 h) | |
| Herrmann-Lunecke et al., 2021 [60] | No specific information for older adults: 120 participants (20 participants per neighborhood) | From September 2018 and November 2018 (2 moths) | Not mentioned | Not mentioned | ||
| Grove 2021 [61] | 15 (10 in WAI) | From December 2017 to September 2018 (10 months) | Not mentioned | 13 min (0 h 13 min) | 130 min (2 h 10 min) | |
| Sun and Lau 2021 [62] | 72 | From January 2019 to March 2019 (3 months) | Not mentioned | Not mentioned. | ||
| Lager et al., 2021 [35] | 12 | No specific information about the duration of data collection. Summer of 2012 and Spring of 2013. | Not mentioned | Not mentioned. | ||
| Kou et al., 2021 [36] | 20 (15 in WAI) | No specific information about the duration of data collection. | Not mentioned | 56 min, SD = 10 (0 h 56 min) | 840 min (14 h) | |
| Hand et al., 2021 [10] | The original study involved 38 participants but results from 2 women only were presented | No specific information about the duration of data collection. | - Nancy: 50 min (0 h 50 min) - Eleanor: 35 min (0 h 35 min) | Not mentioned. | ||
| Saint-Onge et al., 2021 [8] | 26 | From 11 September to 25 October 2017 (2 months) | 60–150 min (1 h–2 h 30 min) | Not mentioned. | 1560–3900 min (26–65 h) | |
| Li and Woolrych 2021 [58] | 64 (WAI: 21) DC: 22 (6) SC: 21 (7) HC: 21 (8) | From December 2019 to January 2020 (2 months) | Not mentioned | Not mentioned. | ||
| Veitch et al., 2020 [7] | 30 | From October 2017 to February 2018 (5 months) | 6−35 min (0 h 06−0 h 35 min) | 16 min (0 h 16 min) | 180–1050 min (3 h−17 h 30 min) | 480 min (8 h) |
| Carroll et al., 2020 [55] | 16 | No specific information about the duration of data collection. | 30 min to more than 120 min (0 h 30 min to more than 2 h) | Not mentioned | 480 min to more than 1920 min (8 h to more than 32 h) | |
| Hand 2020 [56] | 14 (3 in the current study results) | No specific information about the duration of data collection. | 45–120 min (0 h 45 min−2 h) | Not mentioned. | 630–1680 min (10 h 30 min–28 h) | |
| Sundevall and Jansson 2020 [57] | Elderly: 6 | No specific information about the duration of data collection. | 30–84 min (0 h 30–1 h 24 min) | Not mentioned. | 180–504 min (3 h–8 h 24 min) | |
| Cao et al., 2019 [6] | 12 | From August 2018 to September 2018 (2 months) | 9 min to more than 120 min (0 h 09 min to more than 2 h) | Not mentioned. | 108 min to more than 1440 min (1 h 48 min to more than 24 h) | |
| Macintyre et al., 2019 [25] | 10 | Not mentioned | 30–100 min (0 h 30–1 h 40 min) | Not mentioned. | 300–1000 min (5 h–16 h 40 min) | |
| Cassarino et al., 2019 [54] | 112 (7 in WAI) | No specific information about the duration of data collection. | Not mentioned | Not mentioned. | ||
| Thandi et al., 2018 [38] | 4 | No specific information about the duration of data collection. | 30–60 min (0 h 30 min–1 h) | Not mentioned. | 120–240 min (2–4 h) | |
| Lee and Dean 2018 [30] | 28 (3 in WAI) | No specific information about the duration of data collection. | Not mentioned | Not mentioned. | ||
| Hand et al., 2018 [23] | 14 (13 in WAI) | No specific information about the duration of data collection. | 30–120 min (0 h 30 min–2 h) | Not mentioned. | 390–1560 min (6 h 30 min–26 h) | |
