
Assessment of the Antimalarial Treatment Failure in Ebonyi State, Southeast Nigeria

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Sampling
2.3. Chemical Analysis of Sample (Antimalarial Drugs)
2.4. Ethical Consideration
2.5. Statistical Analysis
3. Results and Discussion
3.1. Survey
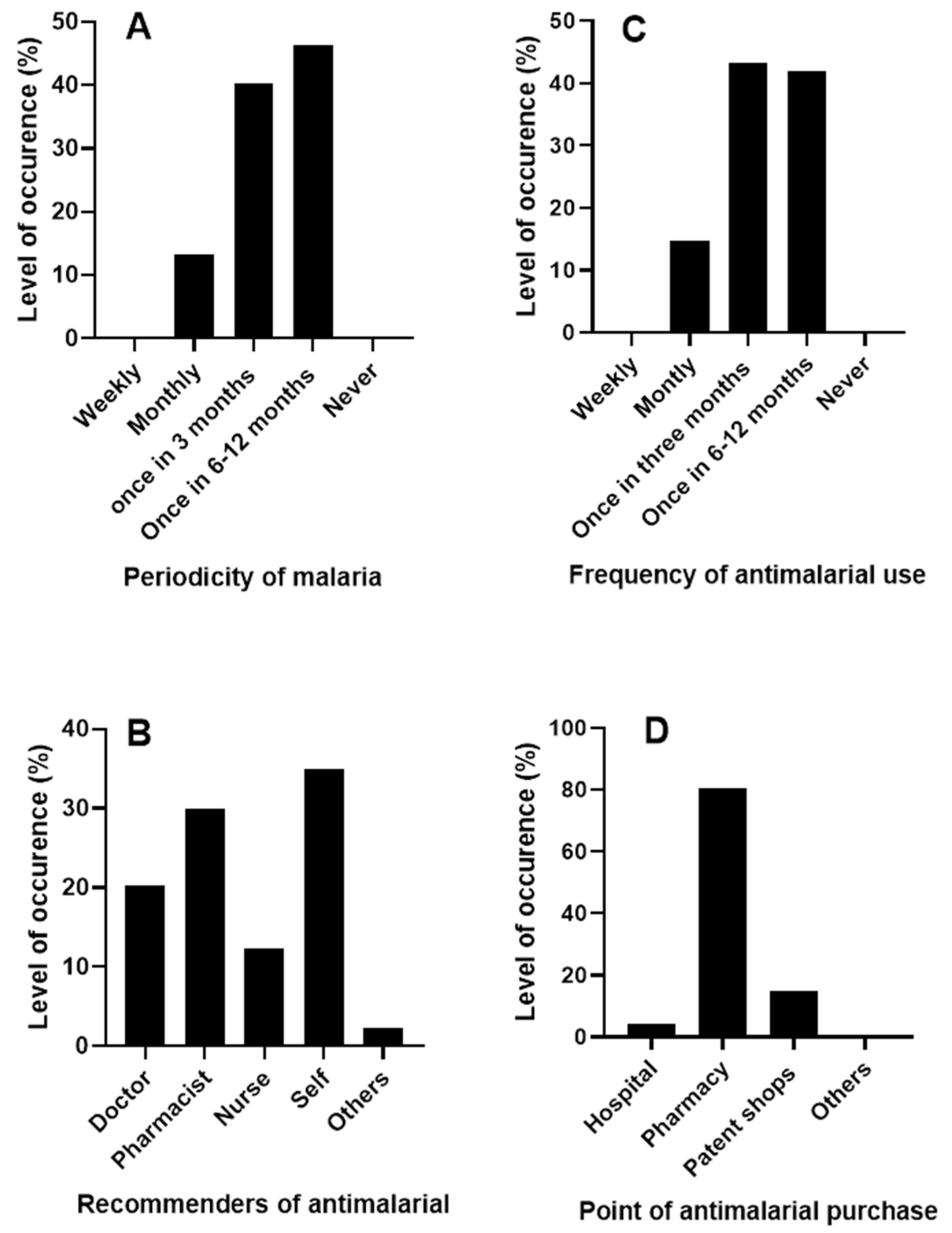
3.1.1. Patient Survey
- Periodicity of malaria and antimalarial drug use
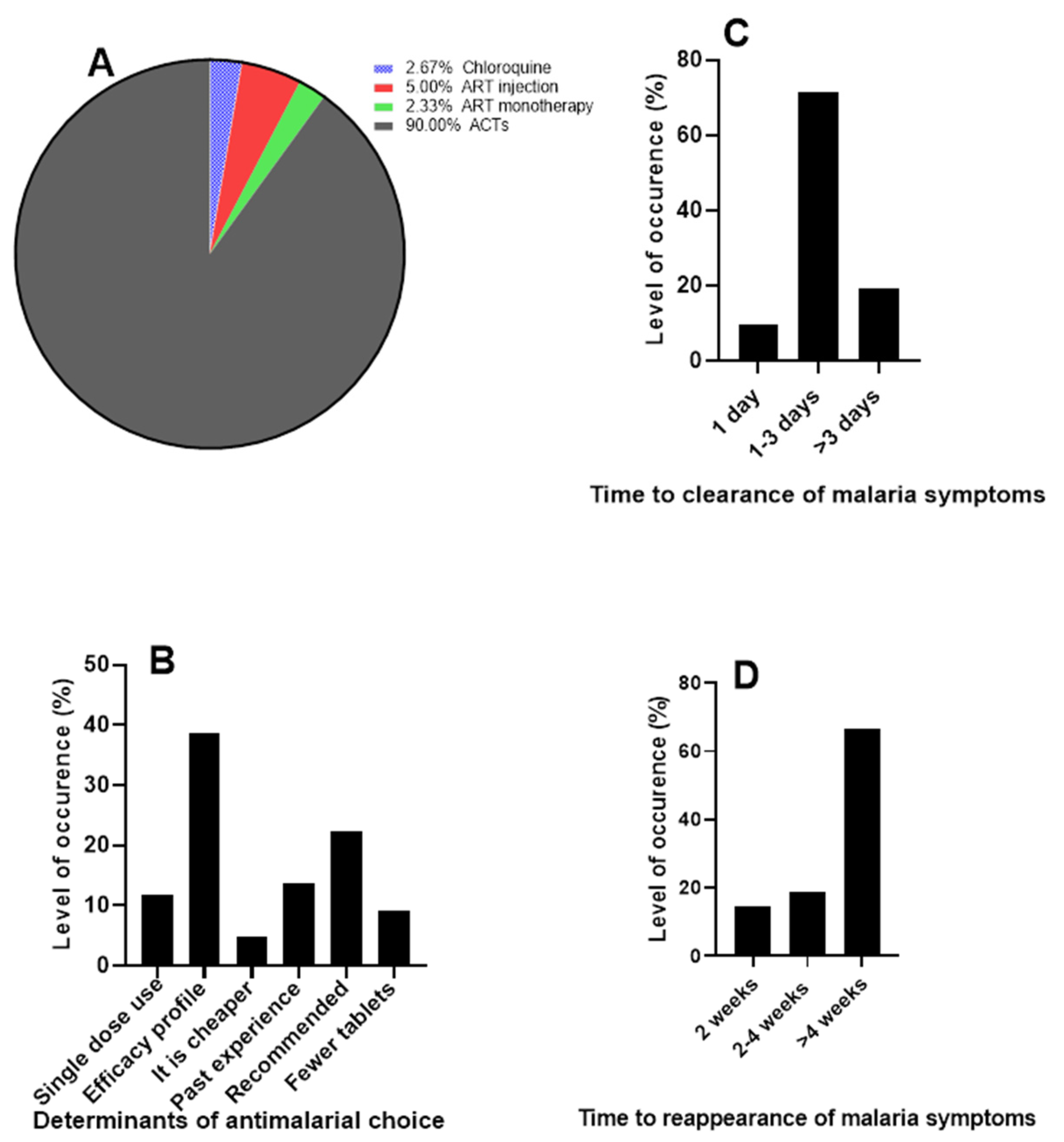
