
The Effect of Antenatal Education on Expectant Fathers’ Attitudes toward Breastfeeding and Attachment to the Fetus


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Study Population
2.3. Measures
- (A)
- The Medical History (general and mental health) and the socio-demographic data of men.
- (B)
- Psychometric Tools
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fahey, J.O.; Shenassa, E. Understanding and meeting the needs of women in the postpartum period: The Perinatal Maternal Health Promotion Model. J. Midwifery Womens Health 2013, 58, 613–621. [Google Scholar] [CrossRef]
- Lowdermilk, D.L.; Perry, S.E.; Cashion, K.; Alden, K.R. Maternity & Women’s Health Care, 12th ed.; Elsevier Mosby Company: Maryland Heights, MI, USA, 2019; ISBN 9780323721530. [Google Scholar]
- Gagnon, A.J.; Sandall, J. Individual or group antenatal education for childbirth or parenthood, or both. Cochrane Database Syst. Rev. 2007, 3, 2. [Google Scholar] [CrossRef]
- Ip, W.Y.; Tang, C.S.K.; Goggins, W.B. An intervention to improve women’s ability to cope with childbirth. J. Clin. Nurs. 2009, 18, 2125–2135. [Google Scholar] [CrossRef]
- Miquelutti, M.A.; Cecatti, J.G.; Makuch, M.Y. Antenatal education and the birthing experience of Brazilian women: A qualitative study. BMC Pregnancy Childbirth 2013, 13, 171. [Google Scholar] [CrossRef] [PubMed]
- Toohill, J.; Fenwick, J.; Gamble, J.; Creedy, D.K.; Buist, A.; Turkstra, E.; Ryding, E.L. A randomized controlled trial of a psycho-education intervention by midwives in reducing childbirth fear in pregnant women. Birth 2014, 41, 384–394. [Google Scholar] [CrossRef]
- Byrne, J.; Hauck, Y.; Fisher, C.; Bayes, S.; Schutze, R. Effectiveness of a mindfulness-based childbirth education pilot study on maternal self-efficacy and fear of childbirth. J. Midwifery Womens Health 2014, 59, 192–197. [Google Scholar] [CrossRef]
- Rosen, I.M.; Krueger, M.V.; Carney, L.M.; Graham, J.A. Prenatal breastfeeding education and breastfeeding outcomes. MCN Am J. Matern. Child Nurs. 2008, 33, 315–319. [Google Scholar] [CrossRef]
- Ahlers-Schmidt, C.R.; Okut, H.; Dowling, J. Impact of Prenatal Education on Breastfeeding Initiation Among Low-Income Women. Am. J. Health Promot. 2020, 34, 919–922. [Google Scholar] [CrossRef]
- Kehinde, J.; O’donnell, C.; Grealish, A. The Effectiveness of Prenatal Breastfeeding Education on Breastfeeding Uptake Postpartum: A Systematic Review. Midwifery 2022, 118, 103579. [Google Scholar] [CrossRef] [PubMed]
- Artieta-Pinedo, I.; Paz-Pascual, C.; Grandes, G.; Bacigalupe, A.; Payo, J.; Montoya, I. Antenatal education and breastfeeding in a cohort of primiparas. J. Adv. Nurs. 2013, 69, 1607–1617. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.K.; Lee, D.T. Factors influencing decision to breastfeed. J. Adv. Nurs. 2004, 46, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Britton, C.; McCormick, R.M.; Renfrew, M.J.; Wade, A.; King, S.E. Support for breastfeeding mothers. Cochrane Database Syst. Rev 2007, 1, 1–23. [Google Scholar] [CrossRef]
- Su, L.L.; Chong, Y.S.; Chan, Y.H.; Chan, Y.S.; Fok, D.; Tun, K.T.; Rauff, M. Antenatal education and postnatal support strategies for improving rates of exclusive breast feeding: Randomised controlled trial. Bmj 2007, 335, 596. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.B.; Kim, K.Y.; Kim, E.S. Changes of Maternal-fetal Attachment and Self Efficacy for Delivery after the Taekyo-perspective Prenatal Class. Korean J. Women Health Nurs. 2001, 7, 7–17. [Google Scholar]