| Suopajärvi 2018 [37] | 16 (10 in WAI) | No specific information about the duration of data collection. | 60–90 min (1 h–1 h 30 min) | Not mentioned. | 600–900 min (10–15 h) | |
| Nordin et al., 2018 [53] | The staff and relatives who were at the RCFs during data collection received information and were invited to participate in the unstructured observations and walk-along interviews. In total, the 83 people included Residents: 54; Staff members: 25; Relatives: 4; Older adults: 58 | Data were collected across a 5-week period during early spring (1 month) | Not mentioned | Not mentioned. | ||
| Zandieh et al., 2017 [52] | 173 (19 in WAI) Low-deprivation area: 93 (9 in WAI) High-deprivation area: 80 (10 in WAI) | From 7 July to October 2012 (4 months) | 30–60 min (0 h 30 min–1 h) | Not mentioned. | 570–1140 min (9 h 30 min–19 h) | |
| Luusua et al., 2016 [32] | 16 (5 older adults) | From December to February (the year is not mentioned) (3 months) | Not mentioned | Not mentioned. | ||
| Ottoni et al., 2016 [49] | Total: 50 T1: 28 T2: 22 | No specific information about the duration of data collection. | Not mentioned | Not mentioned. | ||
| Curl et al., 2016 [50] | 20 | No specific information about the duration of data collection. | Not mentioned | 25.1 min, SD = 10.92 (0 h 25 min) | 502 min (8 h 22 min) | |
| Yoo and Kim 2016 [46] | Older adults: 46 (19 in WAI) | From April 2014 to November 2015 (20 months) | Not mentioned | Not mentioned | ||
| Zandieh et al., 2016 [51] | 173 (19 in WAI) Low-deprivation area: 93 (9 in WAI) High-deprivation area: 80 (10 in WAI) | From July 2012 to November 2012 (5 months) | 30–60 min (0 h 30 min–1 h) | Not mentioned. | 570–1140 min (9 h 30 min–19 h) | |
| Lager et al., 2015 [48] | 7 | From September 2012 and February 2013 (2 months) | 30–90 min (0 h 30–1 h 30 min) | Not mentioned. | 210–630 min (3 h 30–10 h 30 min) | |
| Gardner 2014 [47] | 6 | Data was collected over an 8-month period during. | 120–240 min (2–4 h) | Not mentioned. | 1080–1440 min (18–24 h) | |
| Van Cauwenberg et al., 2012 [5] | 57 | From November 2010 to February 2011 (4 months) | 30 min approximately | Not mentioned. | 1710 min (28 h 30 min) approximately | |
3.4.3. With Whom?
3.4.4. How?
- Before walk-along interview. Preparing every aspects of the WAI:
- During walk-along interview:
- After the walk-along interview:
- Mixed-method approach
4. Discussion
4.1. Study Characteristics
4.2. Participants’ Characteristics
4.3. Walk-along Interview Protocol Data Collection
4.3.1. Environmental Characteristics
4.3.2. When the WAI Takes Place? Seasons, Weather, and Time of Day
4.4. Data Collection
4.4.1. Interviews and/or Questionnaires before WAI?
4.4.2. Who Is the Interviewer?
4.4.3. Interview Guide?
4.4.4. Typology of WAI, Two Ways to Choose the Route
4.4.5. Duration and Distance of WAI, and Stops/Breaks?
4.4.6. WAI Recording: Route Tracking, Field/Reflective Notes, and Visual/Audio Recording
4.5. The Mixed-Methods Approach
4.6. Strengths/Limits and Propositions
4.7. Scoping Limits and Perspectives of the Review
4.8. How to Prepare a “Walk-along Interview”?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World Population Prospects—Summary of Results; Department of Economic and Social Affairs: New York, NY, USA, 2022; Available online: https://population.un.org/wpp/ (accessed on 18 August 2022).
