
An Evaluation of MINDFIT—A Student Therapeutic Running Group as a Multi-Layered Intervention in the United Kingdom

 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. Context
1.2. Physical Activity and Mental Health
1.3. Running, Mood and Anxiety
1.4. Green Exercise
1.5. Parkrun
2. Materials and Methods
2.1. Aim
2.2. Objectives
2.3. Designing the MINDFIT Programme
- Meet and greet;
- Run Leader communicated the plan for the session;
- 5-min warm up walk to the park;
- 5 min dynamic stretching and drills—run by a student sports activator;
- 50 min run/walk;
- 5-min warm down walk;
- 55 min psychoeducation, socialising/drinks and snacks.
2.4. The Therapeutic Approach
2.5. Participants
- Age 18 and over;
- Any gender;
- University registered student or a student on a break in study;
- Have the physical ability to walk and run.
- Unable to provide informed consent;
- Students expressing a risk to life by making suicidal plans, to prevent causing harm through the intervention.
2.6. Recruitment
2.7. Data Collection
3. Results
3.1. Qualitative Findings
3.1.1. Theme 1 Creating a Safe Community
3.1.2. Theme 2 Making Progress
3.1.3. Theme 3 Pathways to Success
3.1.4. Staff Voice
3.1.5. Student Sports Activators
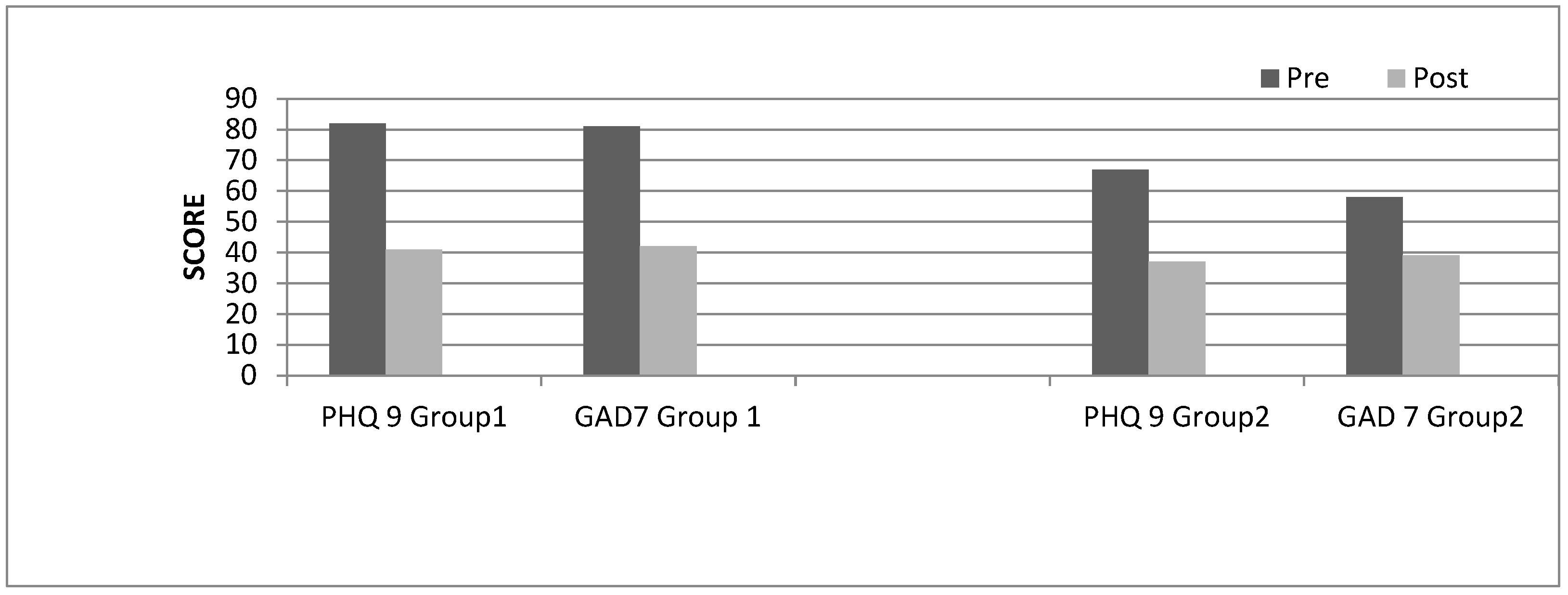
3.2. Quantitative Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NHS Choices. The Couch to 5K Nine-Week Plan. Available online: http://www.nhs.uk/Livewell/c25k/Pages/couch-to-5k-plan.aspx (accessed on 15 November 2022).
