

Survival in Patients with Relapsed-Refractory Multiple Myeloma: Indirect Comparison of Six New Treatments
 , , and
, , and
Abstract
:1. Introduction
2. Methods
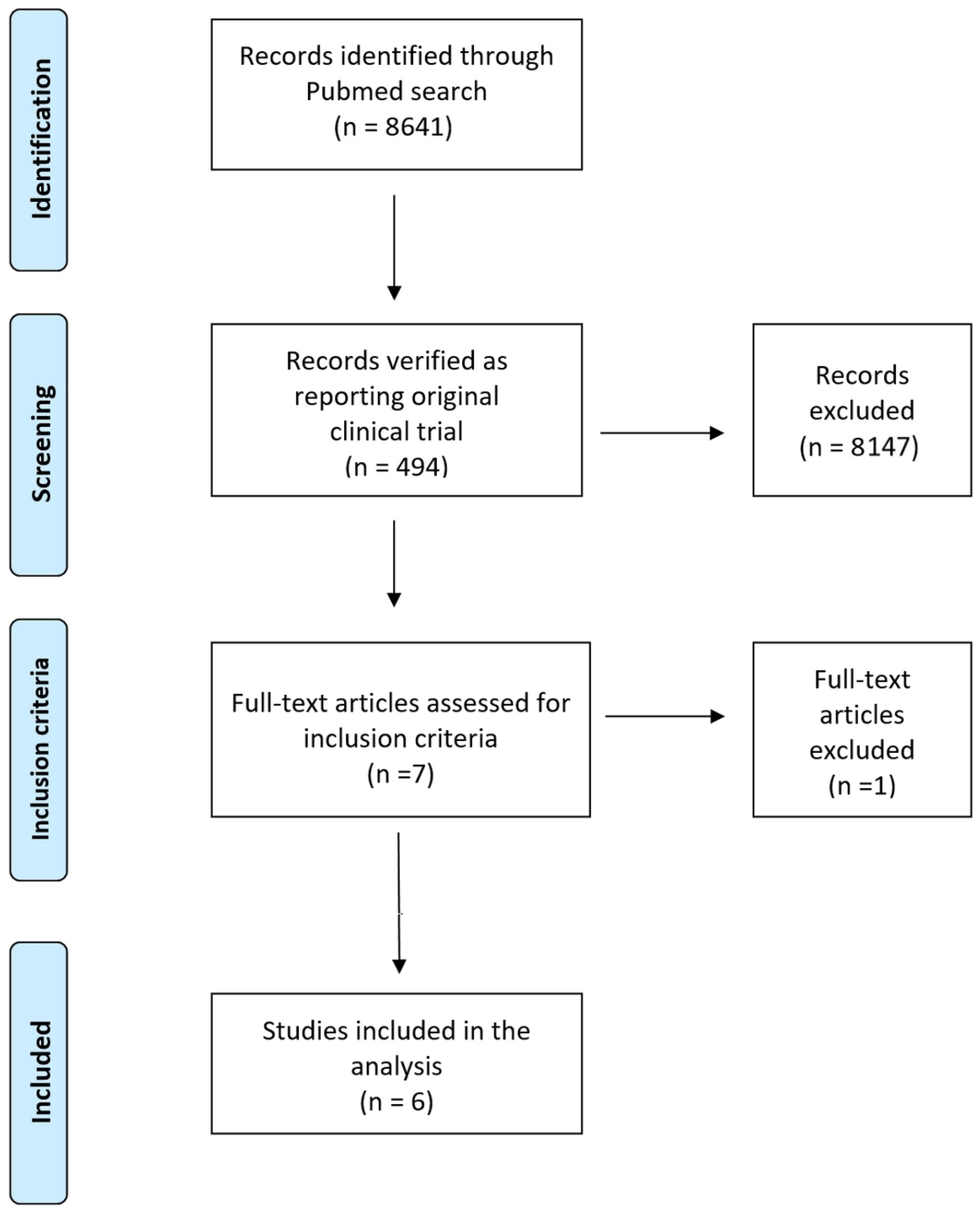
2.1. Literature Search and Selection of Pertinent Clinical Trials
2.2. Analysis of Kaplan-Meier Curves of Overall Survival
2.3. Generation of Treatment-Specific Kaplan-Meier Curves from Reconstructed Patient-Level Data and Statistical Comparison between Treatments
3. Results
3.1. Literature Search and Selection of Pertinent Clinical Trials
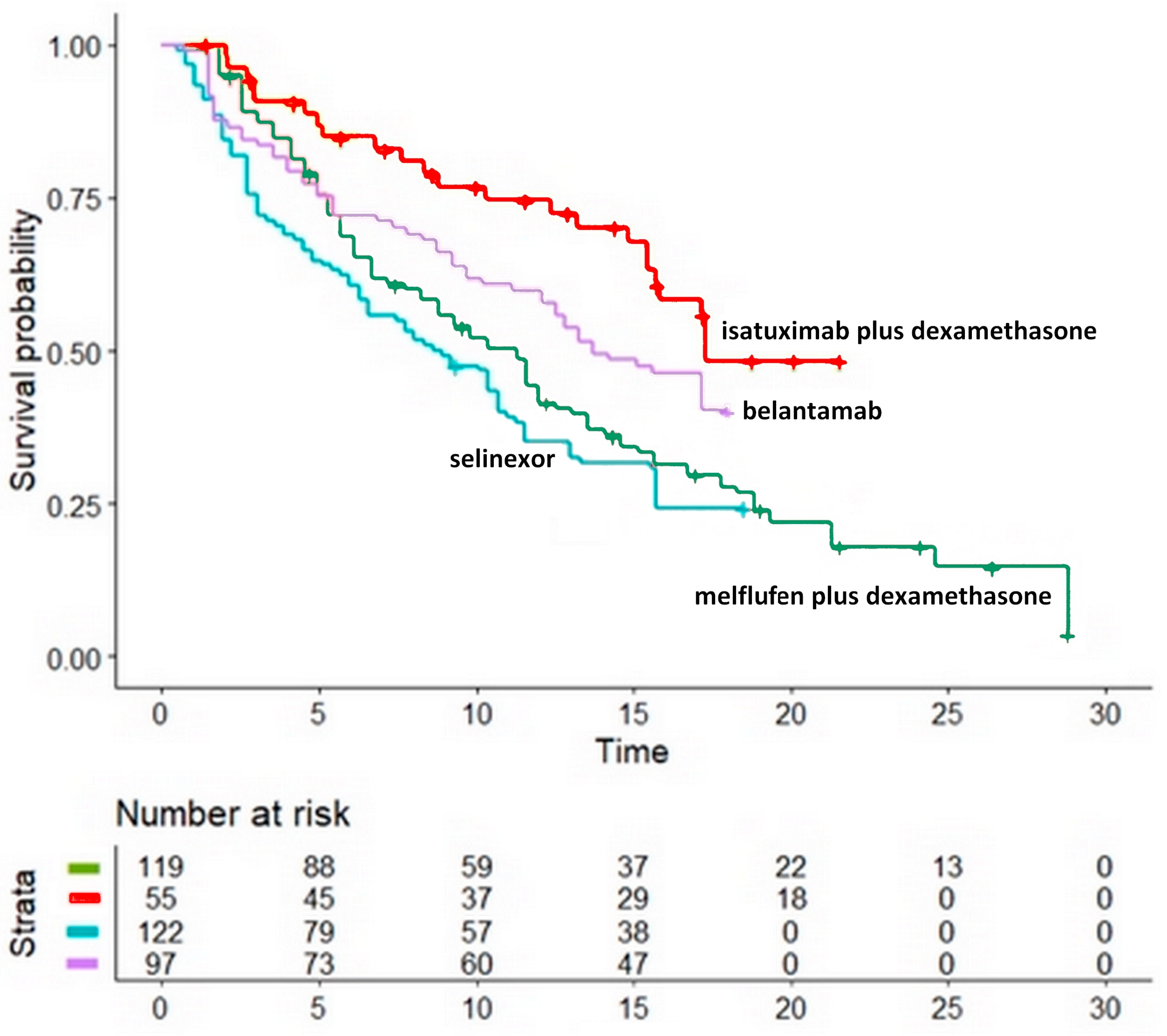
3.2. Comparison of Four Non-CAR-T Treatments
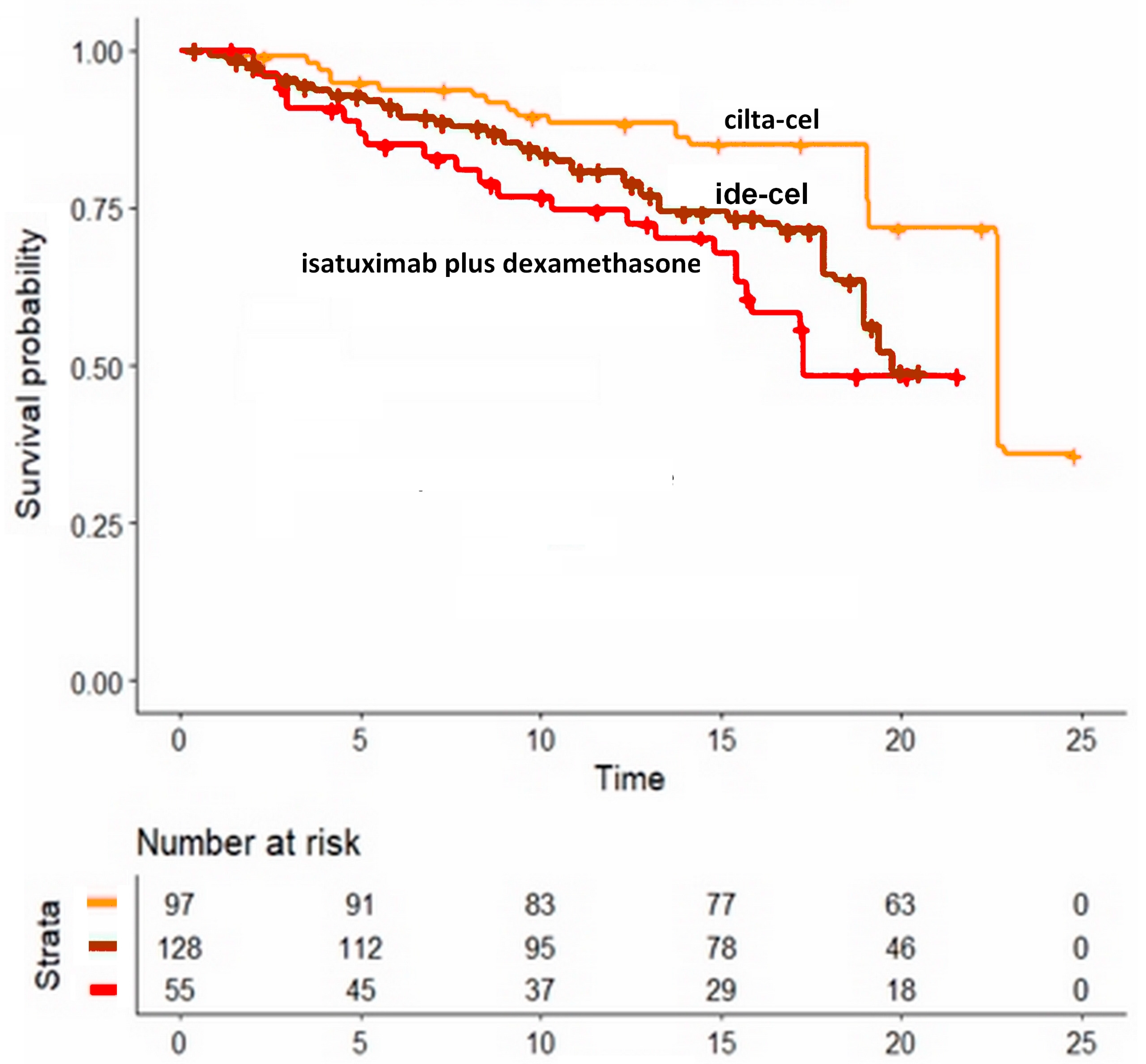
3.3. Comparison of Two CAR-T Products
4. Discussion
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gandhi, U.H.; Cornell, R.F.; Lakshman, A.; Gahvari, Z.J.; McGehee, E.; Jagosky, M.H.; Gupta, R.; Varnado, W.; Fiala, M.A.; Chhabra, S.; et al. Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia 2019, 33, 2266–2275. [Google Scholar] [CrossRef] [PubMed]
- Chari, A.; Vogl, D.T.; Gavriatopoulou, M.; Nooka, A.K.; Yee, A.J.; Huff, C.A.; Moreau, P.; Dingli, D.; Cole, C.; Lonial, S.; et al. Oral Selinexor-Dexamethasone for Triple-Class Refractory Multiple Myeloma. N. Engl. J. Med. 2019, 381, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Lonial, S.; Lee, H.C.; Badros, A.; Trudel, S.; Nooka, A.K.; Chari, A.; Abdallah, A.-O.; Callander, N.; Lendvai, N.; Sborov, D.; et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): A two-arm, randomised, open-label, phase 2 study. Lancet Oncol. 2020, 21, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, M.; Bringhen, S.; Anttila, P.; Capra, M.; Cavo, M.; Cole, C.; Gasparetto, C.; Hungria, V.; Jenner, M.; Vorobyev, V.; et al. Isatuximab as monotherapy and combined with dexamethasone in patients with relapsed/refractory multiple myeloma. Blood 2021, 137, 1154–1165. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Oriol, A.; Larocca, A.; Bladé, J.; Cavo, M.; Rodriguez-Otero, P.; Leleu, X.; Nadeem, O.; Hiemenz, J.W.; Hassoun, H.; et al. Melflufen and Dexamethasone in Heavily Pretreated Relapsed and Refractory Multiple Myeloma. J. Clin. Oncol. 2021, 39, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.-Y.; Zhao, W.-H.; Liu, J.; Chen, Y.-X.; Cao, X.-M.; Yang, Y.; Zhang, Y.-L.; Wang, F.-X.; Zhang, P.-Y.; Lei, B.; et al. Long-term follow-up of a phase 1, first-in-human open-label study of LCAR-B38M, a structurally differentiated chimeric antigen receptor T (CAR-T) cell therapy targeting B-cell maturation antigen (BCMA), in patients (pts) with relapsed/refractory multiple myeloma (RRMM). Blood 2019, 134 (Suppl. S1), 579. [Google Scholar]
- Berdeja, J.G.; Madduri, D.; Usmani, S.Z.; Jakubowiak, A.; Agha, M.; Cohen, A.D.; Stewart, A.K.; Hari, P.; Htut, M.; Lesokhin, A.; et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): A phase 1b/2 open-label study. Lancet 2021, 398, 314–324, Erratum in Lancet 2021, 398, 1216. [Google Scholar] [CrossRef] [PubMed]
- Munshi, N.C.; Anderson, L.D., Jr.; Shah, N.; Madduri, D.; Berdeja, J.; Lonial, S.; Raje, N.; Lin, Y.; Siegel, D.; Oriol, A.; et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2021, 384, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Na Liu, N.; Zhou, Y.; Lee, J.J. IPDfromKM: Reconstruct individual patient data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2021, 21, 111. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed]
- Ankit Rohatgi. Webplotdigitizer. Version 4.5; Pacifica, CA, USA. 2021. Available online: https://apps.automeris.io/wpd/ (accessed on 15 December 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014; Available online: http://www.R-project.org/ (accessed on 15 December 2022).