- Nazik, E. Effect of childbirth education classes on prenatal attachment. New Trends Issues Proc. Humanit. Soc. Sci. 2017, 4, 73–79. [Google Scholar] [CrossRef]
- Toosi, M.; Akbarzadeh, M.; Sharif, F.; Zare, N. The reduction of anxiety and improved maternal attachment to fetuses and neonates by relaxation training in primigravida women. Womens Health Bull. 2014, 1, 1–6. [Google Scholar] [CrossRef]
- Robertson, S. Understanding Men and Health: Masculinities, Identity and Wellbeing; Open University Press: Maidenhead, UK, 2007; ISBN 978-0335221561. [Google Scholar]
- Caltabiano, M.; Castiglioni, M. Changing family formation in Nepal: Marriage, cohabitation and first sexual intercourse. Int. Fam. Plan. Perspect. 2008, 34, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Kitzinger, S. Letter from Europe: Should fathers be banned from birth? Birth 2010, 37, 77–78. [Google Scholar] [CrossRef] [PubMed]
- Turan, J.M.; Nalbant, H.; Bulut, A.; Sahip, Y. Including expectant fathers in antenatal education programmes in Istanbul, Turkey. Sex. Reprod. Health Matters 2001, 9, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Davies, J. Why young dads matter … and how to reach them. Pract. Midwife 2011, 14, 22–24. [Google Scholar]
- Plantin, L.; Olykoya, A.; Ny, P. Positive health outcomes of fathers’ involvment in pregnancy and childbirth paternal support: A scope study literature review. Father. A J. Theory Res. Pract. Men Father. 2011, 9, 87–102. [Google Scholar] [CrossRef]
- Bich, T.H.; Cuong, N.M. Changes in knowledge, attitude and involvement of fathers in supporting exclusive breastfeeding: A community-based intervention study in a rural area of Vietnam. Int. J. Public Health 2017, 62, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Susin, L.; Giugliani, E.; Kummer, S.; Maciel, M.; Simon, C.; Silveira, L. Does parental breastfeeding knowledge increase breastfeeding rates? Birth 1999, 26, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Barona-Vilar, C.; Agüir, V.; Ferrero-Gandía, R. A qualitative approach to social support and breast-feeding decisions. Midwifery 2009, 25, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Mitchell-Box, K.M.; Braun, K.L. Impact of Male-Partner-Focused Interventions on Breastfeeding Initiation, Exclusivity, and Continuation. J. Hum. Lact. 2013, 29, 473–479. [Google Scholar] [CrossRef]
- Türkmen, H.; Güler, S. Factors Affecting Intrauterine Paternal-Foetal Attachment and the Responsibility Status of Fathers Concerning Mothers and Babies. J. Reprod. Infant Psychol. 2022, 40, 451–464. [Google Scholar] [CrossRef] [PubMed]
- Great Britain. Department of Health. Maternity Matters: Choice, Access and Continuity of Care in a Safe Service; The Stationery Office: London, UK, 2007; ISBN M0033377NP. [Google Scholar]
- Great Britain. Department for Children, Schools and Families. Support for All: The Families and Relationships Green Paper; The Stationery Office: London, UK, 2010; ISBN 978-0-10-177872-5. [Google Scholar]
- Royal College of Midwives. Reaching out: Involving Fathers in Maternity Care. Available online: https://www.rcm.org.uk/login/?returnurl=%2fmedia%2f2343%2freaching-out-involving-fathers-in-maternity-care.pdf (accessed on 8 August 2022).
