
Efficacy and Safety of Enteral Human Recombinant Insulin to Reduce the Time to Full Enteral Feeding in Preterm Infants: A Meta-Analytical Study
 , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Quinn, J.-A.; Munoz, F.M.; Gonik, B.; Frau, L.; Cutland, C.; Mallett-Moore, T.; Kissou, A.; Wittke, F.; Das, M.; Nunes, T.; et al. Preterm Birth: Case Definition & Guidelines for Data Collection, Analysis, and Presentation of Immunisation Safety Data. Vaccine 2016, 34, 6047–6056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Preterm Birth Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 19 February 2023).
- Walani, S.R. Global Burden of Preterm Birth. Int. J. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Berseth, C.L.; Nordyke, C. Enteral Nutrients Promote Postnatal Maturation of Intestinal Motor Activity in Preterm Infants. Am. J. Physiol. 1993, 264, G1046–G1051. [Google Scholar] [CrossRef] [PubMed]
- Fanaro, S. Feeding Intolerance in the Preterm Infant. Early Hum. Dev. 2013, 89 (Suppl. S2), S13–S20. [Google Scholar] [CrossRef] [PubMed]
- El Manouni El Hassani, S.; Berkhout, D.J.C.; Niemarkt, H.J.; Mann, S.; de Boode, W.P.; Cossey, V.; Hulzebos, C.V.; van Kaam, A.H.; Kramer, B.W.; van Lingen, R.A.; et al. Risk Factors for Late-Onset Sepsis in Preterm Infants: A Multicenter Case-Control Study. Neonatology 2019, 116, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.; Jefferies, A.L.; Yoon, E.W.; Lee, S.K.; Shah, P.S. Risk Factors and Outcomes of Late-Onset Bacterial Sepsis in Preterm Neonates Born at < 32 Weeks’ Gestation. Am. J. Perinatol. 2015, 32, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.A. Intestinal Failure-Associated Liver Disease: What Do We Know Today? Gastroenterology 2006, 130, S70–S77. [Google Scholar] [CrossRef] [PubMed]
- Koldovský, O.; Thornburg, W. Hormones in Milk. J. Pediatr. Gastroenterol. Nutr. 1987, 6, 172–196. [Google Scholar] [PubMed]
