
Hearing Health Awareness and the Need for Educational Outreach Amongst Teachers in Malawi
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
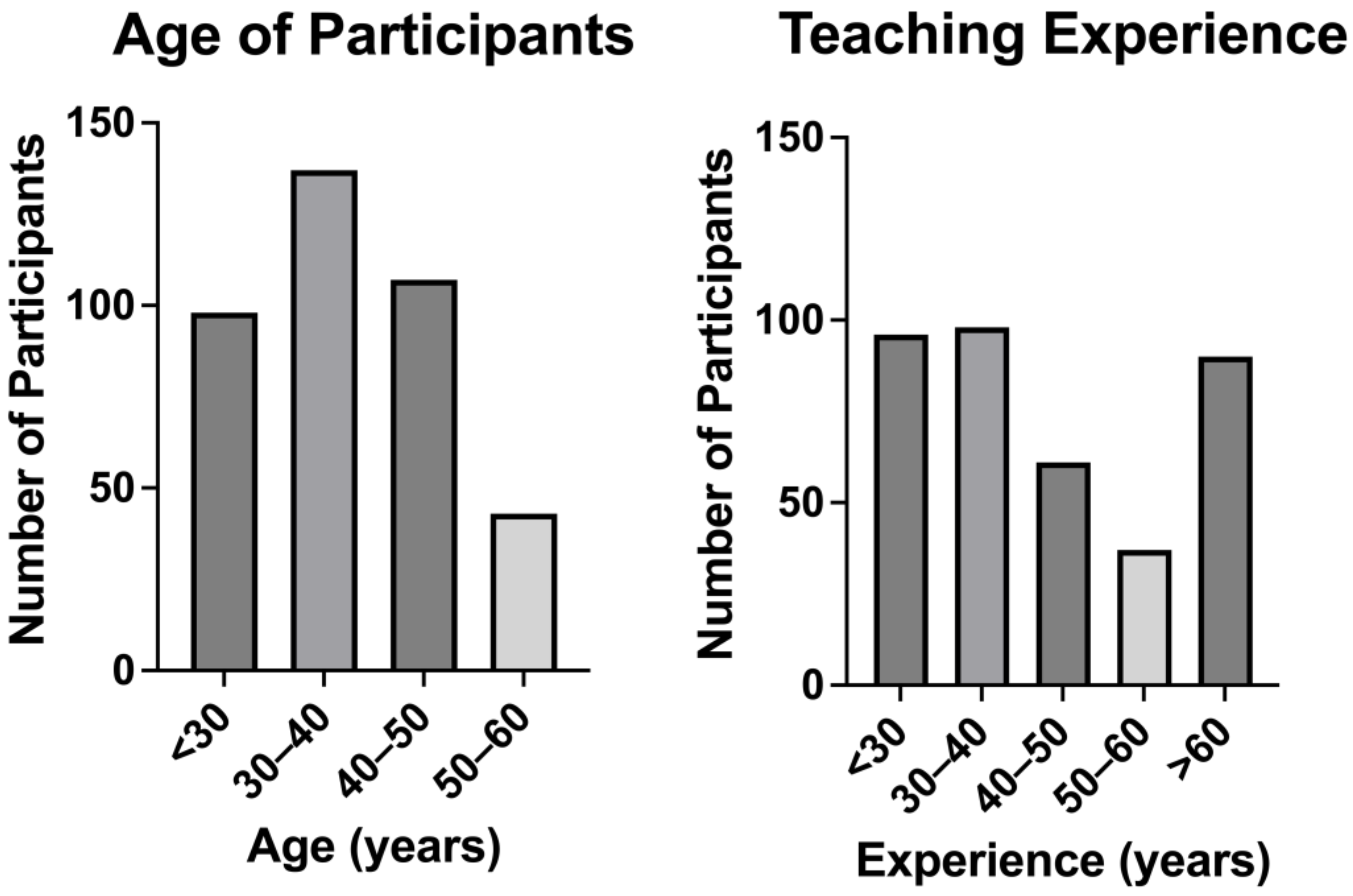
2.1. Overview
2.2. The Pre-Survey
2.3. Educational Intervention
2.4. The Post-Survey
2.5. Data Analysis
3. Results
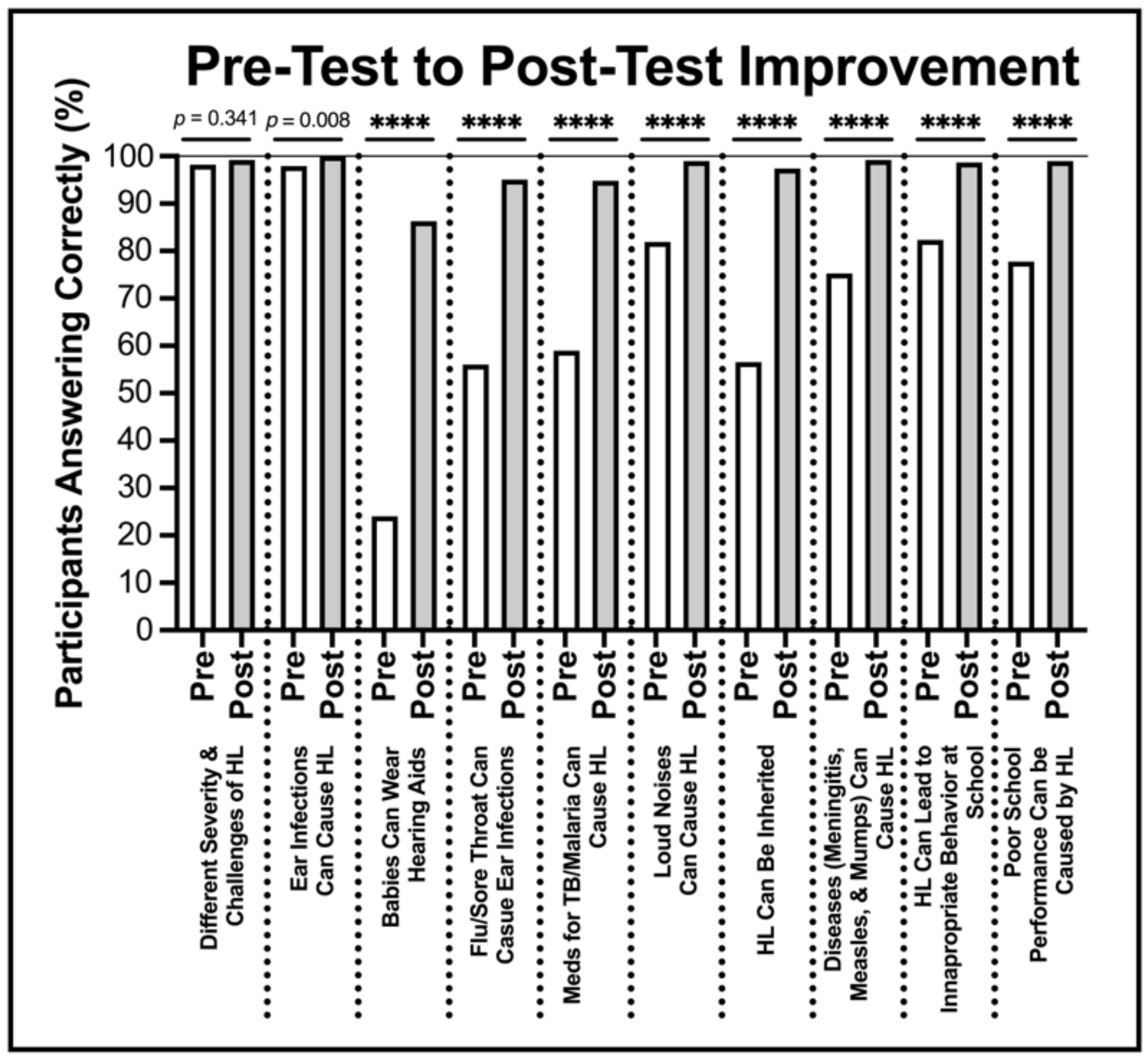
3.1. Pre- and Post-Survey Comparison
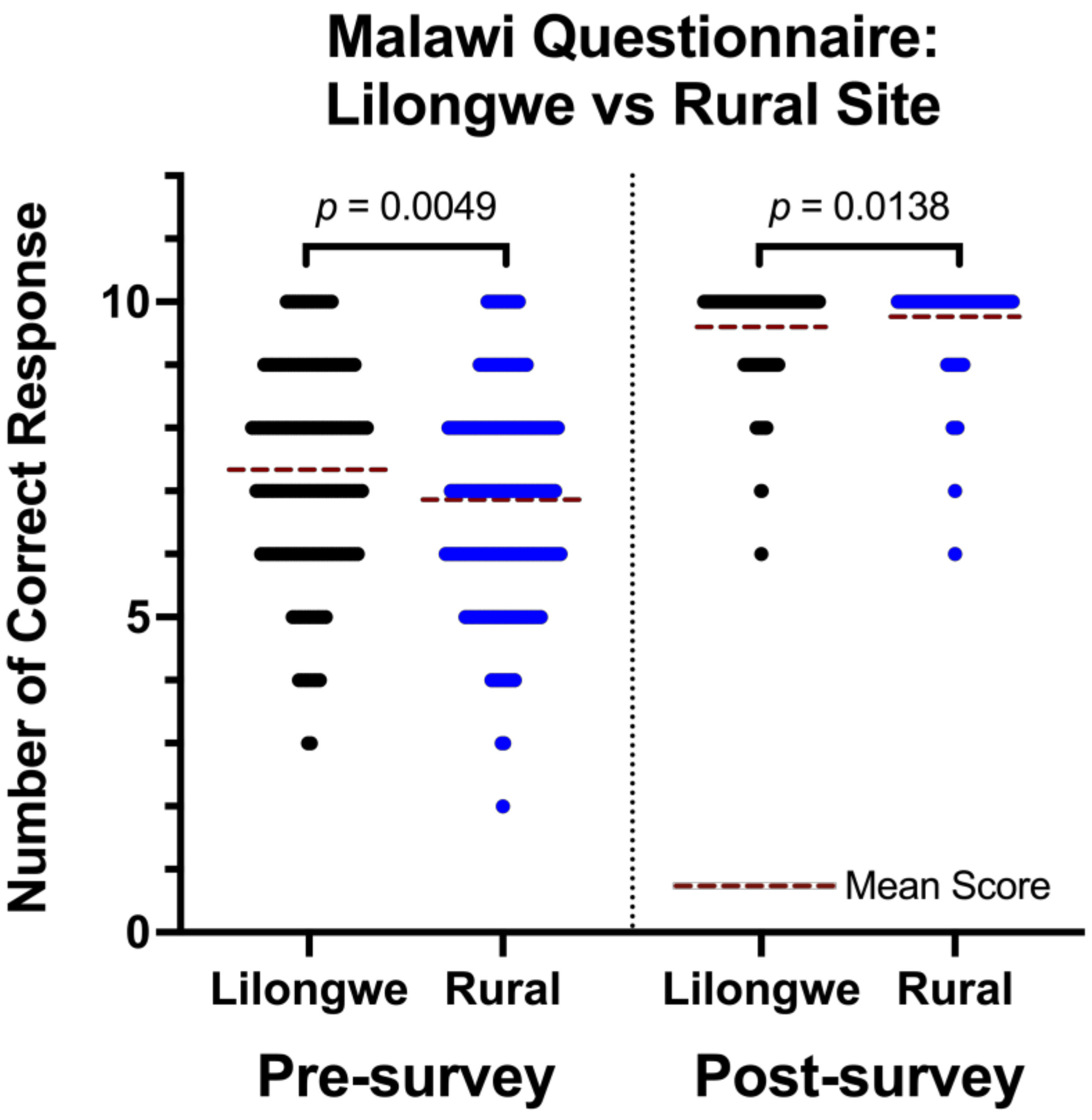
3.2. Lilongwe vs. Rural Sites
