
External Ventricular Drainage: A Practical Guide for Neuro-Anesthesiologists
 , , ,
, , , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Discussion
3.1. Overview
3.2. EVD in Subarachnoid Hemorrhage
3.2.1. Intermittent vs. Continuous Drainage
3.2.2. Rapid vs. Gradual Weaning Strategy
3.3. EVD in Severe TBI
3.4. EVD in Intraparenchymal Hemorrhage with Intraventricular Involvement
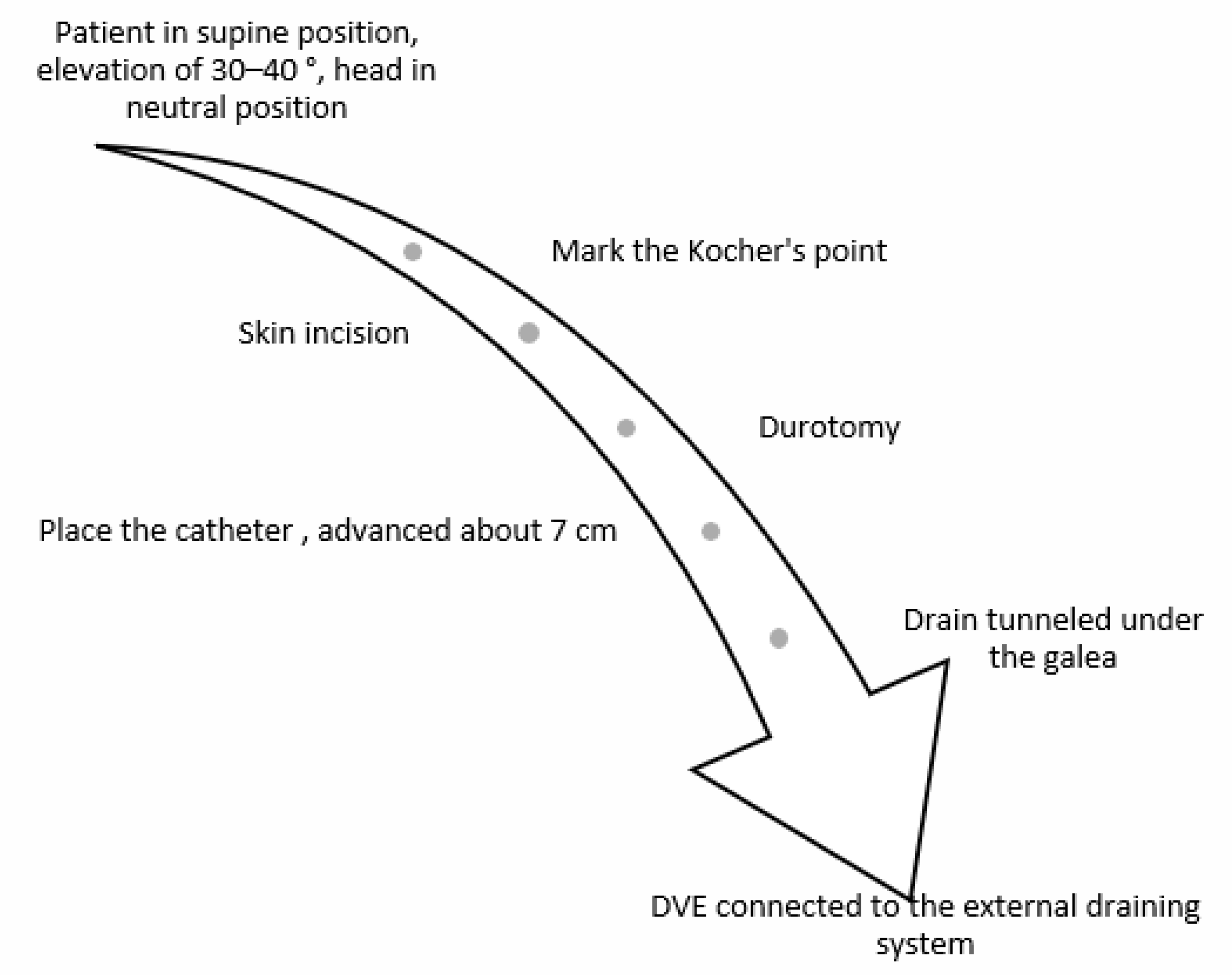
3.5. Surgical Technique
3.6. Complications
3.7. External Lumbar Drainage (ELD) for Refractory Intracranial Hypertension in Traumatic Brain Injury
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Srinivasan, V.M.; O’Neill, B.R.; Jho, D.; Whiting, D.M.; Oh, M.Y. The history of external ventricular drainage: Historical vignette. J. Neurosurg. 2014, 120, 228–236. [Google Scholar] [CrossRef]
- Bales, J.W.; Bonow, R.H.; Buckley, R.T.; Barber, J.; Temkin, N.; Chesnut, R.M. Primary External Ventricular Drainage Catheter Versus Intraparenchymal ICP Monitoring: Outcome Analysis. Neurocritical Care 2019, 31, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Longhitano, Y.; Iannuzzi, F.; Bonatti, G.; Zanza, C.; Messina, A.; Godoy, D.; Dabrowski, W.; Xiuyun, L.; Czosnyka, M.; Pelosi, P.; et al. Cerebral Autoregulation in Non-Brain Injured Patients: A Systematic Review. Front. Neurol. 2021, 12, 732176. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.Y.; Mayer, S.A.; Rordorf, G.A. External Ventricular Drains After Subarachnoid Hemorrhage: Is Less More? Neurocritical Care 2017, 28, 157–161. [Google Scholar] [CrossRef]
- Stevens, A.R.; Soon, W.C.; Chowdhury, Y.A.; Toman, E.; Yim, S.; Veenith, T.; Chelvarajah, R.; Belli, A.; Davies, D. External Lumbar Drainage for Refractory Intracranial Hypertension in Traumatic Brain Injury: A Systematic Review. Cureus 2022, 14, e30033. [Google Scholar] [CrossRef]
- Cinibulak, Z.; Aschoff, A.; Apedjinou, A.; Kaminsky, J.; Trost, H.A.; Krauss, J.K. Current practice of external ventricular drainage: A survey among neurosurgical departments in Germany. Acta Neurochir. 2016, 158, 847–853. [Google Scholar] [CrossRef]
- Schödel, P.; Proescholdt, M.; Ullrich, O.-W.; Brawanski, A.; Schebesch, K.-M. An outcome analysis of two different procedures of burr-hole trephine and external ventricular drainage in acute hydrocephalus. J. Clin. Neurosci. 2012, 19, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Foreman, P.M.; Hendrix, P.; Griessenauer, C.J.; Schmalz, P.G.; Harrigan, M.R. External ventricular drain placement in the intensive care unit versus operating room: Evaluation of complications and accuracy. Clin. Neurol. Neurosurg. 2015, 128, 94–100. [Google Scholar] [CrossRef]
