
Self-Reported Hearing-Aid Use Patterns in an Adult Danish Population
 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Grouping of the “Other” Situations
2.2. Sample
2.3. Statistical Analysis
3. Results
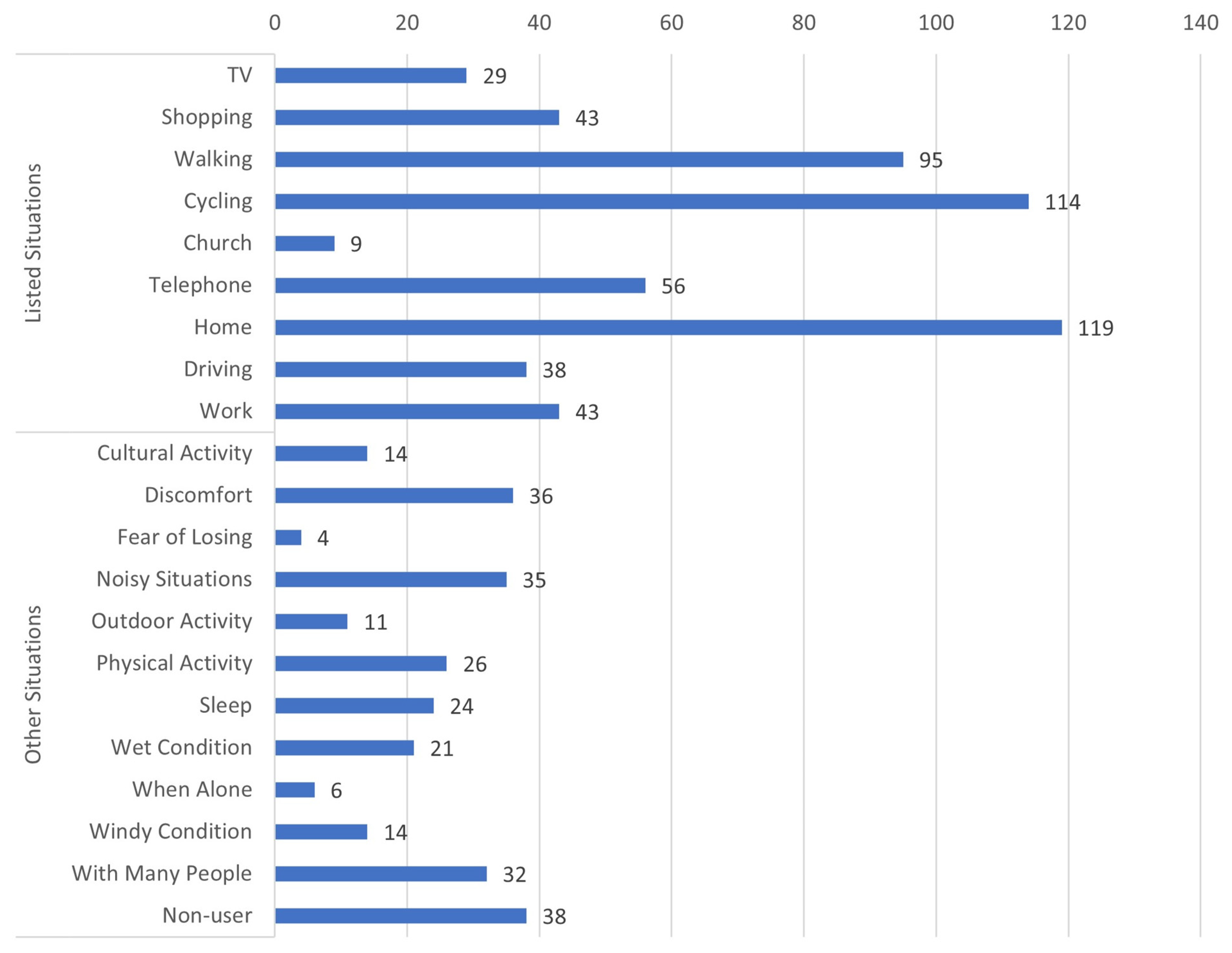
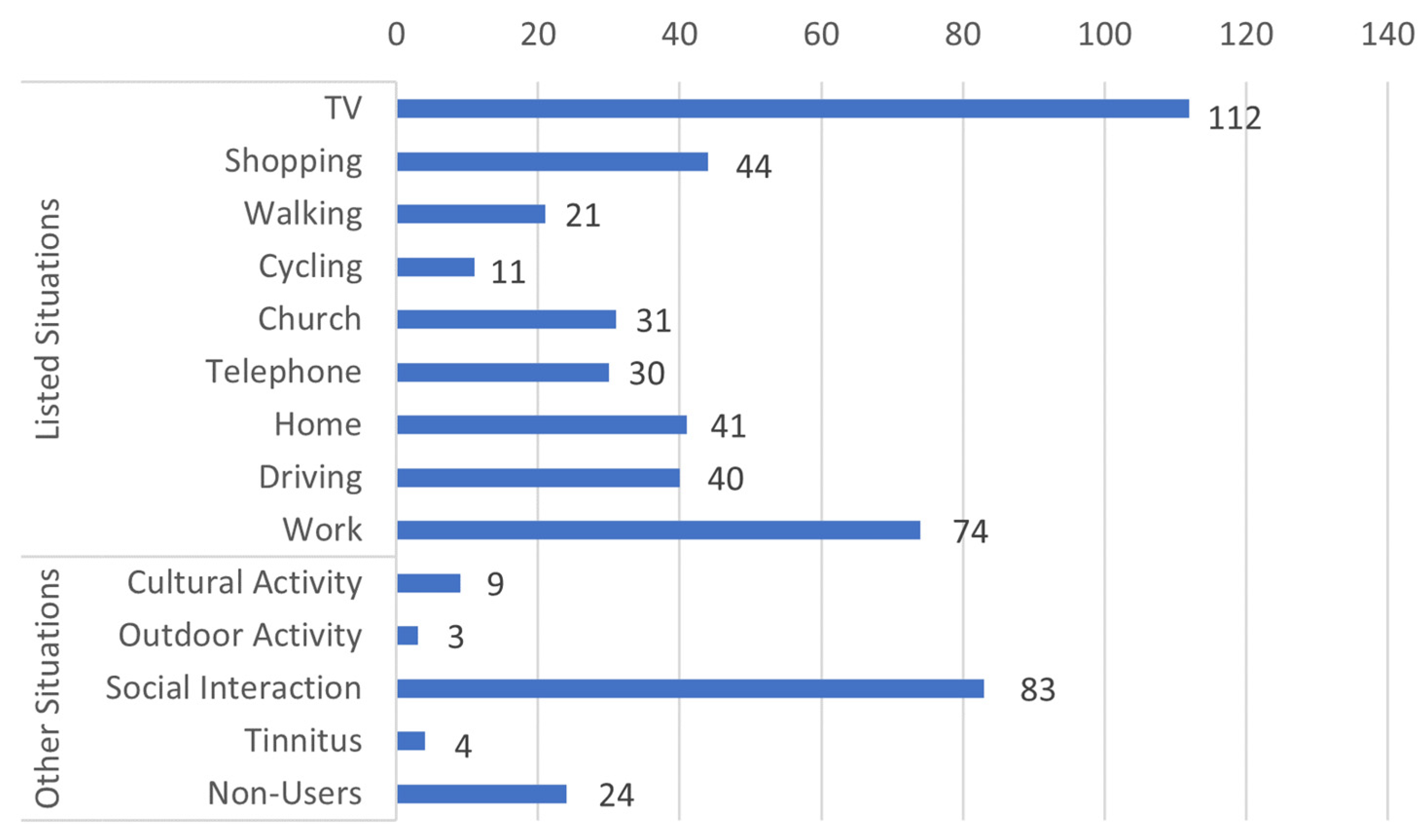
3.1. Situational Non-Use and Situational Use of HAs
3.2. Fitting the Latent Class Models
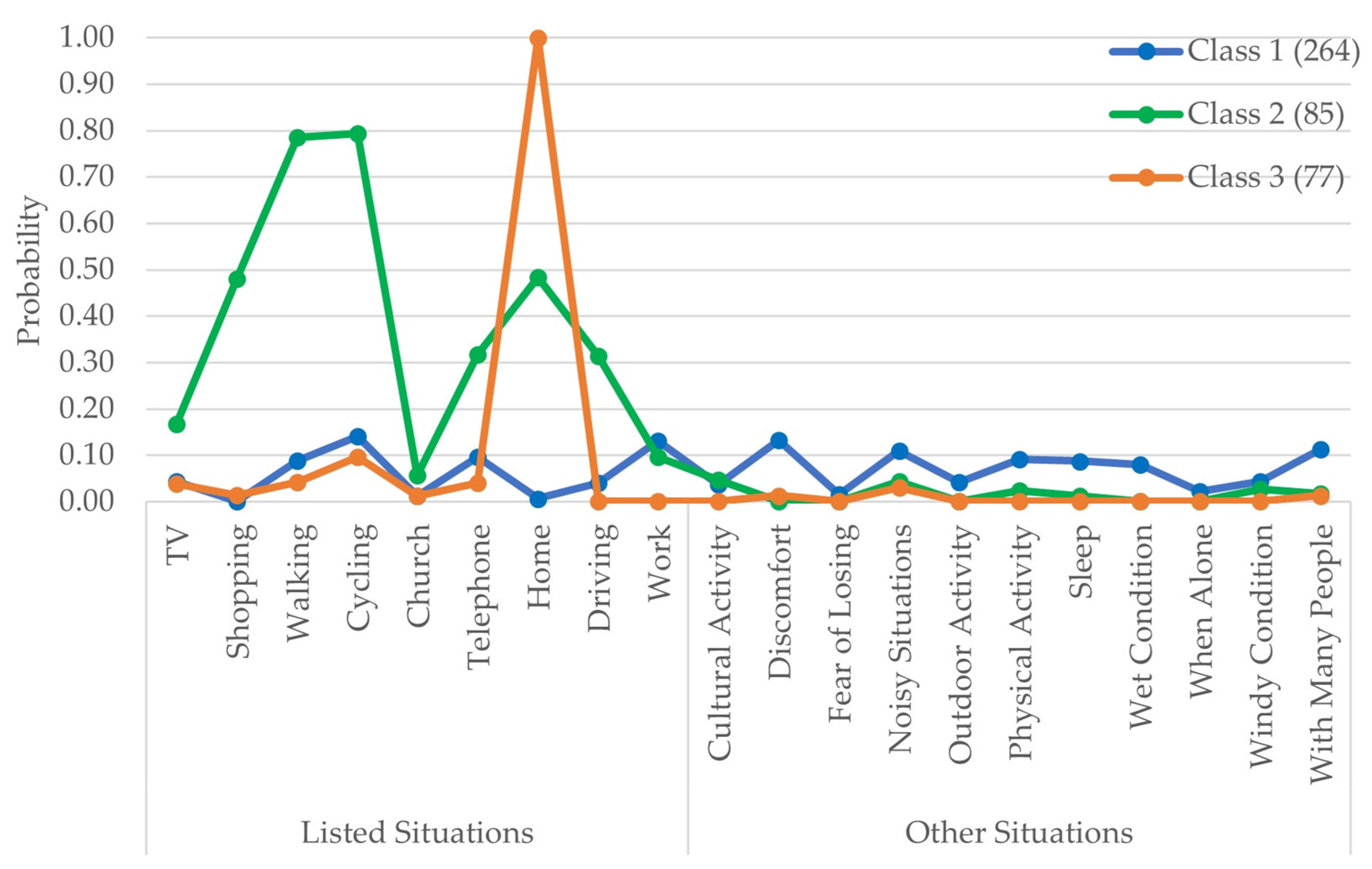
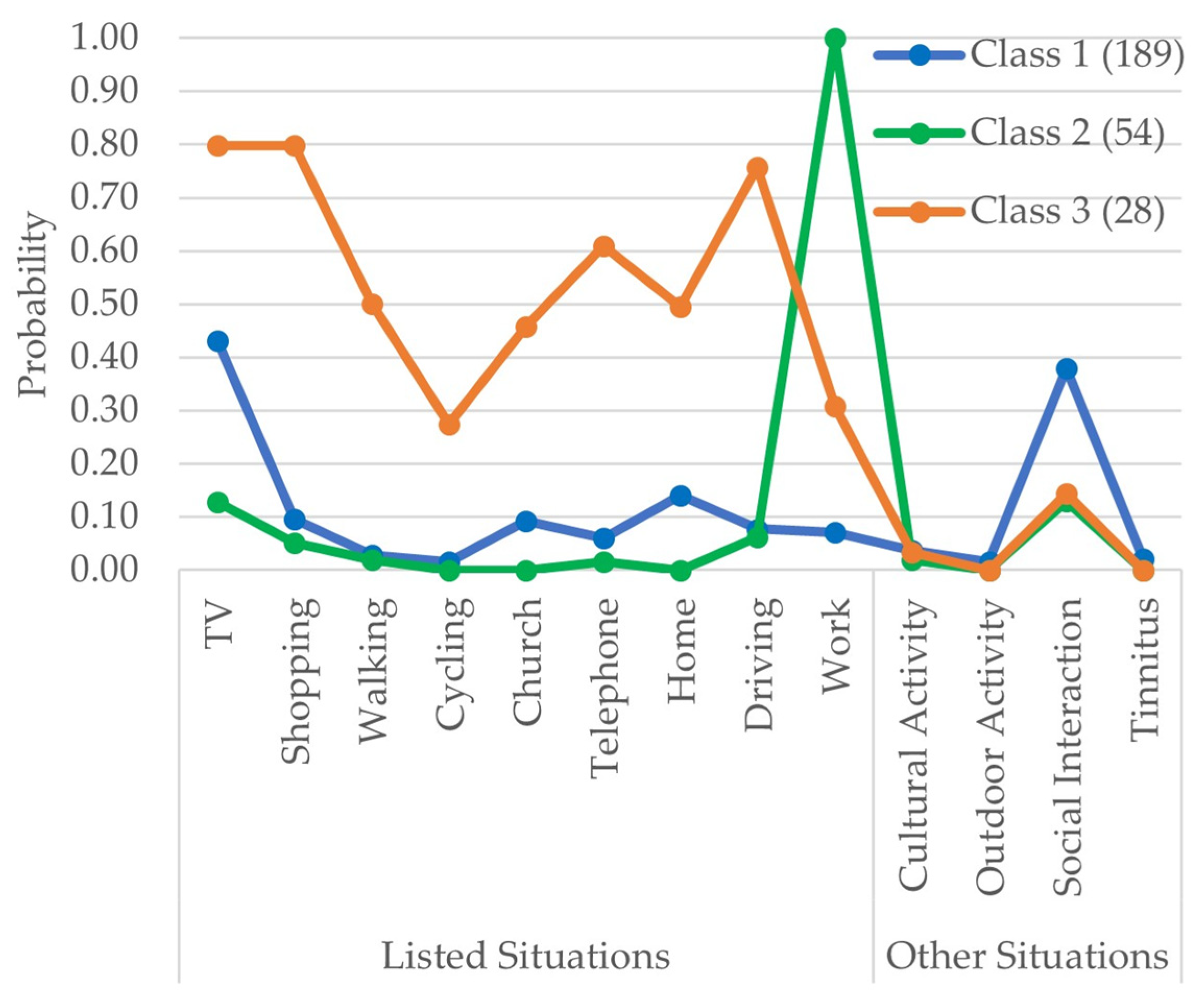
3.3. Fitted 3-Class Latent Class Model
3.4. Covariates
3.5. Self-Reported Outcome
3.5.1. Effect of Situational Use on Self-Reported Outcomes
3.5.2. Effect of Other Variables on Self-Reported Outcomes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williger, B.; Lang, F.R. Hearing aid use in everyday life: Managing contextual variability. Gerontology 2015, 61, 158–165. [Google Scholar] [CrossRef]
- Lunner, T. Cognitive function in relation to hearing aid use. Int. J. Audiol. 2003, 42, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Erber, N.P. Use of hearing aids by older people: Influence of non-auditory factors (vision, manual dexterity). Int. J. Audiol. 2003, 42, 2S21–2S25. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.L.N.; Hickson, L.; McPherson, B. Hearing Aid Satisfaction: What Does Research from the Past 20 Years Say? Trends Amplif. 2003, 7, 117–161. [Google Scholar] [CrossRef] [Green Version]
- Pasta, A.; Szatmari, T.-I.; Christensen, J.H.; Jensen, K.J.; Pontoppidan, N.H.; Sun, K.; Larsen, J.E. Clustering Users Based on Hearing Aid Use: An Exploratory Analysis of Real-World Data. Front. Digit. Health 2021, 3, 725130. [Google Scholar] [CrossRef]
- Christensen, J.H.; Saunders, G.H.; Havtorn, L.; Pontoppidan, N.H. Real-World Hearing Aid Usage Patterns and Smartphone Connectivity. Front. Digit. Health 2021, 3, 722186. [Google Scholar] [CrossRef] [PubMed]
