
Parents’ Evaluation of Developmental Status and Strength and Difficulties Questionnaire as Screening Measures for Children in India: A Scoping Review

Abstract
:1. Introduction
2. Objective and Research Question for the Scoping Review
3. Inclusion and Exclusion Criteria
3.1. Population
3.2. Concepts
3.3. Context
3.4. Types of Sources
4. Search Strategy
4.1. Pre-Identification Process
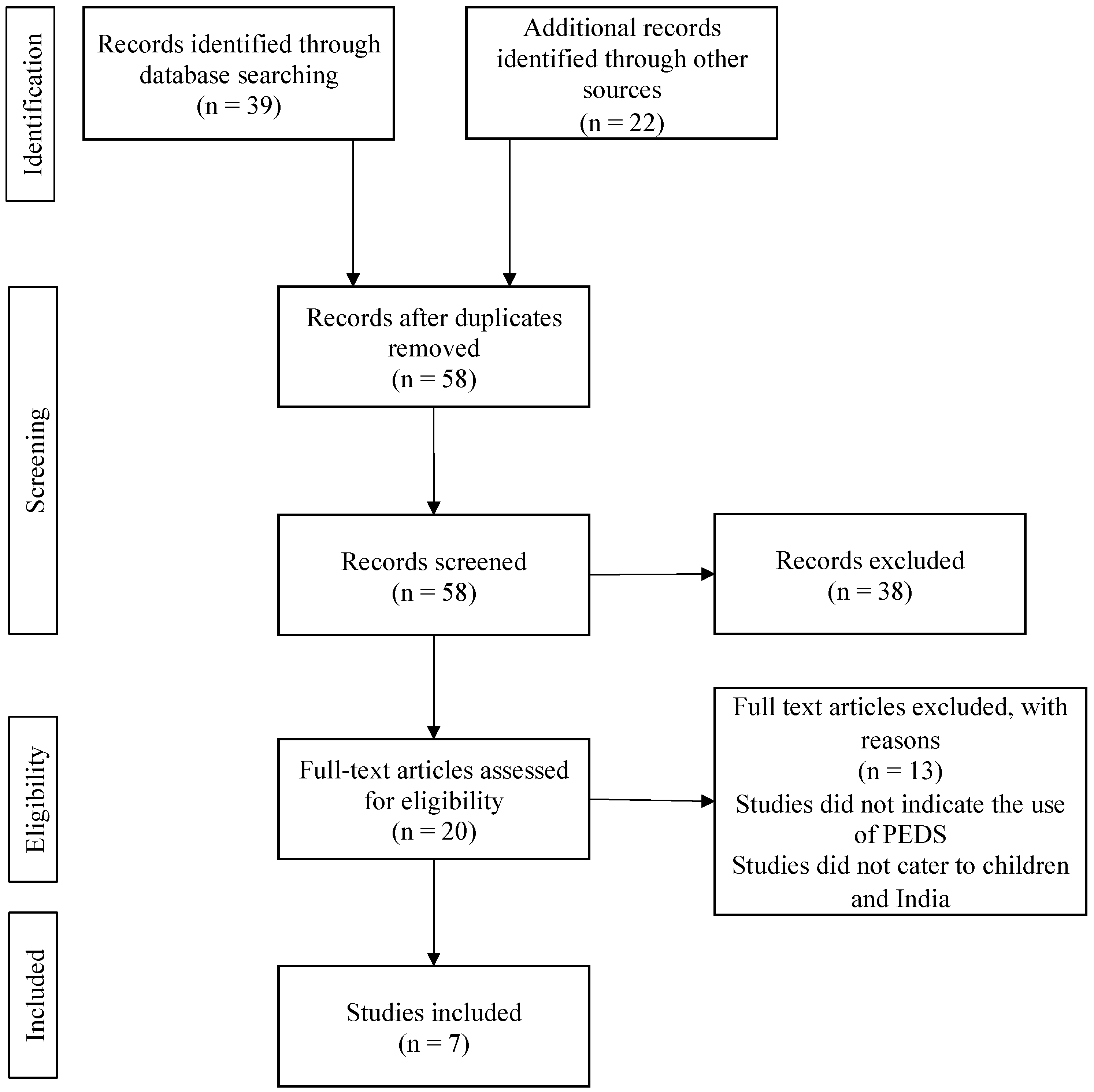
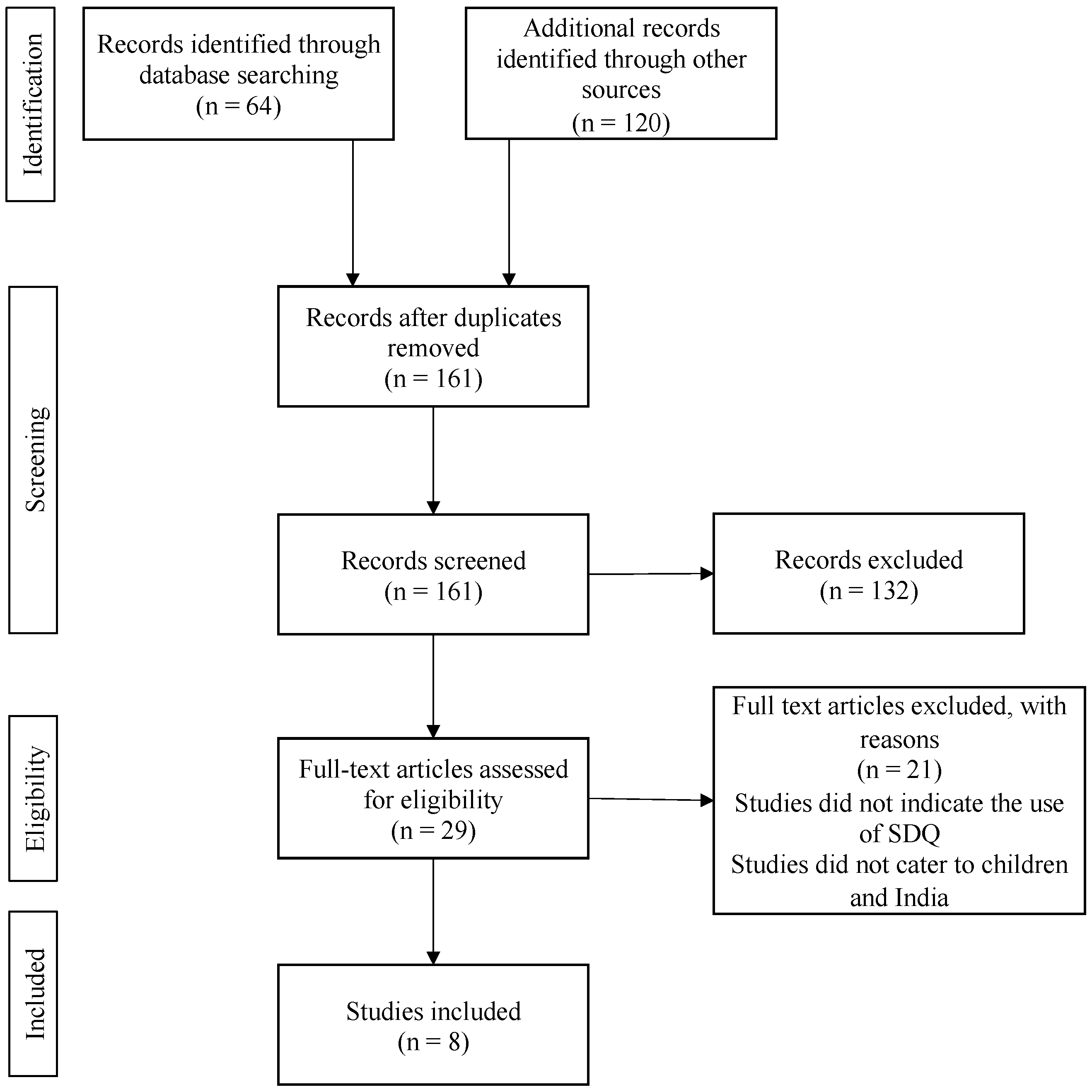
4.2. Identification Stage
4.3. Screening Stage
4.4. Eligibility Stage
4.5. Final Screening Stage
5. Data Extraction Process
6. Results and Discussion of the Scoping Review
7. PEDS and PEDS:DM
8. SDQ
9. Summary
9.1. Limitations of the Existing Research
9.2. Strengths, Limitations, and Implications of this Scoping Review
10. Conclusions
11. Implications for Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Research Ethics
Appendix A

{kind=link}
{kind=link}
| Background Information | |
| Author and Date of Publication | |
| Article Type | |
| Type | |
| City/State | |
| Aim of the Study | |
| Sample | |
| Number of Participants | |
| Age Range | |
| Setting and Measures used | |
| Results | |
| Main Results | |
| Key Findings | |
Appendix B
| SECTION | ITEM | PRISMA-ScR CHECKLIST ITEM | REPORTED ON PAGE # |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a scoping review. | Page 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | Page 2 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | Page 5 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | Page 7 |
| METHODS | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | OSF |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | Page 8 |
| Information sources * | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources) as well as the date the most recent search was executed. | Page 8 |
| Search | 8 | Present the full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | Page 8–10 |
| Selection of sources of evidence † | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | Page 8–10 |
| Data charting process ‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | Page 10–13 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | Page 13 |
| Critical appraisal of individual sources of evidence § | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | - |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | Page 11–12 |
| RESULTS | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | Page 16–18 and 23–25 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted, and provide the citations. | Page 16–18 and 23–25 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | - |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | Page 16–18 and 23–25 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | Page 26 |
| DISCUSSION | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | Page 13–15 and 19–22 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | Page 26–27 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | Page 27–28 |
| FUNDING | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | N.A. |
References
- Zablotsky, B.; Black, L.I.; Maenner, M.J.; Schieve, L.A.; Danielson, M.L.; Bitsko, R.H.; Boyle, C.A. Prevalence and trends of developmental disabilities among children in the United States: 2009–2017. Pediatrics 2019, 144, e20190811. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, G.; Couch, M.A.; Iacono, T. Health issues for adults with developmental disability. Res. Dev. Disabil. 2002, 23, 422–445. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR), 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2022. [Google Scholar]
- International Classification of Diseases, Eleventh Revision (ICD-11); World Health Organization: Geneva, Switzerland, 2021; Available online: https://icd.who.int/browse11/lm/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f605267007 (accessed on 9 November 2021).
