
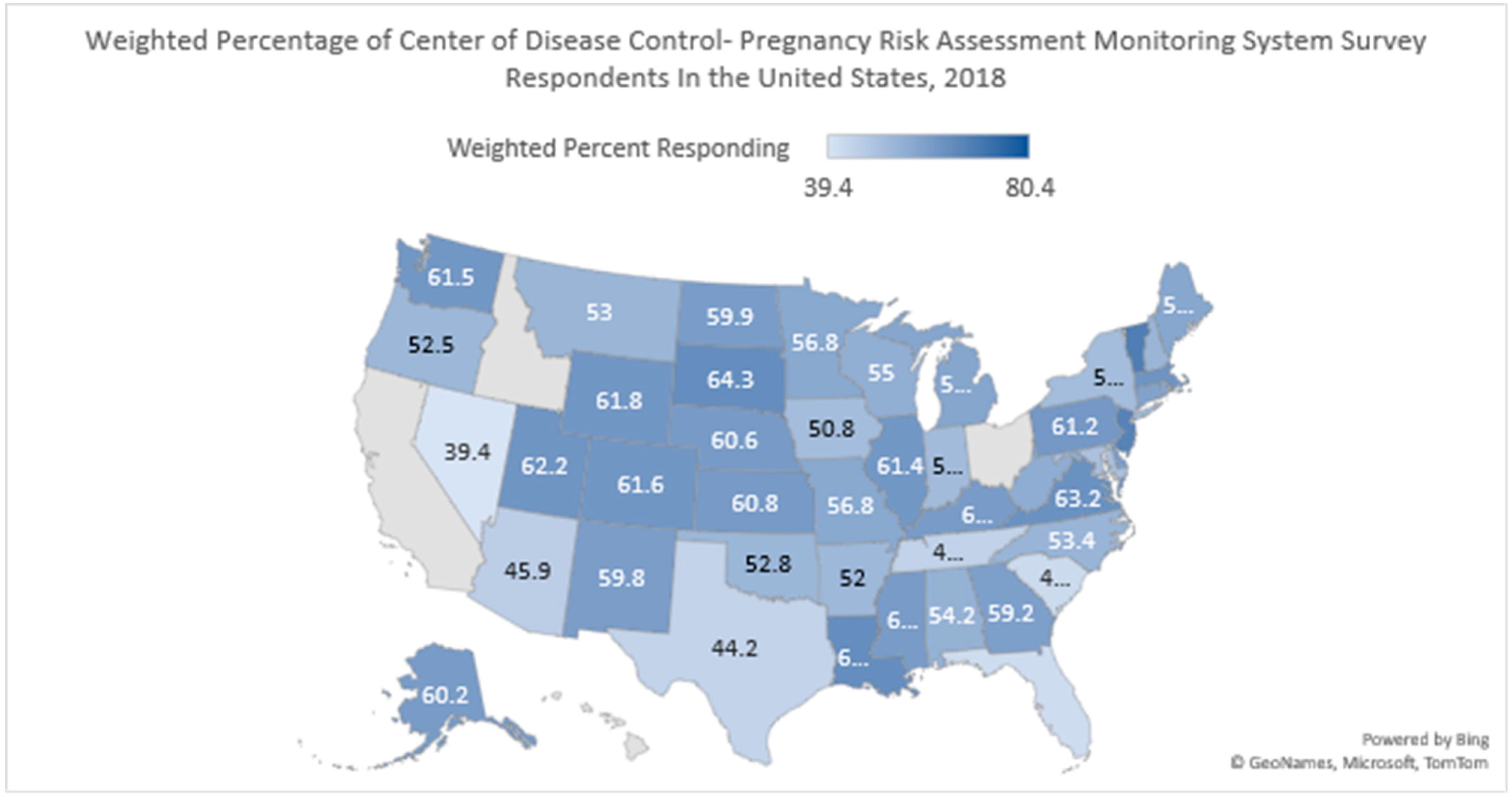
Impact of Prenatal Health Conditions and Health Behaviors in Pregnant Women on Infant Birth Defects in the United States Using CDC-PRAMS 2018 Survey

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Data & Statistics on Birth Defects|CDC. Centers for Disease Control and Prevention. 23 January 2020. Available online: https://www.cdc.gov/ncbddd/birthdefects/data.html (accessed on 12 December 2020).