- Humes, L.; Ahlstrom, J.; Bratt, G.; Peek, B. Studies of Hearing-Aid Outcome Measures in Older Adults: A Comparison of Technologies and an Examination of Individual Differences. Semin. Hear. 2009, 30, 112–128. [Google Scholar] [CrossRef] [Green Version]
- Humes, L.E.; Garner, C.B.; Wilson, D.L.; Barlow, N.N. Hearing-Aid Outcome Measures Following One Month of Hearing Aid Use by the Elderly. J. Speech Lang. Hear. Res. 2001, 44, 469–486. [Google Scholar] [CrossRef] [Green Version]
- Laplante-Lévesque, A.; Knudsen, L.V.; Preminger, J.E.; Jones, L.; Nielsen, C.; Öberg, M.; Lunner, T.; Hickson, L.; Naylor, G.; Kramer, S.E. Hearing help-seeking and rehabilitation: Perspectives of adults with hearing impairment. Int. J. Audiol. 2012, 51, 93–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laplante-Lévesque, A.; Nielsen, C.; Jensen, L.D.; Naylor, G. Patterns of hearing aid usage predict hearing aid use amount (data logged and self-reported) and overreport. J. Am. Acad. Audiol. 2014, 25, 187–198. [Google Scholar] [CrossRef]
- Humes, L.E.; Rogers, S.E.; Main, A.K.; Kinney, D.L. The acoustic environments in which older adults wear their hearing aids: Insights from datalogging sound environment classification. Am. J. Audiol. 2018, 27, 594–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, K.E.; Andersen, L.S.; Christensen, J.H.; Neher, T. Assessing real-life benefit from hearing-aid noise management: Ssq12 questionnaire versus ecological momentary assessment with acoustic data-logging. Am. J. Audiol. 2021, 30, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A. Health-Related Quality of Life Following Hearing Aid Treatment a Large Cohort Study; Aalborg Universitetsforlag: Aalborg, Denmark, 2019. [Google Scholar]