- Choice of antimalarial in use and clearance of malaria signs and symptoms
- Patients’ satisfaction with antimalarial drugs
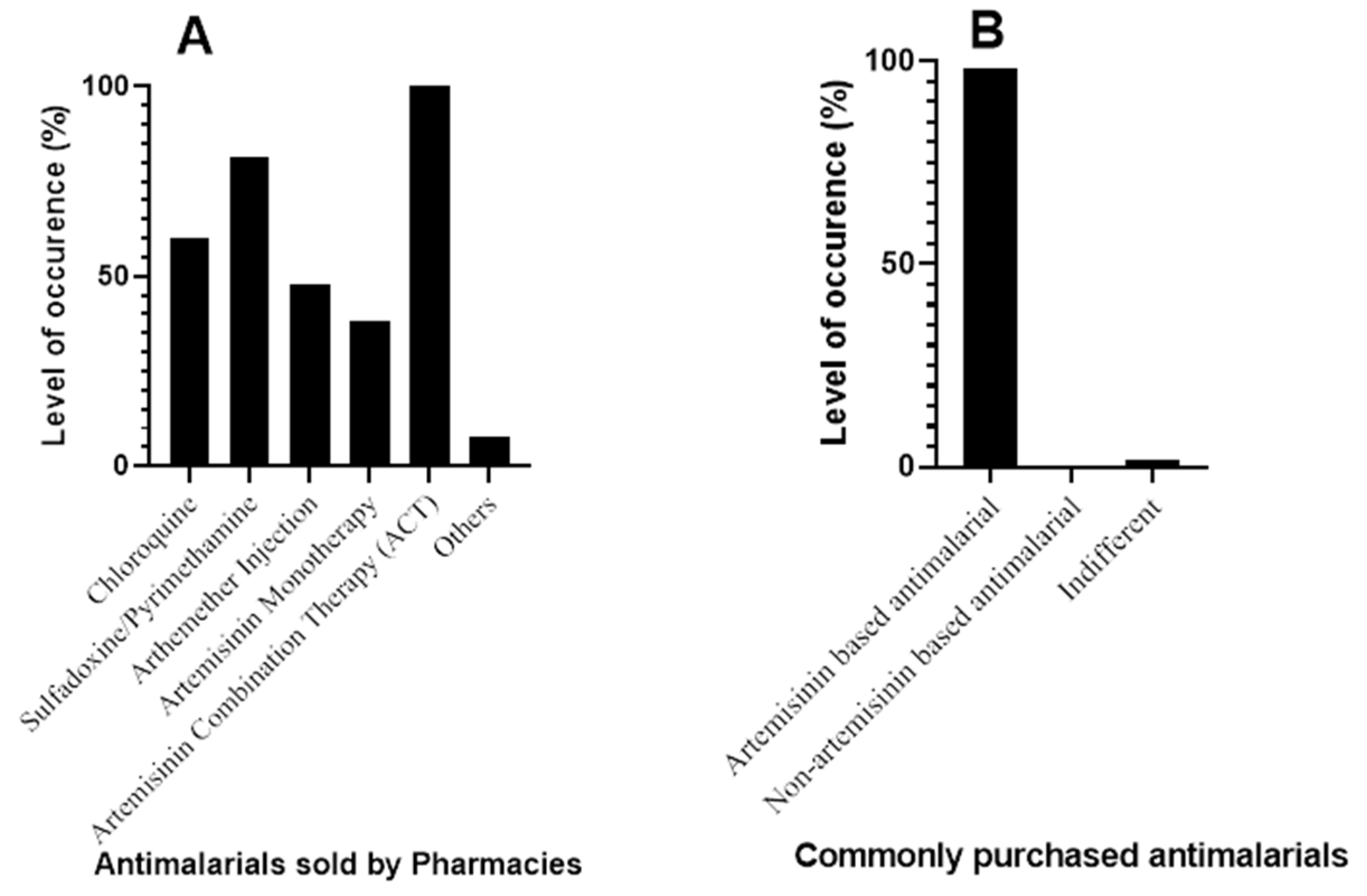
3.1.2. Pharmacy Survey
- Antimalarials used for malaria treatment
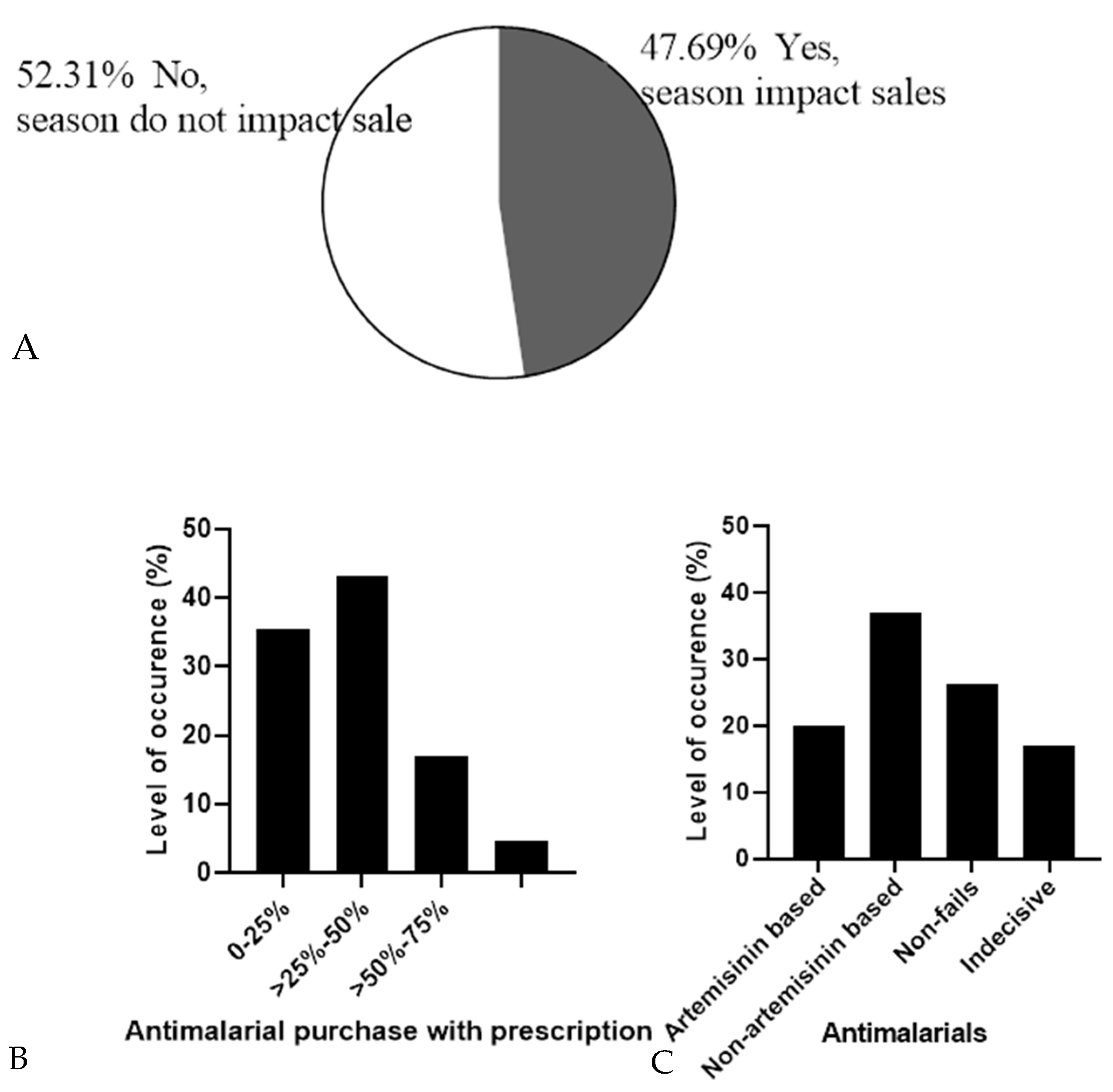
- Pattern of antimalarial drug prescription
- Measurement of malaria relapse by sentiment level of pharmacies
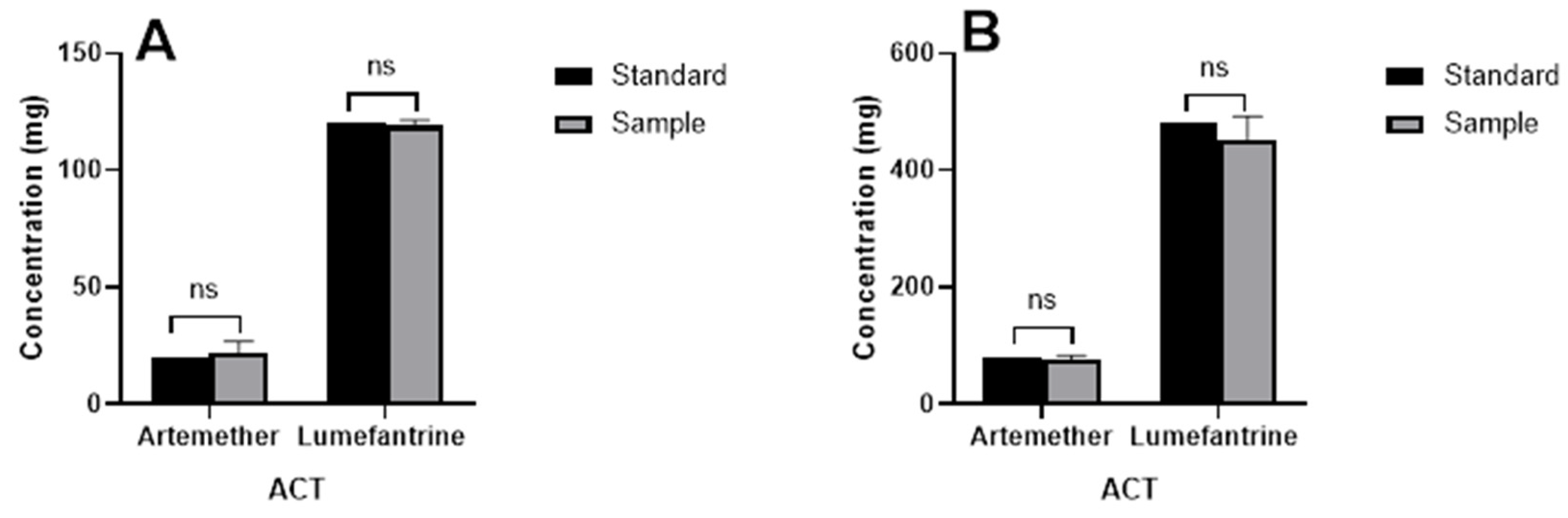
3.2. Active Pharmaceutical Ingredient in Antimalarial Drugs