- Strauss, R.P.; Cassell, C.H. Critical Issues in Craniofacial Care: Quality of Life, Costs of Care, and Implications of Prenatal Diagnosis. Acad. Pediatr. 2009, 9, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.L.; Singer, M.R.; Bradlee, M.L.; Rothman, K.J.; Milunsky, A. A Prospective Study of the Risk of Congenital Defects Associated with Maternal Obesity and Diabetes Mellitus. Epidemiology 2000, 11, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Behavioral Risk Factor Surveillance System 2019 Summary Data Quality Report July 16, 2020. July 2020. Available online: https://www.cdc.gov/brfss/annual_data/2019/pdf/2019-sdqr-508.pdf (accessed on 6 June 2021).
- Hackshaw, A.; Rodeck, C.; Boniface, S. Maternal smoking in pregnancy and birth defects: A systematic review based on 173 687 malformed cases and 11.7 million controls. Hum. Reprod. Updat. 2011, 17, 589–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Impellizzeri, A.; Giannantoni, I.; Polimeni, A.; Barbato, E.; Galluccio, G. Epidemiological characteristic of Orofacial clefts and its associated congenital anomalies: Retrospective study. BMC Oral Health 2019, 19, 290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ban, L.; Gibson, J.; West, J.; Fiaschi, L.; Sokal, R.; Smeeth, L.; Doyle, P.; Hubbard, R.; Tata, L. Maternal Depression, antidepressant prescriptions, and congenital anomaly risk in offspring: A population-based cohort study. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 1471–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.; Jiang, X.; Bao, W.; Xu, G.; Yang, R.; Shen, M. Association of intimate partner violence during pregnancy, prenatal depression, and adverse birth outcomes in Wuhan, China. BMC Pregnancy Childbirth 2018, 18, 469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulman, H.B.; D’Angelo, D.V.; Harrison, L.; Smith, R.A.; Warner, L. The Pregnancy Risk Assessment Monitoring System (PRAMS): Overview of Design and Methodology. Am. J. Public Health 2018, 108, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Chisnall, P.M. Mail and Internet Surveys: The Tailored Design Method. J. Advert. Res. 2007, 47, 207–208. [Google Scholar] [CrossRef]
- PRAMS Methodology|CDC. CDC-PRAMS. 2019. Available online: https://www.cdc.gov/prams/methodology.htm#2 (accessed on 6 January 2021).
- Steinbacher, D.; Sierakowski, S. First Aid for the NBDE Part 1, 3rd ed.; First Aid Series; McGraw Hill/Medical: New York, NY, USA, 2012. [Google Scholar]
- Berg, E.; Lie, R.T.; Sivertsen, S.; Haaland, Y.A. Parental age and the risk of isolated cleft lip: A registry-based study. Ann. Epidemiol. 2015, 25, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, A. Risk factors associated with metabolic syndrome in type 2 diabetes mellitus patients according to World Health Organization, Third Report National Cholesterol Education Program, and International Diabetes Federation definitions. Diabetes Metab. Syndr. Obes. Targets Ther. 2010, 4, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biggio, J.R.; Chapman, V.; Neely, C.; Cliver, S.P.; Rouse, D.J. Fetal Anomalies in Obese Women. Obstet. Gynecol. 2010, 115, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Xuan, Z.; Zhongpeng, Y.; Yanjun, G.; Jiaqi, D.; Yuchi, Z.; Bing, S.; Chenghao, L. Maternal active smoking and risk of oral clefts: A meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 680–690. [Google Scholar] [CrossRef] [PubMed]
- Shelke, G.S.; Marwaha, R.S.; Shah, P.; Challa, S. Role of Patient’s Ethnicity in Seeking Preventive Dental Services at the Community Health Centers of South-Central Texas: A Cross-Sectional Study. Dent. J. 2023, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Home Visiting | MCHB. HRSA. 13 October 2021. Available online: https://mchb.hrsa.gov/programs-impact/programs/home-visiting (accessed on 6 May 2021).