- Houmøller, S.S. Self-Reported Hearing Aid Effectiveness in Patients with Age-Related Hearing Loss; University of Southern Denmark: Odense, Denmark, 2021. [Google Scholar]
- Noble, W.; Jensen, N.S.; Naylor, G.; Bhullar, N.; Akeroyd, M.A. A short form of the Speech, Spatial and Qualities of Hearing scale suitable for clinical use: The SSQ12. Int. J. Audiol. 2013, 52, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.M.; Alexander, G.C. The International Outcome Inventory for Hearing Aids (IOI-HA): Psychometric properties of the english version. Int. J. Audiol. 2002, 41, 30–35. [Google Scholar] [CrossRef]
- Thunberg Jespersen, C.; Bille, M.; Legarth, J.V. Psychometric properties of a revised Danish translation of the international outcome inventory for hearing aids (IOI-HA). Int. J. Audiol. 2014, 53, 302–308. [Google Scholar] [CrossRef] [Green Version]
- Hagenaars, J.A.; McCutcheon, A.L. Applied Latent Class Analysis; Hagenaars, J.A., McCutcheon, A.L., Eds.; Cambridge University Press: Cambridge, UK, 2002; ISBN 9780521594516. [Google Scholar]
- Weller, B.E.; Bowen, N.K.; Faubert, S.J. Latent Class Analysis: A Guide to Best Practice. J. Black Psychol. 2020, 46, 287–311. [Google Scholar] [CrossRef]
- Linzer, D.A.; Lewis, J.B. poLCA: An R package for polytomous variable latent class analysis. J. Stat. Softw. 2011, 42, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Hocking, R.R. A Biometrics Invited Paper. The Analysis and Selection of Variables in Linear Regression. Biometrics 1976, 32, 1–49. [Google Scholar] [CrossRef]
- Leijon, A.; Dillon, H.; Hickson, L.; Kinkel, M.; Kramer, S.E.; Nordqvist, P. Analysis of data from the International Outcome Inventory for Hearing Aids (IOI-HA) using Bayesian Item Response Theory. Int. J. Audiol. 2020, 60, 81–88. [Google Scholar] [CrossRef]
