

Bevacizumab-Induced Thrombotic Microangiopathy (TMA) in Metastatic Lung Adenocarcinoma Patients Receiving Nivolumab Combined with Bevacizumab, Carboplatin and Paclitaxel: Two Case Reports

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Clinical Practice Points
- Drug-induced nephrotoxicity is an uncommon but threatening adverse effect when using ICIs combined with bevacizumab and chemotherapy.
- A kidney biopsy is indicated for metastatic non-squamous cell lung cancer patients experiencing nephrotoxicity during this combination therapy.
2. Introduction
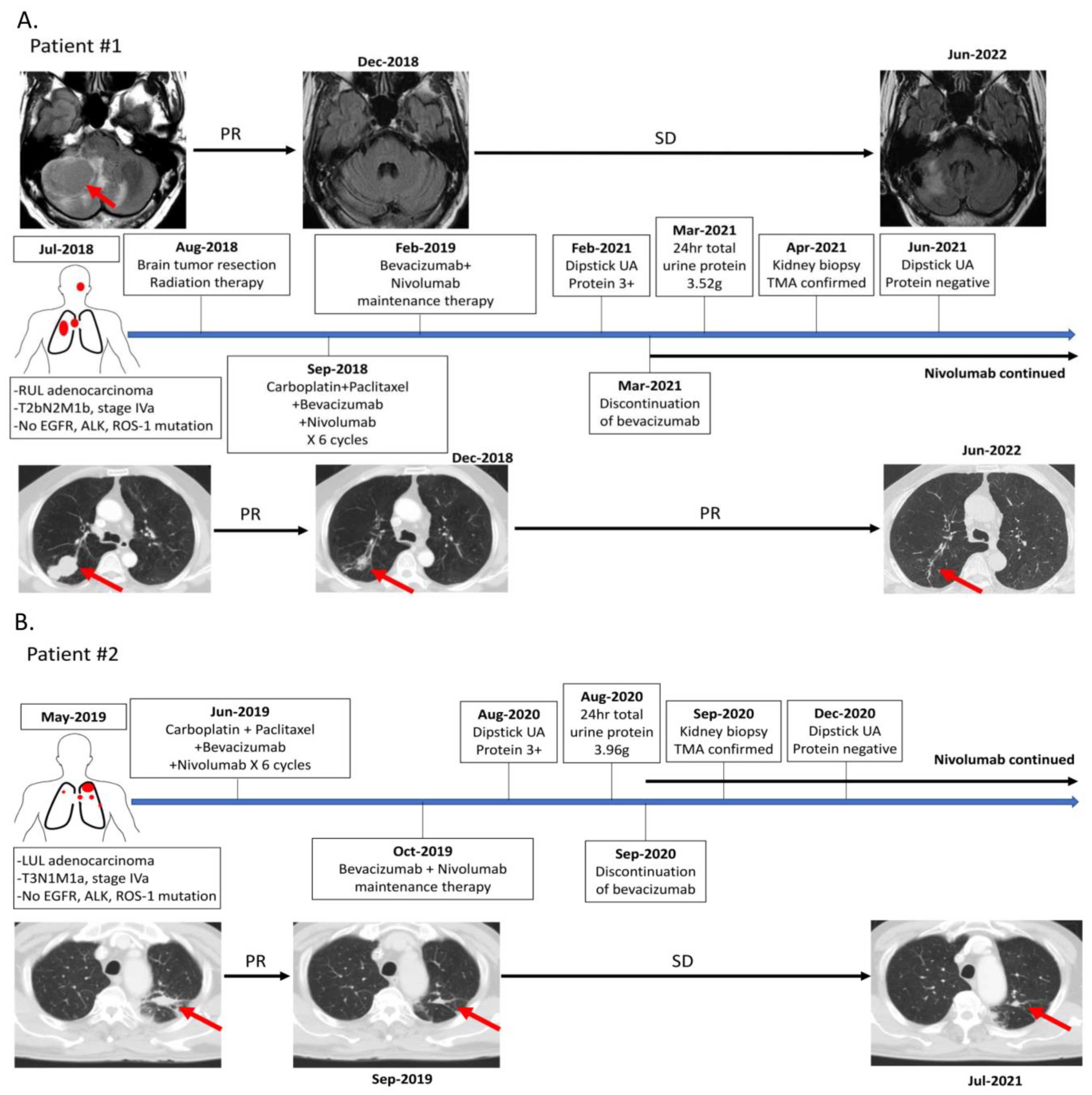
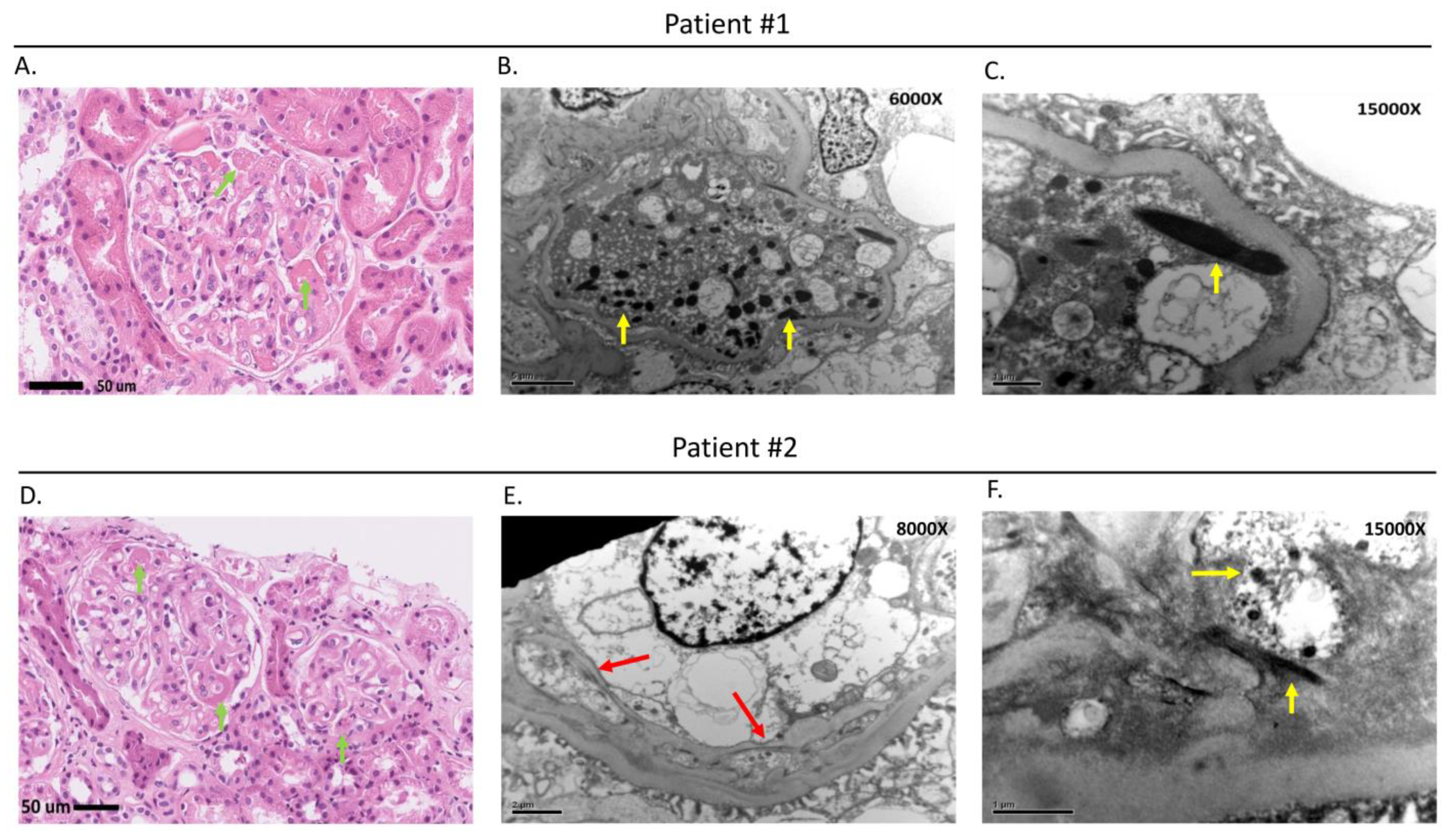
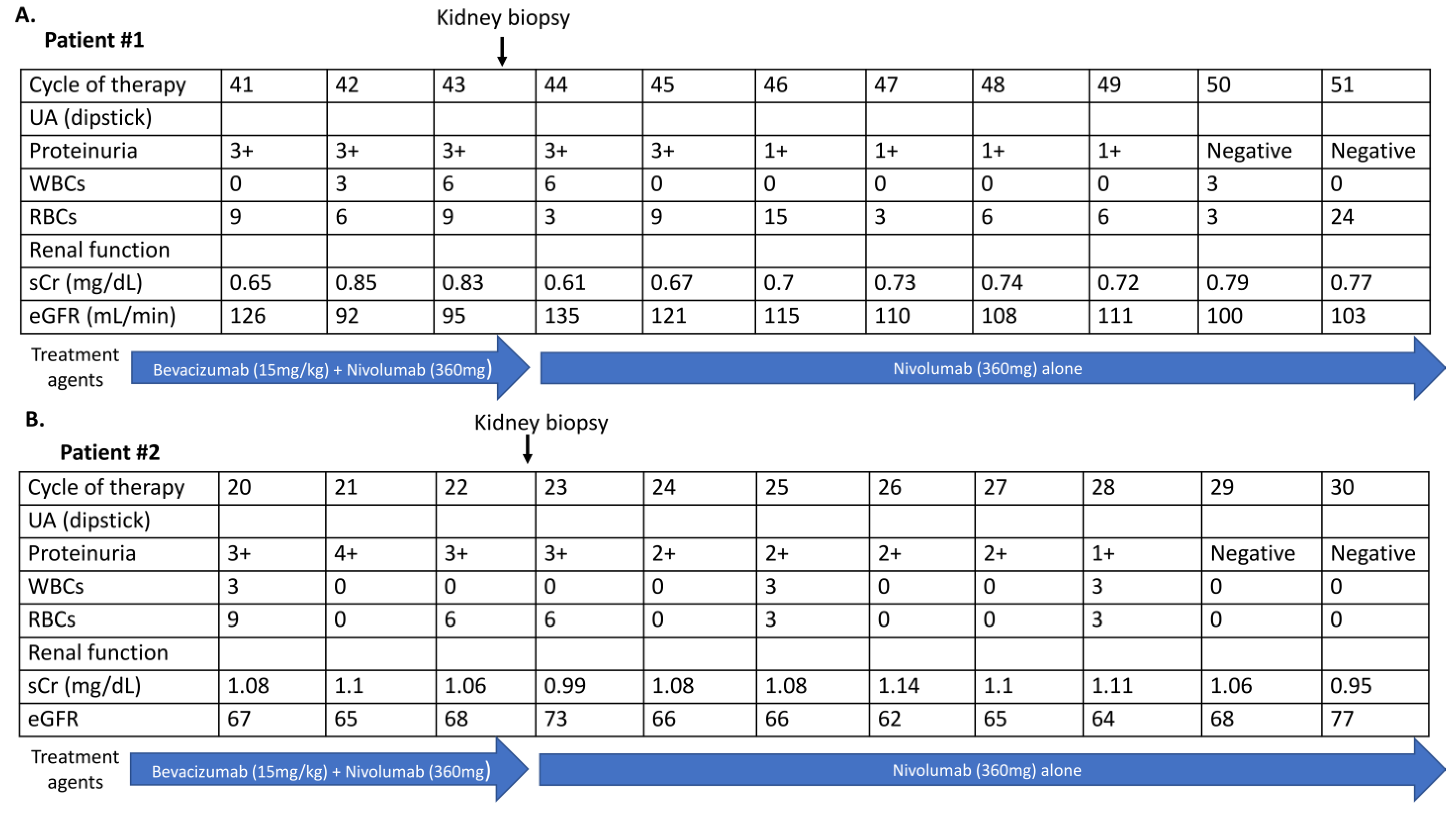
3. Case Presentation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sugawara, S.; Lee, J.S.; Kang, J.H.; Kim, H.R.; Inui, N.; Hida, T.; Lee, K.H.; Yoshida, T.; Tanaka, H.; Yang, C.T.; et al. Nivolumab with carboplatin, paclitaxel, and bevacizumab for first-line treatment of advanced nonsquamous non-small-cell lung cancer. Ann. Oncol. 