- Pereira, A.V.; Fradinho, N.; Carmo, S.; de Sousa, J.M.; Rasteiro, D.; Duarte, R.; Leal, M.J. Associated Malformations in Children with Orofacial Clefts in Portugal. Plast. Reconstr. Surg.-Glob. Open 2018, 6, e1635. [Google Scholar] [CrossRef] [PubMed]

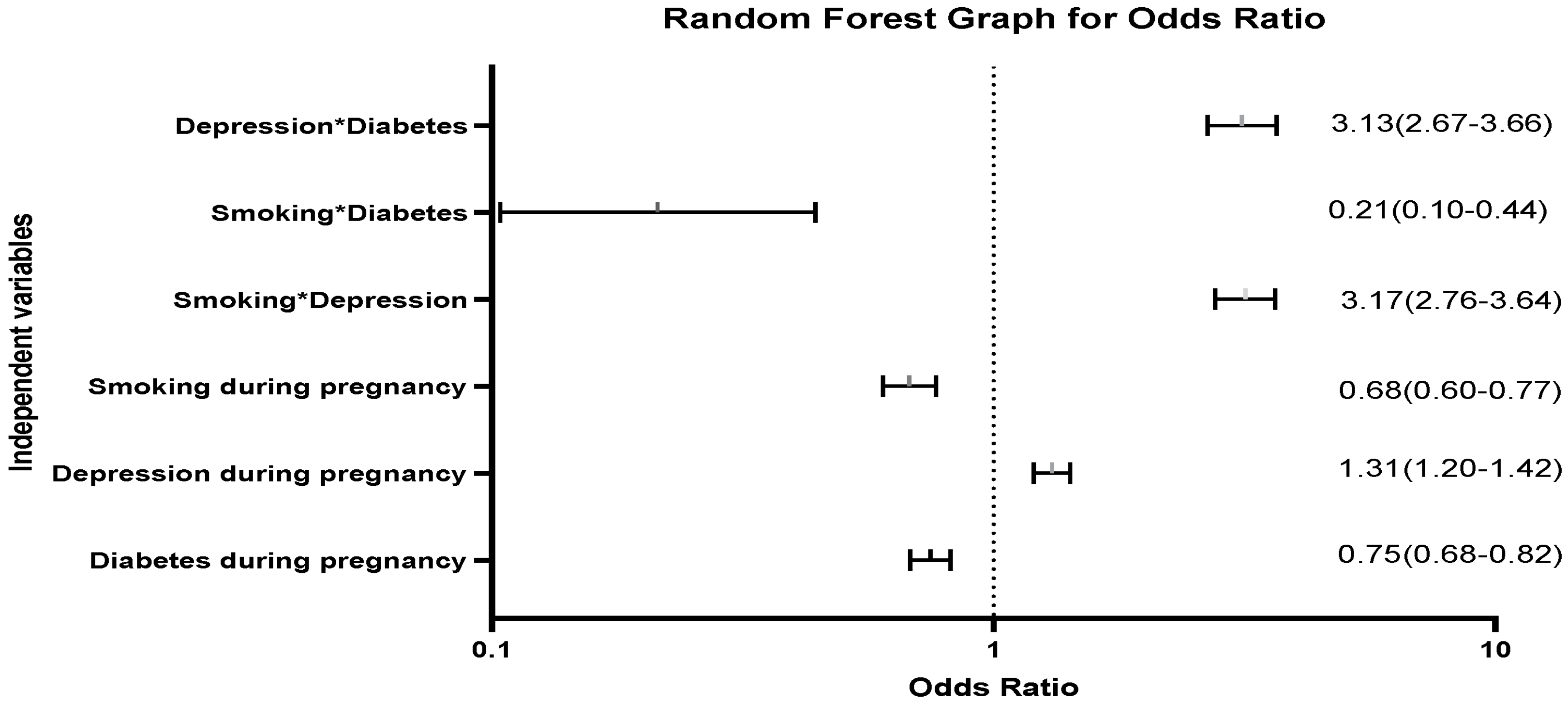
 Represent the confidence interval of odds ratio.