- Messori, A. Synthetizing Published Evidence on Survival by Reconstruction of Patient-Level Data and Generation of a Multi-Trial Kaplan-Meier Curve. Cureus 2021, 13, e19422. [Google Scholar] [CrossRef]
- Cancanelli, L.; Rivano, M.; Di Spazio, L.; Chiumente, M.; Mengato, D.; Messori, A. Efficacy of Immune Checkpoint Inhibitors in Patients with Mismatch Repair-Deficient or Microsatellite Instability-High Metastatic Colorectal Cancer: Analysis of Three Phase-II Trials. Cureus 2021, 13, e19893. [Google Scholar] [CrossRef] [PubMed]
- Messori, A.; Rivano, M.; Mengato, D.; Cancanelli, L.; Di Spazio, L.; Chiumente, M. A preliminary estimate of survival gain and cost-effectiveness of CAR-T in adult patients with acute lymphoblastic leukemia. Leuk Lymphoma. 2021, 63, 1261–1264. [Google Scholar] [CrossRef] [PubMed]
- Di Spazio, L.; Rivano, M.; Cancanelli, L.; Chiumente, M.; Mengato, D.; Messori, A. The Degree of Programmed Death-Ligand 1 (PD-L1) Positivity as a Determinant of Outcomes in Metastatic Triple-Negative Breast Cancer Treated With First-Line Immune Checkpoint Inhibitors. Cureus 2022, 14, e21065. [Google Scholar] [CrossRef] [PubMed]
- Usmani, S.Z.; Quach, H.; Mateos, M.V.; Landgren, O.; Leleu, X.; Siegel, D.; Weisel, K.; Gavriatopoulou, M.; Oriol, A.; Rabin, N.; et al. Carfilzomib, dexamethasone, and daratumumab versus carfilzomib and dexamethasone for patients with relapsed or refractory multiple myeloma (CANDOR): Updated outcomes from a randomised, multicentre, open-label, phase 3 study. Lancet Oncol. 2022, 23, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Messori, A.; Trippoli, S. Current treatments for inoperable mesothelioma: Indirect comparisons based on individual patient data reconstructed retrospectively from 4 trials. J. Chemother. 2022, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Trippoli, S.; Di Spazio, L.; Chiumente, M.; Messori, A. Radiofrequency Ablation, or Cryoballoon Ablation as First-Line Treatment for Paroxysmal Atrial Fibrillation: Interpreting Efficacy Through the Shiny Method. Cureus 2022, 14, e22645. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Wei, R.; Jiang, S.; Jiang, H.; Li, L.; Qiang, W.; He, H.; Shi, L.; Ma, Q.; Yu, K.; et al. CAR-T cell therapy targeting B cell maturation antigen is effective for relapsed/refractory multiple myeloma, even cases with poor performance status. Am. J. Hematol. 2022, 97, 933–941. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Trial | First Author, Year of Publication | Inclusion Criteria | Treatment Group (n/N) | Patients | Events |
|---|---|---|---|---|---|
| HORIZON | Richardson 2021 [5] | Patients had received at least two prior lines of therapy, including an immunomodulatory agent and proteasome inhibitor, and were refractory to pomalidomide and/or an anti-CD38 monoclonal antibody. RRMM was defined as disease that was nonresponsive while on primary or salvage therapy or progressed within 60 days of last therapy. | melflufen plus dexamethasone | 119 | 10 |
| NCT01084252 | Dimopolous 2020 [4] | Eligible patients had MM refractory to both an immunomodulatory agent (IMiD) and a proteasome inhibitor (PI), or had been treated with ≥3 prior lines of therapy, including an IMiD and a PI. Patients had to have received an alkylating agent, achieved at least a minimal response to a prior line of therapy, and could have received prior stem cell transplant. | isatuximab plus dexamethasone | 55 | 41 |
| STORM | Chiari 2019 [2] | Eligible patients had measurable myeloma according to International Myeloma Working Group, had previously received treatment with bortezomib, carfilzomib, lenalidomide, pomalidomide, daratumumab, glucocorticoids, and an alkylating agent, and had disease refractory to at least one immunomodulatory drug, one proteasome inhibitor, daratumumab, glucocorticoids, and their most recent regimen. | selinexor | 122 | 121 |