- Palioura, Z.; Sarantaki, A.; Antoniou, E.; Iliadou, M.; Dagla, M. Fathers’ Educational Needs Assessment in Relation to Their Participation in Perinatal Care: A Systematic Review. Healthcare 2023, 11, 200. [Google Scholar] [CrossRef] [PubMed]
- de la Mora, A.; Russell, D.W.; Dungy, C.I.; Losch, M.; Dusdieker, L. The Iowa infant feeding attitude scale: Analysis of reliability and validity 1. J. Appl. Soc. Psychol. 1999, 29, 2362–2380. [Google Scholar] [CrossRef]
- Iliadou, M.; Lykeridou, K.; Prezerakos, P.; Tzavara, C.; Tziaferi, S.G. Reliability and validity of the Greek Version of the Iowa Infant Feeding Attitude Scale among pregnant women. Mater. Socio-Med. 2019, 31, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Condon, J.T. The assessment of antenatal emotional attachment: Development of a questionnaire instrument. Br. J. Health Psychol. 1993, 66, 167–183. [Google Scholar] [CrossRef]
- Condon, J.T.; Corkindale, C.J.; Boyce, P. Assessment of postnatal paternal–infant attachment: Development of a questionnaire instrument. J. Reprod. Infant Psychol. 2008, 26, 195–210. [Google Scholar] [CrossRef]
- Habib, C.; Lancaster, S. Changes in identity and paternal-foetal attachment across the first pregnancy. J. Reprod. Infant Psychol. 2010, 28, 128–142. [Google Scholar] [CrossRef]
- Raeisi, K.; Shariat, M.; Nayeri, F.; Raji, F.; Dalili, H. A single center study of the effects of trained fathers’ participation in constant breastfeeding. Acta Med. Iran. 2014, 52, 694–696. [Google Scholar] [PubMed]
- Pollock, C.A.; Bustamante-Forest, R.; Giarratano, G. Men of diverse cultures: Knowledge and attitudes about breastfeeding. J. Obstet. Gynecol. Neonatal Nurs. 2002, 31, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Vaaler, M.L.; Castrucci, B.C.; Parks, S.E.; Clark, J.; Stag, J.; Erickson, T. Men’s attitudes toward breastfeeding: Findings from the 2007 Texas behavioral risk factor surveillance system. Matern. Child Health J. 2011, 15, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Chezem, J.C. Breastfeeding attitudes among couples planning exclusive breastfeeding or mixed feeding. Breastfeed. Med. 2012, 7, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Laanterä, S.; Pölkki, T.; Ekström, A.; Pietilä, A.M. Breastfeeding attitudes of Finnish parents during pregnancy. BMC Pregnancy Childbirth 2010, 10, 79. [Google Scholar] [CrossRef] [PubMed]