- Lord, S.; Piché, D. Vieillissement et Aménagement: Perspectives Plurielles; Les Presses de l’Université de Montréal: Montréal, QC, Canada, 2018; ISBN 978-2-7606-3833-4. [Google Scholar]
- Sheller, M.; Urry, J. The New Mobilities Paradigm. Environ. Plan A 2006, 38, 207–226. [Google Scholar] [CrossRef]
- The Spatial Turn: Interdisciplinary Perspectives; Warf, B.; Arias, S. (Eds.) Routledge: London, UK, 2008; ISBN 978-0-203-89130-8. [Google Scholar]
- Van Cauwenberg, J.; Van Holle, V.; Simons, D.; Deridder, R.; Clarys, P.; Goubert, L.; Nasar, J.; Salmon, J.; De Bourdeaudhuij, I.; Deforche, B. Environmental Factors Influencing Older Adults’ Walking for Transportation: A Study Using Walk-along Interviews. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 85. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Heng, C.K.; Fung, J.C. Using Walk-along Interviews to Identify Environmental Factors Influencing Older Adults’ out-of-Home Behaviors in a High-Rise, High-Density Neighborhood. Int. J. Environ. Res. Public Health 2019, 16, 4251. [Google Scholar] [CrossRef] [PubMed]
- Veitch, J.; Flowers, E.; Ball, K.; Deforche, B.; Timperio, A. Designing Parks for Older Adults: A Qualitative Study Using Walk-along Interviews. Urban For. Urban Green. 2020, 54, 126768. [Google Scholar] [CrossRef]
- Saint-Onge, K.; Bernard, P.; Kingsbury, C.; Houle, J. Older Public Housing Tenants’ Capabilities for Physical Activity Described Using Walk-along Interviews in Montreal, Canada. Int. J. Environ. Res. Public Health 2021, 18, 11647. [Google Scholar] [CrossRef]
- Močnik, Š.; Moogoor, A.; Yuen, B. Exploring Facilitators and Barriers of Older Adults’ Outdoor Mobility: A Walk-along Study in Singapore. J. Transp. Health 2022, 26, 101386. [Google Scholar] [CrossRef]
- Hand, C.; Stewart, K.; Rudman, D.L.; McGrath, C.; McFarland, J.; Gilliland, J. Applying the Go-along Method to Enhance Understandings of Occupation in Context. J. Occup. Sci. 2021, 1–14. [Google Scholar] [CrossRef]
- Carpiano, R.M. Come Take a Walk with Me: The “Go-along” Interview as a Novel Method for Studying the Implications of Place for Health and Well-Being. Health Place 2009, 15, 263–272. [Google Scholar] [CrossRef]
- Burns, R.; Gallant, K.A.; Fenton, L.; White, C.; Hamilton-Hinch, B. The Go-along Interview: A Valuable Tool for Leisure Research. Leis. Sci. 2020, 42, 51–68. [Google Scholar] [CrossRef]
- Lima, J.P.; Machado, M.H. Walking Accessibility for Individuals with Reduced Mobility: A Brazilian Case Study. Case Stud. Transp. Policy 2019, 7, 269–279. [Google Scholar] [CrossRef]
- Mysyuk, Y.; Huisman, M. Photovoice Method with Older Persons: A Review. Ageing Soc. 2020, 40, 1759–1787. [Google Scholar] [CrossRef]
- Wang, C.C.; Redwood-Jones, Y.A. Photovoice Ethics: Perspectives from Flint Photovoice. Health Educ. Behav. 2001, 28, 560–572. [Google Scholar] [CrossRef] [PubMed]
- Andress, L.; Hallie, S.S. Co-Constructing Food Access Issues: Older Adults in a Rural Food Environment in West Virginia Develop a Photonarrative. Cogent Med. 2017, 4, 1309804. [Google Scholar] [CrossRef]
- Hand, C.; Rudman, D.L.; Huot, S.; Pack, R.; Gilliland, J. Enacting Agency: Exploring How Older Adults Shape Their Neighbourhoods. Ageing Soc. 2020, 40, 565–583. [Google Scholar] [CrossRef]
- Fang, M.L.; Woolrych, R.; Sixsmith, J.; Canham, S.; Battersby, L.; Sixsmith, A. Place-Making with Older Persons: Establishing Sense-of-Place through Participatory Community Mapping Workshops. Soc. Sci. Med. 2016, 168, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.; Jones, P. The Walking Interview: Methodology, Mobility and Place. Appl. Geogr. 2011, 31, 849–858. [Google Scholar] [CrossRef]
- King, A.C.; Woodroffe, J. Walking Interviews. In Handbook of Research Methods in Health Social Sciences; Springer: Singapore, 2019; pp. 1269–1290. [Google Scholar]