Represent the confidence interval of odds ratio.
Represent the confidence interval of odds ratio.
Represent the confidence interval of odds ratio.


{kind=link}
{kind=link}
{kind=link}
| Variables | Data Characteristics | Birth Defect | ||||
|---|---|---|---|---|---|---|
| N ‡ | Percentage | Yes N ‡ (%) | No N ‡ (%) | Chi-Square § | p-Value † | |
| Mother’s characteristics | ||||||
| Age | ||||||
| <17 | 50,364 | 1.1% | 98 (0.2) | 50,229 (99.8) | 800.13 | <0.001 |
| 18–19 | 139,179 | 3.1% | 399 (0.3) | 138,374 (99.7) | ||
| 20–24 | 845,587 | 18.6% | 3093 (0.4) | 841,067 (99.6) | ||
| 25–29 | 1,314,183 | 29.0% | 2956 (0.2) | 1,308,909 (99.8) | ||
| 30–34 | 1,328,787 | 29.3% | 3230 (0.2) | 1,320,862 (99.8) | ||
| 35–39 | 703,497 | 15.5% | 1653 (0.2) | 700,054 (99.8) | ||
| 40+ | 155,236 | 3.4% | 791 (0.5) | 153,818 (99.5) | ||
| Missing | 34 | 0.0% | ||||
| Income | ||||||
| Zero–USD 28,000 | 1,508,760 | 33.3% | 4255 (0.3) | 1,500,510 (99.7) | 34.9 | <0.001 |
| USD 28,000–57,000 | 879,645 | 19.4% | 2269 (0.3) | 875,240 (99.7) | ||
| USD 57,000–85,000 or More | 1,751,664 | 38.6% | 4362 (0.2) | 1,743,236 (99.8) | ||
| Missing | 396,795 | 8.7% | ||||
| Race | ||||||
| Asian | 229,932 | 5.1% | 666 (0.3) | 228,766 (99.7) | 198.11 | <0.001 |
| Other American Including Tribes | 38,887 | 0.9% | 75 (0.2) | 38,749 (99.8) | ||
| Black | 757,121 | 16.7% | 1539 (0.2) | 753,570 (99.8) | ||
| Mixed Race | 127,388 | 2.8% | 311 (0.2) | 126,918 (99.8) | ||
| Other Non-White | 274,327 | 6.0% | 596 (0.2) | 273,223 (99.8) | ||
| White | 3,051,298 | 67% | 8729 (0.3) | 3,035,422 (99.7) | ||
| Missing | 57,915 | 1.3% | ||||
| Body mass index of mother | ||||||
| Underweight (<18.5) | 141,959 | 3.1% | 494 (0.3) | 141,200 (99.7) | 99.03 | <0.001 |
| Normal (18.5–24.9) | 1,898,401 | 41.8% | 5518 (0.3) | 1,888,558 (99.7) | ||
| Overweight (25.0–29.9) | 1,130,903 | 24.9% | 2711 (0.2) | 1,124,409 (99.8) | ||
| Obese (30+) | 1,151,785 | 25.4% | 3053 (0.3) | 1,146,051 (99.7) | ||
| Missing | 213,819 | 4.7% | ||||
| Mothers who are smokers Regardless of pregnancy status. | ||||||
| Yes | 311,557 | 6.9% | 1876 (0.6) | 308,897 (99.4) | 1375.41 | <0.001 |
| No | 4,203,389 | 92.6% | 10,301 (0.2) | 4,183,100 (99.8) | ||
| Missing | 21,921 | 0.5% | ||||
| Smoking only during pregnancy | ||||||
| Yes | 327,826 | 7.2% | 10,286 (0.2) | 4,118,488 (99.8) | 1032.85 | <0.001 |
| No | 4,138,986 | 91.2% | 1807 (0.6) | 324,968 (99.4) | ||
| Missing | 70,055 | 1.5% | ||||
| Women who reported depression regardless of pregnancy status | ||||||
| Yes | 668,354 | 14.7% | 1922 (0.3) | 664,596 (99.7) | 7.47 | <0.006 |