- Nylund-Gibson, K.; Choi, A.Y. Ten frequently asked questions about latent class analysis. Transl. Issues Psychol. Sci. 2018, 4, 440. [Google Scholar] [CrossRef]
- Kensinger, E.A. Negative emotion enhances memory accuracy: Behavioral and neuroimaging evidence. Curr. Dir. Psychol. Sci. 2007, 16, 213–218. [Google Scholar] [CrossRef]
- Staehelin, K.; Bertoli, S.; Probst, R.; Schindler, C.; Dratva, J.; Stutz, E.Z. Gender and Hearing Aids: Patterns of Use and Determinants of Nonregular Use. Ear Hear. 2011, 32, e26–e37. [Google Scholar] [CrossRef] [PubMed]
- Stock, A.; Fichtl, E.; Heller, O. Comparing Determinants of Hearing Instrument Satisfaction in Germany and the United States. High Perform. Hear. Solut. 1997, 2, 40–46. [Google Scholar]
- Dillon, H.; Birtles, G.; Lovegrove, R. Measuring the Outcomes of a National Rehabilitation Program: Normative Data for the Client Oriented Scale of Improvement (COSI) and the Hearing Aid User’s Questionnaire (HAUQ). J. Am. Acad. Audiol. 1999, 10, 67–79. [Google Scholar] [CrossRef]
- Jerram, J.C.K.; Purdy, S.C. Technology, expectations, and adjustment to hearing loss: Predictors of hearing aid outcome. J. Am. Acad. Audiol. 2001, 12, 64–79. [Google Scholar] [CrossRef]
- Hickson, L.; Timm, M.; Worrall, L.; Bishop, K. Hearing aid fitting: Outcomes for older adults. Aust. J. Audiol. 1999, 21, 9–21. [Google Scholar]
- Houmøller, S.S.; Wolff, A.; Möller, S.; Narne, V.K.; Narayanan, S.K.; Godballe, C.; Hougaard, D.D.; Loquet, G.; Gaihede, M.; Hammershøi, D.; et al. Prediction of successful hearing aid treatment in first-time and experienced hearing aid users: Using the International Outcome Inventory for Hearing Aids. Int. J. Audiol. 2021, 61, 119–129. [Google Scholar] [CrossRef]