- Hodgson, F. Everyday Connectivity: Equity, Technologies, Competencies and Walking. J. Transp. Geogr. 2012, 21, 17–23. [Google Scholar] [CrossRef]
- Chang, J.S. The Docent Method: A Grounded Theory Approach for Researching Place and Health. Qual. Health Res. 2017, 27, 609–619. [Google Scholar] [CrossRef]
- Hand, C.L.; Rudman, D.L.; Huot, S.; Gilliland, J.A.; Pack, R.L. Toward Understanding Person-Place Transactions in Neighborhoods: A Qualitative-Participatory Geospatial Approach. Gerontologist 2018, 58, 89–100. [Google Scholar] [CrossRef]
- Kusenbach, M. Street Phenomenology: The Go-Along as Ethnographic Research Tool. Ethnography 2003, 4, 455–485. [Google Scholar] [CrossRef]
- Macintyre, V.G.; Cotterill, S.; Anderson, J.; Phillipson, C.; Benton, J.S.; French, D.P. I Would Never Come Here Because Ive Got My Own Garden”: Older Adults’ Perceptions of Small Urban Green Spaces. Int. J. Environ. Res. Public Health 2019, 16, 1994. [Google Scholar] [CrossRef] [PubMed]
- Desprès, M.; Lord, S.; Negron-Poblete, P. (Re)Placer La Mobilité Dans Son Contexte: Le Parcours Commenté, Un Outil de Recueil et d’analyse de Données Demobilité. RTS Rech. Transp. Sécurité 2019, 2019, 21. [Google Scholar] [CrossRef]
- Thibaud, J.-P. Les Parcours Commentés. In L’espace Urbain en Méthodes; Grosjean, M., Thibaud, J.-P., Eds.; Editions Parenthèses: Marseille, France, 2001; pp. 79–99. [Google Scholar]
- Emmel, N.; Clark, A. The Methods Used in Connected Lives: Investigating Networks, Neighbourhoods and Communities; National Centre for Research Methods: Leeds, UK, 2009. [Google Scholar]
- Clark, A.; Emmel, N. Using Walking Interviews; Morgan Centre, University of Manchester: Manchester, UK, 2010. [Google Scholar]
- Lee, E.; Dean, J. Perceptions of Walkability and Determinants of Walking Behaviour among Urban Seniors in Toronto, Canada. J. Transp. Health 2018, 9, 309–320. [Google Scholar] [CrossRef]
- Battista, G.A.; Manaugh, K. Using Embodied Videos of Walking Interviews in Walkability Assessment. Transp. Res. Rec. J. Transp. Res. Board 2017, 2661, 12–18. [Google Scholar] [CrossRef]
- Luusua, A.; Pihlajaniemi, H.; Ylipulli, J. Northern Urban Lights: Emplaced Experiences of Urban Lighting as Digital Augmentation. In Architecture and Interaction: Human Computer Interaction in Space and Place; Dalton, N.S., Schnädelbach, H., Wiberg, M., Varoudis, T., Eds.; Human–Computer Interaction Series; Springer International Publishing: Cham, Switzerland, 2016; pp. 275–297. ISBN 978-3-319-30028-3. [Google Scholar]
- Van Cauwenberg, J.; De Bourdeaudhuij, I.; De Meester, F.; Van Dyck, D.; Salmon, J.; Clarys, P.; Deforche, B. Relationship between the Physical Environment and Physical Activity in Older Adults: A Systematic Review. Health Place 2011, 17, 458–469. [Google Scholar] [CrossRef]
- Cerin, E.; Nathan, A.; van Cauwenberg, J.; Barnett, D.W.; Barnett, A.; on behalf of the Council on Environment and Physical Activity (CEPA)—Older Adults working group. The Neighbourhood Physical Environment and Active Travel in Older Adults: A Systematic Review and Meta-Analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 15. [Google Scholar] [CrossRef]
- Lager, D.R.; Van Hoven, B.; Huigen, P.P.P. Neighbourhood Walks as Place-Making in Later Life [Les Promenades de Quartier Comme Fabrique Des Lieux à La Vieillesse]. Soc. Cult. Geogr. 2021, 22, 1080–1098. [Google Scholar] [CrossRef]
- Kou, R.; Hunter, R.F.; Cleland, C.; Ellis, G. Physical Environmental Factors Influencing Older Adults’ Park Use: A Qualitative Study. Urban For. Urban Green. 2021, 65, 127353. [Google Scholar] [CrossRef]
- Suopajärvi, T. From Tar City to Smart City Living with the Smart City Ideology as a Senior City Dweller. Ethnol. Fenn. 2018, 45, 79–102. [Google Scholar] [CrossRef]
