
Comparison of Speech, Spatial, and Qualities of Hearing Scale (SSQ) and the Abbreviated Profile of Hearing Aid Benefit (APHAB) Questionnaires in a Large Cohort of Self-Reported Normal-Hearing Adult Listeners †
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Materials
3. Data Analysis
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gatehouse, S.; Noble, W. The Speech, Spatial and Qualities of Hearing Scale (SSQ). Int. J. Audiol. 2004, 43, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.M.; Alexander, G.C. The Abbreviated Profile of Hearing Aid Benefit. Ear Hear. 1995, 16, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Noble, W.; Tyler, R.S.; Dunn, C.C.; Bhullar, N. Younger and older-age adults with unilateral and bilateral cochlear implants: Speech and spatial hearing self-ratings and performance. Otol. Neurotol. 2009, 30, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Yawn, R.J.; O’Connell, B.P.; Dwyer, R.T.; Sunderhaus, L.W.; Reynolds, S.; Haynes, D.S.; Gifford, R.H. Bilateral cochlear implantation versus bimodal hearing in patients with functional residual hearing: A within-subjects comparison of audiologic performance and quality of life. Otol. Neurotol. 2018, 39, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Dumper, J.; Hodgetts, B.; Liu, R.; Brandner, N. Indications for bone-anchored hearing AIDS: A functional outcomes study. J. Otolaryngol. Head Neck Surg. 2008, 38, 96–105. [Google Scholar] [CrossRef]
- Zahorik, P.; Rothpletz, A.M. Speech, spatial, and qualities of hearing scale (SSQ): Normative data from young, normal-hearing listeners. Proc. Mtgs. Acoust. 2014, 21, 050007. [Google Scholar] [CrossRef]
- Banh, J.; Singh, G.; Pichora-Fuller, M.K. Age affects responses on the Speech, Spatial, and Qualities of hearing scale (SSQ) by adults with minimal audiometric loss. J. Am. Acad. Audiol. 2012, 23, 81–91. [Google Scholar] [CrossRef]
- Saunders, G.H.; Frederick, M.T.; Arnold, M.; Silverman, S.; Chisolm, T.H.; Myers, P. Auditory difficulties in blast-exposed Veterans with clinically normal hearing. J. Rehabil. Res. Dev. 2015, 52, 343–360. [Google Scholar] [CrossRef]
- Singh, G.; Pichora-Fuller, K. Older adults’ performance on the speech, spatial, and qualities of hearing scale (SSQ): Test-retest reliability and a comparison of interview and self-administration methods. Int. J. Audiol. 2010, 49, 733–740. [Google Scholar] [CrossRef]
- Aguiar, R.G.R.; de Almeida, K.; de Miranda-Gonsalez, E.C. Test-Retest Reliability of the Speech, Spatial and Qualities of Hearing Scale (SSQ) in Brazilian Portuguese. Int. Arch. Otorhinolaryngol. 2019, 23, e380–e383. [Google Scholar] [CrossRef]
- Batthyany, C.; Schut, A.R.; van der Schroeff, M.; Vroegop, J. Translation and validation of the speech, spatial, and qualities of hearing scale (SSQ) and the hearing environments and reflection on quality of life (HEAR-QL) questionnaire for children and adolescents in Dutch. Int. J. Audiol. 2022, 6, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Demeester, K.; Topsakal, V.; Hendrickx, J.J.; Fransen, E.; van Laer, E.; Van Camp, G.; van Wieringen, A. Hearing disability measured by the Speech, Spatial, and Qualities of Hearing Scale in clinically normal-hearing and hearing-impaired middle-aged persons, and disability screening by means of a reduced SSQ (the SSQ5). Ear Hear. 2012, 33, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Falzone, C.; Guerzoni, L.; Pizzol, E.; Fabrizi, E.; Cuda, D. An Adaptation and Validation Study of the Speech, Spatial, and Qualities of Hearing Scale (SSQ) in Italian Normal-Hearing Children. Audiol. Res. 2022, 12, 297–306. [Google Scholar] [CrossRef]
