
A Case Report of Ropeginterferon Alfa-2b for Polycythemia Vera during Pregnancy

Abstract
:1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Barbui, T.; Thiele, J.; Gisslinger, H.; Kvasnicka, H.M.; Vannucchi, A.M.; Guglielmelli, P.; Orazi, A.; Tefferi, A. The 2016 WHO classification and diagnostic criteria for myeloproliferative neoplasms: Document summary and in-depth discussion. Blood Cancer J. 2018, 8, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tefferi, A. Myeloproliferative neoplasms: A decade of discoveries and treatment advances. Am. J. Hematol. 2016, 91, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tefferi, A.; Pardanani, A. Myeloproliferative Neoplasms: A Contemporary Review. JAMA Oncol. 2015, 1, 97–105. [Google Scholar] [CrossRef]
- Maze, D.; Kazi, S.; Gupta, V.; Malinowski, A.K.; Fazelzad, R.; Shah, P.S.; Shehata, N. Association of Treatments for Myeloproliferative Neoplasms During Pregnancy With Birth Rates and Maternal Outcomes: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e1912666. [Google Scholar] [CrossRef]
- Greenfield, G.; McMullin, M.F.; Mills, K. Molecular pathogenesis of the myeloproliferative neoplasms. J. Hematol. Oncol. 2021, 14, 103. [Google Scholar] [CrossRef]
- Barbui, T.; Tefferi, A.; Vannucchi, A.M.; Passamonti, F.; Silver, R.T.; Hoffman, R.; Verstovsek, S.; Mesa, R.; Kiladjian, J.J.; Hehlmann, R.; et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: Revised management recommendations from European LeukemiaNet. Leukemia 2018, 32, 1057–1069. [Google Scholar] [CrossRef] [Green Version]
- Marchetti, M.; Vannucchi, A.M.; Griesshammer, M.; Harrison, C.; Koschmieder, S.; Gisslinger, H.; Álvarez-Larrán, A.; De Stefano, V.; Guglielmelli, P.; Palandri, F.; et al. Appropriate management of polycythaemia vera with cytoreductive drug therapy: European LeukemiaNet 2021 recommendations. Lancet Haematol. 2022, 9, e301–e311. [Google Scholar] [CrossRef]
- Belardelli, F.; Gresser, I. The neglected role of type I interferon in the T-cell response: Implications for its clinical use. Immunol. Today 1996, 17, 369–372. [Google Scholar] [CrossRef]
- Hasselbalch, H.C.; Holmstrom, M.O. Perspectives on interferon-alpha in the treatment of polycythemia vera and related myeloproliferative neoplasms: Minimal residual disease and cure? Semin. Immunopathol. 2019, 41, 5–19. [Google Scholar] [CrossRef] [Green Version]