- Thandi, M.K.G.; Phinney, A.; Oliffe, J.L.; Wong, S.; McKay, H.; Sims-Gould, J.; Sahota, S. Engaging Older Men in Physical Activity: Implications for Health Promotion Practice. Am. J. Men’s Health 2018, 12, 2064–2075. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 10, 89. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley: Chichester, UK, 2019. [Google Scholar]
- Wesener, A.; Vallance, S.; Tesch, M.; Edwards, S.; Frater, J.; Moreham, R. A Mobile Sense of Place: Exploring a Novel Mixed Methods User-Centred Approach to Capturing Data on Urban Cycling Infrastructure. Appl. Mobilities 2021, 1–25. [Google Scholar] [CrossRef]
- Hopewell, S.; Clarke, M.; Lefebvre, C.; Scherer, R. Handsearching versus Electronic Searching to Identify Reports of Randomized Trials. Cochrane Database Syst. Rev. 2007, 2, MR000001. [Google Scholar] [CrossRef] [PubMed]
- Richards, D. Handsearching Still a Valuable Element of the Systematic Review. Evid. Based Dent. 2008, 9, 85. [Google Scholar] [CrossRef]
- Farkas, B.; Wagner, D.J.; Nettel-Aguirre, A.; Friedenreich, C.; McCormack, G.R. Evidence Synthesis—A Systematized Literature Review on the Associations between Neighbourhood Built Characteristics and Walking among Canadian Adults. Health Promot. Chronic. Dis. Prev. Can. 2019, 39, 1. [Google Scholar] [CrossRef]
- Christie, C.D.; Consoli, A.; Ronksley, P.E.; Vena, J.E.; Friedenreich, C.M.; McCormack, G.R. Associations between the Built Environment and Physical Activity among Adults with Low Socio-Economic Status in Canada: A Systematic Review. Can. J. Public Health 2021, 112, 152–165. [Google Scholar] [CrossRef]
- Yoo, S.; Kim, D.H. Perceived Urban Neighborhood Environment for Physical Activity of Older Adults in Seoul, Korea: A Multimethod Qualitative Study. Prev. Med. 2017, 103S, S90–S98. [Google Scholar] [CrossRef]
- Gardner, P. The Role of Social Engagement and Identity in Community Mobility among Older Adults Aging in Place. Disabil. Rehabil. 2014, 36, 1249–1257. [Google Scholar] [CrossRef]
- Lager, D.; Van Hoven, B.; Huigen, P.P.P. Understanding Older Adults’ Social Capital in Place: Obstacles to and Opportunities for Social Contacts in the Neighbourhood. Geoforum 2015, 59, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Ottoni, C.A.; Sims-Gould, J.; Winters, M.; Heijnen, M.; McKay, H.A. “Benches Become like Porches”: Built and Social Environment Influences on Older Adults’ Experiences of Mobility and Well-Being. Soc. Sci. Med. 2016, 169, 33–41. [Google Scholar] [CrossRef]
- Curl, A.; Thompson, C.W.; Aspinall, P.; Ormerod, M. Developing an Audit Checklist to Assess Outdoor Falls Risk. Proc. Inst. Civ. Eng. Urban Des. Plan. 2016, 169, 138–153. [Google Scholar] [CrossRef] [PubMed]
- Zandieh, R.; Martinez, J.; Flacke, J.; Jones, P.; Van Maarseveen, M. Older Adults’ Outdoor Walking: Inequalities in Neighbourhood Safety, Pedestrian Infrastructure and Aesthetics. Int. J. Environ. Res. Public Health 2016, 13, 1179. [Google Scholar] [CrossRef] [PubMed]
- Zandieh, R.; Flacke, J.; Martinez, J.; Jones, P.; Van Maarseveen, M. Do Inequalities in Neighborhood Walkability Drive Disparities in Older Adults’ Outdoor Walking? Int. J. Environ. Res. Public Health 2017, 14, 740. [Google Scholar] [CrossRef]
- Nordin, S.; McKee, K.; Wallinder, M.; von Koch, L.; Wijk, H.; Elf, M. The Physical Environment, Activity and Interaction in Residential Care Facilities for Older People: A Comparative Case Study. Scand. J. Caring Sci. 2017, 31, 727–738. [Google Scholar] [CrossRef]
- Cassarino, M.; Bantry-White, E.; Setti, A. Cognitive and Sensory Dimensions of Older People’s Preferences of Outdoor Spaces for Walking: A Survey Study in Ireland. Int. J. Environ. Res. Public Health 2019, 16, 1340. [Google Scholar] [CrossRef] [PubMed]
- Carroll, S.; Jespersen, A.; Troelsen, J. Going along with Older People: Exploring Age-Friendly Neighbourhood Design through Their Lens. J. Hous. Built Environ. 2019, 35, 555–572. [Google Scholar] [CrossRef]
- Hand, C. Older Women’s Engagement in Community Occupations: Considerations of Lifespan and Place. Scand. J. Occup. Ther. 2020, 27, 259–268. [Google Scholar] [CrossRef]