| No | 3,823,333 | 84.3% | 10,277 (0.3) | 3,803,706 (99.7) | ||
| Missing | 45,179 | 1.0% | ||||
| Depression only during pregnancy | ||||||
| Yes | 64,2407 | 14.2% | 2377 (0.4) | 638,081 (99.6) | 261.7 | <0.001 |
| No | 3,808,470 | 83.9% | 9765 (0.3) | 3,789,375 (99.7) | ||
| Missing | 85,990 | 1.9% | ||||
| Mothers reported anxiety regardless of pregnancy status | ||||||
| Yes | 487,461 | 10.7% | 1086 (0.2) | 485,238 (99.8) | 295.1 | <0.001 |
| No | 3,409,226 | 75.1% | 9974 (0.3) | 3,390,314 (99.7) | ||
| Missing | 640,180 | 14.1% | 1158 (0.2) | 637,796 (99.8) | ||
| Abuse only during pregnancy | ||||||
| Yes | 63,450 | 1.4% | 264 (0.4) | 63,029 (99.6) | 51.2 | <0.001 |
| No | 4,392,556 | 96.8% | 11,757 (0.3) | 4,369,716 (99.7) | ||
| Missing | 80,861 | 1.8.% | ||||
| Mothers who reported diabetes regardless of pregnancy status | ||||||
| Yes | 141,146 | 3.1% | 217 (0.2) | 140,473 (99.8) | 73.65 | <0.001 |
| No | 4,344,290 | 95.8% | 11,925 (0.3) | 4,321,576 (99.7) | ||
| Missing | 51,431 | 1.1% | ||||
| Diabetes only during pregnancy | ||||||
| Yes | 434,979 | 9.6% | 1259 (0.3) | 432,752 (99.7) | 5.16 | 0.023 |
| No | 4,036,773 | 89.0% | 10,918 (0.3) | 4,015,612 (99.7) | ||
| Missing | 65,114 | 1.4% | ||||
| Vitamin intake | ||||||
| Folic acid | ||||||
| Yes | 2,238,514 | 49.3% | 5595 (0.3) | 2,227,582 (99.7) | 135.45 | <0.001 |
| No | 1,751,954 | 38.6% | 4764 (0.3) | 1,743,099 (99.7) | ||
| Missing | 546,399 | 12.0% | 1860 (0.3) | 542,667 (99.7) | ||
| Hypertension | ||||||
| Yes | 455,088 | 10% | 1453 (0.3) | 452,020 (99.7) | 49.96 | <0.001 |
| No | 4,074,956 | 89.8% | 10,765 (0.3) | 4,055,870 (99.7) | ||
| Missing | 6823 | 0.2% | ||||
| p-Value † | Odds Ratio | 95% CI ‡ | |
|---|---|---|---|
| Maternal Age | <0.001 | . | |
| <=17 | 0.367 | 0.86 | (0.62–1.20) |
| 18–19 | <0.001 | 1.67 | (1.49–1.87) |
| 20–24 | <0.001 | 1.24 | (1.17–1.32) |
| 25–29 | 1 | ||
| 30–34 | 0.214 | 0.97 | (0.91–1.02) |
| 35–39 | 0.525 | 0.98 | (0.92–1.05) |
| 40+ | <0.001 | 2.20 | (2.01–2.40) |
| Maternal Race | <0.001 | ||
| White | 1 | ||
| Asian | <0.001 | 1.17 | (1.07–1.28) |
| Other American Including Tribes | <0.001 | 0.61 | (0.47–0.80) |
| Black | <0.001 | 0.74 | (0.69–0.79) |
| Mixed Race | 0.895 | 0.99 | (0.88–1.12) |
| Other Non-White | 0.001 | 0.83 | (0.75–0.93) |
| Income | <0.001 | ||
| Zero to USD28,000 | 0.094 | 0.95 | (0.90–1.01) |
| USD 28,000 to 57,000 | 0.012 | 1.08 | (1.02–1.14) |
| USD 57,000 to 85,000 or More | 1 | ||
| Vitamin | <0.001 | ||
| Everyday/Week | 1 | ||
| Didn’t Take Vitamin | <0.001 | 0.81 | (0.77–0.85) |
| 1–3 Times/Week | 0.648 | 0.98 | (0.91–1.06) |
| 4–6 Times/Week | <0.001 | 0.83 | (0.76–0.91) |