- Ferguson, M.; Maidment, D.; Russell, N.; Gregory, M.; Nicholson, R. Motivational engagement in first-time hearing aid users: A feasibility study. Int. J. Audiol. 2016, 55, S23–S33. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categorized Situations | Description |
|---|---|
| Cultural Activity | It included descriptions about using or not using HA while in the cinema, theatre, concerts, listening to music, playing musical instruments, etc. |
| Outdoor Activity | The descriptions included hunting, sailing, gardening, golf club, etc. |
| Social Interaction | Interacting with a small group of people and attending meetings/lectures/talks. |
| Tinnitus | Situations when they experienced tinnitus. |
| Discomfort | Two aspects were described: (1) Physical discomfort caused due to sweating or itching and (2) Emotional discomfort due to fatigue or tiredness. |
| Fear of Losing | Descriptions included situations where there was a fear of losing the HA, for example, while playing with grandchildren and many more. |
| Noisy Situation | This included descriptions of machine noise, reverberation, and other natural noises. |
| Physical Activity | Description of situations included while at the gym, doing yoga, running, and other physical activities. |
| Sleep | During sleep. |
| Wet Condition | The description included situations related to being in the rain or at a swimming pool where there was a chance of HA getting wet. |
| When Alone | When alone at home or elsewhere. |
| Windy Condition | It included situations where a lot of wind noise was described. |
| With Many People | The description included situations such as being alongside many people or very large gatherings. |
| Non-use | Describing the situation that they had stopped using the HAs altogether. |
| Invalid Responses | Severely inconsistent responses. |