3.3. Opinion Surveys
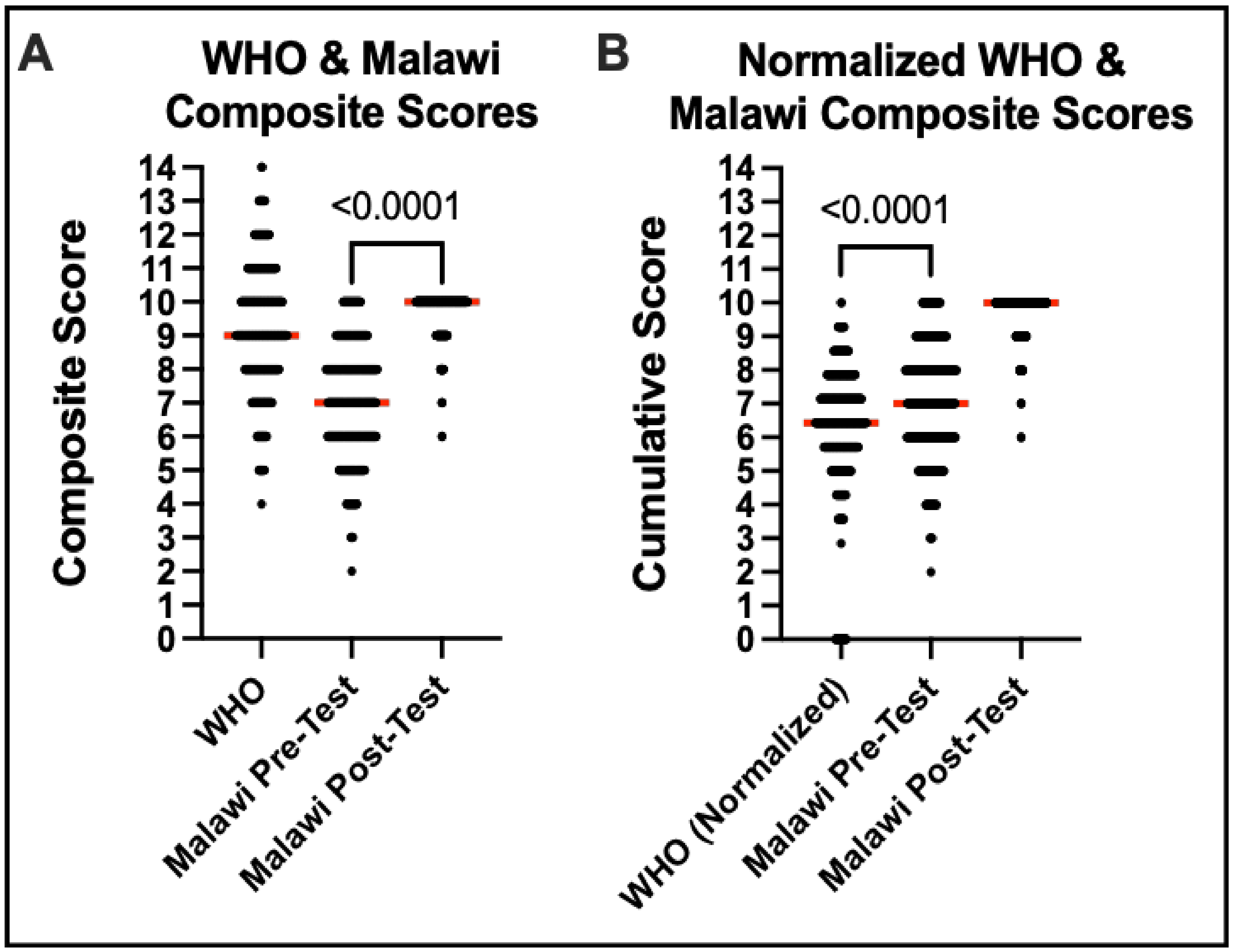
3.4. WHO vs. Malawian Self-Made Survey Scores
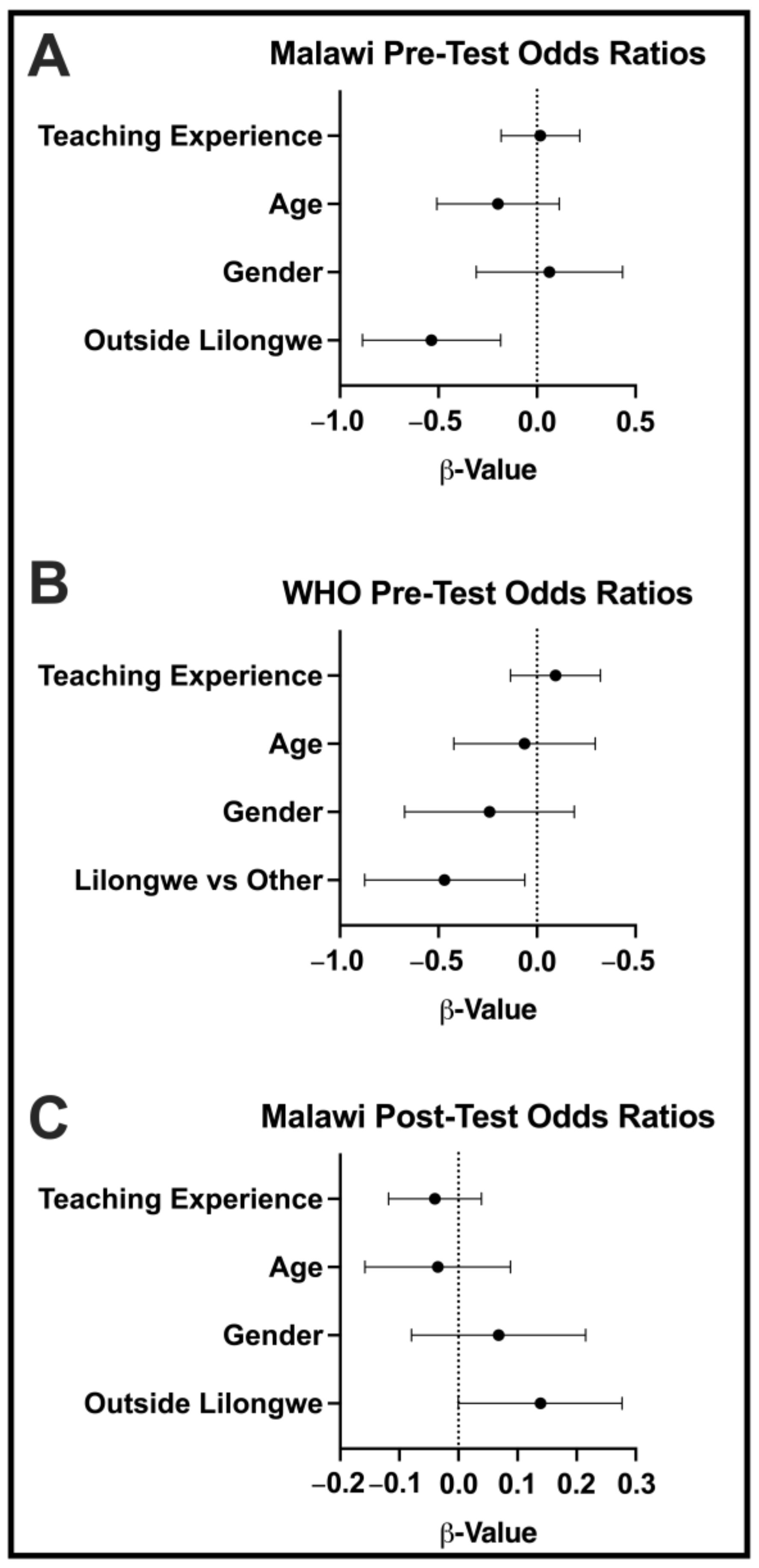
3.5. Multivariate Analysis
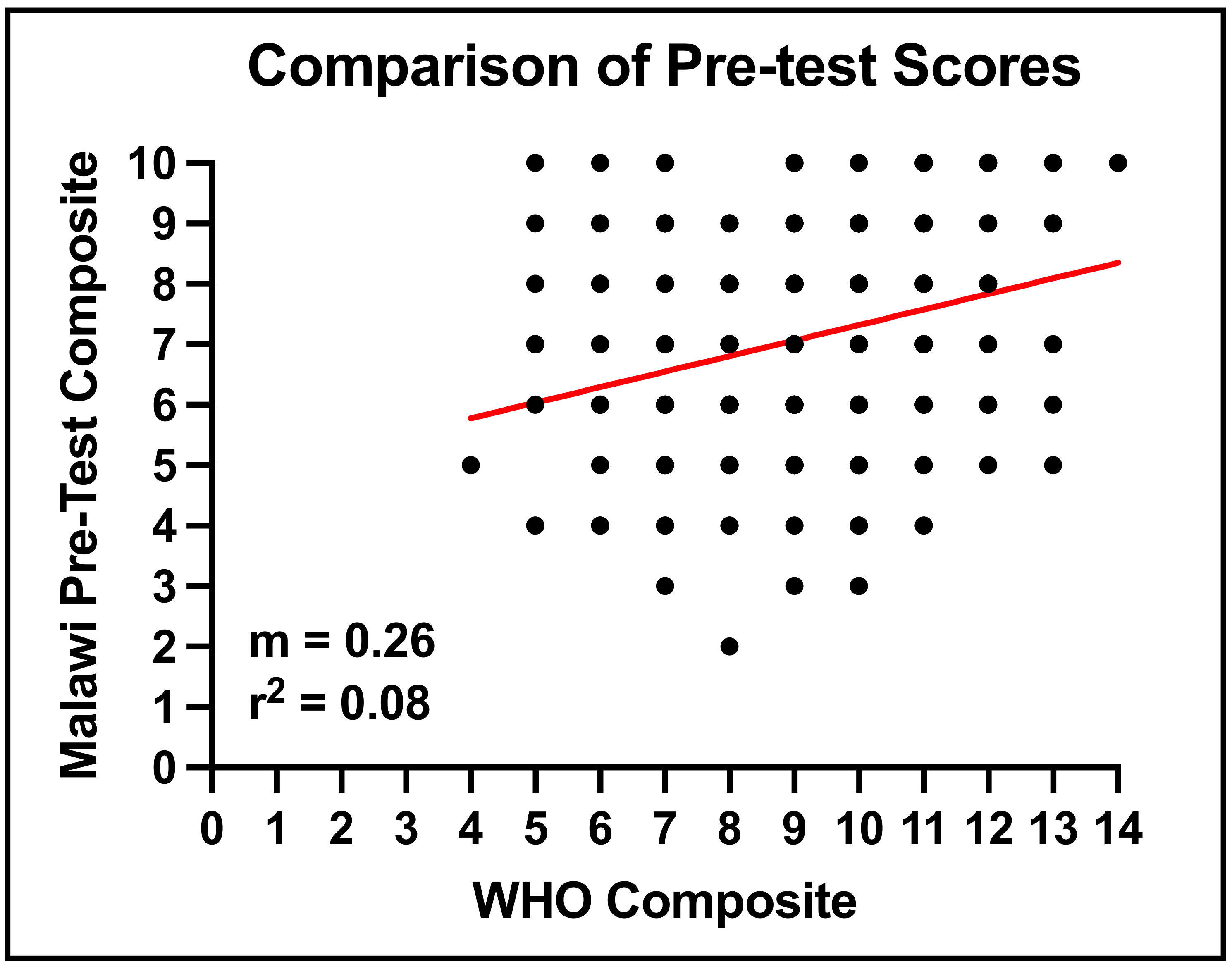
3.6. Cross-Comparison of WHO Survey Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| True or False Questions: Tick Any | True | False |
|---|---|---|
| It is possible to diagnose deafness in infants shortly after birth | ||