- Altschul, D.; Hamad, M.K.; Kobets, A.; Fluss, R.; Lin, C.; Boyke, E.A.; Liu, J.; Thomas, R.; Unda, S.R. A Retrospective Quality Analysis of External Ventricular Drain Infection Rates Following Stroke Diagnoses and Other Brain Injuries: Comparison of Emergency Room and ICU/OR Setting. Cureus 2020, 12, e7173. [Google Scholar] [CrossRef] [Green Version]
- Dawod, G.; Henkel, N.; Karim, N.; Caras, A.; Qaqish, H.; Mugge, L.; Medhkour, A. Does the Setting of External Ventricular Drain Placement Affect Morbidity? A Systematic Literature Review Comparing Intensive Care Unit versus Operating Room Procedures. World Neurosurg. 2020, 140, 131–141. [Google Scholar] [CrossRef]
- Kohli, G.; Singh, R.; Herschman, Y.; Mammis, A. Infection Incidence Associated with External Ventriculostomy Placement: A Comparison of Outcomes in the Emergency Department, Intensive Care Unit, and Operating Room. World Neurosurg. 2018, 110, e135–e140. [Google Scholar] [CrossRef] [PubMed]
- Mikhaylov, Y.; Wilson, T.J.; Rajajee, V.; Thompson, B.G.; Maher, C.O.; Sullivan, S.E.; Jacobs, T.L.; Kocan, M.J.; Pandey, A.S. Efficacy of antibiotic-impregnated external ventricular drains in reducing ventriculostomy-associated infections. J. Clin. Neurosci. 2014, 21, 765–768. [Google Scholar] [CrossRef] [PubMed]
- Telano, L.N.; Baker, S. Physiology, Cerebral Spinal Fluid; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Sheppard, J.P.; Ong, V.; Lagman, C.; Udawatta, M.; Duong, C.; Nguyen, T.; Prashant, G.N.; Plurad, D.S.; Kim, D.Y.; Yang, I. Systemic Antimicrobial Prophylaxis and Antimicrobial-Coated External Ventricular Drain Catheters for Preventing Ventriculostomy-Related Infections: A Meta-Analysis of 5242 Cases. Neurosurgery 2018, 86, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Griffith, M.; Jang, H.J.; Ko, N.; Pelter, M.M.; Abba, J.; Vuong, M.; Tran, N.; Bushman, K.; Hu, X. Intracranial Pressure Monitoring via External Ventricular Drain: Are We Waiting Long Enough Before Recording the Real Value? J. Neurosci. Nurs. 2020, 52, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Palasz, J.; D’Antona, L.; Farrell, S.; Elborady, M.A.; Watkins, L.D.; Toma, A.K. External ventricular drain management in subarachnoid haemorrhage: A systematic review and meta-analysis. Neurosurg. Rev. 2021, 45, 365–373. [Google Scholar] [CrossRef]
- De Rooij, N.K.; Linn, F.H.H.; Van Der Plas, J.A.; Algra, A.; Rinkel, G.J.E. Incidence of subarachnoid haemorrhage: A systematic review with emphasis on region, age, gender and time trends. J. Neurol. Neurosurg. Psychiatry 2007, 78, 1365–1372. [Google Scholar] [CrossRef]