- Shaker, I.; Scott, J.A.; Reid, M. Infant feeding attitudes of expectant parents: Breastfeeding and formula feeding. J. Adv. Nurs. 2004, 45, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Freed, G.L.; Fraley, J.K.; Schanler, R.J. Attitudes of expectant fathers regarding breast-feeding. Pediatrics 1992, 90 Pt 1, 224–227. [Google Scholar] [CrossRef] [PubMed]
- Serçekuş, P.; Başkale, H. Effects of antenatal education on fear of childbirth, maternal self-efficacy and parental attachment. Midwifery 2016, 34, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Setodeh, S.; Pourahmad, S.; Akbarzadeh, M. A study of the efficacy of fathers’ attachment training on paternal-fetal attachment and parental anxiety. J. Family Med. Prim. Care 2017, 19, 393–398. [Google Scholar] [CrossRef]
- Sandbrook, S.P.; Adamson-Macedo, E.N. Maternal-fetal attachment: Searching for a new definition. Neuro Endocrinol. Lett. 2004, 25, 169–182. [Google Scholar]
- Bouchard, G. The role of psychosocial variables in prenatal attachment: An examination of moderational effects. J. Reprod. Infant Psychol. 2011, 29, 197–207. [Google Scholar] [CrossRef]
- Luz, R.; George, A.; Vieux, R.; Spitz, E. Antenatal determinants of parental at- tachment and parenting alliance: How do mothers and fathers differ? Infant Ment. Health J 2017, 38, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Condon, J.; Corkindale, C.; Boyce, P.; Gamble, E. A longitudinal study of father-to-infant attachment: Antecedents and correlates. J. Reprod. Infant Psychol. 2013, 31, 15–30. [Google Scholar] [CrossRef]
- Yu, C.Y.; Hung, C.H.; Chan, T.F.; Yeh, C.H.; Lai, C.Y. Prenatal predictors for father-infant attachment after childbirth. J. Clin. Nurs. 2012, 21, 1577–1583. [Google Scholar] [CrossRef]
- Alhusen, J.L. A literature update on maternal-fetal attachment. J. Obstet. Gynecol. Neonatal Nurs. 2008, 37, 315–328. [Google Scholar] [CrossRef]
- DiPietro, J.A. Psychological and psychophysiological considerations regarding the maternal-fetal relationship. Infant Child Dev. 2010, 19, 27–38. [Google Scholar] [CrossRef]
- Tolman, R.M.; Walsh, T.; Bybee, D.; Davis, N.; Reed, L.A.; Safyer, P.; Singh, V. Paternal Response to Ultrasound Predicts Increased Paternal-Fetal Attachment. J. Fam. Issues 2021, 42, 3001–3023. [Google Scholar] [CrossRef]
- Ustunsoz, A.; Guvenc, G.; Akyuz, A.; Oflaz, F. Comparison of maternal-and paternal-fetal attachment in Turkish couples. Midwifery 2010, 26, e1–e9. [Google Scholar] [CrossRef]
