
Web-Based Exercise Interventions for Children with Neurodevelopmental Disorders
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Selection Process
2.4. Risk of Bias Assessment
2.5. Data Collection Process
3. Results
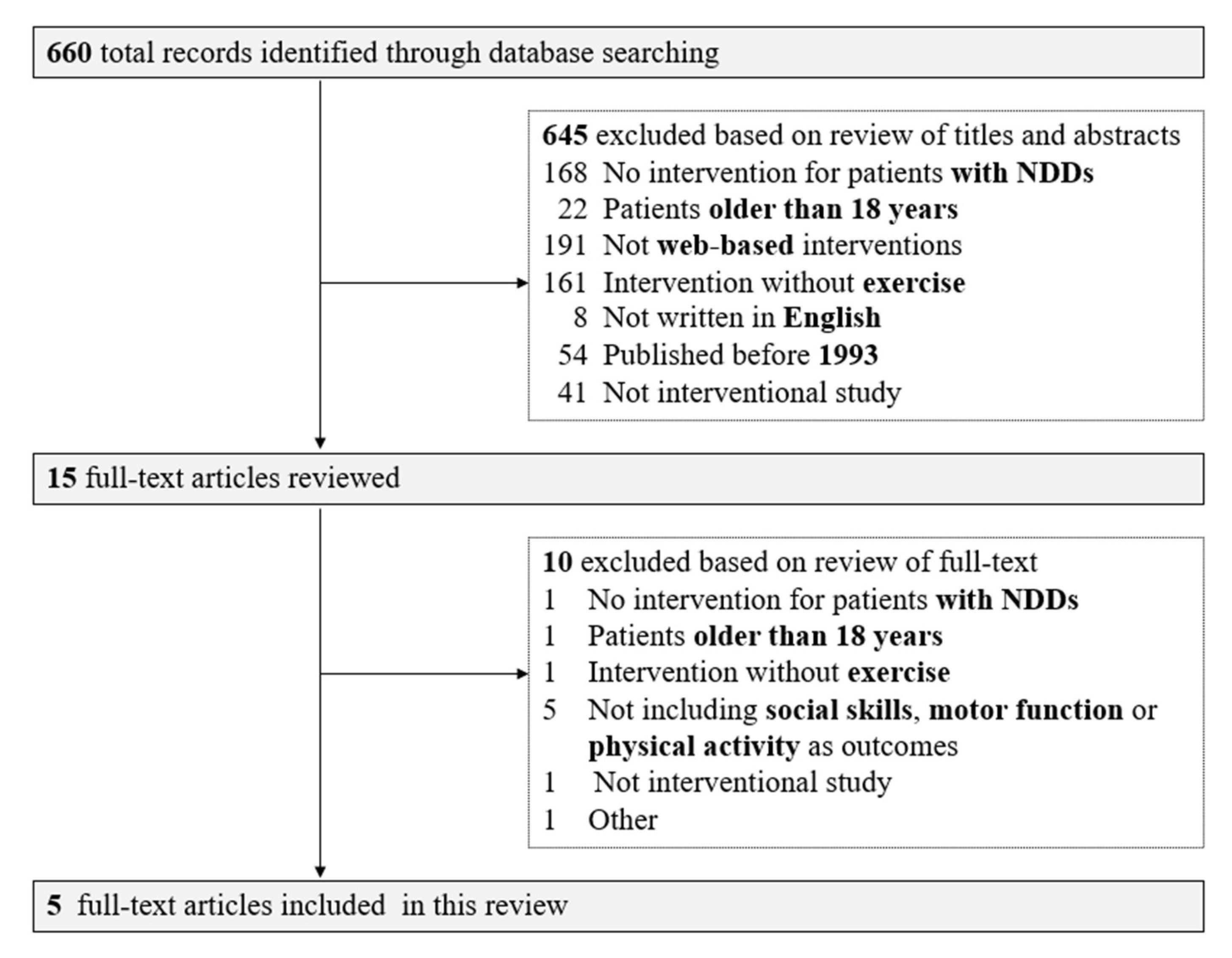
3.1. Results of First and Second Screenings
3.2. Exercise Intervention
3.3. Motor Function
3.4. Executive Function
3.5. Physical Activity
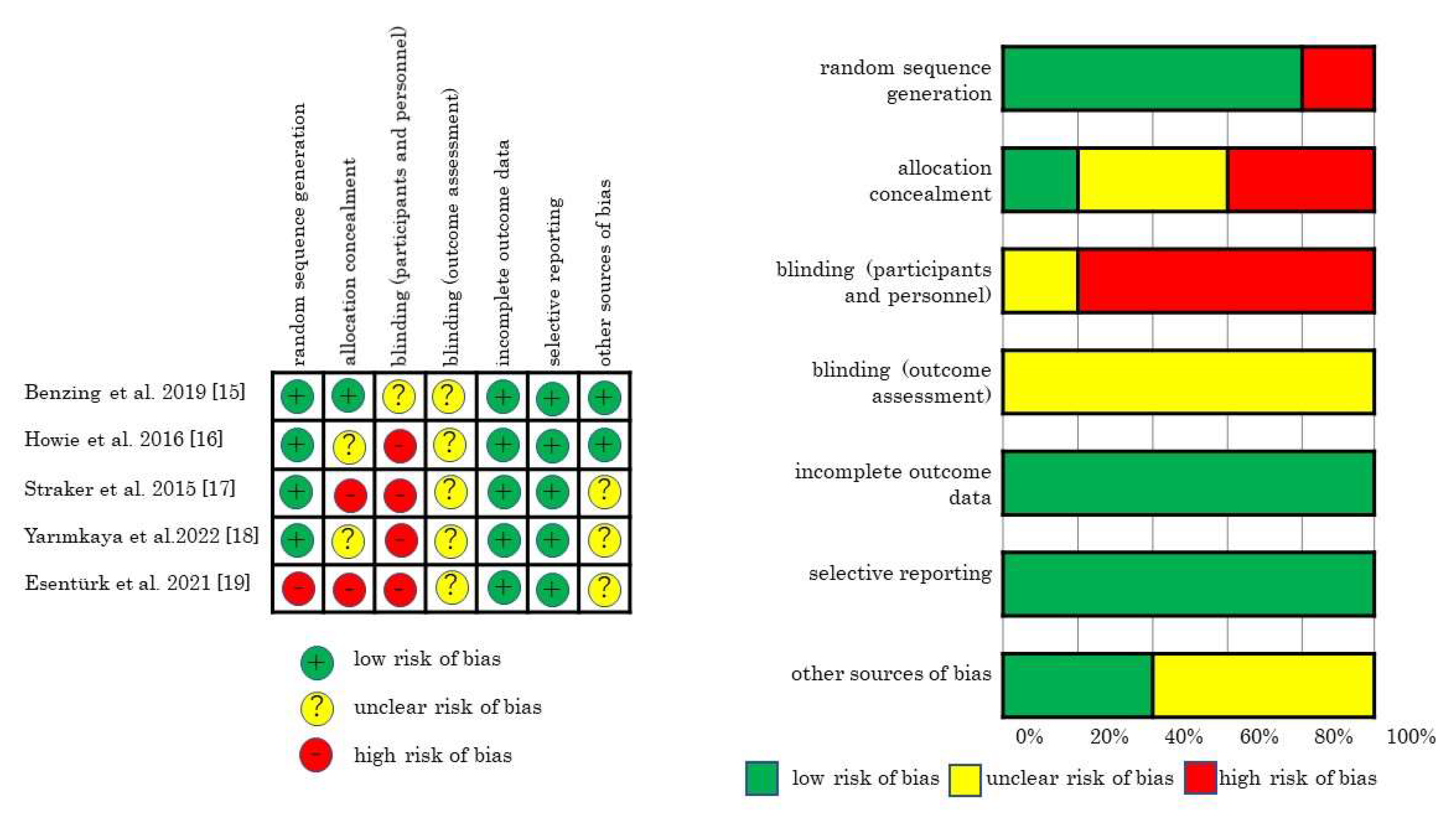
3.6. Risk of Bias in the Studies
4. Discussion
4.1. Brief Summary of This Review
4.2. Comparison with Previous Studies
4.3. Possible Explanations and Implications
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahn, S.; Hwang, S. Cognitive rehabilitation with neurodevelopmental disorder: A systematic review. NeuroRehabilitation 2017, 41, 707–719. [Google Scholar] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Cleaton, M.A.; Kirby, A. Why do we find it so hard to calculate the burden of neurodevelopmental disorders. J. Child Dev. Disord. 2018, 4, 330–338. [Google Scholar]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Ohara, R.; Kanejima, Y.; Kitamura, M.; Izawa, K.P. Association between social skills and motor skills in individuals with autism spectrum disorder: A systematic review. Eur. J. Investig. Health Psychol. Educ. 2019, 10, 276–296. [Google Scholar] [PubMed]
- Healy, S.; Nacario, A.; Braithwaite, R.E.; Hopper, C. The effect of physical activity interventions on youth with autism spectrum disorder: A meta-analysis. Autism Res. 2018, 11, 818–833. [Google Scholar] [CrossRef]
- Cerrillo-Urbina, A.J.; García-Hermoso, A.; Sánchez-López, M.; Pardo-Guijarro, M.J.; Santos Gómez, J.L.; Martínez-Vizcaíno, V. The effects of physical exercise in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis of randomized control trials. Child Care Health Dev. 2015, 41, 779–788. [Google Scholar] [PubMed]
- Khan, K.; Hall, C.L.; Davies, E.B.; Hollis, C.; Glazebrook, C. The effectiveness of web-based interventions delivered to children and young people with neurodevelopmental disorders: Systematic review and meta-analysis. J. Med. Internet Res. 2019, 21, e13478. [Google Scholar] [CrossRef] [PubMed]