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. World Malaria Report 2021. Available online: https://www.who.int/publications/i/item/9789240040496 (accessed on 3 January 2022).
- WHO. World Malaria Report 2020: 20 Years of Global Progress and Challenges. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2020 (accessed on 30 November 2020).
- Walker, E.J.; Peterson, G.M.; Grech, J.; Paragalli, E.; Thomas, J. Are we doing enough to prevent poor-quality antimalarial medicines in the developing world? BMC Public Health 2018, 18, 630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Vugt, M.; van Beest, A.; Sicuri, E.; van Tulder, M.; Grobusch, M.P. Malaria treatment and prophylaxis in endemic and nonendemic countries: Evidence on strategies and their cost–effectiveness. Future Microbiol. 2011, 6, 1485–1500. [Google Scholar] [CrossRef]
- Newton, P.N.; Green, M.D.; Mildenhall, D.C.; Plançon, A.; Nettey, H.; Nyadong, L.; Hostetler, D.M.; Swamidoss, I.; Harris, G.A.; Powell, K.; et al. Poor quality vital anti-malarials in Africa—An urgent neglected public health priority. Malar. J. 2011, 10, 352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. 1 in 10 Medical Products in Developing Countries is Substandard or Falsified. Available online: https://www.who.int/news-room/detail/28-11-2017-1-in-10-medical-products-in-developing-countries-is-substandard-or-falsified (accessed on 3 July 2021).
