
Investigating Non-Pharmacological Stress Reduction Interventions in Pediatric Patients Confirmed with Salivary Cortisol Levels: A Systematic Review
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
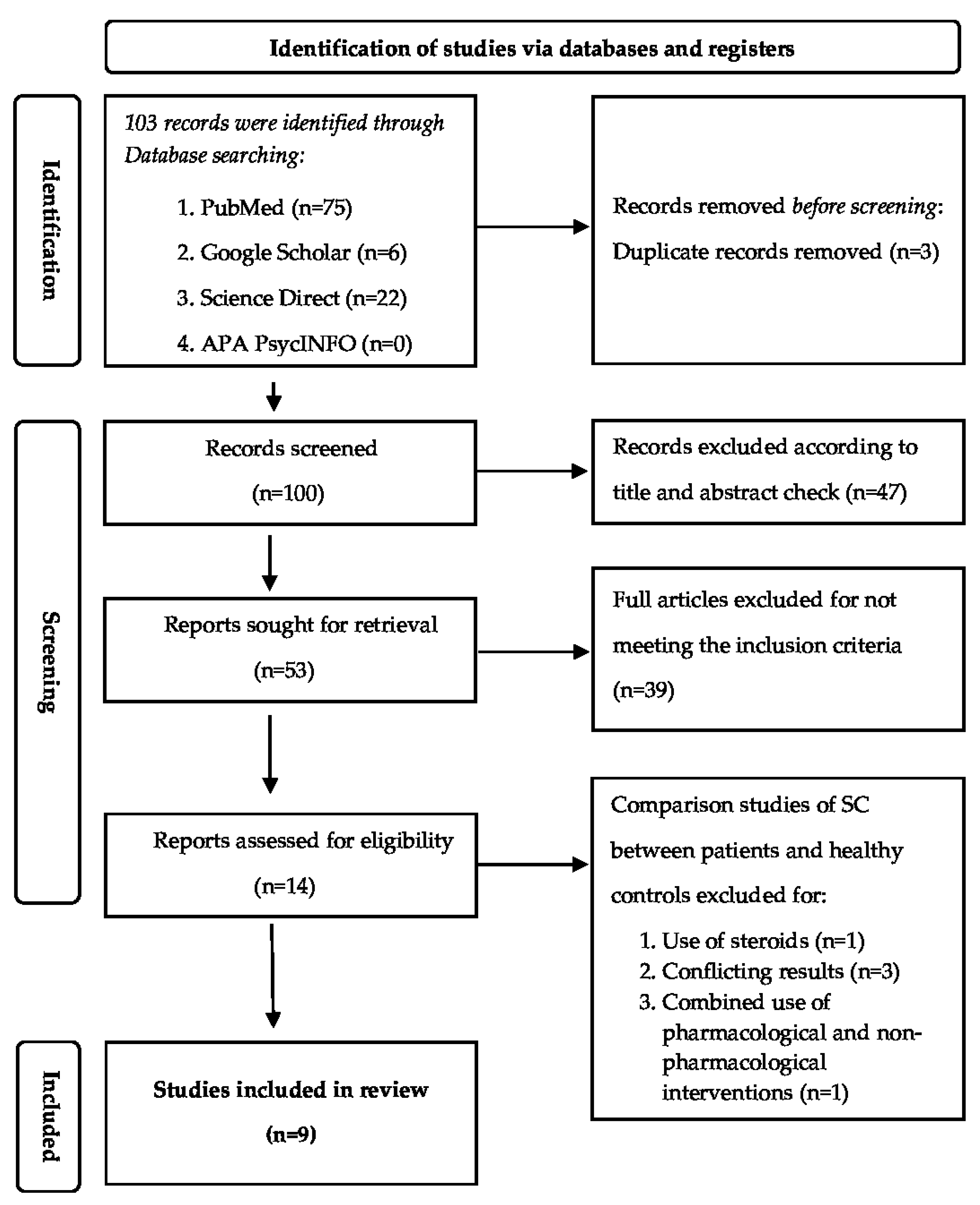
2.2. Search Strategy
- P: the population was children aged 3–18 years, who were visiting the hospital with any physical health condition. There were no limitations on their gender or socio-economic characteristics.