- Oswald, F.; Campbell, J.; Williamson, C.; Richards, J.; Kelly, P. A Scoping Review of the Relationship between Running and Mental Health. Int. J. Environ. Res. Public Health 2020, 17, 8059. [Google Scholar] [CrossRef]
- Britten, A. Students still fear disclosing mental health conditions—Ucas-University Business June 2021. Available online: https://www.ucas.com/corporate/news-and-key-documents/news/450-increase-student-mental-health-declarations-over-last-decade-progress-still-needed-address (accessed on 15 November 2022).
- Chen, T.; Lucock, M. The mental health of university students during the COVID-19 pandemic: An online survey in the UK. PLoS ONE 2022, 17, e0262562. [Google Scholar] [CrossRef]
- Wolf, S.; Zeibig, J.; Seiffer, B.; Welkerling, J.; Brokmeier, L.; Atrott, B.; Ehring, T.; Schuch, F.B. Can physical activity protect against depression and anxiety during the COVID-19 pandemic? A rapid systematic review. Sport. Med. 2020, 51, 1771–1783. [Google Scholar] [CrossRef]
- Hubble, S.; Bolton, P. Support for students with mental health issues in higher education in England. UK Parliam. Brief. Paper. 2020. Available online: https://commonslibrary.parliament.uk/research-briefings/cbp-8593/ (accessed on 30 April 2020).
- Office for Students (OfS). Supporting Student Mental Health. Available online: https://www.officeforstudents.org.uk/publications/coronavirus-briefing-note-supporting-student-mental-health/#resources (accessed on 30 April 2020).
- Kwan, M.Y.; Brown, D.; MacKillop, J.; Beaudette, S.; Van Koughnett, S.; Munn, C. Evaluating the impact of Archway: A personalized program for 1st year student success and mental health and wellbeing. BMC Public Health 2020, 21, 59. [Google Scholar] [CrossRef] [PubMed]
- De Girolamo, G.; Dagani, J.; Purcell, R.; Cocchi, A.; McGorry, P.D. Age of onset of mental disorders and use of mental health services: Needs, opportunities and obstacles. Epidemiol. Psychiatr. Sci. 2012, 21, 47–57. [Google Scholar] [CrossRef]
- Mammen, G.; Faulkner, G. Physical activity and the prevention of depression: A systematic review of prospective studies. Am. J. Prev. Med. 2013, 45, 649–657. [Google Scholar] [CrossRef] [PubMed]
- O’Donovan, G.; Blazevich, A.J.; Boreham, C.; Cooper, A.R.; Crank, H.; Ekelund, U.; Fox, K.R.; Gately, P.; Giles-Corti, B.; Gill, J.M.; et al. The ABC of Physical Activity for Health: A consensus statement from the British Association of Sport and Exercise Sciences. J. Sport. Sci. 2010, 28, 573–591. [Google Scholar] [CrossRef]
- National Institute of Health and Social Care. Depression in adults: Treatment and management NICE guideline [NG222] Published: 29 June 2022. Available online: https://www.nice.org.uk/guidance/ng222 (accessed on 30 April 2020).
- National Institute for Health and Care Excellence (Great Britain). Physical Activity: Exercise Referral Schemes. National Institute for Health and Care Excellence (NICE), 2014. Available online: https://www.nice.org.uk/guidance/ph54 (accessed on 30 April 2020).