- Capion, T.; Lilja-Cyron, A.; Juhler, M.; Mathiesen, T.I.; Wetterslev, J. Prompt closure versus gradual weaning of extraventricular drainage for hydrocephalus in adult patients with aneurysmal subarachnoid haemorrhage: A systematic review protocol with meta-analysis and trial sequential analysis. BMJ Open 2019, 9, e029719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nornes, H. The role of intracranial pressure in the arrest of hemorrhage in patients with ruptured intracranial aneurysm. J. Neurosurg. 1973, 39, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Wang, W.; Cheng, F.; Yuan, Q.; Yang, J.; Hu, J.; Ren, G. External Ventricular Drains versus Intraparenchymal Intracranial Pressure Monitors in Traumatic Brain Injury: A Prospective Observational Study. World Neurosurg. 2015, 83, 794–800. [Google Scholar] [CrossRef]
- Kim, G.S.; Amato, A.; James, M.; Britz, G.W.; Zomorodi, A.; Graffagnino, C.; Olson, D.M. Continuous and Intermittent CSF Diversion after Subarachnoid Hemorrhage: A Pilot Study. Neurocritical Care 2011, 14, 68–72. [Google Scholar] [CrossRef]
- Olson, D.; Zomorodi, M.; Britz, G.W.; Zomorodi, A.R.; Amato, A.; Graffagnino, C. Continuous cerebral spinal fluid drainage associated with complications in patients admitted with subarachnoid hemorrhage. J. Neurosurg. 2013, 119, 974–980. [Google Scholar] [CrossRef] [PubMed]
- Leeds, E.S.; Kong, A.K.; Wise, B.L. Alternative pathways for drainage of cerebrospinal fluid in the canine brain. Lymphology 1989, 22, 144–146. [Google Scholar]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2016, 80, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Klopfenstein, J.D.; Kim, L.J.; Feiz-Erfan, I.; Hott, J.S.; Goslar, P.; Zabramski, J.M.; Spetzler, R.F. Comparison of rapid and gradual weaning from external ventricular drainage in patients with aneurysmal subarachnoid hemorrhage: A prospective randomized trial. J. Neurosurg. 2004, 100, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Mostofi, K.; Samii, M. Secondary communicating hydrocephalus management by implantation of external ventricular shunt and minimal gradual increase of cerebrospinal fluid pressure. Asian J. Neurosurg. 2017, 12, 194–198. [Google Scholar] [CrossRef]
- Chung, D.Y.; Thompson, B.B.; Kumar, M.A.; Mahta, A.; Rao, S.S.; Lai, J.H.; Tadevosyan, A.; Kessler, K.; Locascio, J.J.; Patel, A.B.; et al. Association of External Ventricular Drain Wean Strategy with Shunt Placement and Length of Stay in Subarachnoid Hemorrhage: A Prospective Multicenter Study. Neurocritical Care 2021, 36, 536–545. [Google Scholar] [CrossRef]
- Jabbarli, R.; Pierscianek, D.; Rölz, R.; Reinhard, M.; Oppong, M.D.; Scheiwe, C.; Dammann, P.; Kaier, K.; Wrede, K.H.; Shah, M.; et al. Gradual External Ventricular Drainage Weaning Reduces the Risk of Shunt Dependency After Aneurysmal Subarachnoid Hemorrhage: A Pooled Analysis. Oper. Neurosurg. 2018, 15, 498–504. [Google Scholar] [CrossRef]