- Heo, J.H.; Lee, J.H.; Lee, W.S. Bimodal benefits on objective and subjective outcomes for adult cochlear implant users. Korean J. Audiol. 2013, 17, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Lotfi, Y.; Nazeri, A.R.; Asgari, A.; Moosavi, A.; Bakhshi, E. Iranian Version of Speech, Spatial, and Qualities of Hearing Scale: A Psychometric Study. Acta Med. Iran. 2016, 54, 756–764. [Google Scholar] [PubMed]
- Moulin, A.; Pauzie, A.; Richard, C. Validation of a French translation of the speech, spatial, and qualities of hearing scale (SSQ) and comparison with other language versions. Int. J. Audiol. 2015, 54, 889–898. [Google Scholar] [CrossRef] [PubMed]
- Moulin, A.; Richard, C. Sources of variabiligy for speech, spatial, and qualities of hearing scale (SSQ) scores in normal-hearing and hearing-impaired populations. Int. J. Audiol. 2016, 55, 105–109. [Google Scholar] [CrossRef]
- Alkhodair, M.B.; Mesallam, T.A.; Hagr, A.; Yousef, M.F. Arabic Version of short form of the Speech, Spatial, and Qualities of Hearing Scale (SSQ12). Saudi Med. J. 2021, 42, 1180–1185. [Google Scholar] [CrossRef]
- Moulin, A.; Vergne, J.; Gallégo, S.; Micheyl, C. A new speech, spatial, and qualities of hearing scale short-form: Factor, cluster, and comparative analyses. Ear Hear. 2019, 40, 938–950. [Google Scholar] [CrossRef]
- Noble, W.; Jensen, N.S.; Naylor, G.; Bhullar, N.; Akeroyd, M.A. A short form of the Speech, Spatial and Qualities of Hearing scale suitable for clinical use: The SSQ12. Int. J. Audiol. 2013, 52, 409–412. [Google Scholar] [CrossRef]
- Löhler, J.; Grabner, F.; Wollenberg, B.; Schlattmann, P.; Schonweiler, R. Sensitivity and specificity of the abbreviated profile of hearing aid benefit (APHAB). Eur. Arch. Otorhinolaryngol. 2017, 274, 3593–3598. [Google Scholar] [CrossRef]
- Linstrom, C.J.; Silverman, C.A.; Yu, G.P. Efficacy of the bone-anchored hearing aid for single-sided deafness. Laryngoscope 2009, 119, 713–720. [Google Scholar] [CrossRef] [PubMed]
- García, J.M.; Urquijo, D.P.; Puerta, M.; Mosquera, C.A.; Hernández, L.M.; Aparicio, M.L.; Barõn, C.; Tono, A.M.O.; Peñaranda, A. Cochlear implant in patients with single sided deafness: Hearing results and communicative benefits. Cochlear Implant. Int. 2020, 21, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Duret, S.; Bigand, E.; Guigou, C.; Marty, N.; Lalitte, P.; Grayeli, A.B. Participation of acoustic and electric hearing in perceiving musical sounds. Front. Neurosci. 2021, 15, 558421. [Google Scholar] [CrossRef] [PubMed]
- Brännström, K.J.; Andersson, K.; Sandgren, O.; Whitling, S. Clinical Application and Psychometric Properties of a Swedish Translation of the Abbreviated Profile of Hearing Aid Benefit. J. Am. Acad. Audiol. 2020, 31, 656–665. [Google Scholar] [CrossRef]
- Heggdal, P.O.L.; Nordvik, Ø.; Brännström, J.; Vassbotn, F.; Aarstad, A.K.; Aarstad, H.J. Clinical application and psychometric properties of a Norwegian questionnaire for the self-assessment of communication in quiet and adverse conditions using two revised APHAB subscales. J. Am. Acad. Audiol. 2018, 29, 025–034. [Google Scholar] [CrossRef]
- Löhler, J.; Moser, L.; Heinrich, D.; Hörmann, K.; Walther, L.E. Results of clinical use of the German version of the APHAB. HNO 2012, 60, 626–636. [Google Scholar] [CrossRef]
- Lim, H.J.; Park, M.K.; Cho, Y.S.; Han, G.C.; Choi, J.W.; An, Y.H.; Kim, B.J.; Choi, B.Y. Validation of the Korean version of the abbreviated profile of hearing aid benefit. Korean J. Otorhinolaryngol. Head Neck Surg. 2017, 60, 164–173. [Google Scholar] [CrossRef]
- Hearing Aid Research Lab. Abbreviated Profile of Hearing aid Benefit (APHAB). Available online: https://harlmemphis.org/abbreviated-profile-of-hearing-aid-benefit-aphab/ (accessed on 15 August 2020).