2021, 32, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Xu, X.; Ge, W.; Lei, J.; Cao, D. The association between immune-related adverse events and the prognosis of solid cancer patients treated with immunotherapy: A systematic review and meta-analysis. Ther. Adv. Med. Oncol. 2020, 12, 1758835920980546. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Eremina, V.; Jefferson, J.A.; Kowalewska, J.; Hochster, H.; Haas, M.; Weisstuch, J.; Richardson, C.; Kopp, J.B.; Kabir, M.G.; Backx, P.H.; et al. VEGF inhibition and renal thrombotic microangiopathy. N. Engl. J. Med. 2008, 358, 1129–1136. [Google Scholar] [CrossRef]
- Perazella, M.A.; Izzedine, H. New drug toxicities in the onco-nephrology world. Kidney Int. 2015, 87, 909–917. [Google Scholar] [CrossRef] [Green Version]
- Cortazar, F.B.; Marrone, K.A.; Troxell, M.L.; Ralto, K.M.; Hoenig, M.P.; Brahmer, J.R.; Le, D.T.; Lipson, E.J.; Glezerman, I.G.; Wolchok, J.; et al. Clinicopathological features of acute kidney injury associated with immune checkpoint inhibitors. Kidney Int. 2016, 90, 638–647. [Google Scholar] [CrossRef] [Green Version]