- Staal, A.; Jespersen, E. The lived experiences of participating in physical activity among young people with mental health problems. A recovery-oriented perspective. Phys. Cult. Sport 2015, 65, 41. [Google Scholar] [CrossRef]
- Van Deurzen, E. Everyday Mysteries: A Handbook of Existential Psychotherapy; Routledge: London, UK, 2009. [Google Scholar]
- Bailey, A.P.; Hetrick, S.E.; Rosenbaum, S.; Purcell, R.; Parker, A.G. Treating depression with physical activity in adolescents and young adults: Asystematic review and meta-analysis of randomised controlled trials. Psychol. Med. 2018, 48, 1068–1083. [Google Scholar] [CrossRef]
- Morres, I.D.; Hatzigeorgiadis, A.; Stathi, A.; Comoutos, N.; Arpin-Cribbie, C.; Krommidas, C.; Theodorakis, Y. Aerobic exercise for adult patients with major depressive disorder in mental health services: A systematic review and meta-analysis. Depress. Anxiety 2019, 36, 39–53. [Google Scholar] [CrossRef] [PubMed]
- Wegner, M.; Amatriain-Fernández, S.; Kaulitzky, A.; Murillo-Rodriguez, E.; Machado, S.; Budde, H. Systematic review of meta-analyses: Exercise effects on depression in children and adolescents. Front. Psychiatry 2020, 11, 81. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.; Bailey, A.P.; Craike, M.; Carter, T.; Patten, R.; Stepto, N.; Parker, A. Physical activity and exercise in youth mental health promotion: A scoping review. BMJ Open Sport Exerc. Med. 2020, 6, e000677. [Google Scholar] [CrossRef]
- Dunn, A.L.; Trivedi, M.H.; Kampert, J.B.; Clark, C.G.; Chambliss, H.O. Exercise treatment for depression: Efficacy and dose response. Am. J. Prev. Med. 2005, 28, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rebar, A.L.; Faulkner, G.; Stanton, R. An exploratory study examining the core affect hypothesis of the anti-depressive and anxiolytic effects of physical activity. Ment. Health Phys. Act. 2015, 9, 55–58. [Google Scholar] [CrossRef]
- Carter, T.; Pascoe, M.; Bastounis, A.; Morres, I.D.; Callaghan, P.; Parker, A.G. The effect of physical activity on anxiety in children and young people: A systematic review and meta-analysis. J. Affect. Disord. 2021, 285, 10–21. [Google Scholar] [CrossRef]
- Miller, A.H.; Raison, C. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef]
- Paolucci, E.M.; Loukov, D.; Bowdish, D.M.; Heisz, J.J. Exercise reduces depression and inflammation but intensity matters. Biol. Psychol. 2018, 133, 79–84. [Google Scholar] [CrossRef]
- Su, C.H.; Chuang, H.C.; Hong, C.J. Physical exercise prevents mice from L-Kynurenine-induced depression-like behavior. Asian J. Psychiatry 2020, 48, 101894. [Google Scholar] [CrossRef] [PubMed]
- Ieraci, A.; Beggiato, S.; Ferraro, L.; Barbieri, S.S.; Popoli, M. Kynurenine pathway is altered in BDNF Val66Met knock-in mice: Effect of physical exercise. Brain Behav. Immun. 2020, 89, 440–450. [Google Scholar] [CrossRef]
- Shipway, R.; Holloway, I. Running free: Embracing a healthy lifestyle through distance running. Perspect. Public Health 2010, 130, 270–276. [Google Scholar] [CrossRef]
- Wiltshire, G.; Stevinson, C. Exploring the role of social capital in community-based physical activity: Qualitative insights from parkrun. Qual. Res. Sport Exerc. Health 2018, 10, 47–62. [Google Scholar] [CrossRef]
- Szabo, A.; Ábrahám, J. The psychological benefits of recreational running: A field study. Psychol. Health Med. 2013, 18, 251–261. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Fetzner, M.G.; DeBoer, L.B.; Powers, M.B.; Otto, M.W.; Smits, J.A. Let’s get physical: A contemporary review of the anxiolytic effects of exercise for anxiety and its disorders. Depress. Anxiety 2013, 30, 362–373. [Google Scholar] [CrossRef]