| A deaf-mute cannot speak because of defects in the vocal tract | ||
| Hearing loss may cause attention deficits thus reducing school performance | ||
| Cotton buds are necessary for ear cleaning and are the safest means | ||
| Ear drops are sufficient to treat earache | ||
| Otomicosis (itchy ears) can be contracted at the swimming pool | ||
| Drug abuse does not provoke auditory hallucinations or modifications of hearing quality | ||
| Hearing aids need to fit accurately to provide maximum benefit | ||
| Kisses or slaps on the ears do not cause hearing problems | ||
| Listening to music for more than 3 h a day using earphones may cause permanent hearing loss | ||
| There are no tables recommending a reduction in the duration of exposure to high intensity noises | ||
| Irritating perception of sound (e.g., hearing metallic voices) and/or a reduction in hearing clarity (such as a sensation of having cotton wool in the ears) require medical advice | ||
| Sudden hearing loss is an emergency and requires an immediate audiological assessment | ||
| Age-related hearing loss may affect behavior |
References
- World Health Organization (WHO). (n.d.). Deafness and Hearing Loss, Prevalence. Available online: https://www.who.int/health-topics/hearing-loss#tab=tab_2 (accessed on 6 March 2021).
- World Bank Group. Rural Population (% of Total Population)—Malawi. 2021. Available online: https://data.worldbank.org/indi-cator/SP.RUR.TOTL.ZS?locations=MW (accessed on 6 March 2021).
- Worldometer.Info. (n.d.). Malawi Demographics. Available online: https://www.worldometers.info/demographics/malawi-de-mographics/ (accessed on 6 March 2021).
- World Bank. Malawi Overview. 2020. Available online: https://www.worldbank.org/en/country/malawi/overview (accessed on 6 March 2021).