- Meraz-Muñoz, A.; Amir, E.; Ng, P.; Avila-Casado, C.; Ragobar, C.; Chan, C.; Kim, J.; Wald, R.; Kitchlu, A. Acute kidney injury associated with immune checkpoint inhibitor therapy: Incidence, risk factors and outcomes. J. Immunother. Cancer 2020, 8, e000467. [Google Scholar] [CrossRef]
- Wanchoo, R.; Karam, S.; Uppal, N.N.; Barta, V.S.; Deray, G.; Devoe, C.; Launay-Vacher, V.; Jhaveri, K.D. Cancer and Kidney International Network Workgroup on Immune Checkpoint Inhibitors. Adverse Renal Effects of Immune Checkpoint Inhibitors: A Narrative Review. Am. J. Nephrol. 2017, 45, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Lin, Y.C.; Chiu, L.C.; Ju, J.S.; Tung, P.H.; Huang, A.C.; Li, S.H.; Fang, Y.F.; Chen, C.H.; Kuo, S.C.; et al. Comparison of afatinib and erlotinib combined with bevacizumab in untreated stage IIIB/IV epidermal growth factor receptor-mutated lung adenocarcinoma patients: A multicenter clinical analysis study. Ther. Adv. Med. Oncol. 2022, 14, 17588359221113278. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, P.-C.; Chen, T.-D.; Tsai, T.-Y.; Yang, C.-T. Bevacizumab-Induced Thrombotic Microangiopathy (TMA) in Metastatic Lung Adenocarcinoma Patients Receiving Nivolumab Combined with Bevacizumab, Carboplatin and Paclitaxel: Two Case Reports. Clin. Pract. 2023, 13, 200-205. https://doi.org/10.3390/clinpract13010018
Hsu P-C, Chen T-D, Tsai T-Y, Yang C-T. Bevacizumab-Induced Thrombotic Microangiopathy (TMA) in Metastatic Lung Adenocarcinoma Patients Receiving Nivolumab Combined with Bevacizumab, Carboplatin and Paclitaxel: Two Case Reports. Clinics and Practice. 2023; 13(1):200-205. https://doi.org/10.3390/clinpract13010018
Chicago/Turabian StyleHsu, Ping-Chih, Tai-Di Chen, Tsung-Yu Tsai, and Cheng-Ta Yang. 2023. "Bevacizumab-Induced Thrombotic Microangiopathy (TMA) in Metastatic Lung Adenocarcinoma Patients Receiving Nivolumab Combined with Bevacizumab, Carboplatin and Paclitaxel: Two Case Reports" Clinics and Practice 13, no. 1: 200-205. https://doi.org/10.3390/clinpract13010018