- Fuss, J.; Steinle, J.; Bindila, L.; Auer, M.K.; Kirchherr, H.; Lutz, B.; Gass, P. A runner’s high depends on cannabinoid receptors in mice. Proc. Natl. Acad. Sci. USA 2015, 112, 3105–3108. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, T. Parkrun: A panacea for health and wellbeing? J. Res. Nurs. 2021, 26, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.; Hine, R.; Wood, C.; Pretty, J. Green Exercise Linking Nature, Health and Well-Being; Routledge: London, UK, 2016. [Google Scholar]
- Rogerson, M.; Gladwell, V.F.; Gallagher, D.J.; Barton, J.L. Influences of green outdoors versus indoors environmental settings on psychological and social outcomes of controlled exercise. Int. J. Environ. Res. Public Health 2016, 13, 363. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed]
- Grunseit, A.; Richards, J.; Merom, D. Running on a high: Parkrun and personal well-being. BMC Public Health 2018, 18, 59. [Google Scholar] [CrossRef]
- Quirk, H.; Haake, S. How can we get more people with long-term health conditions involved in parkrun? A qualitative study evaluating parkrun’s PROVE project. BMC Sport. Sci. Med. Rehabil. 2020, 11, 22. [Google Scholar] [CrossRef]
- Morris, P. Not just a run inthe park: A qualitative exploration of parkrun and mental health. Adv. Ment. Health 2019, 17, 110–123. [Google Scholar] [CrossRef]
- Stevinson, C.; Wiltshire, G.; Hickson, M. Facilitating participation in health-enhancing physical activity: A qualitative study of parkrun. Int. J. Behav. Med. 2015, 22, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Aylett, E.; Small, N.; Bower, P. Exercise in the treatment of clinical anxiety in general practice—A systematic review and meta-analysis. BMC Health Serv. Res. 2018, 18, 559. [Google Scholar] [CrossRef]
- Miller, W.; Rollnick, S. Talking oneself into change: Motivational interviewing, stages of change, and therapeutic process. J. Cogn. Psychother. 2004, 184, 299–308. [Google Scholar] [CrossRef]
- Marshall, C.; Rossman, G.B. Designing Qualitative Research; Sage Publications: London, UK, 2014. [Google Scholar]
- Clarke, C. An introduction to interpretative phenomenological analysis: A useful approach for occupational therapy research. Br. J. Occup. Ther. 2009, 72, 37–39. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Tavakol, M.; Sandars, J. AMEE medical education guide no. 90 part I: Quantitative and qualitative methods in medical education research. Med.Teach. 2014, 36, 838–848. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.L. Commentary—After triangulation, what next? J. Mix. Methods Res. 2019, 13, 6–11. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Alghadir, A.; Manzar, M.D.; Answer, S.; Albougami, A.; Salahuddin, M. Psychometric properties of the generalized anxiety disorder scale among Saudi University male students. Neuropsychiatr. Dis. Treat. 2020, 16, 1427. [Google Scholar] [CrossRef]
- Duff, C. Networks, resources and agencies: On the character and production of enabling. Health Place 2011, 171, 149–156. [Google Scholar] [CrossRef]
- Grant, G.; Machaczek, K.; Pollard, N.; Allmark, P. Walking places. sustainability and health: Findings from a study of a walking for health group. Health Soc. Care Community 2017, 25, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- Doughty, K. Walking together: The embodied and mobile production of a therapeutic landscape. Health Place 2013, 24, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health? A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef]