| Predictors | IOI-HA Factor 1 Adj R2 = 0.36 | IOI-HA Factor 2 Adj R2 = 0.12 | Total SSQ12 Adj R2 = 0.15 | |||
|---|---|---|---|---|---|---|
| Estimates [CI] | p-Value | Estimates [CI] | p-Value | Estimates [CI] | p-Value | |
| (Intercept) | 0.93 [0.40–1.46] | 0.001 | −0.14 [−0.73–0.46] | 0.649 | 5.06 [4.63–5.50] | <0.001 |
| Hearing aid use (Ref: Regular use) | ||||||
| Class 1 | −2.03 [−2.52–−1.53] | <0.001 | −0.51 [−0.90–−0.11] | 0.012 | −0.17 [−0.46–0.11] | 0.229 |
| Class 2 | −4.02 [−4.77–−3.26] | <0.001 | −0.77 [−1.37–−0.17] | 0.012 | −0.44 [−0.88–−0.01] | 0.045 |
| Class 3 | −3.13 [−3.90–−2.35] | <0.001 | −0.53 [−1.15–0.09] | 0.092 | −0.47 [−0.92–−0.03] | 0.038 |
| Non-use | −8.88 [−9.95–−7.82] | <0.001 | −2.74 [−3.58–−1.90] | <0.001 | −0.55 [−1.16–0.05] | 0.073 |
| Age | −0.19 [−0.42–0.04] | 0.102 | NA | NA | ||
| Gender, Male (Ref. Female) | NA | −0.26 [−0.61–0.10] | 0.152 | 0.36 [0.10–0.62] | 0.006 | |
| User Type, First time (Ref. Experienced) | NA | 0.79 [0.38–1.20] | <0.001 | 0.54 [0.24–0.83] | <0.001 | |
| Better hearing ear PTA4 | 0.27 [0.04–0.51] | 0.024 | −0.30 [−0.51–−0.09] | 0.005 | −0.33 [−0.48–−0.18] | <0.001 |
| Better hearing ear WRS | NA | 0.23 [0.04–0.41] | 0.017 | 0.23 [0.09–0.36] | 0.001 | |
| PTA-based Symmetric HL (Ref: asymmetric HL) | 0.58 [0.03–1.12] | 0.039 | 0.62 [0.19–1.06] | 0.005 | 0.60 [0.28–0.91] | <0.001 |
| Tinnitus (Present) (Ref: not present) | NA | −0.51 [−0.95–−0.08] | 0.020 | −0.92 [−1.23–−0.61] | <0.001 | |
| Motivation Q1 score (Readiness) | NA | −0.27 [−0.47–−0.06] | 0.010 | NA | ||
| Mean motivation Q2 score (Self-efficacy) | 0.69 [0.47–0.91] | <0.001 | 0.24 [0.04–0.45] | 0.020 | 0.21 [0.08–0.33] | 0.001 |
| Work status (Ref. Working) Not part of the job market | NA | 0.11 [−0.29–0.51] | 0.585 | NA | ||
| Not working | −0.96 [−1.89–−0.03] | 0.042 | ||||