- Intervention: any interactive non-pharmacological strategy utilized.
- Comparison: the comparison was between CS levels of patients undergoing the intervention (Intervention Group, IG) and control group (CG).
- Outcome: saliva cortisol levels before and after intervention in the IG and CG.
- Study Design: randomized, quasi-randomized controlled trials and cohort studies.
2.3. Inclusion and Exclusion Criteria
2.4. Study Selection
2.5. Data Extracted
2.6. Classification of Non-Pharmacological Interventions and Definitions
- Educational intervention was defined as any approach which provided information, explanation, and preparations relevant to any surgical or medical intervention.
- Behavioral intervention was defined as the strategy which encouraged children to relieve pain or anxiety from a painful event.
- Parental presence was a strategy to reduce a child’s anxiety by parental comforting and attendance during procedures such as induction of anesthesia.
- Complementary and alternative strategies were defined as interactive approaches constructed to be performed alone or with other techniques to relieve anxiety of fear feelings during any medical or perioperative procedures [15].
3. Results
3.1. Studies Characteristics

{kind=link}
| Authors/Year | Age: Range or Mean ± SD Years or Months | N [Gender (M/F)] | Reasons of Hospitalization | Type of Intervention | Outcome Results Based on SC Levels |
|---|---|---|---|---|---|
| Wennström et al. [23], 2011 | IG: 94 ± 23 (months) CG: 91 ± 26 (months) | 93 [79/14] | Day-surgery operations | IG: PD CG1: standard care CG2: standard care + information | Significantly lower SC levels (p = 0.003) an in the PD group post-op |
| Calcaterra et al. [24], 2015 | IG: 8.59 ± 3.7 (yrs) CG: 7.36 ± 2.48 (yrs) Range: 7–17 (yrs) | 40 [32/8] | Day-surgery operations | IG: AAT CG: common care | No statistically differences between groups (p = 0.70) |
| Lima et al. [25], 2015 | Range: 6–14 (yrs) | 40 [NI] | Urological surgery | IG: Interactive Musical Activities CG: no music | No differences in SC levels between groups (p > 0.05) |
| Saliba et al. [26], 2016 | 6–7 (yrs) | 36 [NI] | Appendicitis, femur fracture, adenoid hypertrophy, trachea trauma, phimosis, paraphimosis, pneumonia | IG: CD at lunch CG: CD at dinner | SC levels were significantly reduced after CD intervention in both groups (p < 0.01 and p < 0.01, respectively Better satisfaction for CD at lunch |
| Branson et al. [27], 2017 | IG: 13.43 ± 0.59 CG: 12.83 ± 0.58 p = 0.364 | 48 [24/24] | Surgical, pneumological, trauma, neurological, immunological, endocrine, psychiatric, gastrointestinal, and liver disorders | IG: AAA CG: no person or live dog | Increased positive effect and decreased negative effect in the AAA group compared to CG, but not significant. No statistical differences in SC levels between groups (p = 0.47) |
| Ozdogan et al. [28], 2017 | IG: 7.41 ± 2.30 (yrs) CG: 7.37 ± 2.06 (yrs) p = 0.94 | 48 [21/27] | Tonsillectomy and or adenoidectomy | IG: Mother’s presence CG: Mother’s absence | SC levels were significantly increased in CG after induction and in recovery room compared to IG (p = 0.001 and p = 0.02, respectively) |
| Volkan et al. [29], 2019 | IG: 11.55 ± 2.52 CG:11.44 ± 2.66 p = 0.773 | 184 [85/99] | Gastroscopy | IG: Detailed information CG: brief information | SC levels significantly less in the IG (p < 0.001) |
| Alarcon-Yacketto et al. [30], 2021 | IG: 9.35 ± 1.59 CG: 10.33 ± 1.39 p: 0.091 | 29 [18/11] | Various types of acute appendicitis, bone fractures, mastoiditis | * IG: Augmented reality books # CG: standard books | Marked decreased in SC levels in IG vs. CG (p < 0.001) |
| Brockingston et al. [31], 2021 | Total: 7.06 ± 2.23 (yrs) IG: 7.02 ± 2.14 (yrs) CG: 7.1 ± 2.34 (yrs) | 81 [40/41] | PICU (respiratory diseases most common) | IG: Storytelling CG: Riddle | Marked decreased of SC in the IG vs. CG (p < 0.001) |
3.2. Study Population
3.3. Types of Intervention
3.3.1. Educational Intervention
3.3.2. Behavioral Interventions
3.3.3. Maternal Presence
3.3.4. Complementary Interventions
- Animal-Assisted Therapy
- a.