- Camarneiro, A.P.F.; De Miranda Justo, J.M.R. Prenatal attachment and 46 sociodemographic and clinical factors in portuguese couples. J. Reprod. Infant Psychol. 2017, 35, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Göbel, A.; Barkmann, C.; Arck, P.; Hecher, K.; Schulte-Markwort, M.; Diemert, A.; Mudra, S. Couples’prenatal bonding to the fetus and the association with one’s own and partner’s emotional well-being and adult romantic attachment style. Midwifery 2019, 79, 102549. [Google Scholar] [CrossRef]
- Vreeswijk, C.M.; Maas, A.J.; Rijk, C.H.; van Bakel, H.J. Fathers’ experiences during pregnancy: Paternal prenatal attachment and representations of the fetus. Psychol Men. Masc. 2014, 15, 129–137. [Google Scholar] [CrossRef]
- Fraser, W.; Maunsell, E.; Hodnett, E.; Moutquin, J.M. Randomized controlled trial of a prenatal vaginal birth after cesarean section education and support program. Childbirth Alternatives Post-Cesarean Study Group. Am. J. Obstet. Gynecol. 1997, 176, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Mehdizadeh, A.; Roosta, F.; Chaichian, S.; Alaghehbandan, R. Evaluation of the impact of birth preparation courses on the health of the mother and the newborn. Am. J. Perinatol. 2005, 22, 7–9. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Demographic Characteristics | N M | % SD |
|---|---|---|
| Age | 36.93 | 4.17 |
| Education | ||
| High school | 51 | 23.6 |
| Bachelor’s degree | 81 | 37.5 |
| Postgraduate studies | 84 | 38.9 |
| Total | 216 | 100.0 |
| Occupation | ||
| Private-sector employee | 121 | 56.0 |
| Public-sector employee | 23 | 10.6 |
| Freelancer | 68 | 31.5 |
| Total/Missing | 212/4 | 98.1/1.9 |
| Family financial managing | ||
| Sometimes difficult | 44 | 20.4 |
| Not that well | 50 | 23.1 |
| Easy | 121 | 56.0 |
| Total/Missing | 215/1 | 99.5/.5 |
| Marital status | ||
| Married | 161 | 74.5 |
| Cohabitation agreement | 32 | 14.8 |
| Living with partner | 18 | 8.3 |
| Total/Missing | 211/5 | 97.7/2.3 |
| Perinatal Characteristics | ||
| Antenatal education | ||
| No | 31 | 14.29 |
| Yes | 185 | 85.71 |
| Total | 216 | 100.0 |
| IIFAS score at the beginning of the program | 63.98 | 7.86 |
| IIFAS score at the end of the program | 65.48 | 8.55 |
| PAAS score at the beginning of the program | 61.46 | 6.57 |
| PAAS score at the end of the program | 64.99 | 7.16 |
| Psycho-emotional Characteristics | ||
| Partner’s emotional support | ||
| Not at all to Moderate | 41 | 19.0 |
| Quite a lot | 62 | 28.7 |
| Very much | 113 | 52.3 |
| Total | 216 | 100.0 |
| Relationship difficulties | ||
| No difficulties | 124 | 57.4 |
| Relative difficulties | 72 | 33.3 |
| Moderate difficulties | 20 | 9.3 |
| Total | 216 | 100.0 |