- Vilcek, J. Fifty years of interferon research: Aiming at a moving target. Immunity 2006, 25, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Kiladjian, J.J.; Cassinat, B.; Chevret, S.; Turlure, P.; Cambier, N.; Roussel, M.; Bellucci, S.; Grandchamp, B.; Chomienne, C.; Fenaux, P. Pegylated interferon-alfa-2a induces complete hematologic and molecular responses with low toxicity in polycythemia vera. Blood 2008, 112, 3065–3072. [Google Scholar] [CrossRef]
- Kiladjian, J.J.; Cassinat, B.; Turlure, P.; Cambier, N.; Roussel, M.; Bellucci, S.; Menot, M.L.; Massonnet, G.; Dutel, J.L.; Ghomari, K.; et al. High molecular response rate of polycythemia vera patients treated with pegylated interferon alpha-2a. Blood 2006, 108, 2037–2040. [Google Scholar] [CrossRef]
- Masarova, L.; Patel, K.P.; Newberry, K.J.; Cortes, J.; Borthakur, G.; Konopleva, M.; Estrov, Z.; Kantarjian, H.; Verstovsek, S. Pegylated interferon alfa-2a in patients with essential thrombocythaemia or polycythaemia vera: A post-hoc, median 83 month follow-up of an open-label, phase 2 trial. Lancet Haematol. 2017, 4, e165–e175. [Google Scholar] [CrossRef] [Green Version]
- Quintas-Cardama, A.; Kantarjian, H.; Manshouri, T.; Luthra, R.; Estrov, Z.; Pierce, S.; Richie, M.A.; Borthakur, G.; Konopleva, M.; Cortes, J.; et al. Pegylated interferon alfa-2a yields high rates of hematologic and molecular response in patients with advanced essential thrombocythemia and polycythemia vera. J. Clin. Oncol. 2009, 27, 5418–5424. [Google Scholar] [CrossRef] [Green Version]
- Yazdani Brojeni, P.; Matok, I.; Garcia Bournissen, F.; Koren, G. A systematic review of the fetal safety of interferon alpha. Reprod. Toxicol. 2012, 33, 265–268. [Google Scholar] [CrossRef]
- Gisslinger, H.; Zagrijtschuk, O.; Buxhofer-Ausch, V.; Thaler, J.; Schloegl, E.; Gastl, G.A.; Wolf, D.; Kralovics, R.; Gisslinger, B.; Strecker, K.; et al. Ropeginterferon alfa-2b, a novel IFNalpha-2b, induces high response rates with low toxicity in patients with polycythemia vera. Blood 2015, 126, 1762–1769. [Google Scholar] [CrossRef]
- Gisslinger, H.; Klade, C.; Georgiev, P.; Krochmalczyk, D.; Gercheva-Kyuchukova, L.; Egyed, M.; Rossiev, V.; Dulicek, P.; Illes, A.; Pylypenko, H.; et al. Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): A randomised, non-inferiority, phase 3 trial and its extension study. Lancet Haematol. 2020, 7, e196–e208. [Google Scholar] [CrossRef]