- Chung, D.Y.; Olson, D.M.; John, S.; Mohamed, W.; Kumar, M.A.; Thompson, B.B.; Rordorf, G.A. Evidence-Based Management of External Ventricular Drains. Curr. Neurol. Neurosci. Rep. 2019, 19, 94. [Google Scholar] [CrossRef]
- Chau, C.Y.C.; Craven, C.L.; Rubiano, A.M.; Adams, H.; Tülü, S.; Czosnyka, M.; Servadei, F.; Ercole, A.; Hutchinson, P.J.; Kolias, A.G. The Evolution of the Role of External Ventricular Drainage in Traumatic Brain Injury. J. Clin. Med. 2019, 8, 1422. [Google Scholar] [CrossRef] [Green Version]
- Zanza, C.; Piccolella, F.; Racca, F.; Romenskaya, T.; Longhitano, Y.; Franceschi, F.; Savioli, G.; Bertozzi, G.; De Simone, S.; Cipolloni, L.; et al. Ketamine in Acute Brain Injury: Current Opinion Following Cerebral Circulation and Electrical Activity. Healthcare 2022, 10, 566. [Google Scholar] [CrossRef]
- Nieuwkamp, D.J.; De Gans, K.; Rinkel, G.J.E.; Algra, A. Treatment and outcome of severe intraventricular extension in patients with subarachnoid or intracerebral hemorrhage: A systematic review of the literature. J. Neurol. 2000, 247, 117–121. [Google Scholar] [CrossRef]
- Nieuwkamp, D.J.; Verweij, B.H.; Rinkel, G.J.E. Massive intraventricular haemorrhage from aneurysmal rupture: Patient proportions and eligibility for intraventricular fibrinolysis. J. Neurol. 2010, 257, 354–358. [Google Scholar] [CrossRef] [Green Version]
- Naff, N.J.; Hanley, D.F.; Keyl, P.M.; Tuhrim, S.; Kraut, M.; Bederson, J.; Bullock, R.; Mayer, S.A.; Schmutzhard, E. Intraventricular Thrombolysis Speeds Blood Clot Resolution: Results of a Pilot, Prospective, Randomized, Double-blind, Controlled Trial. Neurosurgery 2004, 54, 577–584. [Google Scholar] [CrossRef]
- Burke, J.F.; Magill, S.T. Letter: Craniometrics and Ventricular Access: A Review of Kocher’s, Kaufman’s, Paine’s, Menovksy’s, Tubbs’, Keen’s, Frazier’s, Dandy’s, and Sanchez’s Points. Oper. Neurosurg. 2020, 19, E550–E551. [Google Scholar] [CrossRef] [PubMed]
- Konovalov, A.N.; Grebenev, F.V.; Rybakov, V.A.; Pilipenko, Y.V.; Shekhtman, O.D.; Okishev, D.N.; Yershova, O.N.; Eliava, S.S. External Ventricular Drainage Complication Risks and Accuracy Analysis. World Neurosurg. 2021, 156, e276–e282. [Google Scholar] [CrossRef] [PubMed]
- Kerry, G.; Holtmannspoetter, M.; Kubitz, J.C.; Steiner, H.-H. Factors which influence the complications of external ventricular cerebrospinal fluid drainage. Acta Neurochir. 2021, 164, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Romenskaya, T.; Longhitano, Y.; Piccolella, F.; Berger, J.M.; Artico, M.; Taurone, S.; Maconi, A.; Saviano, A.; Caramuta, M.; Savioli, G.; et al. Cerebral Vasospasm: Practical Review of Diagnosis and Management. Rev. Recent Clin. Trials 2022, 17, 1. [Google Scholar] [CrossRef]