| DREAMM-2 | Lonial 2021 [3] | Patients with relapsed or refractory multiple myeloma with disease progression after three or more lines of therapy and who were refractory to immunomodulatory drugs and proteasome inhibitors, as well as refractory or intolerant (or both) to an anti-CD38 monoclonal antibody with an Eastern Cooperative Oncology Group performance status of 0–2, were recruited. | belantamab | 97 | 97 |
| CARTITUDE-1 | Berdeja 2021 [7] | Patients with a diagnosis of multiple myeloma who received three or more previous lines of therapy or were double-refractory to a proteasome inhibitor and an immunomodulatory drug and had received a proteasome inhibitor, immunomodulatory drug, and anti-CD38 antibody | ciltacabtagene autoleucel | 97 | 88 |
| KarMMa | Munshi 2021 [8] | Patients with disease after at least three previous regiments, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 antibody were enrolled | idecabtagene vicleucel | 128 | 101 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cancanelli, L.; Rivano, M.; Di Spazio, L.; Chiumente, M.; Mengato, D.; Messori, A. Survival in Patients with Relapsed-Refractory Multiple Myeloma: Indirect Comparison of Six New Treatments. Hematol. Rep. 2023, 15, 57-65. https://doi.org/10.3390/hematolrep15010006
Cancanelli L, Rivano M, Di Spazio L, Chiumente M, Mengato D, Messori A. Survival in Patients with Relapsed-Refractory Multiple Myeloma: Indirect Comparison of Six New Treatments. Hematology Reports. 2023; 15(1):57-65. https://doi.org/10.3390/hematolrep15010006
Chicago/Turabian StyleCancanelli, Luca, Melania Rivano, Lorenzo Di Spazio, Marco Chiumente, Daniele Mengato, and Andrea Messori. 2023. "Survival in Patients with Relapsed-Refractory Multiple Myeloma: Indirect Comparison of Six New Treatments" Hematology Reports 15, no. 1: 57-65. https://doi.org/10.3390/hematolrep15010006