| Income (in DKK) (Ref. 100,000–300,000) (EUR 12,500–40,000) under 100,000 (under EUR 12,500) | NA | NA | 1.16 [−2.04–−0.28] | 0.010 | ||
| 300,000–600,000 (EUR 40,000–80,000) | 0.30 [−0.00–0.60] | 0.052 | ||||
| 600,000–900,000 (EUR 80,000–120,000) | 0.32 [−0.10–0.73] | 0.134 | ||||
| Above 900,000 (Above EUR 120,000) | 0.81 [0.16–1.46] | 0.015 | ||||
| Undisclosed | −0.20 [−0.57–0.18] | 0.299 | ||||
| Predictors | IOI-HA Factor 1 Adj R2 = 0.38 | IOI-HA Factor 2 Adj R2 = 0.13 | Total SSQ12 Adj R2 = 0.17 | |||
|---|---|---|---|---|---|---|
| Estimates [CI] | p-Value | Estimates [CI] | p-Value | Estimates [CI] | p-Value | |
| (Intercept) | 0.33 [−0.24–0.89] | 0.261 | −0.06 [−0.66–0.53] | 0.833 | 5.10 [4.68–5.53] | <0.001 |
| Hearing aid use | ||||||
| (Ref: Regular use) | ||||||
| Class 1 | −4.06 [−4.59–−3.54] | <0.001 | −0.71 [−1.14–−0.28] | 0.001 | −0.31 [−0.62–−0.00] | 0.047 |
| Class 2 | −2.24 [−3.13–−1.34] | <0.001 | −0.67 [−1.41–0.06] | 0.071 | −0.44 [−0.97–0.09] | 0.104 |
| Class 3 | −1.88 [−3.05–−0.71] | 0.002 | −1.40 [−2.34–−0.45] | 0.004 | −1.15 [−1.83–−0.47] | 0.001 |
| Non-use | −9.42 [−10.69–−8.15] | <0.001 | −3.65 [−4.67–−2.63] | <0.001 | −1.00 [−1.74–−0.26] | 0.008 |
| Age | −0.21 [−0.44–0.03] | 0.080 | NA | −0.11 [−0.26–0.03] | 0.122 | |
| Gender, Male (Ref. Female) | NA | −0.32 [−0.67–0.03] | 0.074 | 0.36 [0.11–0.62] | 0.005 | |
| User Type, First time (Ref. Experienced) | 0.46 [−0.05–0.97] | 0.078 | 0.71 [0.30–1.12] | 0.001 | 0.50 [0.20–0.79] | 0.001 |
| Better hearing ear PTA4 | 0.46 [0.21–0.71] | <0.001 | −0.30 [−0.51–−0.09] | 0.005 | −0.31 [−0.46–−0.15] | <0.001 |
| Better hearing ear WRS | NA | 0.23 [0.05–0.42] | 0.014 | 0.21 [0.07–0.34] | 0.003 | |
| PTA-based Symmetric HL (Ref: asymmetric HL) | 0.56 [0.03–1.09] | 0.040 | 0.66 [0.23–1.09] | 0.003 | 0.60 [0.29–0.91] | <0.001 |