- Sundevall, E.P.; Jansson, M. Inclusive Parks across Ages: Multifunction and Urban Open Space Management for Children, Adolescents, and the Elderly. Int. J. Environ. Res. Public Health 2020, 17, 9357. [Google Scholar] [CrossRef]
- Li, M.; Woolrych, R. Experiences of Older People and Social Inclusion in Relation to Smart “Age-Friendly” Cities: A Case Study of Chongqing, China. Front. Public Health 2021, 9. [Google Scholar] [CrossRef]
- Lauwers, L.; Leone, M.; Guyot, M.; Pelgrims, I.; Remmen, R.; Van den Broeck, K.; Keune, H.; Bastiaens, H. Exploring How the Urban Neighborhood Environment Influences Mental Well-Being Using Walking Interviews. Health Place 2021, 67, 102497. [Google Scholar] [CrossRef]
- Herrmann-Lunecke, M.G.; Mora, R.; Vejares, P. Perception of the Built Environment and Walking in Pericentral Neighbourhoods in Santiago, Chile. Travel Behav. Soc. 2021, 23, 192–206. [Google Scholar] [CrossRef]
- Grove, H. Ageing as Well as You Can in Place: Applying a Geographical Lens to the Capability Approach. Soc. Sci. Med. 2021, 288, 113525. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.; Lau, C.Y. Go-along with Older People to Public Transport in High-Density Cities: Understanding the Concerns and Walking Barriers through Their Lens. J. Transp. Health 2021, 21, 101072. [Google Scholar] [CrossRef]
- Pollard, T.M.; Wagnild, J.M. Gender Differences in Walking (for Leisure, Transport and in Total) across Adult Life: A Systematic Review. BMC Public Health 2017, 17, 341. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Shmotkin, D.; Blumstein, Z.; Shorek, A.; Eyal, N.; Hazan, H. CALAS Team The Old, Old-Old, and the Oldest Old: Continuation or Distinct Categories? An Examination of the Relationship between Age and Changes in Health, Function, and Wellbeing. Int. J. Aging Hum. Dev. 2013, 77, 37–57. [Google Scholar] [CrossRef] [PubMed]
- Cerin, E.; Leslie, E.; Owen, N. Explaining Socio-Economic Status Differences in Walking for Transport: An Ecological Analysis of Individual, Social and Environmental Factors. Soc. Sci. Med. 2009, 68, 1013–1020. [Google Scholar] [CrossRef]
- Kamphuis, C.B.; van Lenthe, F.J.; Giskes, K.; Huisman, M.; Brug, J.; Mackenbach, J.P. Socioeconomic Differences in Lack of Recreational Walking among Older Adults: The Role of Neighbourhood and Individual Factors. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 1. [Google Scholar] [CrossRef]
- Del Porto, H.; Pechak, C.; Smith, D.; Reed-Jones, R. Biomechanical Effects of Obesity on Balance. Int. J. Exerc. Sci. 2012, 5, 301–320. [Google Scholar]
- Wearing, S.C.; Hennig, E.M.; Byrne, N.M.; Steele, J.R.; Hills, A.P. The Biomechanics of Restricted Movement in Adult Obesity. Obes. Rev. 2006, 7, 13–24. [Google Scholar] [CrossRef]
- Capodaglio, P.; Gobbi, M.; Donno, L.; Fumagalli, A.; Buratto, C.; Galli, M.; Cimolin, V. Effect of Obesity on Knee and Ankle Biomechanics during Walking. Sensors 2021, 21, 7114. [Google Scholar] [CrossRef]
- de Oliveira Máximo, R.; de Oliveira, D.C.; Ramírez, P.C.; Luiz, M.M.; de Souza, A.F.; Delinocente, M.L.B.; Steptoe, A.; de Oliveira, C.; da Silva Alexandre, T. Dynapenia, Abdominal Obesity or Both: Which Accelerates the Gait Speed Decline Most? Age Ageing 2021, 50, 1616–1625. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Lewis, C.L.; Gill, S.V. Effects of Obesity and Foot Arch Height on Gait Mechanics: A Cross-Sectional Study. PLoS ONE 2021, 16, e0260398. [Google Scholar] [CrossRef] [PubMed]
- Pau, M.; Capodaglio, P.; Leban, B.; Porta, M.; Galli, M.; Cimolin, V. Kinematics Adaptation and Inter-Limb Symmetry during Gait in Obese Adults. Sensors 2021, 21, 5980. [Google Scholar] [CrossRef] [PubMed]
- Rosso, V.; Agostini, V.; Takeda, R.; Tadano, S.; Gastaldi, L. Influence of BMI on Gait Characteristics of Young Adults: 3D Evaluation Using Inertial Sensors. Sensors 2019, 19, 4221. [Google Scholar] [CrossRef]