- Masi, A.; Diaz, A.M.; Tully, L.; Azim, S.I.; Woolfenden, S.; Efron, D.; Eapen, V. Impact of the COVID-19 pandemic on the well-being of children with neurodevelopmental disabilities and their parents. J. Paediatr. Child Health. 2021, 57, 631–636. [Google Scholar] [PubMed]
- Zhang, J.; Shuai, L.; Yu, H.; Wang, Z.; Qiu, M.; Lu, L.; Cao, X.; Xia, W.; Wang, Y.; Chen, R. Acute stress, behavioural symptoms and mood states among school-age children with attention-deficit/hyperactive disorder during the COVID-19 outbreak. Asian J. Psychiatr. 2020, 51, 102077. [Google Scholar] [PubMed]
- Althiabi, Y. Attitude, anxiety and perceived mental health care needs among parents of children with Autism Spectrum Disorder (ASD) in Saudi Arabia during COVID-19 pandemic. Res. Dev. Disabil. 2021, 111, 103873. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 5th ed.; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011, 343, d5928. [Google Scholar] [PubMed]
- Benzing, V.; Schmidt, M. The effect of exergaming on executive functions in children with ADHD: A randomized clinical trial. Scand. J. Med. Sci. Sports 2019, 29, 1243–1253. [Google Scholar] [CrossRef] [PubMed]
- Howie, E.K.; Campbell, A.C.; Straker, L.M. An active video game intervention does not improve physical activity and sedentary time of children at-risk for developmental coordination disorder: A crossover randomized trial. Child Care Health Dev. 2016, 42, 253–260. [Google Scholar] [PubMed]
- Straker, L.; Howie, E.; Smith, A.; Jensen, L.; Piek, J.; Campbell, A. A crossover randomised and controlled trial of the impact of active video games on motor coordination and perceptions of physical ability in children at risk of Developmental Coordination Disorder. Hum. Mov. Sci. 2015, 42, 146–160. [Google Scholar] [PubMed]