- Tabernero, P.; Fernández, F.M.; Green, M.; Guerin, P.J.; Newton, P.N. Mind the gaps—The epidemiology of poor-quality anti-malarials in the malarious world—Analysis of the WorldWide Antimalarial Resistance Network database. Malar. J. 2014, 13, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, S.; Weiss, D.J.; Cameron, E.; Bisanzio, D.; Mappin, B.; Dalrymple, U.; Battle, K.E.; Moyes, C.L.; Henry, A.; Eckhoff, P.A.; et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015, 526, 207–211. [Google Scholar] [CrossRef] [Green Version]
- Lalani, M.; Kaur, H.; Mohammed, N.; Mailk, N.; Wyk, A.; van Jan, S.; Kakar, R.M.; Mojadidi, M.K.; Leslie, T. Substandard Antimalarials Available in Afghanistan: A Case for Assessing the Quality of Drugs in Resource Poor Settings. Am. J. Trop. Med. Hyg. 2015, 92, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.A.; Tan, M.S.Y.; Bisson, C.; Borg, A.; Umrekar, T.R.; Hackett, F.; Hale, V.L.; Vizcay-Barrena, G.; Fleck, R.A.; Snijders, A.P.; et al. A protease cascade regulates release of the human malaria parasite Plasmodium falciparum from host red blood cells. Nat. Microbiol. 2018, 3, 447–455. [Google Scholar] [CrossRef]
- Yewhalaw, D.; Wassie, F.; Steurbaut, W.; Spanoghe, P.; Van Bortel, W.; Denis, L.; Tessema, D.A.; Getachew, Y.; Coosemans, M.; Duchateau, L.; et al. Multiple Insecticide Resistance: An Impediment to Insecticide-Based Malaria Vector Control Program. PLoS ONE 2011, 6, e16066. [Google Scholar] [CrossRef] [Green Version]
- Newton, P.N.; Green, M.D.; Fernández, F.M. Impact of poor-quality medicines in the “developing” world. Trends Pharmacol. Sci. 2010, 31, 99–101. [Google Scholar] [CrossRef] [Green Version]
- Newton, P.N.; Caillet, C.; Guerin, P.J. A link between poor quality antimalarials and malaria drug resistance? Expert Rev. Anti. Infect. Ther. 2016, 14, 531–533. [Google Scholar] [CrossRef]
- Newton, P.N.; Amin, A.A.; Bird, C.; Passmore, P.; Dukes, G.; Tomson, G.; Simons, B.; Bate, R.; Guerin, P.J.; White, N.J. The primacy of public health considerations in defining poor quality medicines. PLoS Med. 2011, 8, e1001139. [Google Scholar] [CrossRef] [Green Version]
- Kelesidis, T.; Falagas, M.E. Substandard/Counterfeit Antimicrobial Drugs. Clin. Microbiol. Rev. 2015, 28, 443–464. [Google Scholar] [CrossRef] [Green Version]
- White, N.J.; Pongtavornpinyo, W.; Maude, R.J.; Saralamba, S.; Aguas, R.; Stepniewska, K.; Lee, S.J.; Dondorp, A.M.; White, L.J.; Day, N.P. Hyperparasitaemia and low dosing are an important source of anti-malarial drug resistance. Malar. J. 2009, 8, 253. [Google Scholar] [CrossRef] [Green Version]
- Karunamoorthi, K. The counterfeit anti-malarial is a crime against humanity: A systematic review of the scientific evidence. Malar. J. 2014, 13, 209. [Google Scholar] [CrossRef] [Green Version]
- Onwujekwe, O.; Kaur, H.; Dike, N.; Shu, E.; Uzochukwu, B.; Hanson, K.; Okoye, V.; Okonkwo, P. Quality of anti-malarial drugs provided by public and private healthcare providers in south-east Nigeria. Malar. J. 2009, 8, 22. [Google Scholar] [CrossRef] [Green Version]
- Chimezie, R.O. Malaria Hyperendemicity: The Burden and Obstacles to Eradication in Nigeria. J. Biosci. Med. 2020, 8, 165–178. [Google Scholar] [CrossRef]
- Shafie, M.; Eyasu, M.; Muzeyin, K.; Worku, Y.; Martín-Aragón, S. Prevalence and determinants of self-medication practice among selected households in Addis Ababa community. PLoS ONE 2018, 13, e0194122. [Google Scholar] [CrossRef] [Green Version]