- Denham, S.A.; Brown, C. “Plays Nice with Others”: Social-Emotional Learning and Academic Success. Early Educ. Dev. 2010, 21, 652–680. [Google Scholar] [CrossRef]
- Ryan-Enright, T.; O’Connor, R.; Bramham, J.; Taylor, L.K. A systematic review of autistic children’s prosocial behaviour. Res. Autism Spectr. Disord. 2022, 98, 102023. [Google Scholar] [CrossRef]
- Sachidananda Kamath, S. Childhood disability—Our responsibility. Indian Pediatr. 2015, 52, 13–14. [Google Scholar] [CrossRef]
- Datta, P.; Ganguly, S.; Roy, B.N. The prevalence of behavioral disorders among children under parental care and out of parental care: A comparative study in India. Int. J. Pediatr. Adolesc. 2018, 5, 145–151. [Google Scholar] [CrossRef]
- Juneja, M.; Mohanty, M.; Jain, R.; Ramji, S. Ages and Stages Questionnaire as a screening tool for developmental delay in Indian children. Indian Pediatr. 2012, 49, 457–461. [Google Scholar] [CrossRef]
- Mukherjee, S.B.; Aneja, S.; Krishnamurthy, V.; Srinivasan, R. Incorporating developmental screening and surveillance of young children in office practice. Indian Pediatr. 2014, 51, 627–635. [Google Scholar] [CrossRef]
- Mukherjee, S.B.; Mukherjee, S.; Ghosh, S.; Singh, A. Providing services for Indian children with developmental delay and disabilities in the community: Rashtriya Bal Suraksha Karyakram. Indian Pediatr. 2021, 58, 73–79. [Google Scholar] [CrossRef]
- Mayank, S. Rashtriya Bal Swasthya Karyakram: A Novel Way of Harnessing the Potential of Ayurvedic Graduates. Int. J. Health Sci. Res. 2015, 5, 396–401. [Google Scholar]
- Ministry of Health and Family Welfare. Rashtriya Bal Swasthya Karyakram (RBSK). 2013. Available online: https://rbsk.gov.in/RBSKLive/ (accessed on 15 June 2020).
- Hema Priya, A.S.; Arun Krishna, S.R.; Jasmine, S.S. Insights of Rashtriya Bal Swasthya Karyakram: A strength, weaknesses, opportunities, and threats analysis. Int. J. Community Med. Public Health 2022, 9, 4279–4282. [Google Scholar]
- Kingdon, G.G. The private schooling phenomenon in India: A review. J. Dev. Stud. 2020, 56, 1795–1817. [Google Scholar] [CrossRef] [Green Version]
- Meisels, S. Developmental screening in early childhood: The interaction of research and social policy. Annu. Rev. Public Health. 1988, 9, 527–550. [Google Scholar] [CrossRef]
- Rydz, D.; Shevell, M.I.; Majnemer, A.; Oskoui, M. Topical Review: Developmental Screening. J. Child Neurol. 2005, 20, 4–21. [Google Scholar] [CrossRef] [PubMed]
- Fischer, V.J.; Morris, J.; Martines, J. Developmental screening tools: Feasibility of use at primary healthcare level in low- and middle-income settings. J. Health Popul. Nutr. 2014, 32, 314–326. [Google Scholar] [CrossRef]
- Madaan, P.; Saini, L.; Sondhi, V. Development Assessment Scale for Indian Infants: A Systematic Review and Perspective on Dwindling Cutoffs. Indian J. Pediatr. 2021, 88, 918–920. [Google Scholar] [CrossRef]
- Lancaster, G.A.; McCray, G.; Kariger, P.; Dua, T.; Titman, A.; Chandna, J.; McCoy, D.; Abubakar, A.; Hamadani, J.D.; Fink, G.; et al. Creation of the WHO Indicators of Infant and Young Child Development (IYCD): Metadata synthesis across 10 countries. BMJ Glob. Health 2018, 3, e000747. [Google Scholar] [CrossRef] [Green Version]