- Yarımkaya, E.; Esentürk, O.K.; İlhan, E.L.; Kurtipek, S.; Işım, A.T. Zoom-delivered Physical activities can increase perceived physical activity level in children with autism spectrum disorder: A pilot study. J. Dev. Phys. Disabil. 2022, 3, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Esentürk, O.K.; Yarımkaya, E. WhatsApp-based physical activity intervention for children with autism spectrum disorder during the novel Coronavirus (COVID-19) pandemic: A feasibility trial. Adapt. Phys. Activ. Q. 2021, 38, 569–584. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.N.; Crawford, S.G. The developmental coordination questionnaire 2007 (DCDQ’07). In Administrative Manual for the DCDQ’07 with Psychometric Properties; Alberta Health Services: Calgary, Canada, 2012. [Google Scholar]
- Schopler, E.; Wellman, G.J.; Love, S.R. Childhood Autism Rating Scale, 2nd ed.; Western Psychological Services: Torrance, CA, USA, 2010. [Google Scholar]
- Robins, D.L.; Fei, D.; Barton, M.L.; Green, J.A. The Modified Checklist for Autism in Toddlers: An initial study investigating the early detection of autism and pervasive developmental disorders. J. Autism Dev. Disord. 2001, 31, 131–144. [Google Scholar] [PubMed]
- Bös, K.; Schlenker, L.; Büsch, D.; Lämmle, L.; Müller, H.; Oberger, J. Deutscher Motorik-Test 6–18 (DMT 6–18) [German Motor Performance Test (DMT 6–18)]; Czwalina: Hamburg, Germany, 2009. [Google Scholar]
- Henderson, S.E.; Sugden, D.A.; Barnett, A.L. Movement Assessment Battery for Children-2: Movement ABC-2: Examiner’s Manual; Pearson: London, UK, 2007. [Google Scholar]
- Jelsma, D.; Geuze, R.H.; Mombarg, R.; Smits-Engelsman, B.C. The impact of Wii Fit intervention on dynamic balance control in children with probable Developmental Coordination Disorder and balance problems. Hum. Mov. Sci. 2014, 33, 404–418. [Google Scholar] [CrossRef] [PubMed]
- Barnhart, R.C.; Davenport, M.J.; Epps, S.B.; Nordquist, V.M. Developmental coordination disorder. Phys. Ther. 2003, 83, 722–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Study | Study Design | Disease | Sample Size | Age (Years) | Female (%) | Outcome Measures | Frequency (/Week) | Time | Duration (Weeks) | Type | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Benzing et al. 2019 [15] | RCT | ADHD | 51 | 8–12 | 18.6 | E-Prime Software, Conners-3 scales, DSM-Ⅳ-TR symptom scales, German Motor Test | 3 | 10 min/day | 8 | Xbox Kinect | Exergames significantly improved EFs, general psychopathology, and motor abilities. |
