The Utility of Lesser Trochanter Version to Estimate Femoral Anteversion in Total Hip Arthroplasty: A Three-Dimensional Computed Tomography Study

 ,
,
Abstract
:1. Introduction
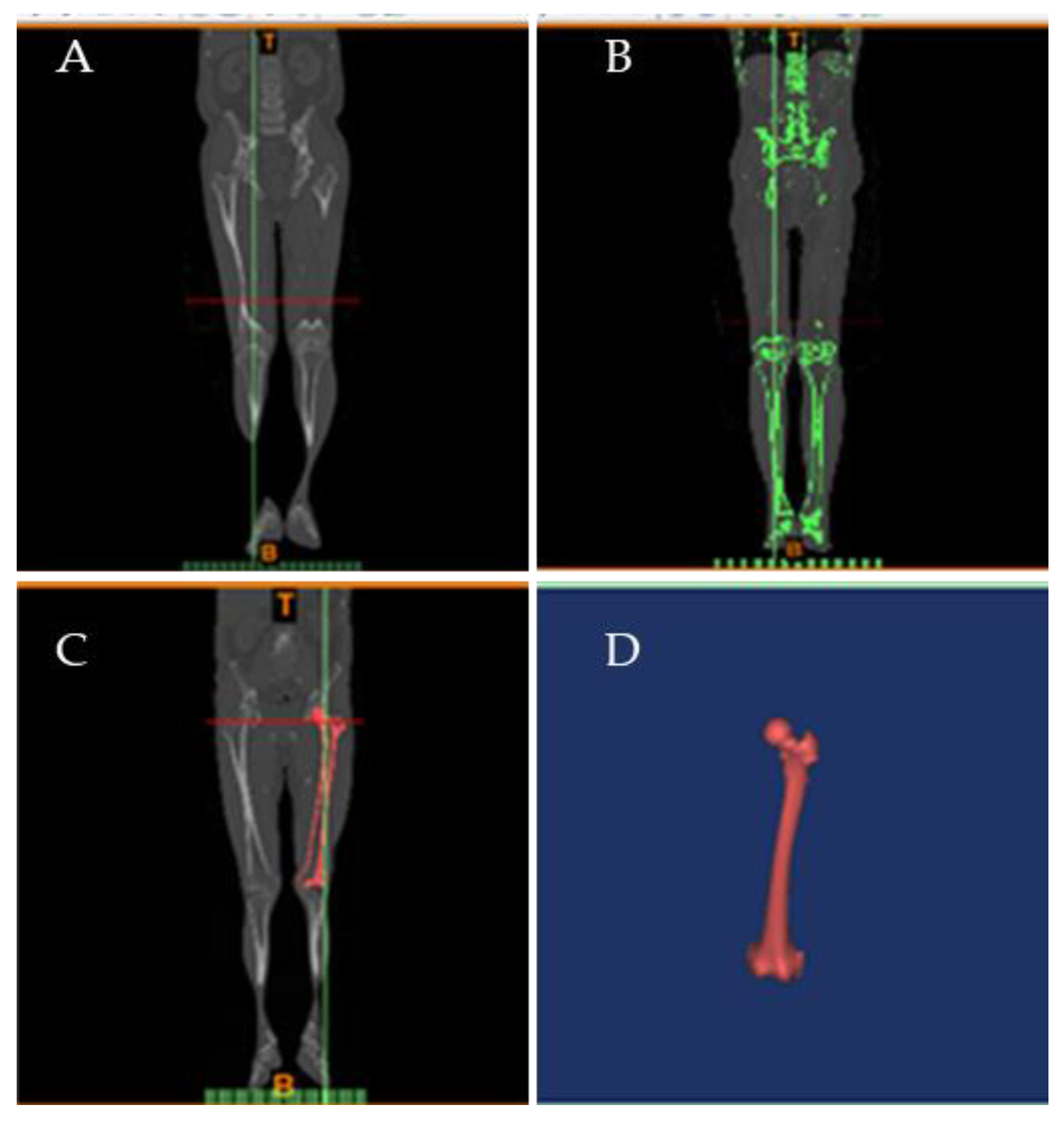
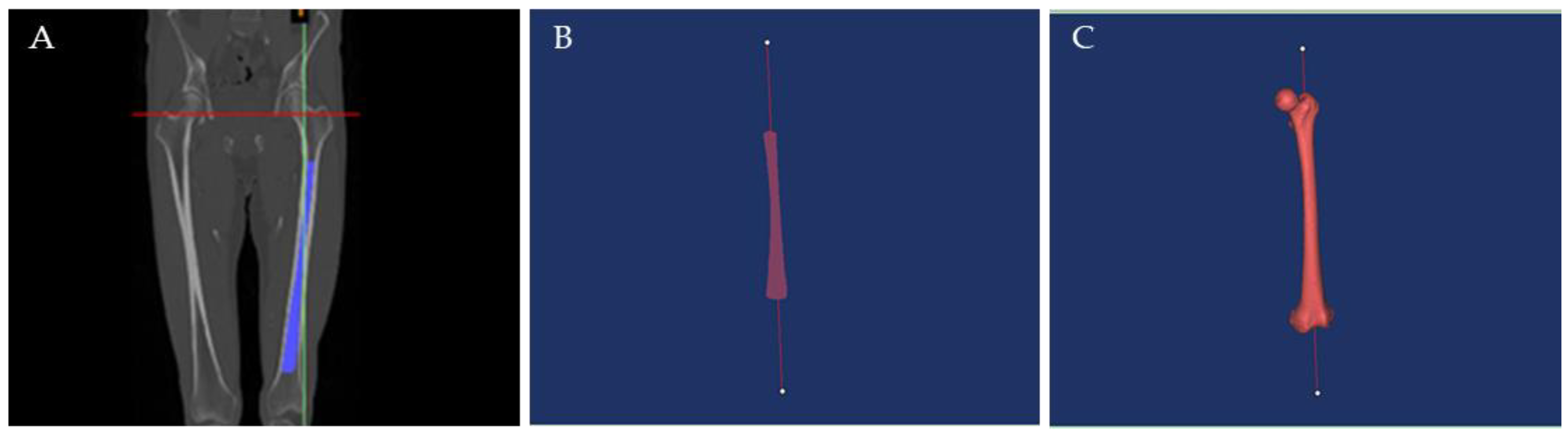
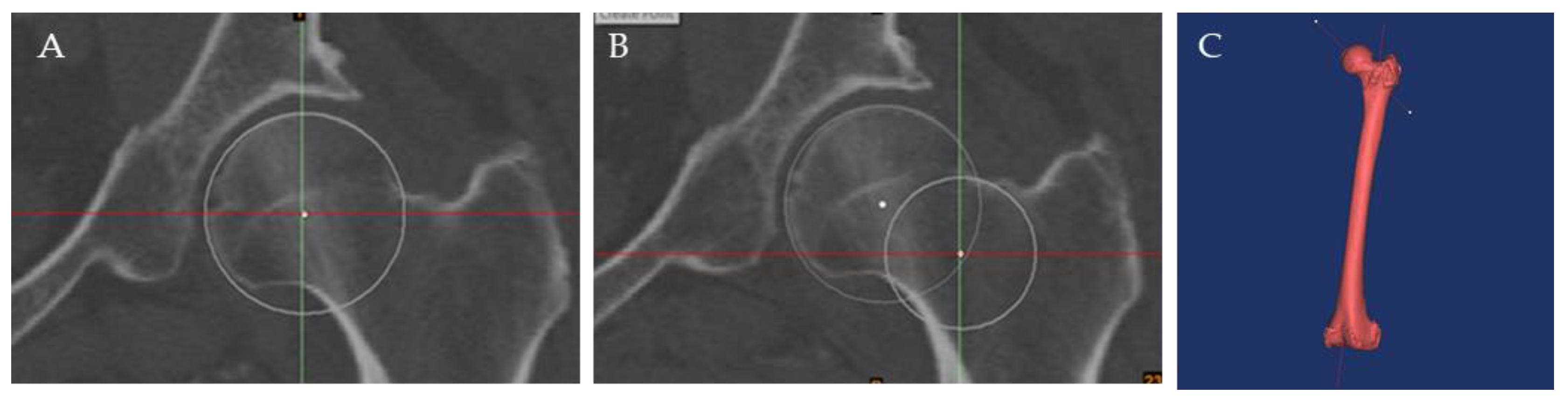
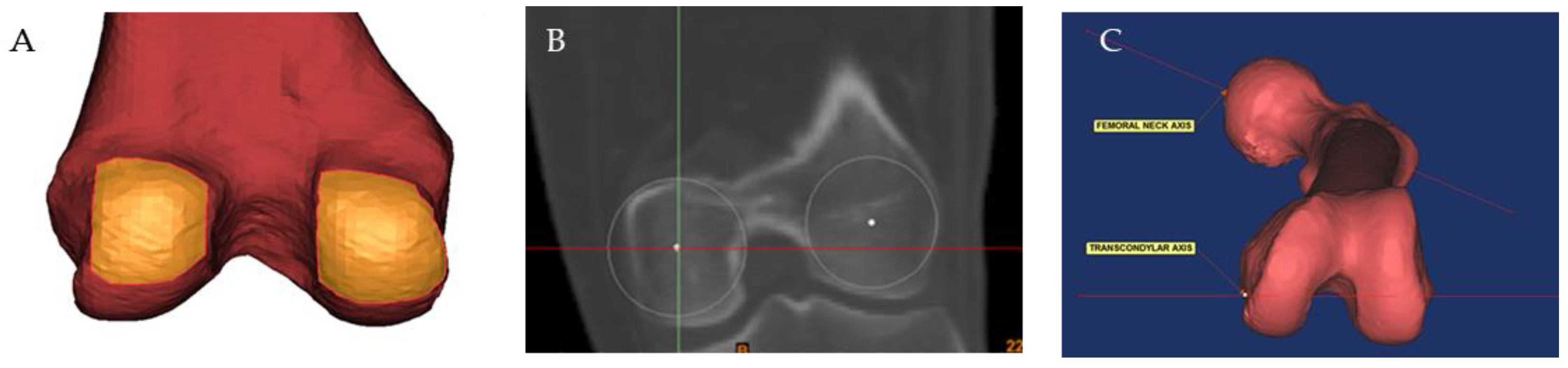
2. Methods
3. Results
3.1. Participants
3.2. Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, Y.; Xiao, H.; Xue, F. Causes of and treatment options for dislocation following total hip arthroplasty (Review). Exp. Ther. Med. 2019, 18, 1715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fessy, M.H.; Putman, S.; Viste, A.; Isida, R.; Ramdane, N.; Ferreira, A.; Leglise, A.; Rubens-Duval, B.; Bonin, N.; Bonnomet, F.; et al. What are the risk factors for dislocation in primary total hip arthroplasty? A multicenter case-control study of 128 unstable and 438 stable hips. Orthop. Traumatol. Surg. Res. 2017, 103, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Dorr, L.D.; Malik, A.; Dastane, M.; Wan, Z. Combined anteversion technique for total hip arthroplasty. In Clinical Orthopaedics and Related Research; Springer: New York, NY, USA, 2009; Volume 467, pp. 119–127. [Google Scholar]
- Schwartz, A.M.; Farley, K.X.; Guild, G.N.; Bradbury, T.L. Projections and Epidemiology of Revision Hip and Knee Arthroplasty in the United States to 2030. J. Arthroplasty 2020, 35, S79–S85. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, M.; Feinberg, J.R.; Capello, W.N.; D’Antonio, J.A. Morphologic Features of the Acetabulum and Femur: Anteversion Angle and Implant Positioning. Clin. Orthop. Relat. Res. 2001, 393. Available online: https://journals.lww.com/clinorthop/Fulltext/2001/12000/Morphologic_Features_of_the_Acetabulum_and_Femur_.6.aspx (accessed on 27 March 2022). [CrossRef]
- Ranawac, C.S.; Maynard, M.J. Modern technique of cemented total hip arthroplasty. Tech. Orthop. 1991, 6, 17–25. Available online: https://journals.lww.com/techortho/Fulltext/1991/09000/Modern_technique_of_cemented_total_hip.4.aspx (accessed on 27 March 2022). [CrossRef]
- Tönnis, D.; Heinecke, A. Acetabular and femoral anteversion: Relationship with osteoarthritis of the hip. J. Bone Jt. Surg.—Ser. A 1999, 81, 1747–1770. [Google Scholar] [CrossRef]
- Khattak, M.J.; Ashraf, U.; Nawaz, Z.; Noordin, S.; Umer, M. Surgical management of metastatic lesions of proximal femur and the hip. Ann. Med. Surg. 2018, 36, 90–95. [Google Scholar] [CrossRef]
- Jenkins, S.E.M.; Harrington, M.E.; Zavatsky, A.B.; O’Connor, J.J.; Theologis, T.N. Femoral muscle attachment locations in children and adults, and their prediction from clinical measurement. Gait Posture 2003, 18, 13–22. [Google Scholar] [CrossRef]
- Yun, H.H.; Yoon, J.R.; Yang, J.H.; Song, S.Y.; Park, S.B.; Lee, J.W. A validation study for estimation of femoral anteversion using the posterior lesser trochanter line. An analysis of computed tomography measurement. J. Arthroplasty 2013, 28, 1776–1780. [Google Scholar] [CrossRef]
- Khang, G.; Choi, K.; Kim, C.-S.; Yang, J.S.; Bae, T.-S. A study of Korean femoral geometry. Clin. Orthop. Relat. Res. 2003, 406, 116–122. [Google Scholar] [CrossRef]