- Global Burden of Diseases. Malawi: What Causes the Most Deaths? 2019. Available online: www.healthdata.org/malawi (accessed on 6 March 2021).
- Jiskoot, P. On-the-job training of clinical officers in Malawi. Malawi Med. J. 2008, 20, 74–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Health Statistics. Health, United States. 2019. Available online: https://www.cdc.gov/nchs/hus/con-tents2019.htm (accessed on 6 March 2021).
- Gordie, K.; Davis, N.; Lister, J.J.; Bartlett, P.; Vallario, J.; Khomera, M.; Kapalamula, G.; Toman, J. Audiology in Malawi. 2021. Available online: https://globalaudiology.org/index.php/audiology-in-malawi/ (accessed on 24 February 2022).
- Mulwafu, W.; Tataryn, M.; Polack, S.; Viste, A.; Goplen, F.K.; Kuper, H. Children with hearing impairment in Malawi, a cohort study. Bull. World Health Organ 2019, 97, 654. [Google Scholar] [CrossRef] [PubMed]
- Hunt, L.; Mulwafu, W.; Knott, V.; Ndamala, C.B.; Naunje, A.W.; Dewhurst, S.; Hall, A.; Mortimer, K. Prevalence of paediatric chronic suppurative otitis media and hearing impairment in rural Malawi: A cross-sectional survey. PLoS ONE 2017, 12, e0188950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swanepoel, D.; Clark, J.L. Hearing healthcare in remote or resource-constrained environments. J. Laryngol. Otol 2019, 133, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olusanya, B.O.; Neumann, K.J.; Saunders, J.E. The global burden of disabling hearing impairment: A call to action. Bull. World Health Organ. 2014, 92, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Di Berardino, F.; Forti, S.; Iacona, E.; Orlandi, G.P.; Ambrosetti, U.; Cesarani, A. Public awareness of ear and hearing management as measured using a specific questionnaire. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 449–453. [Google Scholar] [CrossRef]
- Alshehri, K.A.; Alqulayti, W.M.; Yaghmoor, B.E.; Alem, H. Public awareness of ear health and hearing loss in Jeddah, Saudi Arabia. S. Afr. J. Commun. Disord. 2019, 66, a633. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.M.; Bielko, S.L.; Barnes, P.A.; Evans, S.S.; Main, A.L. Feasibility of a low-cost hearing screening in rural Indiana. BMC Public Health 2017, 17, 715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, A.; Pakulski, L.; Price, J.; Kleinfelder, J. Health teachers’ perceptions and teaching practices regarding hearing loss conservation. Am. J. Health Educ. 2013, 44, 335–342. [Google Scholar] [CrossRef]
- Chataika, L.E.M.; Kamchedzera, E.T.; Semphere, N.K. An Exploration of the Challenges Faced by Regular Primary School Teachers in Planning Instructional Strategies for Inclusive Classrooms. Afr. J. Spec. Incl. Educ. 2017, 2, 12–21. [Google Scholar]
- Mulwafu, W.; Kuper, H.; Viste, A.; Goplen, F.K. Feasibility and acceptability of training community health workers in ear and hearing care in Malawi: A cluster randomised controlled trial. BMJ Open 2017, 7, e016457. [Google Scholar] [CrossRef] [PubMed] [Green Version]






| Question | Pre-Survey Percent Correct | Post-Survey Percent Correct | Percent Increase |
|---|---|---|---|
| 98% | 99% | 1% |
| 98% | 100% | 2% |
| 24% | 86% | 259% |
| 56% | 95% | 70% |
| 59% | 95% | 62% |
| 82% | 99% | 21% |
| 57% | 97% | 72% |
| 75% | 99% | 33% |
| 82% | 99% | 21% |
| 78% | 99% | 27% |
| Total average | 71% * | 97% * | 37% * |
| District (n) | Pre-Avg Score | Post-Avg Score | Percent Increase | School (n) | Pre-Avg Score | Post-Avg Score | Percent Increase |
|---|---|---|---|---|---|---|---|