- Tefferi, A.; Barbui, T. Polycythemia vera and essential thrombocythemia: 2017 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2017, 92, 94–108. [Google Scholar] [CrossRef]
- Huang, C.E.; Wu, Y.Y.; Hsu, C.C.; Chen, Y.J.; Tsou, H.Y.; Li, C.P.; Lai, Y.H.; Lu, C.H.; Chen, P.T.; Chen, C.C. Real-world experience with Ropeginterferon-alpha 2b (Besremi) in Philadelphia-negative myeloproliferative neoplasms. J. Formos Med. Assoc. 2021, 120, 863–873. [Google Scholar] [CrossRef]
- Hultcrantz, M.; Ravn Landtblom, A.; Andreasson, B.; Samuelsson, J.; Dickman, P.W.; Kristinsson, S.Y.; Bjorkholm, M.; Andersson, T.M. Incidence of myeloproliferative neoplasms - trends by subgroup and age in a population-based study in Sweden. J. Intern. Med. 2020, 287, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.; Lee, J.O.; Bang, S.M. Incidence, Survival and Prevalence Statistics of Classical Myeloproliferative Neoplasm in Korea. J. Korean Med. Sci. 2016, 31, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.S.; Hong, J.; Hwang, S.M.; Lee, J.H.; Ma, Y.; Kim, S.A.; Lee, J.Y.; Lee, J.O.; Bang, S.M. Evaluation of the need for cytoreduction and its potential carcinogenicity in children and young adults with myeloproliferative neoplasms. Ann. Hematol. 2021, 100, 2567–2574. [Google Scholar] [CrossRef] [PubMed]
- Lavi, N.; Brenner, B.; Avivi, I. Management of pregnant women with myeloproliferative neoplasms. Thromb. Res. 2013, 131 (Suppl. 1), S11–S13. [Google Scholar] [CrossRef]
- Alimam, S.; Bewley, S.; Chappell, L.C.; Knight, M.; Seed, P.; Gray, G.; Harrison, C.; Robinson, S. Pregnancy outcomes in myeloproliferative neoplasms: UK prospective cohort study. Br. J. Haematol. 2016, 175, 31–36. [Google Scholar] [CrossRef]
- Robinson, S.E.; Harrison, C.N. How we manage Philadelphia-negative myeloproliferative neoplasms in pregnancy. Br. J. Haematol. 2020, 189, 625–634. [Google Scholar] [CrossRef]
- Tefferi, A.; Barbui, T. Polycythemia vera and essential thrombocythemia: 2021 update on diagnosis, risk-stratification and management. Am. J. Hematol. 2020, 95, 1599–1613. [Google Scholar] [CrossRef]
- Barbui, T.; Barosi, G.; Grossi, A.; Gugliotta, L.; Liberato, L.N.; Marchetti, M.; Mazzucconi, M.G.; Rodeghiero, F.; Tura, S. Practice guidelines for the therapy of essential thrombocythemia. A statement from the Italian Society of Hematology, the Italian Society of Experimental Hematology and the Italian Group for Bone Marrow Transplantation. Haematologica 2004, 89, 215–232. [Google Scholar]