- Botser, I.B.; Ozoude, G.C.; Martin, D.E.; Siddiqi, A.J.; Kuppuswami, S.; Domb, B.G. Femoral anteversion in the hip: Comparison of measurement by computed tomography, magnetic resonance imaging, and physical examination. Arthrosc.—J. Arthrosc. Relat. Surg. 2012, 28, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Sugano, N.; Noble, P.C.; Kamaric, E. A comparison of alternative methods of measuring femoral anteversion. J. Comput. Assist. Tomogr. 1998, 22, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Sariali, E.; Mouttet, A.; Pasquier, G.; Durante, E. Three-Dimensional Hip Anatomy in Osteoarthritis. Analysis of the Femoral Offset. J. Arthroplasty 2009, 24, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Siston, R.A.; Patel, J.J.; Goodman, S.B.; Delp, S.L.; Giori, N.J. The variability of femoral rotational alignment in total knee arthroplasty. J. Bone Jt. Surg.—Ser. A 2005, 87, 2276–2280. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.B.; Simon, S.R.; Kijewski, P.K.; Wilkinson, R.H.; Griscom, N.T. Femoral anteversion. J. Bone Jt. Surg.—Ser. A 1987, 69, 1169–1176. [Google Scholar] [CrossRef]
- Hoiseth, A.; Reikeras, O.; Fonstelien, E. Basic concepts of femoral neck anteversion: Comparison of two definitions. Br. J. Radiol. 1989, 62, 114–116. [Google Scholar] [CrossRef]
- Matsuda, S.; Miura, H.; Nagamine, R.; Mawatari, T.; Tokunaga, M.; Nabeyama, R.; Iwamoto, Y. Anatomical analysis of the femoral condyle in normal and osteoarthritic knees. J. Orthop. Res. 2004, 22, 104–109. [Google Scholar] [CrossRef]