- In the study by Calcaterra et al. [24], the authors evaluated the impact of animal-assisted therapy (AAT) on the children’s response to stress and pain in the immediate postoperative period. They randomly assigned 40 patients into two groups: IG (20 patients) and CG (20 patients). The primary end-point concerned the impact of AAT in IG on neurological signs as measured with electroencephalogram. Secondary end-points concerned the impact of AAT on the cardiovascular system by measuring vital signs (heart rate, blood pressure, oxygen saturation, and cerebral prefrontal oxygenation) and endocrinological impact as measured by SC levels at two hours after surgery (T1), at 20 min following T (T2), and only for SC levels at midnight (T3), the time when cortisol is normally at its lowest. Additionally, a faces pain scale was used to measure child self-reported pain at T1 and T2.
- b.
- Music Therapy
- Clown Doctors (CD)
3.4. Effect of Non-Pharmacological Interventions on SC Levels in Hospitalized Children and Adolescents
3.4.1. Educational Intervention
3.4.2. Behavioral Intervention
3.4.3. Maternal Presence
3.4.4. Complementary Interventions
3.4.5. Additional Findings
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, M.E.; Megel, M.E.; Enenbach, L.; Carlson, K.L. The voices of children: Stories about hospitalization. J. Pediatr. Health Care 2010, 24, 95–102. [Google Scholar] [CrossRef]
- Caldas, J.C.S.; Pais-Ribeiro, J.L.; Carneiro, S.R. General anesthesia, surgery and hospitalization in children and their effects upon cognitive, academic, emotional and sociobehavioral development—A review. Pediatr. Anesth. 2004, 14, 910–915. [Google Scholar] [CrossRef]
- Mîndru, D.E.; Stănescu, R.S.; Mioara, C.M.; Duceac, L.D.; Rugina, A.; Temneanu, O.R.; Ungureanu, M.; Florescu, L. Stress in Pediatric Patients—The Effect of Prolonged Hospitalization. Rev. Med. Chir. A Soc. De Med. Si Nat. Din Iasi 2016, 120, 417–423. [Google Scholar]
- Coyne, I. Children’s experiences of hospitalization. J. Child Health Care Prof. Work. Child. Hosp. Community 2006, 10, 326–336. [Google Scholar] [CrossRef]
- Ahmed, M.I.; Farrell, M.A.; Parrish, K.; Karla, A. Preoperative anxiety in children risk factors and non-pharmacological management. Middle East J. Anaesthesiol. 2011, 21, 153–164. [Google Scholar]
- Li, W.H.C.; Chung, J.O.K.; Ho, K.Y.; Kwok, B.M.C. Play interventions to reduce anxiety and negative emotions in hospitalized children. BMC Pediatr. 2016, 16, 36. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Cho, B.K.; Cho, D.H.; Park, H.J. Expression of hypothalamic-pituitary-adrenal axis in common skin diseases: Evidence of its association with stress-related disease activity. Acta Derm. Venereol. 2013, 93, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Egliston, K.-A.; McMahon, C.; Austin, M.-P. Stress in pregnancy and infant HPA axis function: Conceptual and methodological issues relating to the use of salivary cortisol as an outcome measure. Psychoneuroendocrinology 2007, 32, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, V.M.; Mondelli, M.; José, M.R.; Gomide, M.R.; Lauris, J.R.P.; Feniman, M.R. Salivary Cortisol and Sustained Auditory Attention in Children with and without Cleft Lip and Palate. Int. Arch. Otorhinolaryngol. 2022, 26, e605–e614. [Google Scholar] [CrossRef]