- Gangat, N.; Tefferi, A. Myeloproliferative neoplasms and pregnancy: Overview and practice recommendations. Am. J. Hematol. 2021, 96, 354–366. [Google Scholar] [CrossRef]
- How, J.; Leiva, O.; Bogue, T.; Fell, G.G.; Bustoros, M.W.; Connell, N.T.; Connors, J.M.; Ghobrial, I.M.; Kuter, D.J.; Mullally, A.; et al. Pregnancy outcomes, risk factors, and cell count trends in pregnant women with essential thrombocythemia. Leuk. Res. 2020, 98, 106459. [Google Scholar] [CrossRef]
- Landtblom, A.R.; Andersson, T.M.; Johansson, A.L.V.; Wendel, S.B.; Lundberg, F.E.; Samuelsson, J.; Bjorkholm, M.; Hultcrantz, M. Pregnancy and childbirth outcomes in women with myeloproliferative neoplasms-a nationwide population-based study of 342 pregnancies in Sweden. Leukemia 2022, 36, 2461–2467. [Google Scholar] [CrossRef]
- Lishner, M.; Avivi, I.; Apperley, J.F.; Dierickx, D.; Evens, A.M.; Fumagalli, M.; Nulman, I.; Oduncu, F.S.; Peccatori, F.A.; Robinson, S.; et al. Hematologic Malignancies in Pregnancy: Management Guidelines From an International Consensus Meeting. J. Clin. Oncol. 2016, 34, 501–508. [Google Scholar] [CrossRef]
- Barbui, T.; Barosi, G.; Birgegard, G.; Cervantes, F.; Finazzi, G.; Griesshammer, M.; Harrison, C.; Hasselbalch, H.C.; Hehlmann, R.; Hoffman, R.; et al. Philadelphia-negative classical myeloproliferative neoplasms: Critical concepts and management recommendations from European LeukemiaNet. J. Clin. Oncol. 2011, 29, 761–770. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, I.; Woodley, C.; Durgam, G.; Curto-Garcia, N.; Sullivan, J.O.; Robinson, S.E.; Ali, S.; McLornan, D.; Harrison, C. A case of polycythaemia vera treated with ropeginterferon-2b during pregnancy. Br. J. Haematol. 2021, 193, 118–119. [Google Scholar]
- Shechter-Maor, G.; Sadeh-Mestechkin, D.; Ganor Paz, Y.; Sukenik Halevy, R.; Markovitch, O.; Biron-Shental, T. Does parity affect pregnancy outcomes in the elderly gravida? Arch. Gynecol. Obstet. 2020, 301, 85–91. [Google Scholar] [CrossRef]
- Reese, J.A.; Peck, J.D.; Deschamps, D.R.; McIntosh, J.J.; Knudtson, E.J.; Terrell, D.R.; Vesely, S.K.; George, J.N. Platelet Counts during Pregnancy. N. Engl. J. Med. 2018, 379, 32–43. [Google Scholar] [CrossRef]