- Iranpour, F.; Merican, A.M.; Dandachli, W.; Amis, A.A.; Cobb, J.P. The geometry of the trochlear groove. Clin. Orthop. Relat. Res. 2010, 468, 782–788. [Google Scholar] [CrossRef] [Green Version]
- Shon, W.Y.; Yun, H.H.; Yang, J.H.; Song, S.Y.; Park, S.B.; Lee, J.W. The Use of the Posterior Lesser Trochanter Line to Estimate Femoral Neck Version. An Analysis of Computed Tomography Measurements. J. Arthroplasty 2013, 28, 352–358. [Google Scholar] [CrossRef]
- Worlicek, M.; Weber, M.; Craiovan, B.; Zeman, F.; Grifka, J.; Renkawitz, T.; Wörner, M. Posterior lesser trochanter line should not be used as reference for assessing femoral version in CT scans: A retrospective reliability and agreement study. Acta Radiol. 2017, 58, 1101–1107. [Google Scholar] [CrossRef]
- Worlicek, M.C.; Wörner, M.L.; Craiovan, B.S.; Zeman, F.; Grifka, J.; Renkawitz, T.F.; Weber, M. Lesser Trochanter Size on Plain Anteroposterior Radiographs Correlates With Native Femoral Anteversion. J. Arthroplasty 2017, 32, 2892–2897. [Google Scholar] [CrossRef] [PubMed]
- Boddu, K.; Siebachmeyer, M.; Lakkol, S.; Rajayogeswaran, B.; Kavarthapu, V.; Li, P.L.S. Predicting the underestimation of the femoral offset in anteroposterior radiographs of the pelvis using “lesser trochanter index” A 3D CT derived simulated radiographic analysis. J. Arthroplasty 2014, 29, 1278–1284. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Hoyos, J.; Schröder, R.; Reddy, M.; Palmer, I.J.; Martin, H.D. Femoral neck anteversion and lesser trochanteric retroversion in patients with ischiofemoral impingement: A case-control magnetic resonance