

Frail Multiple Myeloma Patients Deserve More Than Just a Score

Abstract
:1. Introduction
2. The Current Use of Frailty Scores in Clinical Practice
3. The Future Potential of Frailty Scores
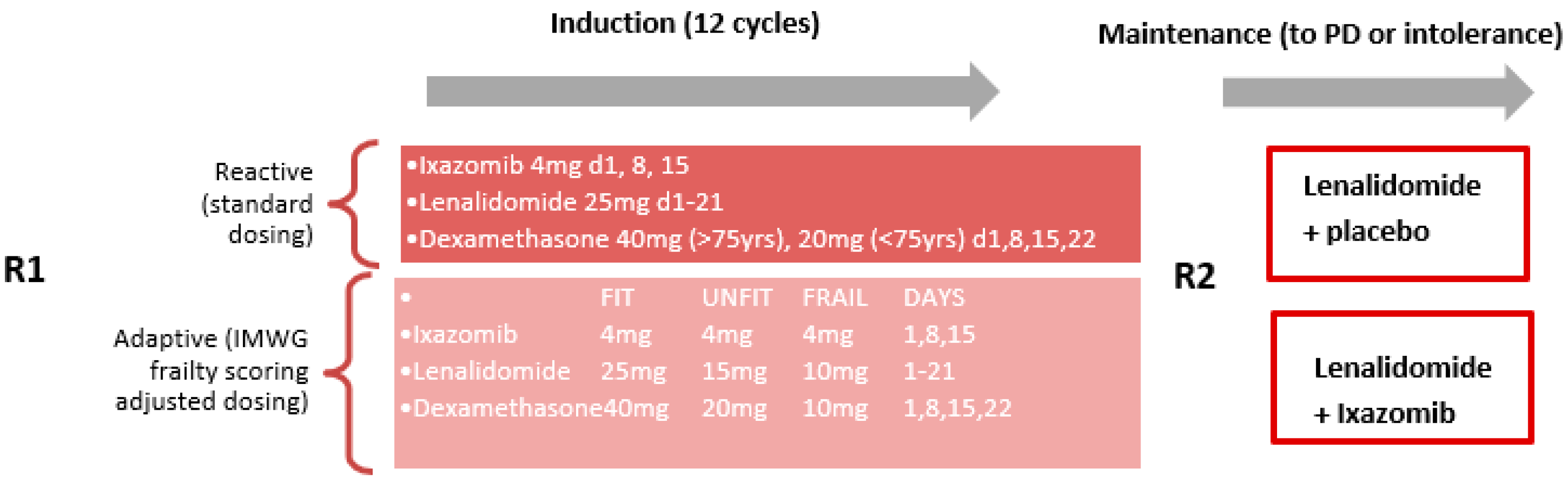
3.1. In the Trial Setting
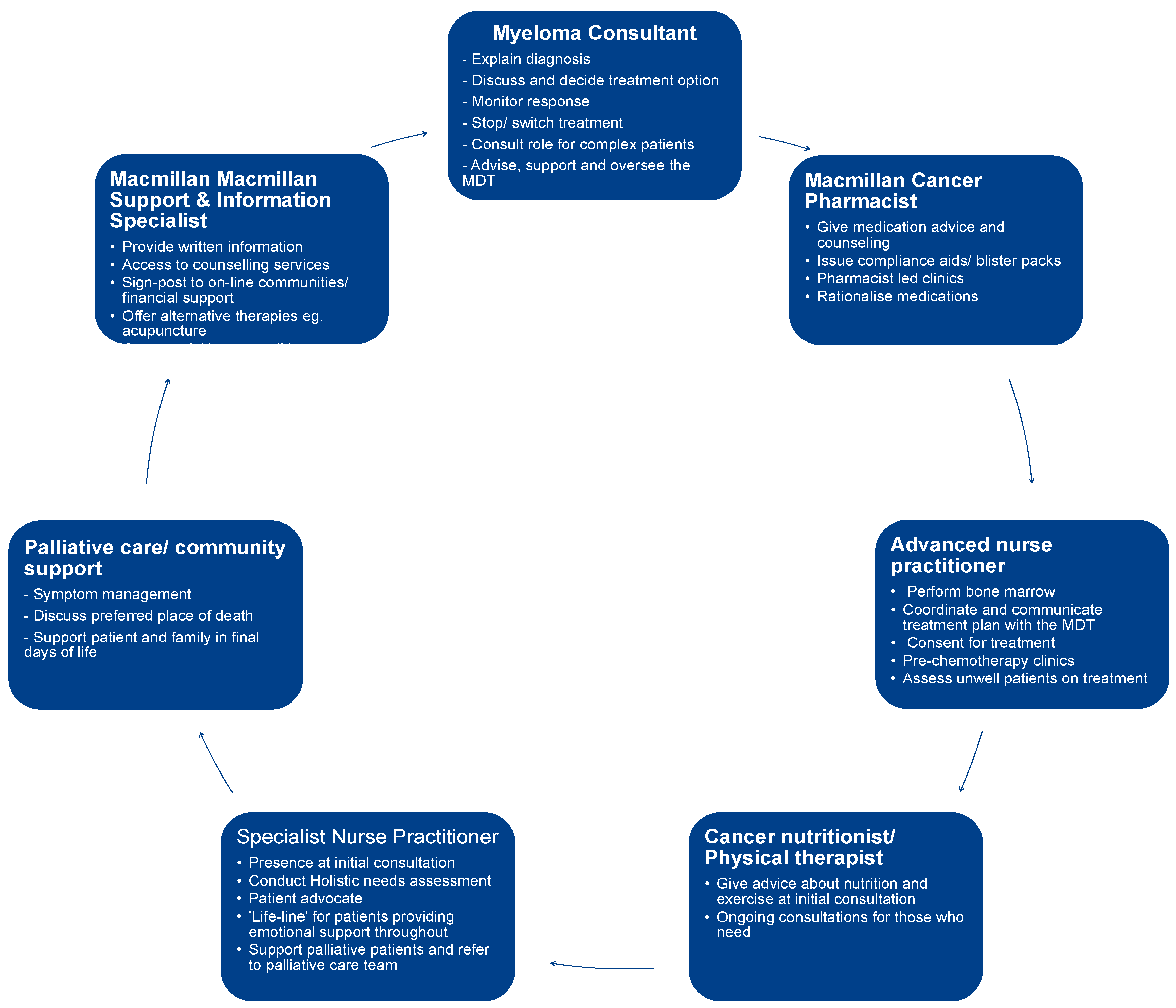
3.2. In the Clinic Setting
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Myelom UK. What Is Myeloma? 2022. Available online: https://www.myeloma.org.uk/understanding-myeloma/what-is-myeloma/ (accessed on 19 February 2022).
- Dede, R.J.; Pruemer, J.M. Comparing venous thromboembolism prophylactic strategies for ambulatory multiple myeloma patients on immunomodulatory drug therapy. J. Oncol. Pharm. Pract. 2016, 22, 248–255. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Prevalence | Background Information | Multiple Myeloma | CKS | NICE. 2021. Available online: https://cks.nice.org.uk/topics/multiple-myeloma/background-information/prevalence/ (accessed on 23 October 2021).
- Belotti, A.; Ribolla, R.; Cancelli, V.; Crippa, C.; Bianchetti, N.; Ferrari, S.; Bottelli, C.; Cattaneo, C.; Tucci, A.; De La Fuente Barrigon, C.; et al. Transplant eligibility in elderly multiple myeloma patients: Prospective external validation of the international myeloma working group frailty score and comparison with clinical judgment and other comorbidity scores in unselected patients aged 65–75 years. Am. J. Hematol. 2020, 95, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q. The frailty syndrome: Definition and natural history. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Bringhen, S.; Mateos, M.; Larocca, A.; Facon, T.; Kumar, S.K.; Offidani, M.; McCarthy, P.; Evangelista, A.; Lonial, S.; et al. Geriatric assessment predicts survival and toxicities in elderly myeloma patients: An International Myeloma Working Group report. Blood 2015, 125, 2068–2074. [Google Scholar] [CrossRef] [PubMed]
- Cook, G.; Royle, K.; Pawlyn, C.; Hockaday, A.; Shah, V.; Kaiser, M.F.; Brown, S.R.; Gregory, W.M.; Child, J.A.; Davies, F.E.; et al. A clinical prediction model for outcome and therapy delivery in transplant-ineligible patients with myeloma (UK Myeloma Research Alliance Risk Profile): A development and validation study. Lancet Haematol. 2019, 6, e154–e166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redder, L.; Klausen, T.W.; Vangsted, A.J.; Gregersen, H.; Andersen, N.F.; Pedersen, R.S.; Szabo, A.G.; Frederiksen, M.; Frølund, U.C.; Helleberg, C.; et al. Validation of the UK myeloma research alliance risk profile, a new clinical prediction model for outcome in patients with newly diagnosed multiple myeloma not eligible for autologous stem cell transplantation; a population-based study from the Danish national multiple myeloma registry. Br. J. Haematol. 2021, 193, 119–124. [Google Scholar] [PubMed]
- Cook, G.; Larocca, A.; Facon, T.; Zweegman, S.; Engelhardt, M. Defining the vulnerable patient with myeloma—A frailty position paper of the European Myeloma Network. Leukemia 2020, 34, 2285–2294. [Google Scholar] [CrossRef] [PubMed]
- University Medical Center Freiburg. R-MCI: Myeloma Comorbidity Index for Myeloma Patients. 2017. Available online: https://www.myelomacomorbidityindex.org/en_calc.html (accessed on 28 December 2021).