- Choi, H.; Lim, J.; Lee, S. Body Fat-Related Differences in Gait Parameters and Physical Fitness Level in Weight-Matched Male Adults. Clin. Biomech. 2021, 81, 105243. [Google Scholar] [CrossRef]
- Lockhart, T.E.; Frames, C.W.; Soangra, R.; Lieberman, A. Effects of Obesity and Fall Risk on Gait and Posture of Community-Dwelling Older Adults. Int. J. Progn. Health Manag. 2019, 10, 19. [Google Scholar] [CrossRef]
- Gonzalez, M.; Gates, D.H.; Rosenblatt, N.J. The Impact of Obesity on Gait Stability in Older Adults. J. Biomech. 2020, 100, 109585. [Google Scholar] [CrossRef]
- Law, N.-H.; Li, J.X.; Law, N.-Y.; Varin, D.; Lamontagne, M. Effects of Body Mass and Sex on Kinematics and Kinetics of the Lower Extremity during Stair Ascent and Descent in Older Adults. Sports Med. Health Sci. 2021, 3, 165–170. [Google Scholar] [CrossRef]
- Desrochers, P.C.; Kim, D.; Keegan, L.; Gill, S.V. Association between the Functional Gait Assessment and Spatiotemporal Gait Parameters in Individuals with Obesity Compared to Normal Weight Controls: A Proof-of-Concept Study. J. Musculoskelet. Neuronal Interact. 2021, 21, 335–342. [Google Scholar]
- Gill, S.V. Effects of Obesity Class on Flat Ground Walking and Obstacle Negotiation. J. Musculoskelet. Neuronal Interact. 2019, 19, 448–454. [Google Scholar]
- Wu, X.; Nussbaum, M.A.; Madigan, M.L. Executive Function and Measures of Fall Risk Among People With Obesity. Percept. Mot. Ski. 2016, 122, 825–839. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.J.; Lord, S.R.; Harvey, L.A.; Close, J.C.T. Associations between Obesity and Overweight and Fall Risk, Health Status and Quality of Life in Older People. Aust. N. Z. J. Public Health 2014, 38, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Neri, S.G.R.; Oliveira, J.S.; Dario, A.B.; Lima, R.M.; Tiedemann, A. Does Obesity Increase the Risk and Severity of Falls in People Aged 60 Years and Older? A Systematic Review and Meta-Analysis of Observational Studies. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.; Walford, N.; Hockey, A.; Foreman, N.; Lewis, M. Older People and Outdoor Environments: Pedestrian Anxieties and Barriers in the Use of Familiar and Unfamiliar Spaces. Geoforum 2013, 47, 113–124. [Google Scholar] [CrossRef]
- Delclòs-Alió, X.; Marquet, O.; Vich, G.; Schipperijn, J.; Zhang, K.; Maciejewska, M.; Miralles-Guasch, C. Temperature and Rain Moderate the Effect of Neighborhood Walkability on Walking Time for Seniors in Barcelona. Int. J. Environ. Res. Public Health 2020, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Tucker, P.; Gilliland, J. The Effect of Season and Weather on Physical Activity: A Systematic Review. Public Health 2007, 121, 909–922. [Google Scholar] [CrossRef]
- Amaya, V.; Moulaert, T.; Gwiazdzinski, L.; Vuillerme, N. Assessing and Qualifying Neighborhood Walkability for Older Adults: Construction and Initial Testing of a Multivariate Spatial Accessibility Model. Int. J. Environ. Res. Public Health 2022, 19, 1808. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Manzi, F.; Del Riccio, M.; Setola, N.; Naldi, E.; Milani, C.; Giorgetti, D.; Dellisanti, C.; Lorini, C. Impact of the Built Environment and the Neighborhood in Promoting the Physical Activity and the Healthy Aging in Older People: An Umbrella Review. Int. J. Environ. Res. Public Health 2020, 17, 6127. [Google Scholar] [CrossRef]
- Rosso, A.; Auchincloss, A.; Michael, Y. The Urban Built Environment and Mobility in Older Adults: A Comprehensive Review. J. Aging Res. 2011, 2011, 816106. [Google Scholar] [CrossRef]
- King, A.C.; Orpin, P.; Woodroffe, J.; Boyer, K. Eating and Ageing in Rural Australia: Applying Temporal Perspectives from Phenomenology to Uncover Meanings in Older Adults’ Experiences. Ageing Soc. 2017, 37, 753–776. [Google Scholar] [CrossRef]