imaging study. Arthroscopy 2016, 32, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Dimovski, R.; Teitge, R.; Bolz, N.; Schafer, P.; Bobba, V.; Vaidya, R. Elimination of the femoral neck in measuring femoral version allows for less variance in interobserver reliability. Medicina 2021, 57, 1363. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Mean (SD) | Range | Intra-Observer ICC | Inter-Observer ICC |
|---|---|---|---|---|
| Lesser trochanter version | 38.54° ± 7.86° | 16.99° to 54.38° | 0.98 | 0.98 |
| Femoral anteversion | 11.84° ± 10.06° | −17.63° to 43.98° | 0.99 | 0.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohamed Thajudeen, M.Z.b.; Mahmood Merican, A.; Hashim, M.S.; Nordin, A. The Utility of Lesser Trochanter Version to Estimate Femoral Anteversion in Total Hip Arthroplasty: A Three-Dimensional Computed Tomography Study. Surg. Tech. Dev. 2022, 11, 54-61. https://doi.org/10.3390/std11020005
Mohamed Thajudeen MZb, Mahmood Merican A, Hashim MS, Nordin A. The Utility of Lesser Trochanter Version to Estimate Femoral Anteversion in Total Hip Arthroplasty: A Three-Dimensional Computed Tomography Study. Surgical Techniques Development. 2022; 11(2):54-61. https://doi.org/10.3390/std11020005
Chicago/Turabian StyleMohamed Thajudeen, Mohamed Zaim bin, Azhar Mahmood Merican, Muhammad Sufian Hashim, and Abid Nordin. 2022. "The Utility of Lesser Trochanter Version to Estimate Femoral Anteversion in Total Hip Arthroplasty: A Three-Dimensional Computed Tomography Study" Surgical Techniques Development 11, no. 2: 54-61. https://doi.org/10.3390/std11020005