- Diamond, E.; Lahoud, O.B.; Landau, H. Managing multiple myeloma in elderly patients. Leuk. Lymphoma 2018, 59, 1300–1311. [Google Scholar] [CrossRef] [PubMed]
- Farcet, A.; de Decker, L.; Pauly, V.; Rousseau, F.; Bergman, H.; Molines, C.; Retornaz, F. Frailty Markers and Treatment Decisions in Patients Seen in Oncogeriatric Clinics: Results from the ASRO Pilot Study. PLoS ONE 2016, 11, e0149732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zweegman, S.; Engelhardt, M.; Larocca, A. Elderly patients with multiple myeloma: Towards a frailty approach? Curr. Opin. Oncol. 2017, 29, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Facon, T.; Dimopoulos, M.A.; Meuleman, N.; Belch, A.; Mohty, M.; Chen, W.; Kim, K.; Zamagni, E.; Rodriguez-Otero, P.; Renwick, W.; et al. A simplified frailty scale predicts outcomes in transplant-ineligible patients with newly diagnosed multiple myeloma treated in the FIRST (MM-020) trial. Leukemia 2020, 34, 224–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaweme, N.M.; Changwe, G.J.; Zhou, F. Approaches and Challenges in the Management of Multiple Myeloma in the Very Old: Future Treatment Prospects. Front. Med. 2021, 8, 612696. [Google Scholar] [CrossRef] [PubMed]
- Larocca, A.; Palumbo, A. How I treat fragile myeloma patients. Blood 2015, 126, 2179–2185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, G.; Pawlyn, C.; Royle, K.-L.; Coulson, A.B.; Bird, J.; Bowcock, S.; Jenner, M.; Kishore, B.; Parrish, C.; Rabin, N.; et al. Fitness, a UK Myeloma Research Alliance (UK-MRA) Frailty-Adjusted Therapy Study, Supports the Feasibility of Recruiting Frail Newly Diagnosed Myeloma Patients to Large Clinical Trials. Blood 2021, 138 (Suppl. S1), 81. [Google Scholar] [CrossRef]
- Sharpley, F.A.; Miller, H.; Spencer, R.; Bradwell, D.; Parkinson, J.; Ibbotson, Y.; Jowitt, S. Is It Time for a More Holistic Approach to the Treatment of Multiple Myeloma? Hemato 2021, 2, 40. [Google Scholar] [CrossRef]
- Facon, T.; Dimopoulos, M.A.; Dispenzieri, A.; Catalano, J.V.; Belch, A.; Cavo, M.; Pinto, A.; Weisel, K.; Ludwig, H.; Bahlis, N.J.; et al. Final analysis of survival outcomes in the phase 3 FIRST trial of up-front treatment for multiple myeloma. Blood 2018, 131, 301–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DuMontier, C.; Fillmore, N.R.; Yildirim, C.; Cheng, D.; La, J.; Orkaby, A.R.; Charest, B.; Cirstea, D.; Yellapragada, S.; Gaziano, J.M.; et al. Contemporary Analysis of Electronic Frailty Measurement in Older Adults with Multiple Myeloma Treated in the National US Veterans Affairs Healthcare System. Cancers 2021, 13, 3053. [Google Scholar] [CrossRef] [PubMed]
- Möller, M.D.; Gengenbach, L.; Graziani, G.; Greil, C.; Wäsch, R.; Engelhardt, M. Geriatric assessments and frailty scores in multiple myeloma patients: A needed tool for individualized treatment? Curr. Opin. Oncol. 2021, 33, 648–657. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Frailty Score | Biological Components | Functionality Tests | Comparison with IMWG | Populations Tested | Prospective Evaluation? |
|---|---|---|---|---|---|
| IMWG | Age, CCI | ADL, IADL | - | CT | No |
| R-MCI | eGFR, PFTs, Frailty, Age +/− CG | PS (Karnofsky) | Yes | CT, RW | Yes |
| UK MRA MRP | R-ISS, CRP, Age | PS (WHO) | No | CT, RW | No |
| Mayo Risk Score | NT-proBNP, Age | PS (WHO) | No | RW | No |
| Ancona Vulnerability Score | CCI | PS (WHO) | No | RW | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, H.L.; Sharpley, F.A. Frail Multiple Myeloma Patients Deserve More Than Just a Score. Hematol. Rep. 2023, 15, 151-156. https://doi.org/10.3390/hematolrep15010015
Miller HL, Sharpley FA. Frail Multiple Myeloma Patients Deserve More Than Just a Score. Hematology Reports. 2023; 15(1):151-156. https://doi.org/10.3390/hematolrep15010015
Chicago/Turabian StyleMiller, Hannah Louise, and Faye Amelia Sharpley. 2023. "Frail Multiple Myeloma Patients Deserve More Than Just a Score" Hematology Reports 15, no. 1: 151-156. https://doi.org/10.3390/hematolrep15010015