- Ramanan, M.; Lipman, J.; Shorr, A.; Shankar, A. A meta-analysis of ventriculostomy-associated cerebrospinal fluid infections. BMC Infect. Dis. 2015, 15, 3. [Google Scholar] [CrossRef] [Green Version]
- Abulhasan, Y.B.; Al-Jehani, H.; Valiquette, M.A.; McMAnus, A.; Dolan-Cake, M.; Ayoub, O.; Angle, M.; Teitelbaum, J. Lumbar drainage for the treatment of severe bacterial meningitis. Neurocritical Care 2013, 19, 199–205. [Google Scholar] [CrossRef]
- Ginalis, E.E.; Fernández, L.L.; Ávila, J.P.; Aristizabal, S.; Rubiano, A.M. A review of external lumbar drainage for the management of intracranial hypertension in traumatic brain injury. Neurochirurgie 2022, 68, 206–211. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, H.; Zhang, K.; Daneshnia, F.; Fang, W.; He, P.; Kuang, W.; Jiang, G.; Chen, M.; Pan, W.; et al. Lumbar drainage for the treatment of refractory intracranial hypertension in HIV-negative cryptococcal meningitis. Future Microbiol. 2019, 14, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Hawryluk, G.W.; Aguilera, S.; Buki, A.; Bulger, E.; Citerio, G.; Cooper, D.J.; Arrastia, R.D.; Diringer, M.; Figaji, A.; Gao, G.; et al. A management algorithm for patients with intracranial pressure monitoring: The Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med. 2019, 45, 1783–1794. [Google Scholar] [CrossRef] [Green Version]
- Jamjoom, A.A.B.; Joannides, A.J.; Poon, M.T.-C.; Chari, A.; Zaben, M.; Abdulla, M.A.H.; Roach, J.; Glancz, L.J.; Solth, A.; Duddy, J.; et al. Prospective, multicentre study of external ventricular drainage-related infections in the UK and Ireland. J. Neurol. Neurosurg. Psychiatry 2018, 89, 120–126. [Google Scholar] [CrossRef] [Green Version]
- Abadal-Centellas, J.M.; Llompart-Pou, J.A.; Homar-Ramírez, J.; Pérez-Bárcena, J.; Rosselló-Ferrer, A.; Ibáñez-Juvé, J. Neurologic outcome of posttraumatic refractory intracranial hypertension treated with external lumbar drainage. J. Trauma 2007, 62, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.I.; Rekate, H.L.; Cherny, W.B.; Manwaring, K.; Moss, S.D.; Baldwin, H.Z. Controlled lumbar drainage in pediatric head injury. J. Neurosurg. 1995, 83, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Murad, A.; Ghostine, S.; Colohan, A.R. A case for further investigating the use of controlled lumbar cerebrospinal fluid drainage for the control of intracranial pressure. World Neurosurg. 2012, 77, 160–165. [Google Scholar] [CrossRef]
- Tuettenberg, J.; Czabanka, M.; Horn, P.; Woitzik, J.; Barth, M.; Thomé, C.; Vajkoczy, P.; Schmiedek, P.; Muench, E. Clinical evaluation of the safety and efficacy of lumbar cerebrospinal fluid drainage for the treatment of refractory increased intracranial pressure. J. Neurosurg. 2009, 110, 1200–1208. [Google Scholar] [CrossRef] [Green Version]