- Gladstone, M.J.; Lancaster, G.A.; Jones, A.P.; Maleta, K.; Mtitimila, E.; Ashorn, P.; Smyth, R.L. Can Western developmental screening tools be modified for use in a rural Malawian setting? Arch. Dis. Child. 2008, 93, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Gridley, N.; Blower, S.; Dunn, A.; Bywater, T.; Bryant, M. Psychometric Properties of Child (0–5 Years) Outcome Measures as used in Randomized Controlled Trials of Parent Programs: A Systematic Review. Clin. Child Fam. Psychol. Rev. 2019, 22, 388–405. [Google Scholar] [CrossRef] [Green Version]
- Durkin, M.S.; Elsabbagh, M.; Barbaro, J.; Gladstone, M.; Happe, F.; Hoekstra, R.A.; Lee, L.-C.; Rattazzi, A.; Stapel-Wax, J.; Stone, W.L.; et al. Autism screening and diagnosis in low resource settings: Challenges and opportunities to enhance research and services worldwide. Autism Res. 2015, 8, 473–476. [Google Scholar] [CrossRef] [Green Version]
- Bayley, N. Bayley Scales of Infant Development, 2nd ed.; Psychological Corporation: San Antonio, TX, USA, 1993. [Google Scholar]
- Squires, J.; Potter, L.; Bricker, D. The ASQ User’s Guide for the Ages & Stages Questionnaires: A Parent-Completed, Child-Monitoring System; Paul H Brookes Publishing: Baltimore, MD, USA, 1995. [Google Scholar]
- Ertem, I.O.; Dogan, D.G.; Gok, C.G.; Kizilates, S.U.; Caliskan, A.; Atay, G.; Vatandas, N.; Karaaslan, T.; Baskan, S.G.; Cicchetti, D.V. A guide for monitoring child development in low-and middle-income countries. Pediatrics 2008, 121, e581–e589. [Google Scholar] [CrossRef] [PubMed]
- Glascoe, F.P. Collaborating with Parents: Using Parents’ Evaluation of Developmental Status to Detect and Address Developmental and Behavioral Problems; Ellsworth & Vandermeer Press: Austin, TX, USA, 1998. [Google Scholar]
- Eyberg, S.M.; Ross, A.W. Assessment of child behavior problems: The validation of a new inventory. J. Clin. Child Psychol. 1978, 7, 113–116. [Google Scholar] [CrossRef]
- Achenbach, T.M. Child Behavior Checklist for Ages 2–3; University of Vermont, Centre for Children, Youth, and Families: Burlington, VT, USA, 1992. [Google Scholar]
- Thorlacius, Ö.; Gudmundsson, E. The Effectiveness of the Children’s Emotional Adjustment Scale (CEAS) in Screening for Mental Health Problems in Middle Childhood. Sch. Ment. Health 2018, 11, 400–412. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry Allied Discip. 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Barnes, K.E.; Stark, A. The Denver Development Screening Test. A normative study. Am. J. Public Health 1975, 65, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Boggs, D.; Milner, K.M.; Chandna, J.; Black, M.; Cavallera, V.; Dua, T.; Fink, G.; Ashish, K.; Grantham-McGregor, S.; Hamadani, J. Rating early child development outcome measurement tools for routine health programme use. Arch. Dis. Child. 2019, 104, S22–S33. [Google Scholar] [CrossRef] [Green Version]
- Kaptein, S.; Jansen, D.; Vogels, A.; Reijneveld, S. Mental health problems in children with intellectual disability: Use of the Strengths and Difficulties Questionnaire. J. Intellect. Disabil. Res. 2008, 52, 125–131. [Google Scholar] [CrossRef]
- Goldfeld, S.; Yousafzai, A. Monitoring tools for child development: An opportunity for action. Lancet Glob. Health 2018, 6, e232–e233. [Google Scholar] [CrossRef] [Green Version]
- Limbos, M.M.; Joyce, D.P. Comparison of the ASQ and PEDS in screening for developmental delay in children presenting for primary care. J. Dev. Behav. Pediatr. 2011, 32, 499–511. [Google Scholar] [CrossRef] [Green Version]