- Mackay, M.; Nelson, T.; Perkins, H.C. Interpretive Walks: Advancing the Use of Mobile Methods in the Study of Entrepreneurial Farm Tourism Settings. Geogr. Res. 2018, 56, 167–175. [Google Scholar] [CrossRef]
- Lord, S.; Negron-Poblete, P.; Després, M. Vieillir chez soi dans la diversité des formes urbaines et rurales du Québec, Canada. Une exploration des enjeux d’aménagement des territoires vus par leurs habitants. Retraite Et Société 2017, 76, 43–66. [Google Scholar] [CrossRef]
- Cleland, V.; Sodergren, M.; Otahal, P.; Timperio, A.; Ball, K.; Crawford, D.; Salmon, J.; McNaughton, S.A. Associations Between the Perceived Environment and Physical Activity Among Adults Aged 55–65 Years: Does Urban-Rural Area of Residence Matter? J. Aging Phys. Act. 2015, 23, 55–63. [Google Scholar] [CrossRef]
- Jo, H.; Lee, H.H.; Kim, D.-H.; Kong, I.D. Satisfaction with the Walking-Related Environment during COVID-19 in South Korea. PLoS ONE 2022, 17, e0266183. [Google Scholar] [CrossRef] [PubMed]
- Bucko, A.G.; Porter, D.E.; Saunders, R.; Shirley, L.; Dowda, M.; Pate, R.R. Walkability Indices and Children’s Walking Behavior in Rural vs. Urban Areas. Health Place 2021, 72, 102707. [Google Scholar] [CrossRef] [PubMed]
- Damon, J.; Marchal, H.; Stébé, J.-M. Les sociologues et le périurbain: Découverte tardive, caractérisations mouvantes, controverses nourries. Rev. Française De Sociol. 2016, 57, 619–639. [Google Scholar] [CrossRef]
- Stébé, J.-M. L’INSEE et ses zonages: Au-delà de l’opposition urbain-rural. Constructif 2021, 60, 22–26. [Google Scholar] [CrossRef]
- Smith, L.K.; Lelas, J.L.; Kerrigan, D.C. Gender Differences in Pelvic Motions and Center of Mass Displacement during Walking: Stereotypes Quantified. J. Women’s Health Gend. -Based Med. 2002, 11, 453–458. [Google Scholar] [CrossRef]
- Akande, V.O.; Ruiter, R.A.C.; Kremers, S.P.J. Environmental and Motivational Determinants of Physical Activity among Canadian Inuit in the Arctic. Int. J. Environ. Res. Public Health 2019, 16, E2437. [Google Scholar] [CrossRef]
- Chapman, D.; Nilsson, K.L.; Rizzo, A.; Larsson, A. Winter City Urbanism: Enabling All Year Connectivity for Soft Mobility. Int. J. Environ. Res. Public Health 2019, 16, E1820. [Google Scholar] [CrossRef]
- Rosenberg, D.E.; Huang, D.L.; Simonovich, S.D.; Belza, B. Outdoor Built Environment Barriers and Facilitators to Activity among Midlife and Older Adults with Mobility Disabilities. Gerontologist 2013, 53, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Marcotte, J.; Grandisson, M.; Milot, É.; Dupéré, S. The Walking Interview: A Promising Method for Promoting the Participation of Autistic People in Research Projects. Int. J. Qual. Methods 2022, 21, 16094069221090064. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amaya, V.; Chardon, M.; Klein, H.; Moulaert, T.; Vuillerme, N. What Do We Know about the Use of the Walk-along Method to Identify the Perceived Neighborhood Environment Correlates of Walking Activity in Healthy Older Adults: Methodological Considerations Related to Data Collection—A Systematic Review. Sustainability 2022, 14, 11792. https://doi.org/10.3390/su141811792
Amaya V, Chardon M, Klein H, Moulaert T, Vuillerme N. What Do We Know about the Use of the Walk-along Method to Identify the Perceived Neighborhood Environment Correlates of Walking Activity in Healthy Older Adults: Methodological Considerations Related to Data Collection—A Systematic Review. Sustainability. 2022; 14(18):11792. https://doi.org/10.3390/su141811792
Chicago/Turabian StyleAmaya, Valkiria, Matthias Chardon, Helen Klein, Thibauld Moulaert, and Nicolas Vuillerme. 2022. "What Do We Know about the Use of the Walk-along Method to Identify the Perceived Neighborhood Environment Correlates of Walking Activity in Healthy Older Adults: Methodological Considerations Related to Data Collection—A Systematic Review" Sustainability 14, no. 18: 11792. https://doi.org/10.3390/su141811792