- Bauer, M.; Sohm, F.; Thomé, C.; Ortler, M. Refractory intracranial hypertension in traumatic brain injury: Proposal for a novel score to assess the safety of lumbar cerebrospinal fluid drainage. Surg. Neurol. Int. 2017, 8, 265. [Google Scholar] [CrossRef]
- Llompart-Pou, J.A.; Abadal, J.M.; Pérez-Bárcena, J.; Molina, M.; Brell, M.; Ibáñez, J.; Raurich, J.-M.; Homar, J. Long-term follow-up of patients with post-traumatic refractory high intracranial pressure treated with lumbar drainage. Anaesth. Intensive Care. 2011, 39, 79–83. [Google Scholar] [CrossRef] [Green Version]
- Manet, R.; Payen, J.-F.; Guerin, R.; Martinez, O.; Hautefeuille, S.; Francony, G.; Gergele, L. Using external lumbar CSF drainage to treat communicating external hydrocephalus in adult patients after acute traumatic or nontraumatic brain injury. Acta Neurochir 2017, 159, 2003–2009. [Google Scholar] [CrossRef]
- Schade, R.P.; Schinkel, J.; Visser, L.G.; Van Dijk, J.M.; Voormolen, J.H.; Kuijper, E.J. Bacterial meningitis caused by the use of ventricular or lumbar cerebrospinal fluid catheters. J. Neurosurg. 2005, 102, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Coplin, W.M.; Avellino, A.M.; Kim, D.K.; Winn, H.R.; Grady, M.S. Bacterial meningitis associated with lumbar drains: A retrospective cohort study. J. Neurol. Neurosurg. Psychiatry 1999, 67, 468–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bota, D.P.; Lefranc, F.; Vilallobos, H.R.; Brimioulle, S.; Vincent, J.-L. Ventriculostomy-related infections in critically ill patients: A 6-year experience. J. Neurosurg. 2005, 103, 468–472. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertuccio, A.; Marasco, S.; Longhitano, Y.; Romenskaya, T.; Elia, A.; Mezzini, G.; Vitali, M.; Zanza, C.; Barbanera, A. External Ventricular Drainage: A Practical Guide for Neuro-Anesthesiologists. Clin. Pract. 2023, 13, 219-229. https://doi.org/10.3390/clinpract13010020
Bertuccio A, Marasco S, Longhitano Y, Romenskaya T, Elia A, Mezzini G, Vitali M, Zanza C, Barbanera A. External Ventricular Drainage: A Practical Guide for Neuro-Anesthesiologists. Clinics and Practice. 2023; 13(1):219-229. https://doi.org/10.3390/clinpract13010020
Chicago/Turabian StyleBertuccio, Alessandro, Stefano Marasco, Yaroslava Longhitano, Tatsiana Romenskaya, Angela Elia, Gianluca Mezzini, Matteo Vitali, Christian Zanza, and Andrea Barbanera. 2023. "External Ventricular Drainage: A Practical Guide for Neuro-Anesthesiologists" Clinics and Practice 13, no. 1: 219-229. https://doi.org/10.3390/clinpract13010020