- Marlow, M.; Servili, C.; Tomlinson, M. A review of screening tools for the identification of autism spectrum disorders and developmental delay in infants and young children: Recommendations for use in low- and middle-income countries. Autism Res. 2019, 12, 176–199. [Google Scholar] [CrossRef]
- Glascoe, F.P. Parents’ Concerns About Children’s Development: Prescreening Technique or Screening Test? Pediatrics 1997, 99, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Chunsuwan, I.; Hansakunachai, T.; Pornsamrit, S. Parent Evaluation of Developmental Status (PEDS) in screening: The Thai experience. Pediatr. Int. 2016, 58, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Wong, B.; Grundy, S.; Tshering, L.; Tshering, K.; Mateen, F.J. Assessment of a neuro-developmental screening tool in children in Bhutan. Gates Open Res. 2019, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Shahshahani, S.; Vameghi, R.; Sajedi, F.; Biglarian, A. Comparing the Results of Developmental Screening of 4 to 60-Month-Old Children in Tehran Using Parents Evaluation of Developmental Status and Ages and Stages Questionnaires. Iran. J. Pediatr. 2016, 27, e6179. [Google Scholar] [CrossRef]
- Malhi, P.; Singhi, P. Accuracy of parents’ concerns in identifying children with developmental problems. Stud. Psychol. 2001, 43, 313–320. [Google Scholar]
- Malhi, P.; Singhi, P. Role of Parents’ Evaluation of Developmental Status in Detecting Developmental Delay in Young Children. Indian Pediatr. 2002, 39, 271–275. [Google Scholar]
- Adeniyi, Y.; Omigbodun, O. Psychometric Properties of the Self-report Strengths and Difficulties Questionnaire (SDQ) in a Nigerian Adolescents Sample. Int. Neuropsychiatr. Dis. J. 2017, 10, 1–9. [Google Scholar] [CrossRef]
- Dang, H.-M.; Nguyen, H.; Weiss, B. Incremental validity of the Child Behavior Checklist (CBCL) and the Strengths and Difficulties Questionnaire (SDQ) in Vietnam. Asian J. Psychiatry 2017, 29, 96–100. [Google Scholar] [CrossRef]
- Dursun, O.B.; Öğütlü, H.; Esın, İ.S. Psychometric Properties of Turkish Version of the Strength and Difficulties Questionnaire for Age 2–4. Noro Psikiyatr. Ars. 2020, 57, 44–49. [Google Scholar] [CrossRef]
- Woerner, W.; Nuanmanee, S.; Becker, A.; Wongpiromsarn, Y.; Mongkol, A. Normative data and psychometric properties of the Thai version of the Strengths and Difficulties Questionnaire (SDQ). J. Ment. Health Thail. 2011, 19, 42–57. [Google Scholar]
- Michelson, D.; Malik, K.; Parikh, R.; Weiss, H.A.; Doyle, A.M.; Bhat, B.; Sahu, R.; Chilhate, B.; Mathur, S.; Krishna, M.; et al. Effectiveness of a brief lay counsellor-delivered, problem-solving intervention for adolescent mental health problems in urban, low-income schools in India: A randomised controlled trial. Lancet Child Adolesc. Health 2020, 4, 571–582. [Google Scholar] [CrossRef]
- Phillips Owen, J.A.; Mirza, K.A.H.; Goodman, R. Validating Screening Tool in Malayalam for Mental Disorders. Indian J. Pediatr. 2015, 82, 595–600. [Google Scholar] [CrossRef]
- Singh, K.; Junnarkar, M.; Sharma, S. Anxiety, stress, depression, and psychosocial functioning of Indian adolescents. Indian J. Pediatr. 2015, 57, 367–374. [Google Scholar] [CrossRef]
- Glascoe, F.P. Re: Parents’ Evaluation of Developmental Status. J. Paediatr. Child Health 2003, 41, 615–616. [Google Scholar] [CrossRef] [PubMed]
- Glascoe, F.P. Summary of PEDS Research from Page Glascoe, PhD Collaboratingwith Parents, 2nd ed.; PEDStest.com LLC: Nolensville, TN, USA, 2013; Available online: https://pedstest.com/static/research/summaryOfPedsResearchByGlascoe.html (accessed on 1 November 2019).