- Bertozzi, I.; Rumi, E.; Cavalloni, C.; Cazzola, M.; Fabris, F.; Randi, M.L. Pregnancy outcome and management of 25 pregnancies in women with polycythemia vera. Am. J. Hematol. 2018, 93, E234–E235. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Date | Hct (%) | PLT (×109/L) | Hb (g/dL) | WBC (×109/L) | ANC (×109/L) | Treatment Status |
|---|---|---|---|---|---|---|
| 18 December 2017 | 55.6 | 821 | 18.2 | 13.87 | At the time of diagnosis | |
| December 2020~November 2021 (Mean ± SD) | 46.3 ± 2.2 | 835 ± 130 | 13.9 ± 0.7 | 18.65 ± 0.58 | 13.88 ± 0.71 | Phlebotomy and HU, ANA |
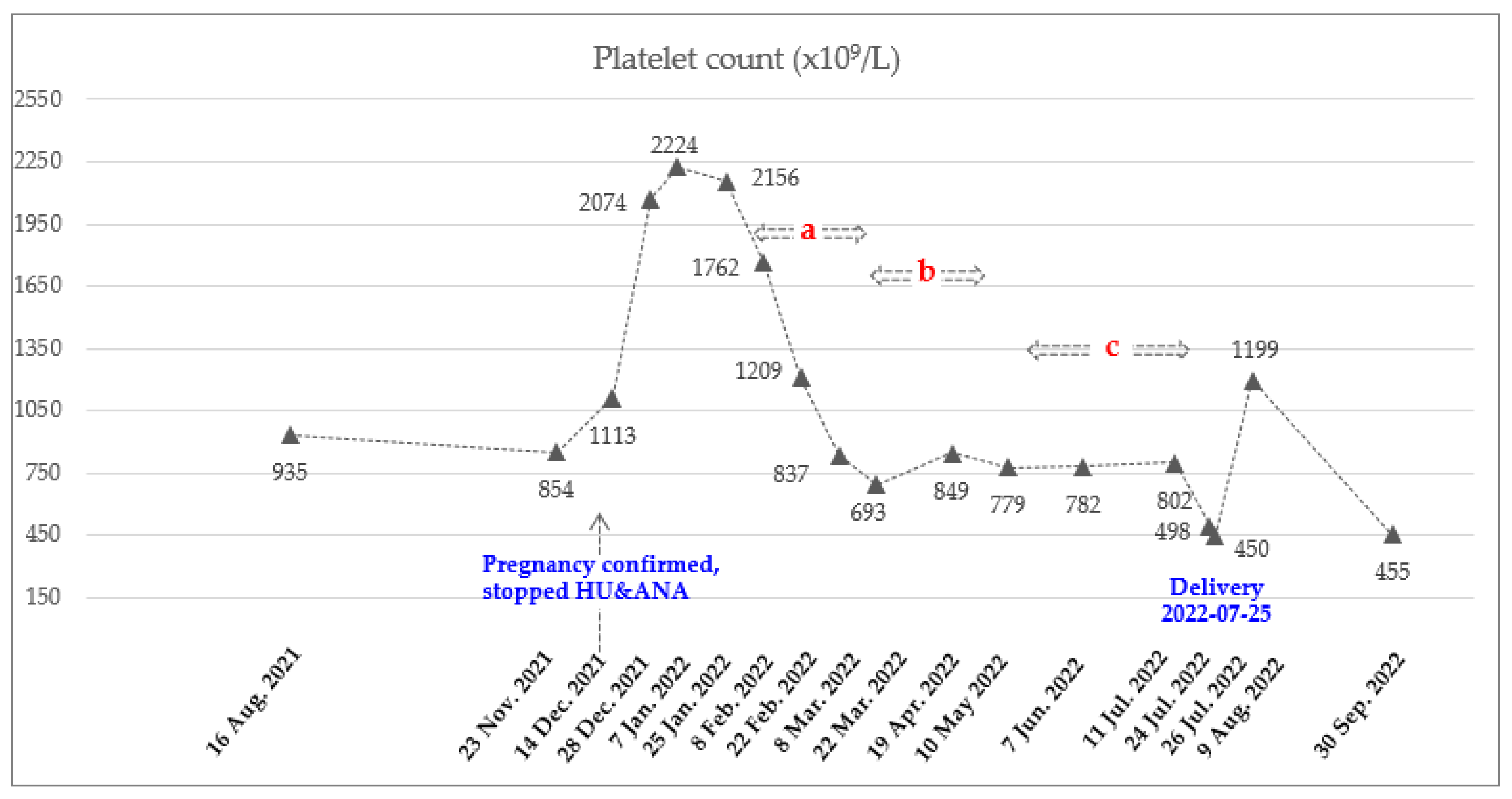
| 14 December 2021 | 44.8 | 1113 | 13.8 | 21.93 | 17.98 | Pregnancy confirmed, stopped HU and ANA |
| 28 December 2021~25 January 2022 (Mean ± SD) | 47.8 ± 0.5 | 2151 ± 75 | 14.8 ± 0.5 | 28.24 ± 6.73 | 23.05 ± 6.62 | |
| 8 February 2022 | 48.2 | 1762 | 14.9 | 22.06 | 18.53 | Ropeginterferon alfa-2b 250 mcg |
| 22 February 2022 | 51.1 | 1209 | 15.9 | 14.23 | 10.67 | Ropeginterferon alfa-2b 350 mcg |
| 8 March 2022 | 50.8 | 837 | 15.8 | 10.17 | 7.42 | Ropeginterferon alfa-2b 500 mcg |
| 22 March 2022 | 47.9 | 693 | 15.2 | 10.51 | 8.09 | Ropeginterferon alfa-2b 500 mcg every 3 weeks (2 times) |
| 19 April 2022 | 49.7 | 849 | 15.9 | 14.2 | 11.79 | |
| 10 May 2022 ~11 July 2022 (Mean ± SD) | 45.3 ± 2.8 | 788 ± 13 | 14.7 ± 0.9 | 16.46 ± 2.83 | 13.54 ± 2.73 | Ropeginterferon alfa 2b 500 mcg every 4 weeks (3 times) Final date of injection 11 July 2022 |
| 24 July 2022 | 44.5 | 498 | 14.3 | 15.93 | 12.82 | LMWH (11 July 2022~23 July 2022) |
| 26 July 2022 | 42.8 | 450 | 14.1 | 14.46 | 11.96 | Delivery (25 July 2022) |
| 9 August 2022 | 48.6 | 1199 | 15.9 | 21.53 | 18.09 | Phlebotomy and HU, ANA |
| 30 September 2022 | 54.1 | 455 | 17.2 | 15.68 | 12.54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bang, S.-Y.; Lee, S.-E. A Case Report of Ropeginterferon Alfa-2b for Polycythemia Vera during Pregnancy. Hematol. Rep. 2023, 15, 172-179. https://doi.org/10.3390/hematolrep15010018
Bang S-Y, Lee S-E. A Case Report of Ropeginterferon Alfa-2b for Polycythemia Vera during Pregnancy. Hematology Reports. 2023; 15(1):172-179. https://doi.org/10.3390/hematolrep15010018
Chicago/Turabian StyleBang, Su-Yeon, and Sung-Eun Lee. 2023. "A Case Report of Ropeginterferon Alfa-2b for Polycythemia Vera during Pregnancy" Hematology Reports 15, no. 1: 172-179. https://doi.org/10.3390/hematolrep15010018