| Prevalent emotions during pregnancy | ||
| Happy | 25 | 11.69 |
| Very happy | 191 | 88.31 |
| Total | 216 | 100 |
| Sadness during pregnancy | ||
| Not at all | 163 | 75.32 |
| A bit to Moderate | 53 | 24.68 |
| Total | 216 | 100 |
| Anxiety during pregnancy | ||
| Moderate | 34 | 15.58 |
| Quite a lot | 80 | 37.16 |
| Very much | 102 | 47.26 |
| Total | 216 | 100 |
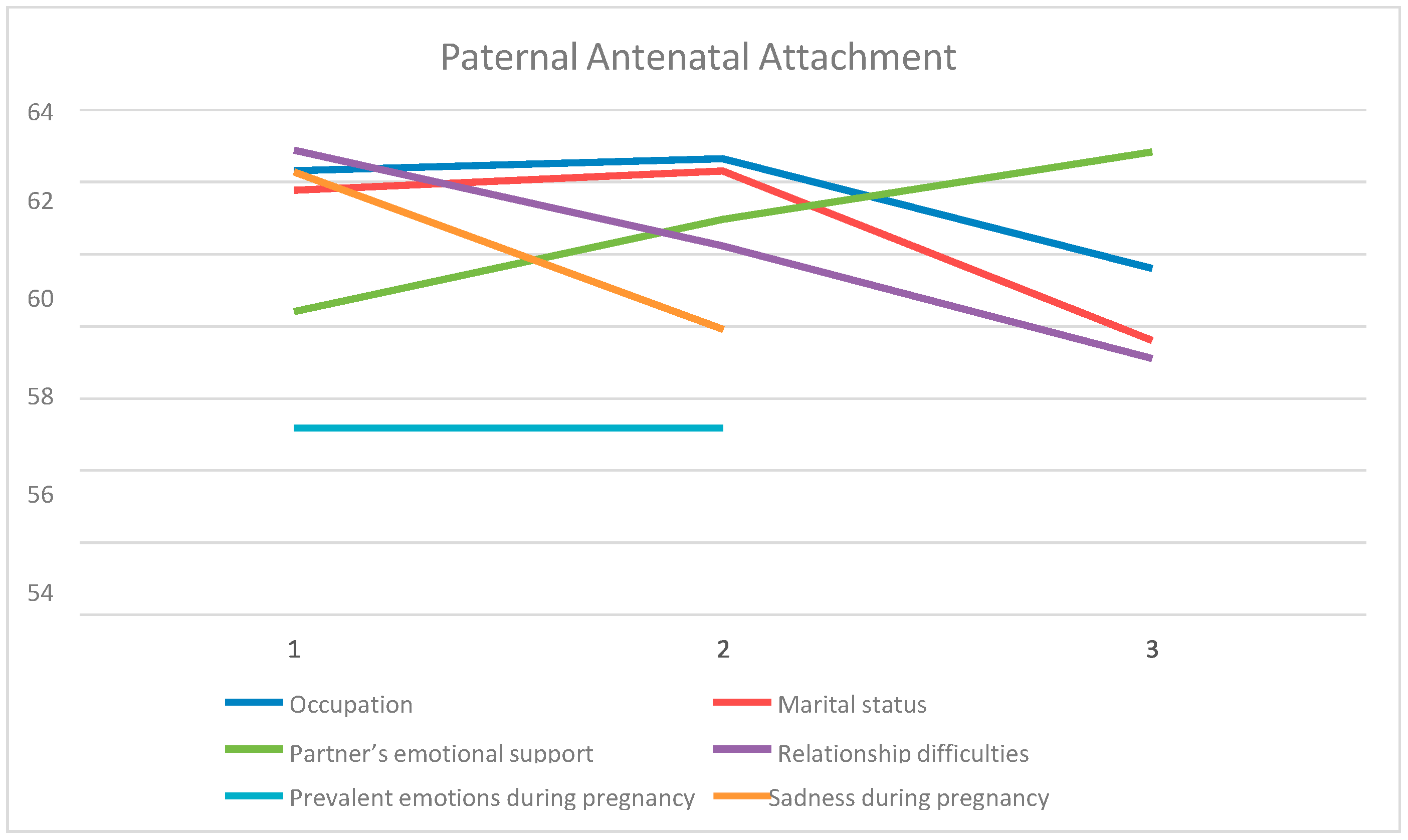
| Paternal Antenatal Attachment | ||||||
|---|---|---|---|---|---|---|
| M | SD | F | df | p | η2 | |
| Occupation | ||||||
| Private-sector employee | 62.32 a | 5.95 | ||||
| Public-sector employee | 62.65 ab | 4.90 | 4.189 | 2 | 0.016 | 0.039 |
| Freelancer | 59.60 b | 7.85 | ||||
| Marital status | ||||||
| Married | 61.78 a | 6.56 | ||||
| Cohabitation agreement | 62.31 b | 6.17 | 3.699 | 2 | 0.026 | 0.034 |
| Living with partner | 57.61 c | 5.65 | ||||
| Partner’s emotional support | ||||||
| Not at all to Moderate | 58.41 a | 9.69 | ||||
| Quite much | 60.97 ab | 5.01 | 7.494 | 2 | 0.001 | 0.066 |
| Very much | 62.84 b | 5.50 | ||||
| Relationship difficulties | ||||||
| No difficulties | 62.89 a | 5.479 | 9.259 | 2 | p < 0.001 | 0.080 |
| Relative difficulties | 60.229 b | 7.09 | ||||
| Moderate difficulties | 57.109 c | 8.279 | ||||
| Prevalent emotions during pregnancy | ||||||
| Happy | 55.18 | 8.21 | 56.523 | 1 | p < 0.001 | 0.209 |
| Very happy | 62.89 | 5.19 | ||||
| Sadness during pregnancy | ||||||
| Not at all | 62.28 | 6.53 | 4.789 | 1 | 0.009 | 0.043 |
| A bit to Moderate | 57.92 | 6.39 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dagla, C.; Antoniou, E.; Sarantaki, A.; Iliadou, M.; Mrvoljak-Theodoropoulou, I.; Andersson, E.; Dagla, M. The Effect of Antenatal Education on Expectant Fathers’ Attitudes toward Breastfeeding and Attachment to the Fetus. Nurs. Rep. 2023, 13, 243-254. https://doi.org/10.3390/nursrep13010023
Dagla C, Antoniou E, Sarantaki A, Iliadou M, Mrvoljak-Theodoropoulou I, Andersson E, Dagla M. The Effect of Antenatal Education on Expectant Fathers’ Attitudes toward Breastfeeding and Attachment to the Fetus. Nursing Reports. 2023; 13(1):243-254. https://doi.org/10.3390/nursrep13010023
Chicago/Turabian StyleDagla, Calliope, Evangelia Antoniou, Antigoni Sarantaki, Maria Iliadou, Irina Mrvoljak-Theodoropoulou, Ewa Andersson, and Maria Dagla. 2023. "The Effect of Antenatal Education on Expectant Fathers’ Attitudes toward Breastfeeding and Attachment to the Fetus" Nursing Reports 13, no. 1: 243-254. https://doi.org/10.3390/nursrep13010023