- Brothers, K.B.; Glascoe, F.P.; Robertshaw, N.S. PEDS: Developmental Milestones—An Accurate Brief Tool for Surveillance and Screening. Clin. Pediatr. 2008, 47, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, S.; Halvorsen, M.B. The Strengths and Difficulties Questionnaire self-report-, parent-, and teacher version in children with intellectual and developmental disabilities. Res. Dev. Disabil. 2022, 123, 104194. [Google Scholar] [CrossRef]
- Camden, C.; Wilson, B.; Kirby, A.; Sugden, D.; Missiuna, C. Best practice principles for management of children with developmental coordination disorder (DCD): Results of a scoping review. Child Care Health Dev. 2015, 41, 147–159. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef] [Green Version]
- Poon, J.K.; Larosa, A.C.; Shashidhar Pai, G. Developmental delay: Timely identification and assessment. Indian Pediatr. 2010, 47, 415–422. [Google Scholar] [CrossRef]
- Woolfenden, S.; Eapen, V.; Williams, K.; Hayen, A.; Spencer, N.; Kemp, L. A systematic review of the prevalence of parental concerns measured by the Parents’ Evaluation of Developmental Status (PEDS) indicating developmental risk. BMC Pediatr. 2014, 14, 231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bele, S.D.; Bodhare, T.N.; Valsangkar, S.; Saraf, A. An epidemiological study of emotional and behavioral disorders among children in an urban slum. Psychol Health Med. 2013, 18, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Chari, U.; Hirisave, U. Psychological health of young children undergoing treatment for Acute Lymphoblastic Leukaemia: A cross-sectional study. J. Indian Assoc. Child Adolesc. Ment. Health 2020, 16, 66–79. [Google Scholar] [CrossRef]
- Kiron, S. D Dimer as a Diagnostic Tool to Diagnose la Thrombus in Rheumatic Mitral Stenosis (1). Catch Them Young: Can Younger Age Pediatric Cardiac Interventions Alter the Psychosocial Impact of Congenital Heart Diseases on Growing Children. Unpublished. Master’s Thesis, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Kerala, India, 2012. [Google Scholar]
- Malhotra, S.; Kohli, A.; Kapoor, M.; Pradhan, B. Incidence of childhood psychiatric disorders in India. Indian J. Psychiatry 2009, 51, 101–107. [Google Scholar] [CrossRef]
- Trinh, T.-A. Mental Health Impacts of Child Labour: Evidence from Vietnam and India. J. Dev. Stud. 2020, 56, 2251–2265. [Google Scholar] [CrossRef]
- Huynh, H.V.; Limber, S.P.; Gray, C.L.; Thompson, M.P.; Wasonga, A.I.; Vann, V.; Itemba, D.; Eticha, M.; Madan, I.; Whetten, K. Factors affecting the psychosocial well-being of orphan and separated children in five low- and middle-income countries: Which is more important, quality of care or care setting? PLoS ONE 2019, 14, e0218100. [Google Scholar] [CrossRef] [Green Version]
- Anita, M.; Maninder, S. Neurobehavioral comorbidities in children with epilepsy. J. Neurol. Neurophysiol. 2016, 7, 1–5. [Google Scholar] [CrossRef]
- Galab, S.; Reddy, M.G.; Antony, P.; McCoy, A.; Ravi, C.; Raju, D.S.; Mayuri, K.; Reddy, P.P. Young Lives Preliminary Country Report; Save the Children Organization: Gurugram, India, 2003. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]


| Population | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Author | Article Type | Design | City in India | Aim/Purpose | Size | Age Range | Setting and Measures Used | Main Results | Key Findings |
| Marlow, Servili, and Tomlinson, 2019 [37] | Peer reviewed | Systematic review | Chandigarh, India (Reference to Malhi and Singhi, 2001 study) | Identify current screening instruments for DD and ASD, create screening profiles, and provide recommendation for screening in LMIC. | A sample of more than 300 participants for each instrument | 0–7 years | Search Strategy of the tools (2014–2017); Inclusion and exclusion criteria and specific criteria for screening instruments. | The review identified 10 screening tools suitable to screen children in LMIC for ASD and 7 screening tools for DD. | PEDS is adapted and able to detect DD in LMIC. |
| Woolfenden et al., 2014 [59] | Peer reviewed | Systematic review | Chandigarh, India (Reference to Malhi and Singhi, 2001 study) | To understand the worldwide prevalence of parental concerns measured by PEDS that indicated developmental risks and associated risk factors. | 20 to 54,602 | Less than 1 month to 7 years and 11 months | Search Strategy of PEDS; Inclusion and exclusion criteria for study participants and review process. | 14% of parents raised concerns associated with a high risk of developmental problems, and 19% raised concerns about a moderate risk for developmental problems. | Eight studies of PEDS were conducted in low- and medium-income countries (including India). |
| Malhi and Singhi, 2001 [42] | Peer reviewed | Diagnostic test accuracy | Chandigarh, India | To identify the range of concerns that parents have about their child’s development and its relationship to the child’s developmental status. | 55 parent–child dyads | 6 to 60 months | Patients recruited through outpatient paediatric care in a tertiary care teaching hospital. | 38% of parents indicated no concerns, and 20% raised non-significant developmental concerns about their child’s development. From these children, 90.6% passed the development screening. | Of the parents who expressed one or more significant developmental concerns about their child, 47.8% of these children failed the screening. In addition, 43% of the parents whose children failed developmental screening expressed medical concerns, 35.7% reported expressive language concerns, and 28% indicated global/cognitive concerns. |