- Matos Wunderlich, F.I. Walking and rhythmicity: Sensing urban space. J. Urban Des. 2008, 13, 125–139. [Google Scholar] [CrossRef]
- St Quinton, T.; Brunton, J.A. The key psychological beliefs underlying student participation in recreational sport. Recreat. Sport. J. 2020, 44, 38–50. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Macmillan: New York, NY, USA, 1997. [Google Scholar]
- Tramonti, F. Steps to an ecology of psychotherapy: The legacy of Gregory Bateson. Syst. Res. Behav. Sci. 2019, 36, 128–139. [Google Scholar] [CrossRef]
- Putnam, R.D. Bowling Alone: The Collapse and Revival of American Community; Simon and Schuster: New York, NY, USA, 2000. [Google Scholar]
- Grant, F.; Hogg, M.A.; Crano, W.D. Yes, we can: Physical activity and group identification among healthy adults. J. Appl. Soc. Psychol. 2015, 45, 383–390. [Google Scholar] [CrossRef]
- Wunsch, K.; Kasten, N.; Fuchs, R. The effect of physical activity on sleep quality, well-being, and affect in academic stress periods. Nat. Sci. Sleep 2017, 9, 117–126. [Google Scholar] [CrossRef]
- Herbert, C. Enhancing Mental Health, Well-Being and Active Lifestyles of University Students by Means of Physical Activity and Exercise Research Programs. Front. Public Health 2022, 10, 849093. [Google Scholar] [CrossRef] [PubMed]
- Woodfield, R. Undergraduate retention and attainment across the disciplines. High. Educ. Acad. 2014, 27, 1–77. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 1113–1127. [Google Scholar]


{kind=link}
| Week | Content |
|---|---|
| 1 | Meet the group. Reiterate the MINDFIT philosophy. Share what you want to get from MINDFIT. Walking session, give shirts. Create belonging |
| 2 | Meditation and group chat about wellbeing. Feedback on the student experience |
| 3 | Physio input—strength and conditioning and stretching |
| 4 | Meditation and group chat—general about wellbeing and being part of a group creating community/feedback about their experience of the group |
| 5 | Cognitive Behavioural Therapy five system |
| 6 | Meditation group chat/feedback—spontaneous wellbeing topics |
| 7 | Mindfully strong speaker and activities |
| 8 | Hallam Parkrun founder talked about the parkrun philosophy, community and resilience needed when he set it up |
| 9 | Arrangement/preparation for parkrun and dealing with pre-event nerves |
| 10 | Arrangement/preparation for parkrun and dealing with pre-event nerves |
| Group | Referred | Triaged | Started | Completed | Non Completed |
|---|---|---|---|---|---|
| Group 1 | 16 | 9 | 9 | 6 | 3 |
| Group 2 | 25 | 11 | 9 | 9 | 0 |
| Group 3 | 21 | 13 | 10 | 9 | 1 |
| Group 4 | 27 | 17 | 15 | Canc | N/A |
| Totals | 89 | 50 | 43 | 24/28 * | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gurung, J.; Turner, J.; Freeman, E.; Coleman, C.; Iacovou, S.; Hemingway, S. An Evaluation of MINDFIT—A Student Therapeutic Running Group as a Multi-Layered Intervention in the United Kingdom. Nurs. Rep. 2023, 13, 456-469. https://doi.org/10.3390/nursrep13010042
Gurung J, Turner J, Freeman E, Coleman C, Iacovou S, Hemingway S. An Evaluation of MINDFIT—A Student Therapeutic Running Group as a Multi-Layered Intervention in the United Kingdom. Nursing Reports. 2023; 13(1):456-469. https://doi.org/10.3390/nursrep13010042
Chicago/Turabian StyleGurung, Jan, James Turner, Elizabeth Freeman, Charlotte Coleman, Susan Iacovou, and Steve Hemingway. 2023. "An Evaluation of MINDFIT—A Student Therapeutic Running Group as a Multi-Layered Intervention in the United Kingdom" Nursing Reports 13, no. 1: 456-469. https://doi.org/10.3390/nursrep13010042