- Simons, S.S.H.; Beijers, R.; Cillessen, A.H.N.; Weerth, C.d. Development of the cortisol circadian rhythm in the light of stress early in life. Psychoneuroendocrinology 2015, 62, 292–300. [Google Scholar] [CrossRef]
- Knutsson, U.; Dahlgren, J.; Marcus, C.; Rosberg, S.; Brönnegård, M.; Stierna, P.; Albertsson-Wikland, K. Circadian Cortisol Rhythms in Healthy Boys and Girls: Relationship with Age, Growth, Body Composition, and Pubertal Development. J. Clin. Endocrinol. Metab. 1997, 82, 536–540. [Google Scholar] [CrossRef]
- Rosmalen, J.G.M.; Oldehinkel, A.J.; Ormel, J.; de Winter, A.F.; Buitelaar, J.K.; Verhulst, F.C. Determinants of salivary cortisol levels in 10–12 year old children; a population-based study of individual differences. Psychoneuroendocrinology 2005, 30, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Seltzer, M.M.; Greenberg, J.S.; Hong, J.; Smith, L.E.; Almeida, D.M.; Coe, C.; Stawski, R.S. Maternal cortisol levels and behavior problems in adolescents and adults with ASD. J. Autism Dev. Disord. 2010, 40, 457–469. [Google Scholar] [CrossRef] [PubMed]
- Tzortzi, C.; Proff, P.; Redlich, M.; Aframian, D.J.; Palmon, A.; Golan, I.; Muessig, D.; Wichelhaus, A.; Baumert, U. Cortisol daily rhythm in saliva of healthy school children. Int. Dent. J. 2009, 59, 12–18. [Google Scholar]
- Agbayani, C.G.; Fortier, M.A.; Kain, Z.N. Non-pharmacological methods of reducing perioperative anxiety in children. BJA Educ. 2020, 20, 424–430. [Google Scholar] [CrossRef]
- Rantala, A.; Pikkarainen, M.; Miettunen, J.; He, H.G.; Pölkki, T. The effectiveness of web-based mobile health interventions in paediatric outpatient surgery: A systematic review and meta-analysis of randomized controlled trials. J. Adv. Nurs. 2020, 76, 1949–1960. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane. 2022. Available online: www.training.cochrane.org/handbook (accessed on 29 March 2023).
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Šimleša, S.; Cepanec, M. Executive Functions during Childhood, Development of. In International Encyclopedia of the Social & Behavioral Sciences, 2nd ed.; Wright, J.D., Ed.; Elsevier: Oxford, UK, 2015; pp. 489–496. [Google Scholar] [CrossRef]
- Dereci, O.; Saruhan, N. The Comparison of Dental Anxiety between Patients Treated with Impacted Third Molar Surgery and Conventional Dental Extraction. BioMed Res. Int. 2021, 2021, 7492852. [Google Scholar] [CrossRef]
- Kumari, A.; Chandra, P.; Roy, S.; Agarwal, R.; Singh, A.; Sharan, S. Evaluation of Preoperative Salivary Cortisol Level in Patients Undergoing Major Maxillofacial Surgery. J. Pharm. Bioallied Sci. 2021, 13, S120–S123. [Google Scholar] [CrossRef]
- Wennström, B.; Törnhage, C.J.; Nasic, S.; Hedelin, H.; Bergh, I. The perioperative dialogue reduces postoperative stress in children undergoing day surgery as confirmed by salivary cortisol. Pediatr. Anesth. 2011, 21, 1058–1065. [Google Scholar] [CrossRef]
- Calcaterra, V.; Veggiotti, P.; Palestrini, C.; De Giorgis, V.; Raschetti, R.; Tumminelli, M.; Mencherini, S.; Papotti, F.; Klersy, C.; Albertini, R. Post-operative benefits of animal-assisted therapy in pediatric surgery: A randomised study. PLoS ONE 2015, 10, e0125813. [Google Scholar] [CrossRef]
- Lima, V.; Domenice, S.; Costa, E.; Brito, V.; Inacio, M.; Mendonca, B. Effects of Interactive Musical Activities on the Well-being of Children with Urogenital Anomalies during Hospitalization for Surgery. Res. Humanit. Soc. Sci. 2015, 5, 61–70. [Google Scholar]