| Howie et al. 2016 [16] | Crossover RCT | DCD | 21 | 9–12 | 52.4 | MABC-2, accelerometers | 4–5 | 140 min/week | 16 | PlayStation 3, Xbox360, non-violent games | There were no differences in PA after the AVG intervention. |
| Straker et al. 2015 [17] | Crossover RCT | DCD | 21 | 9–12 | 52.4 | MABC-2, accelerometers | 4–5 | 140 min/week | 16 | PlayStation3, Xbox360, non-violent games | There were no differences in motor coordination during an intervention with AVGs. |
| Yarımkaya et al. 2022 [18] | Explanatory mixed methods design | ASD | 22 | 10.7 (average) | 31.8 | LTEQ, semi-structured interview questions | 4 | 30–35 min/day | 10 | Home-based exercise, dance activities, fitness activities (Zoom) | PA significantly increased through Zoom-delivered physical activity compared to the control group. |
| Esentürk et al. 2021 [19] | Feasibility study | ASD | 14 | 9–14 | 42.9 | Feasibility questionnaire, LTEQ | 7 | 20–30 min/day | 4 | Home-based exercise, fun games, dance, housework, meditation, fitness activities (WhatsApp) | PA was positively affected after the WhatsApp-based intervention. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikezawa, N.; Yoshihara, R.; Kitamura, M.; Osumi, A.; Kanejima, Y.; Ishihara, K.; Izawa, K.P. Web-Based Exercise Interventions for Children with Neurodevelopmental Disorders. Pediatr. Rep. 2023, 15, 119-128. https://doi.org/10.3390/pediatric15010010
Ikezawa N, Yoshihara R, Kitamura M, Osumi A, Kanejima Y, Ishihara K, Izawa KP. Web-Based Exercise Interventions for Children with Neurodevelopmental Disorders. Pediatric Reports. 2023; 15(1):119-128. https://doi.org/10.3390/pediatric15010010
Chicago/Turabian StyleIkezawa, Natsumi, Ryo Yoshihara, Masahiro Kitamura, Ayami Osumi, Yuji Kanejima, Kodai Ishihara, and Kazuhiro P. Izawa. 2023. "Web-Based Exercise Interventions for Children with Neurodevelopmental Disorders" Pediatric Reports 15, no. 1: 119-128. https://doi.org/10.3390/pediatric15010010