- Shehadeh, N.; Gelertner, L.; Blazer, S.; Perlman, R.; Solovachik, L.; Etzioni, A. Importance of Insulin Content in Infant Diet: Suggestion for a New Infant Formula. Acta Paediatr. 2001, 90, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Mank, E.; van Toledo, L.; Heijboer, A.C.; van den Akker, C.H.P.; van Goudoever, J.B. Insulin Concentration in Human Milk in the First Ten Days Postpartum: Course and Associated Factors. J. Pediatr. Gastroenterol. Nutr. 2021, 73, e115–e119. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Shehadeh, N.; Simmonds, A.; Zangen, S.; Riskin, A.; Shamir, R. Efficacy and Safety of Enteral Recombinant Human Insulin for Reduction of Time-to-Full Enteral Feeding in Preterm Infants: A Randomized, Double-Blind, Placebo-Controlled Trial. Isr. Med. Assoc. J. 2021, 23, 563–568. [Google Scholar] [PubMed]
- Shamir, R.; Shehadeh, N. Insulin in Human Milk and the Use of Hormones in Infant Formulas. In Nestlé Nutrition Institute Workshop Series; Karger Publishers: Basel, Switzerland, 2013; Volume 77, pp. 57–64. ISBN 1664-2147. [Google Scholar]
- Shulman, R.J. Effect of Enteral Administration of Insulin on Intestinal Development and Feeding Tolerance in Preterm Infants: A Pilot Study. Arch. Dis. Child. Fetal Neonatal Ed. 2002, 86, F131–F133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mank, E.; Sáenz de Pipaón, M.; Lapillonne, A.; Carnielli, V.P.; Senterre, T.; Shamir, R.; van Toledo, L.; van Goudoever, J.B.; van Goudoever, J.B.; Mank, E.; et al. Efficacy and Safety of Enteral Recombinant Human Insulin in Preterm Infants: A Randomized Clinical Trial. JAMA Pediatr. 2022, 176, 452. [Google Scholar] [CrossRef] [PubMed]
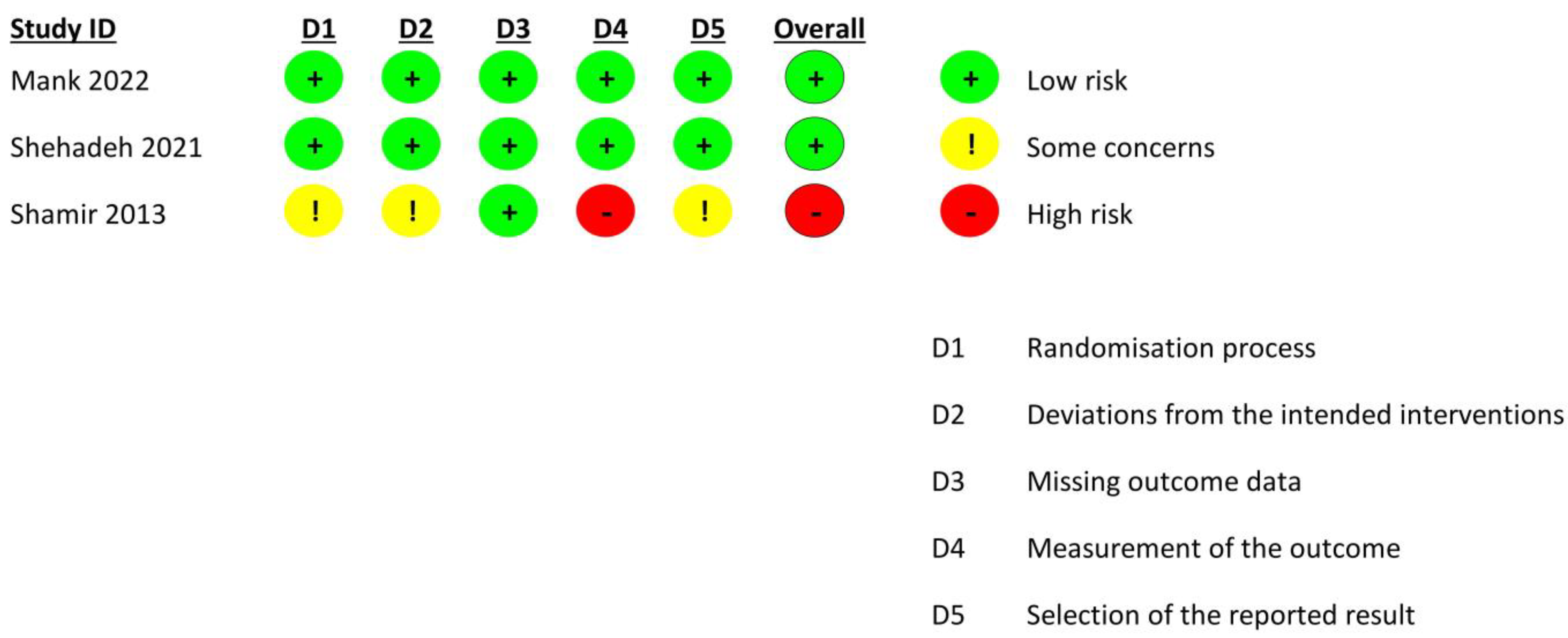
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHLBI Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 19 February 2023).