- Saliba, F.G.; Adiwardana, N.S.; Uehara, E.U.; Silvestre, R.N.; Leite, V.V.; Faleiros, F.T.; Padovani, F.H.; De Gobbi, J.I. Salivary Cortisol Levels: The Importance of Clown Doctors to Reduce Stress. Pediatr. Rep. 2016, 8, 6188. [Google Scholar] [CrossRef]
- Branson, S.M.; Boss, L.; Padhye, N.S.; Trötscher, T.; Ward, A. Effects of Animal-assisted Activities on Biobehavioral Stress Responses in Hospitalized Children: A Randomized Controlled Study. J. Pediatr. Nurs. 2017, 36, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Ozdogan, H.K.; Cetinalp, S.; Kuran, G.; Tugal, O.; Tahiroglu, M.; Herdem, U.E.; Haytoglu, S. The effects of maternal presence during anesthesia induction on salivary cortisol levels in children undergoing tonsillectomy and/or adenoidectomy. J. Clin. Anesth. 2017, 39, 64–66. [Google Scholar] [CrossRef]
- Volkan, B.; Bayrak, N.A.; Ucar, C.; Kara, D.; Yıldız, S. Preparatory information reduces gastroscopy-related stress in children as confirmed by salivary cortisol. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2019, 25, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Alarcón-Yaquetto, D.E.; Tincopa, J.P.; Guillén-Pinto, D.; Bailon, N.; Cárcamo, C.P. Effect of augmented reality books in salivary cortisol levels in hospitalized pediatric patients: A randomized cross-over trial. Int. J. Med. Inform. 2021, 148, 104404. [Google Scholar] [CrossRef]
- Brockington, G.; Gomes Moreira, A.P.; Buso, M.S.; Gomes da Silva, S.; Altszyler, E.; Fischer, R.; Moll, J. Storytelling increases oxytocin and positive emotions and decreases cortisol and pain in hospitalized children. Proc. Natl. Acad. Sci. USA 2021, 118, e2018409118. [Google Scholar] [CrossRef] [PubMed]
- Jaaniste, T.; Hayes, B.; Von Baeyer, C.L. Providing children with information about forthcoming medical procedures: A review and synthesis. Clin. Psychol. Sci. Pract. 2007, 14, 124. [Google Scholar] [CrossRef]
- Hatipoglu, Z.; Gulec, E.; Lafli, D.; Ozcengiz, D. Effects of auditory and audiovisual presentations on anxiety and behavioral changes in children undergoing elective surgery. Niger. J. Clin. Pract. 2018, 21, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Tomaszek, L.; Cepuch, G.; Fenikowski, D. Influence of preoperative information support on anxiety, pain and satisfaction with postoperative analgesia in children and adolescents after thoracic surgery: A randomized double blind study. Biomed. Pap. 2019, 163, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Lilik Lestari, M.P.; Wanda, D.; Hayati, H. The effectiveness of distraction (Cartoon-Patterned Clothes and Bubble-Blowing) on pain and anxiety in preschool children during venipuncture in the emergency department. Compr. Child Adolesc. Nurs. 2017, 40, 22–28. [Google Scholar] [CrossRef] [PubMed]
- MacLaren, J.E.; Cohen, L.L. A Comparison of Distraction Strategies for Venipuncture Distress in Children. J. Pediatr. Psychol. 2005, 30, 387–396. [Google Scholar] [CrossRef]
- Kain, Z.N.; Mayes, L.C.; Caldwell-Andrews, A.A.; Saadat, H.; McClain, B.; Wang, S.M. Predicting which children benefit most from parental presence during induction of anesthesia. Paediatr. Anaesth. 2006, 16, 627–634. [Google Scholar] [CrossRef]