| Hypertension | |||
| No | 1 | ||
| Yes | <0.001 | 1.28 | (1.20–1.36) |
| Body mass index of Mother | <0.001 | ||
| Normal (18.5–24.9) | 1 | ||
| Underweight (<18.5) | <0.001 | 1.41 | (1.28–1.55) |
| Overweight (25.0–29.9) | <0.001 | 0.82 | (0.78–0.86) |
| Obese (30.0+) | 0.005 | 1.08 | (1.02–1.13) |
| Abuse only during pregnancy | |||
| No | 1 | ||
| Yes | 0.175 | 1.11 | (0.96–1.29) |
| Mothers who are smokers regardless of pregnancy status. | |||
| No | 1 | ||
| Yes | <0.001 | 2.29 | (2.09–2.51) |
| Mothers who reported diabetes regardless of pregnancy status | |||
| No | 1 | ||
| Yes | <0.001 | 0.31 | (0.25–0.39) |
| Mothers who reported depression regardless of pregnancy status | |||
| No | 1 | ||
| Yes | <0.001 | 0.58 | (0.53–0.63) |
| Diabetes only during pregnancy | |||
| No | 1 | ||
| Yes | <0.001 | 0.75 | (0.68–0.82) |
| Depression only during pregnancy | |||
| No | 1 | ||
| Yes | <0.001 | 1.31 | (1.20–1.42) |
| Smoking only during pregnancy | |||
| No | 1 | ||
| Yes | <0.001 | 0.68 | (0.60–0.77) |
| Folic acid intake | <0.001 | ||
| Yes | 1 | ||
| Missing | <0.001 | 1.42 | (1.33–1.51) |
| No | <0.001 | 1.16 | (1.11–1.22) |
| Mothers reported anxiety regardless of pregnancy status | <0.001 | ||
| No | 1 | ||
| Missing | <0.001 | 0.68 | (0.63–0.72) |
| Yes | <0.001 | 0.75 | (0.70–0.81) |
| Smoking 1 * depression 2 * diabetes 3 | |||
| No | 1 | ||
| Yes | 0.966 | 0 | 0 |
| Smoking 1 * depression 2 | |||
| No | 1 | ||
| Yes | <0.001 | 3.17 | (2.76–3.64) |
| Smoking 1 * diabetes 3 | |||
| No | 1 | ||
| Yes | <0.001 | 0.21 | (0.10–0.44) |
| Depression 2 * diabetes 3 | . | ||
| No | 1 | ||
| Yes | <0.001 | 3.13 | (2.67–3.66) |
| Constant | 0 | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shelke, G.S.; Marwaha, R.; Shah, P.; Challa, S.N. Impact of Prenatal Health Conditions and Health Behaviors in Pregnant Women on Infant Birth Defects in the United States Using CDC-PRAMS 2018 Survey. Pediatr. Rep. 2023, 15, 197-208. https://doi.org/10.3390/pediatric15010015
Shelke GS, Marwaha R, Shah P, Challa SN. Impact of Prenatal Health Conditions and Health Behaviors in Pregnant Women on Infant Birth Defects in the United States Using CDC-PRAMS 2018 Survey. Pediatric Reports. 2023; 15(1):197-208. https://doi.org/10.3390/pediatric15010015
Chicago/Turabian StyleShelke, Girish Suresh, Rochisha Marwaha, Pankil Shah, and Suman N. Challa. 2023. "Impact of Prenatal Health Conditions and Health Behaviors in Pregnant Women on Infant Birth Defects in the United States Using CDC-PRAMS 2018 Survey" Pediatric Reports 15, no. 1: 197-208. https://doi.org/10.3390/pediatric15010015