| Malhi and Singhi, 2002 [43] | Peer reviewed | Diagnostic test accuracy | Chandigarh, India | To identify the range of concerns parents have about their child’s development and evaluate the relationship between parent concern and the child’s developmental status. | 79 parent–child dyads | 24 to 60 months | Patients recruited through outpatient paediatric care in a tertiary care teaching hospital; Two questionnaires used: PEDS and Developmental Profile II. | Parents’ concerns about the developmental milestones of their child were moderately sensitive predictors of DD in children between 2 and 5 years. | The authors advised against using the PEDS as a substitute for standardized developmental screening measures because its specificity and sensitivity were lower than those reported by the US. The PEDS can be used as a pre-screening tool to find children who might need comprehensive developmental screening in outpatient settings. |
| Glascoe, Malhi, and Singhi, 2001 and 2003 [42,51] | Grey literature | Letter to the authors | N.A. | 79 parent–child dyads | 24 to 60 months | Patients recruited through outpatient paediatric care in a tertiary care teaching hospital; Two questionnaires used: PEDS and Developmental Profile II. | Parents’ concerns about the developmental milestones of their child were moderately sensitive predictors of DD in children between 2 and 5 years. | The author’s letter noted that the scoring method utilized in the paper was not clear. Given that DP-II has a propensity to overidentify developmental issues, the concurrent test utilized to evaluate the accuracy of PEDS is questionable. PEDS would gain from the use of a different scoring system. | |
| Poon, Larosa, and Pai, 2010 [58] | Peer reviewed | Text and opinion study | The paper discusses the prevalence of DD in children and recent literature regarding the benefits of early identification and benefits of developmental screening and surveillance. | Not specified | N.A. | The review’s key conclusions stated that it is important to pay attention to parents’ worries while maintaining regular surveillance, integrating routine screening, making early referrals to paediatricians and therapists, and offering early intervention services and therapies that have been proven to be successful regardless of the medical diagnosis. | PEDS has been used in India. The tool has been translated to over 10 different languages and is completed by parents. | ||
| Mukherjee et al., 2014 [10] | Peer reviewed | Text and opinion Study | India | The aim of the article was to review existing tools for children under the age of five that were validated in India and to provide a purposed paradigm for developmental screening in office practice. | Not specified | Under the age of 5 years | N.A. | Tools developed in India lack psychometric properties and were developed by healthcare workers, and the screening tools developed in the US are costly and not easily accessible. | PEDS has been found reliable in developing countries. However, there is limited research from India. |
| Population | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Author | Article Type | Design | City in India | Aim/Purpose | Size | Age Range | Setting and Measures Used | Outcome | Key Findings |
| Bele et al., 2013 [60] * | Peer reviewed | Cross-sectional study | Gauthaminagar in Karimnagar district of Andhra Pradesh | To estimate the prevalence of emotional and behavioural disorders using standardised instruments among children in urban slums. | N = 370 | 5–10 years | Emotional and behavioural problems among children were evaluated using the Strength and Difficulties Questionnaire (SDQ), and depression was assessed using Patient Health Questionnaire (PHQ-9). | On at least one SDQ domain, 22% of the children scored abnormally. The children’s behavioural issues and poorer academic achievement were found to be significantly correlated. | SDQ scores and mean values for affected and unaffected groups were compared, and a significant variance was found in the total problems score in the affected group (borderline and abnormal score) compared to the unaffected group. |
| Malhotra et al., 2009 [63] ** | Peer reviewed | Prevalence study/Longitudinal study | Chandigarh, India | To establish the incidence of psychiatric disorders in school children in India. | N = 873 | 4–11 years | Rutter B (teachers rating), Childhood Psychopathology Measurement Schedule, Temperament Measurement Scale, Parent Handling Questionnaire, Parent Interview Schedule, Life event scale for Indian children, and SDQ. | A total of 20 of the 186 children that were monitored had a psychological condition. In terms of age, gender, and psychological (temperament, parental handling, life stress, and IQ) factors at baseline, children with the disorder at follow-up did not vary from those without it. | Children scoring above a cut-off score on the SDQ (≥14) were clinically examined by a psychiatrist at home or at the clinic. |
| Trinh, 2020 [64] * | Peer reviewed | Longitudinal study | India and Vietnam | To study the mental health impact of child labour. | N = 978 children in Vietnam and 956 children in India | 7–9 years | SDQ to measure child mental health and child participation in the labour market was assessed by understanding if the child has undertaken any activity to earn money. | Child labour did not uniformly affect the five dimensions of the SDQ. Compared to children who did not work, those who participated in the labour market in Vietnam were more likely to experience conduct problems, hyperactivity, peer issues, and less prosocial behaviour. The outcomes for working children in Vietnam were noticeably lower regarding peer issues and less prosocial behaviour. Hyperactivity and a decline in prosocial behaviour were significantly linked with child labour and mental health symptoms in India. | In the five scales of the SDQ, peer problems and prosocial behaviour were found to be significantly impacted by working in both countries. |