- Esan, D.T.; Fasoro, A.A.; Odesanya, O.E.; Esan, T.O.; Ojo, E.F.; Faeji, C.O. Assessment of Self-Medication Practices and Its Associated Factors among Undergraduates of a Private University in Nigeria. J. Environ. Public Health 2018, 2018, 5439079. [Google Scholar] [CrossRef] [Green Version]
- Voorberg-van der Wel, A.; Kocken, C.H.M.; Zeeman, A.M. Modeling Relapsing Malaria: Emerging Technologies to Study Parasite-Host Interactions in the Liver. Front. Cell. Infect. Microbiol. 2021, 10, 871. [Google Scholar] [CrossRef]
- Howes, R.E.; Reiner, R.C.; Battle, K.E.; Longbottom, J.; Mappin, B.; Ordanovich, D.; Tatem, A.J.; Drakeley, C.; Gething, P.W.; Zimmerman, P.A.; et al. Plasmodium vivax Transmission in Africa. PLoS Negl. Trop. Dis. 2015, 9, e0004222. [Google Scholar] [CrossRef]
- Buusman, A.; Andersen, M.; Merrild, C.; Elverdam, B. Factors influencing GPs’ choice between drugs in a therapeutic drug group. A qualitative study. Scand. J. Prim. Health Care 2007, 25, 208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staines, H.M.; Krishna, S. Treatment and Prevention of Malaria: Antimalarial Drug Chemistry, Action and Use; Springer: Basel, Switzerland, 2012; ISBN 9783034604802. [Google Scholar]
- Van Vugt, M.; Brockman, A.; Gemperli, B.; Luxemburger, C.; Gathmann, I.; Royce, C.; Slight, T.; Looareesuwan, S.; White, N.J.; Nosten, F. Randomized comparison of artemether-benflumetol and artesunate—Mefloquine in treatment of multidrug-resistant falciparum malaria. Antimicrob. Agents Chemother. 1998, 42, 135–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbah, M.; Sunday, O.; Mark, O. Commonly Used Antimalarial Drugs in Calabar Metropolis, Nigeria. J. Infect. Dis. Travel Med. 2020, 4, 000138. [Google Scholar] [CrossRef]
- Mbouna, A.D.; Tompkins, A.M.; Lenouo, A.; Asare, E.O.; Yamba, E.I.; Tchawoua, C. Modelled and observed mean and seasonal relationships between climate, population density and malaria indicators in Cameroon. Malar. J. 2019, 18, 359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samdi, L.M.; Ajayi, J.A.; Oguche, S.; Ayanlade, A. Seasonal variation of malaria parasite density in paediatric population of Northeastern Nigeria. Glob. J. Health Sci. 2012, 4, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Asare, E.O.; Amekudzi, L.K. Assessing climate driven malaria variability in Ghana using a regional scale dynamical model. Climate 2017, 5, 20. [Google Scholar] [CrossRef] [Green Version]
- Kublin, J.G.; Cortese, J.F.; Njunju, E.M.; Mukadam, R.A.G.; Wirima, J.J.; Kazembe, P.N.; Djimdé, A.A.; Kouriba, B.; Taylor, T.E.; Plowe, C.V. Reemergence of chloroquine-sensitive Plasmodium falciparum malaria after cessation of chloroquine use in Malawi. J. Infect. Dis. 2003, 187, 1870–1875. [Google Scholar] [CrossRef] [Green Version]
- Laufer, M.K.; Thesing, P.C.; Eddington, N.D.; Masonga, R.; Dzinjalamala, F.K.; Takala, S.L.; Taylor, T.E.; Plowe, C.V. Return of Chloroquine Antimalarial Efficacy in Malawi. N. Engl. J. Med. 2006, 355, 1959–1966. [Google Scholar] [CrossRef]
- Sowunmi, A.; Adewoye, E.O.; Gbotsho, G.O.; Happi, C.T.; Sijuade, A.; Folarin, O.A.; Okuboyejo, T.M.; Michael, O.S. Factors contributing to delay in parasite clearance in uncomplicated falciparum malaria in children. Malar. J. 2010, 9, 53. [Google Scholar] [CrossRef] [Green Version]
- WHO. World Malaria Report 2018. Available online: https://www.mmv.org/sites/default/files/uploads/docs/publications/WorldMalariaReport2018.pdf (accessed on 25 December 2020).