| Tinnitus (Present) (Ref: not present) | NA | −0.54 [−0.97–−0.11] | 0.013 | −0.99 [−1.30–−0.68] | <0.001 | |
| Motivation Q1 score (Readiness) | NA | −0.29 [−0.49–−0.08] | 0.006 | −0.15 [−0.29–0.00] | 0.056 | |
| Mean motivation Q2 score (Self-efficacy) | 0.56 [0.34–0.77] | <0.001 | 0.20 [−0.01–0.40] | 0.062 | 0.25 [0.01–0.40] | 0.001 |
| Work status (Ref. Working) Not part of the job market | NA | 0.04 [−0.37–0.46] | 0.840 | NA | ||
| Not working | −0.97 [−1.91–−0.02] | 0.045 | ||||
| Income (in DKK) (Ref. 100,000–300,000) (EUR 12,500–40,000) under 100,000 (under EUR 12,500) | NA | NA | −1.19 [−2.07–−0.31] | 0.008 | ||
| 300,000–600,000 (EUR 40,000–80,000) | 0.28 [−0.02–0.58] | 0.065 | ||||
| 600,000–900,000 (EUR 80,000–120,000) | 0.32 [−0.11–0.75] | 0.145 | ||||
| Above 900,000 (Above EUR 120,000) | 0.74 [0.09–1.40] | 0.026 | ||||
| Undisclosed | −0.17 [−0.55–0.20] | 0.361 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Narayanan, S.K.; Houmøller, S.S.; Wolff, A.; Lund, K.; Möller, S.; Hougaard, D.D.; Gaihede, M.; Schmidt, J.H.; Hammershøi, D. Self-Reported Hearing-Aid Use Patterns in an Adult Danish Population. Audiol. Res. 2023, 13, 221-235. https://doi.org/10.3390/audiolres13020021
Narayanan SK, Houmøller SS, Wolff A, Lund K, Möller S, Hougaard DD, Gaihede M, Schmidt JH, Hammershøi D. Self-Reported Hearing-Aid Use Patterns in an Adult Danish Population. Audiology Research. 2023; 13(2):221-235. https://doi.org/10.3390/audiolres13020021
Chicago/Turabian StyleNarayanan, Sreeram K., Sabina S. Houmøller, Anne Wolff, Katja Lund, Sören Möller, Dan D. Hougaard, Michael Gaihede, Jesper H. Schmidt, and Dorte Hammershøi. 2023. "Self-Reported Hearing-Aid Use Patterns in an Adult Danish Population" Audiology Research 13, no. 2: 221-235. https://doi.org/10.3390/audiolres13020021