- Dornhoffer, J.R.; Meyer, T.A.; Dubno, J.R.; McRackan, T.R. Assessment of hearing aid benefit using patient-reported outcomes and audiologic measures. Audiol. Neurotol. 2020, 25, 215–223. [Google Scholar] [CrossRef]
- de Andrade, A.N.; Soares, A.; Skarzynska, M.B.; Skarzynski, P.H.; Sanfins, M.D.; Gil, D. Self-Perception of Hearing Difficulties and Quality of Life in Individuals with Hearing Loss. Audiol. Res. 2022, 12, 527–538. [Google Scholar] [CrossRef]
- Valente, M.; Oeding, K.; Brockmeyer, A.; Smith, S.; Kallogjeri, D. Differences in word and phoneme recognition in quiet, sentence recognition in noise, and subjective outcomes between manufacturer first-fit and hearing aids programmed to NAL-NL2 using real-ear measures. J. Am. Acad. Audiol. 2018, 29, 706–721. [Google Scholar] [CrossRef] [PubMed]
- Dillon, M.T.; Buss, E.; Rooth, M.A.; King, E.R.; Deres, E.J.; Buchman, C.A.; Pillsbury, H.C.; Brown, K.D. Effect of cochlear implantation on quality of life in adults with unilateral hearing loss. Audiol. Neurotol. 2017, 22, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Fullgrabe, C.; Moore, B.C.J.; Stone, M.A. Age-group differences in speech identification despite matched audiometrically normal hearing: Contributions from auditory temporal processing and cognition. Front. Aging Neurosci. 2015, 6, 125. [Google Scholar] [CrossRef]
- Cox, R.M.; Alexander, G.C.; Gray, G.A. Audiometric correlates of the unaided APHAB. J. Am. Acad. Audiol. 2003, 14, 361–371. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
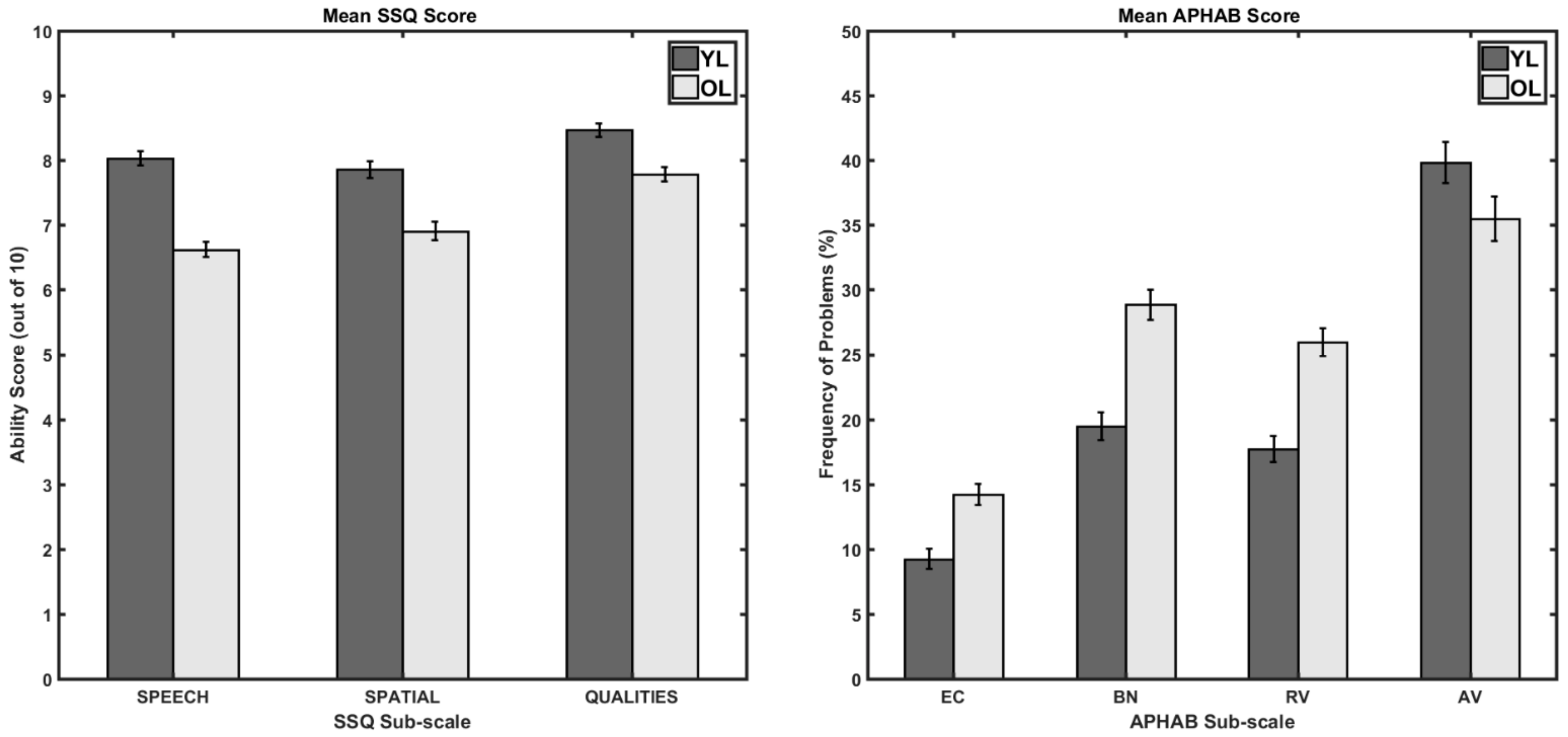
| Questionnaire | Sub Scale | Younger Listeners | Older Listeners | Simple Effect Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | 95% CI | M | SD | 95% CI | ||||||