- WHO. Methods for Surveillance of Antimalarial Drug Efficacy. Available online: https://www.who.int/publications/i/item/9789241597531 (accessed on 1 July 2022).
- Watsierah, C.A.; Jura, W.G.Z.O.; Oyugi, H.; Abong’o, B.; Ouma, C. Factors determining anti-malarial drug use in a peri-urban population from malaria holoendemic region of western Kenya. Malar. J. 2010, 9, 295. [Google Scholar] [CrossRef]
- Atemnkeng, M.A.; De Cock, K.; Plaizier-Vercammen, J. Quality control of active ingredients in artemisinin-derivative antimalarials within Kenya and DR Congo. Trop. Med. Int. Health 2007, 12, 68–74. [Google Scholar] [CrossRef]
- Vranić, E. Basic Principles of Drug—Excipients Interactions. Bosn. J. Basic Med. Sci. 2004, 4, 56. [Google Scholar] [CrossRef]
- WHO. Report on Antimalarial Drug Efficacy, Resistance and Response: 10 Years of Surveillance (2010–2019). Available online: https://www.who.int/publications/i/item/9789240012813 (accessed on 27 December 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sentiment Level | Numerical Value | Response | Total |
|---|---|---|---|
| Highly Satisfactory | 5 | 92 | 460 |
| Satisfactory | 4 | 178 | 712 |
| Neutral | 3 | 22 | 66 |
| Unsatisfactory | 2 | 7 | 14 |
| Highly Unsatisfactory | 1 | 1 | 1 |
| Total | 300 | 1253 | |
| Average sentiment level | 4.18 |
| Question | Strongly Agree | Agree | Undecided | Disagree | Strongly Disagree | Average Sentiment |
|---|---|---|---|---|---|---|
| Patients come back earlier than normal to buy antimalarial for treatment again due to failure of treatment? | 15 | 10 | 10 | 11 | 19 | 2.86 |
| Relapse is higher in patients without prescription | 10 | 8 | 22 | 11 | 14 | 2.83 |
| Antimalarial purchase without prescription contributes to treatment failure | 13 | 15 | 17 | 7 | 13 | 3.12 |
| Most patients buy antimalarial without diagnosis | 31 | 19 | 9 | 5 | 1 | 4.14 |
| Diagnosis before treatment can reduce treatment failure | 51 | 7 | 3 | 2 | 2 | 4.58 |
| Patients that have experienced treatment failure stick to the class of drug leading | 2 | 4 | 9 | 18 | 27 | 1.93 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egwu, C.O.; Aloke, C.; Chukwu, J.; Nwankwo, J.C.; Irem, C.; Nwagu, K.E.; Nwite, F.; Agwu, A.O.; Alum, E.; Offor, C.E.; et al. Assessment of the Antimalarial Treatment Failure in Ebonyi State, Southeast Nigeria. J. Xenobiot. 2023, 13, 16-26. https://doi.org/10.3390/jox13010003
Egwu CO, Aloke C, Chukwu J, Nwankwo JC, Irem C, Nwagu KE, Nwite F, Agwu AO, Alum E, Offor CE, et al. Assessment of the Antimalarial Treatment Failure in Ebonyi State, Southeast Nigeria. Journal of Xenobiotics. 2023; 13(1):16-26. https://doi.org/10.3390/jox13010003
Chicago/Turabian StyleEgwu, Chinedu Ogbonnia, Chinyere Aloke, Jennifer Chukwu, Joshua Chidiebere Nwankwo, Chinemerem Irem, Kingsley E. Nwagu, Felix Nwite, Anthony Ogbonnaya Agwu, Esther Alum, Christian E. Offor, and et al. 2023. "Assessment of the Antimalarial Treatment Failure in Ebonyi State, Southeast Nigeria" Journal of Xenobiotics 13, no. 1: 16-26. https://doi.org/10.3390/jox13010003