| Anita et al., 2016 [66] ** | Peer reviewed | Prospective case control study | Mumbai, India | To study the prevalence, type, and impact of neurobehavioral disorders in children with and without epilepsy. | N = 222 | 5–12 years | SDQ was assessed in four groups: epilepsy, epilepsy control, irregular school attendance, and school dropout. | The study revealed that 14.4% of children with epilepsy during schooling had learning problems, and 10.3% had behavioural problems compared to non-epileptics. In addition, 63% of the people with epilepsy had emotional difficulties and abnormal conduct scores. High hyperactivity, poor peer relations, and poor pro-social behaviour led to low school attendance in 35% of epileptic patients. | Screening of cases and controls with the SDQ-P (parent version) was conducted, and the total difficulties score was abnormal in 39% of cases and 7.9% of controls, and it was normal in 44.5% of cases and 88.9% of controls. |
| Chari and Hirisave, 2020 [61] * | Peer reviewed | Cross-sectional study | Bangalore, India | To examine the psychological health of young children undergoing treatment for acute lymphoblastic leukaemia. | N = 40 | 4–8 years | SDQ to assess psychiatric disturbances, feeling cards to examine the subject’s current emotional state, and teddy bear’s picnic to examine personal construct. | Children with ALL (acute lymphoblastic leukaemia) were reported on SDQ to display more behavioural disturbances. | On the SDQ, there were significant differences between groups in total difficulties, conduct, and peer problems. However, median scores were in the normative range. Children with ALL demonstrated more disruptive behaviours and peer problems than healthy children. |
| Galab et al., 2003 [67] *** | Grey literature | Literature review | Andhra Pradesh | The report provides a brief literature on childhood poverty in Andhra Pradesh in India and explains how national policies have impacted childhood poverty in that state. | N = 3000 | 1–8 years | The SDQ was used to assess the mental health of children of 8 years of age. | The Young Lives results reported that nearly 20% of children were classified as abnormal and 20% as borderline. However, the authors recommended that these results should be interpreted with caution since the SDQ has not been validated in Andhra Pradesh and normative data is not available. | Previously, the SDQ had not been validated in Andhra Pradesh, and normative data were unavailable. The study was the first to use the SDQ in Andhra Pradesh, and the findings suggest that child mental health issues may be a potential problem, especially in the rural areas of Andhra Pradesh, where the prevalence of abnormal cases was over 20%. |
| Huynh et al., 2019 [65] ** | Peer reviewed | Longitudinal study | Five low- and middle-income countries: Battambang District, Cambodia; Nagaland and Hyderabad, India; Bungoma District, Kenya; Kilimanjaro Region, Tanzania; and Addis Ababa, Ethiopia. Children were enrolled between 2006 and 2008 and followed biannually | To examine the psychological wellbeing of orphans and separate children in under-resourced societies in LMIC and to associate quality of care with children’s psychosocial wellbeing. | N = 2013 (923 residential care and 1090 community-based sample) | 6–12 years at baseline; 36 months of follow-up data | Quality of care was assessed using the Child Status Index, and child’s psychosocial wellbeing was assessed using the SDQ. | Child psychosocial well-being across different levels of quality of care showed negligible differences between residential- and community-based care settings, suggesting the critical factor in child well-being is quality of care rather than environment of care. | When the authors controlled the orphan’s gender, status, and age, components of quality of care predicted SDQ total difficulties better than care setting. Mean SDQ total difficulties scores across “high” and “low” quality of care showed differences between care settings to be minimal. There were no meaningful differences in SDQ total difficulties across care settings. Orphans and separated children (OCS) in residential care settings had higher SDQ total difficulties scores than in community-based settings. |
| Kiron, 2012 [62] *** | Grey literature | Cross-sectional study (Project 2) | Sree Chitra Tirunal Institute of Medical Science and Technology, Kerala, India | To analyse whether those children who grow up without being aware of their congenital heart disease have any psychosocial advantage over those children who grow up being aware that they have undergone a major interventional procedure for their congenital heart disease. | N = 242 (only 147 parents responded to SDQ) | Less than 10 years | The SDQ was used to ascertain the impact of CHD in children. | On being assessed with the total difficulties score, children who were aware of their congenital heart disease were at substantial risk of clinically significant problems compared to the other group. | Children not aware of their CHD had significantly lower levels of problems compared to children who were aware and had experienced CHD. In addition, children in the first group were higher in prosocial behaviour compared to the second group. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheel, H.; Suárez, L.; Marsh, N.V. Parents’ Evaluation of Developmental Status and Strength and Difficulties Questionnaire as Screening Measures for Children in India: A Scoping Review. Pediatr. Rep. 2023, 15, 175-196. https://doi.org/10.3390/pediatric15010014
Sheel H, Suárez L, Marsh NV. Parents’ Evaluation of Developmental Status and Strength and Difficulties Questionnaire as Screening Measures for Children in India: A Scoping Review. Pediatric Reports. 2023; 15(1):175-196. https://doi.org/10.3390/pediatric15010014
Chicago/Turabian StyleSheel, Hina, Lidia Suárez, and Nigel V. Marsh. 2023. "Parents’ Evaluation of Developmental Status and Strength and Difficulties Questionnaire as Screening Measures for Children in India: A Scoping Review" Pediatric Reports 15, no. 1: 175-196. https://doi.org/10.3390/pediatric15010014