- Yoo, J.-B.; Kim, M.-J.; Cho, S.-H.; Shin, Y.-J.; Kim, N.-C. The effects of pre-operative visual information and parental presence intervention on anxiety, delirium, and pain of post-operative pediatric patients in PACU. J. Korean Acad. Nurs. 2012, 42, 333–341. [Google Scholar] [CrossRef]
- Kain, Z.N.; Mayes, L.C.; Wang, S.M.; Caramico, L.A.; Hofstadter, M.B. Parental presence during induction of anesthesia versus sedative premedication: Which intervention is more effective? Anesthesiology 1998, 89, 1147–1156. [Google Scholar] [CrossRef]
- Kain, Z.N.; Mayes, L.C.; Caramico, L.A.; Silver, D.; Spieker, M.; Nygren, M.M.; Anderson, G.; Rimar, S. Parental presence during induction of anesthesia. A randomized controlled trial. Anesthesiology 1996, 84, 1060–1067. [Google Scholar] [CrossRef]
- Kain, Z.N.; Mayes, L.C.; Wang, S.M.; Caramico, L.A.; Krivutza, D.M.; Hofstadter, M.B. Parental presence and a sedative premedicant for children undergoing surgery: A hierarchical study. Anesthesiology 2000, 92, 939–946. [Google Scholar] [CrossRef]
- Yip, P.; Middleton, P.; Cyna, A.M.; Carlyle, A.V. Non-pharmacological interventions for assisting the induction of anaesthesia in children. Cochrane Database Syst. Rev. 2009, 3, CD006447. [Google Scholar] [CrossRef]
- Zand, F.; Allahyary, E.; Hamidi, A.R. Postoperative agitation in preschool children following emergence from sevoflurane or halothane anesthesia: A randomized study on the forestalling effect of midazolam premedication versus parental presence at induction of anesthesia. Acta Anaesthesiol. Taiwanica Off. J. Taiwan Soc. Anesthesiol. 2011, 49, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.M.; Monico, E.; Kao, G.; Guffey, D.; Kim, E.; Khatker, M.; Gilbert, C.; Biard, M.; Marcus, M.; Roth, I.; et al. Addressing Pain with Inpatient Integrative Medicine at a Large Children’s Hospital. Clin. Pediatr. 2019, 58, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Okita, S.Y. Self-other’s perspective taking: The use of therapeutic robot companions as social agents for reducing pain and anxiety in pediatric patients. Cyberpsychol. Behav. Soc. Netw. 2013, 16, 436–441. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grigoropoulou, M.; Kapetanakis, E.I.; Attilakos, A.; Charalampopoulos, A.; Dimopoulou, A.; Vamvakas, E.; Mavrigiannaki, E.; Zavras, N. Investigating Non-Pharmacological Stress Reduction Interventions in Pediatric Patients Confirmed with Salivary Cortisol Levels: A Systematic Review. Pediatr. Rep. 2023, 15, 349-359. https://doi.org/10.3390/pediatric15020031
Grigoropoulou M, Kapetanakis EI, Attilakos A, Charalampopoulos A, Dimopoulou A, Vamvakas E, Mavrigiannaki E, Zavras N. Investigating Non-Pharmacological Stress Reduction Interventions in Pediatric Patients Confirmed with Salivary Cortisol Levels: A Systematic Review. Pediatric Reports. 2023; 15(2):349-359. https://doi.org/10.3390/pediatric15020031
Chicago/Turabian StyleGrigoropoulou, Maria, Emmanouil I. Kapetanakis, Achilleas Attilakos, Anestis Charalampopoulos, Anastasia Dimopoulou, Efstratios Vamvakas, Eleftheria Mavrigiannaki, and Nikolaos Zavras. 2023. "Investigating Non-Pharmacological Stress Reduction Interventions in Pediatric Patients Confirmed with Salivary Cortisol Levels: A Systematic Review" Pediatric Reports 15, no. 2: 349-359. https://doi.org/10.3390/pediatric15020031