- McGuire, W.; Henderson, G.; Fowlie, P.W. Feeding the Preterm Infant. BMJ 2004, 329, 1227–1230. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year, Country | Main Inclusion Criteria | Number of Randomized Neonates (n) | Initiation and Duration of the Study Intervention | Mean Gestational Age (SD)/Median (IQR) Weeks | Mean Birth Weight (SD), Median (IQR) g | Primary Outcome(s) | Secondary Outcome(s) | Other Reported Outcome(s) |
|---|---|---|---|---|---|---|---|---|
| Shulman RJ, 2002, USA [15] | 26–30 weeks of gestation, appropriate size for gestational age; postnatal age < 96 h | Insulin Group = 8, Control Group = 80 | Insulin administration was initiated on the 4th day of life and continued until the 28th day of life. Intestinal lactase activity in both groups of neonates was determined at 28 days of age. | Insulin Group 27.8 (2.5), Control Group 27.8 (1.2) | Insulin Group 973 (310), Control Group 1042 (172) | Intestinal lactase activity Mean number of neonates with gastric residuals > 2 mL/kg | - | - |
| Shamir R, 2013, Israel [14] | Preterm Infants | 8 neonates | Day 1–28 after birth | 27.8 (2.5) | 800 and above | Weight gain and time to achieve FEF | - | - |
| Shehadeh N, 2021, Israel [13] | Preterm Infants at 26–33 weeks of gestation, birth wt. ≥ 750 g, postnatal age ≤ 7 days | 33 preterm infants | Within 24 h of enrollment for 28 days or until the time of discharge, whichever was sooner | Placebo 30.6 ± 2.1, Insulin 30.9 ± 1.5 | Placebo 1446.8 ± 364.8, Insulin 1470.7 ± 299.7 | Time required to achieve FEF | Severe adverse effects | Weight gain in the first 28 days after birth |
| Mank E, 2022, Netherlands [16] | 26–32 weeks of gestation, weight of 500 g or more, able to tolerate enteral feeding | 303 neonates | Within 5 days post-partum (up to 120 h). In the neonates exclusively fed with mother’s milk, treatment was not initiated until 72 h post-partum. The standard duration of the intervention was 28 days | Low-dose insulin 29.1 (28.1–30.4), High-dose insulin 29.0 (27.7–30.5), Placebo 28.8 (27.6–30.4) | Low-dose group 1200 (976–1425), High-dose group 1250 (1020–1445), Placebo group 1208 (1021–1430) | Time to achieve full enteral feeding (FEF) defined as an enteral intake of 150 mL/kg per day or more for 3 consecutive days. | The proportion of neonates who achieved FEF in the first 6, 8, and 10 days of intervention | Assessment of severe adverse Effects after the administration of different doses of enteral insulin. |
| Criteria | Shulman RJ 2002, USA [15] |
|---|---|
| Was the research question or objective in this paper clearly stated? | ✔ |
| Was the study population clearly specified and defined? | ✔ |
| Was the participation rate of eligible persons at least 50%? | ✔ |
| Were all the subjects selected or recruited from the same or similar populations? | ✔ |
| Was a sample size justification, power description, or variance and effect estimates provided? | ✔ |
| For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured? | ✔ |
| Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed? | ✔ |
| For exposures that can vary in amount or level, did the study examine different levels of the exposure? | NA |
| Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? | ✔ |
| Was the exposure(s) assessed more than once over time? | NA |
| Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? | ✔ |
| Were the outcome assessors blinded to the exposure status of participants? | CD |
| Was loss to follow-up after baseline 20% or less? | ✔ |
| Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)? | No |
| Summary Quality | Fair |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qudsia, F.; Adil, M.; Kamran, M.; Azam, M.; Cheema, H.A.; Shahid, A.; Cherrez-Ojeda, I. Efficacy and Safety of Enteral Human Recombinant Insulin to Reduce the Time to Full Enteral Feeding in Preterm Infants: A Meta-Analytical Study. Pediatr. Rep. 2023, 15, 373-380. https://doi.org/10.3390/pediatric15020033
Qudsia F, Adil M, Kamran M, Azam M, Cheema HA, Shahid A, Cherrez-Ojeda I. Efficacy and Safety of Enteral Human Recombinant Insulin to Reduce the Time to Full Enteral Feeding in Preterm Infants: A Meta-Analytical Study. Pediatric Reports. 2023; 15(2):373-380. https://doi.org/10.3390/pediatric15020033
Chicago/Turabian StyleQudsia, Faiza, Muhammad Adil, Maha Kamran, Muhammad Azam, Huzaifa Ahmad Cheema, Abia Shahid, and Ivan Cherrez-Ojeda. 2023. "Efficacy and Safety of Enteral Human Recombinant Insulin to Reduce the Time to Full Enteral Feeding in Preterm Infants: A Meta-Analytical Study" Pediatric Reports 15, no. 2: 373-380. https://doi.org/10.3390/pediatric15020033