| LB | UB | LB | UB | F (1, 252) | p | ||||||
| SSQ | SPCH | 8.02 | 1.11 | 7.83 | 8.21 | 6.62 | 1.49 | 6.35 | 6.89 | 73.61 | <0.001 |
| SPAL | 7.86 | 1.46 | 7.62 | 8.11 | 6.91 | 1.56 | 6.63 | 7.19 | 25.03 | <0.001 | |
| QUAL | 8.47 | 1.03 | 8.31 | 8.64 | 7.77 | 1.37 | 7.52 | 8.02 | 20.39 | <0.001 | |
| APHAB | EC | 9.22 | 7.14 | 8.02 | 10.43 | 14.2 | 10.79 | 12.23 | 16.17 | 19.22 | <0.001 |
| BN | 19.45 | 11.96 | 17.42 | 21.48 | 28.3 | 13.12 | 25.91 | 30.69 | 35.43 | <0.001 | |
| RV | 17.72 | 10.58 | 15.93 | 19.51 | 25.96 | 12.97 | 23.59 | 28.32 | 31.05 | <0.001 | |
| AV | 39.79 | 20.29 | 36.35 | 43.23 | 35.46 | 16.07 | 32.53 | 38.39 | 3.46 | 0.064 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srinivasan, N.; O’Neill, S. Comparison of Speech, Spatial, and Qualities of Hearing Scale (SSQ) and the Abbreviated Profile of Hearing Aid Benefit (APHAB) Questionnaires in a Large Cohort of Self-Reported Normal-Hearing Adult Listeners. Audiol. Res. 2023, 13, 143-150. https://doi.org/10.3390/audiolres13010014
Srinivasan N, O’Neill S. Comparison of Speech, Spatial, and Qualities of Hearing Scale (SSQ) and the Abbreviated Profile of Hearing Aid Benefit (APHAB) Questionnaires in a Large Cohort of Self-Reported Normal-Hearing Adult Listeners. Audiology Research. 2023; 13(1):143-150. https://doi.org/10.3390/audiolres13010014
Chicago/Turabian StyleSrinivasan, Nirmal, and Sadie O’Neill. 2023. "Comparison of Speech, Spatial, and Qualities of Hearing Scale (SSQ) and the Abbreviated Profile of Hearing Aid Benefit (APHAB) Questionnaires in a Large Cohort of Self-Reported Normal-Hearing Adult Listeners" Audiology Research 13, no. 1: 143-150. https://doi.org/10.3390/audiolres13010014