| Lilongwe Urban (102) | 76% | 96% | 27% | Mvama (25) | 78% | 98% | 26% |
| Msambeta (16) | 75% | 99% | 32% | ||||
| Kabwabwa (21) | 70% | 97% | 37% | ||||
| Lilongwe Demonstration (20) | 77% | 95% | 23% | ||||
| Kalambo (20) | 78% | 93% | 20% | ||||
| Lilongwe Rural (82) | 71% | 96% | 36% | Lilongwe Air Base (10) | 73% | 97% | 33% |
| Njewa Primary (15) | 75% | 94% | 26% | ||||
| Likuni Girls Primary (18) | 73% | 98% | 35% | ||||
| Chitedze (20) | 67% | 93% | 40% | ||||
| Malingunde (19) | 65% | 96% | 47% | ||||
| Ntchisi (61) | 69% | 97% | 40% | Phangwa (13) | 66% | 96% | 45% |
| Kalema (15) | 76% | 98% | 29% | ||||
| Buzi (10) | 68% | 97% | 43% | ||||
| Mpalo (15) | 68% | 94% | 38% | ||||
| Madanjala (8) | 66% | 98% | 47% | ||||
| Salima (76) | 68% | 98% | 45% | Mgoza (7) | 69% | 100% | 46% |
| Salima LEA (17) | 69% | 98% | 42% | ||||
| MAFCO Primary (12) | 69% | 97% | 40% | ||||
| Msalura Primary (25) | 69% | 98% | 43% | ||||
| Kambwiri (15) | 64% | 99% | 55% | ||||
| Dedza (66) | 68% | 98% | 44% | Kapesi (15) | 71% | 95% | 34% |
| Mwenji (12) | 70% | 98% | 39% | ||||
| Kanama Primary (14) | 68% | 99% | 46% | ||||
| Kabango (10) | 59% | 100% | 69% | ||||
| Magaleta (16) | 73% | 99% | 35% |
| Question | Agreement (%) | Disagreement (%) | Undecided (%) |
|---|---|---|---|
| Further hearing care training is necessary. | 97% | 3% | 1% |
| My teacher training program prepared me for teaching a child with hearing loss. | 59% | 37% | 2% |
| The school can adequately help students with hearing difficulties. | 48% | 47% | 5% |
| We have access to enough support for hearing issues at the nearby hospital. | 29% | 59% | 12% |
| Question | Agreement (%) | Disagreement (%) | Undecided (%) |
|---|---|---|---|
| This hearing training has been helpful. | 99% | 1% | 1% |
| We need more hearing training. | 99% | 1% | 2% |
| I know what audiologists do. | 95% | 5% | 0% |
| We can easily access services at ABC HCTC. | 88% | 7.5% | 4.5% |
| Question | Pre- Agreement (%) | Post- Agreement (%) | Percent Increase |
|---|---|---|---|
| I can identify a student with hearing difficulties. | 88% | 97% | 10% |
| I understand the impact of hearing loss on a child’s education and development. | 87% | 97% | 12% |
| I know how to manage a student with hearing difficulties. | 53% | 88% | 65% |
| I know how to prevent hearing loss. | 44% | 97% | 121% |
| Country | Malawi Teachers (%) | Saudi Arabia [14] (%) | Rural Indiana, USA [15] (%) |
|---|---|---|---|
| Overall score | 61% | 76% | 67% |
| Infant hearing loss | 67% | 68% | DNA * |
| Cleaning and treatment | 58% | 80% | DNA * |
| Physical agents and over exposure | 55% | 68% | DNA * |
| Diagnostic delay | 86% | 86% | DNA * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapalamula, G.; Gordie, K.; Khomera, M.; Porterfield, J.Z.; Toman, J.; Vallario, J. Hearing Health Awareness and the Need for Educational Outreach Amongst Teachers in Malawi. Audiol. Res. 2023, 13, 271-284. https://doi.org/10.3390/audiolres13020024
Kapalamula G, Gordie K, Khomera M, Porterfield JZ, Toman J, Vallario J. Hearing Health Awareness and the Need for Educational Outreach Amongst Teachers in Malawi. Audiology Research. 2023; 13(2):271-284. https://doi.org/10.3390/audiolres13020024
Chicago/Turabian StyleKapalamula, Grant, Kelly Gordie, Memory Khomera, J. Zachary Porterfield, Julia Toman, and Jenna Vallario. 2023. "Hearing Health Awareness and the Need for Educational Outreach Amongst Teachers in Malawi" Audiology Research 13, no. 2: 271-284. https://doi.org/10.3390/audiolres13020024