
Multiplex Detection of Antimicrobial Resistance Genes for Rapid Antibiotic Guidance of Urinary Tract Infections
Abstract
:1. Introduction, Background and Significance
2. Materials and Methods
| CDC/FDA AR Bank Isolate Panels | Panel Codes | Number of Samples |
| Acinetobacter baumanii Panel | ACI | 29 |
| Aminoglycoside/Tetracycline Resistance Panel | ATR | 30 |
| Ceftazidime/Avibactam Panel | CZA | 20 |
| Ceftolozane/Tavibactam Panel | CTV | 20 |
| Drug Resistance Candida Panel (CAN) | CAN | 23 |
| Enteric Pathogen Diversity Panel | GI | 29 |
| Enterobacteriaceae Carbapenem Breakpoint Panel | BIT | 22 |
| Enterobacteriaceae Carbapenemase Diversity Panel | CRE | 29 |
| Gram-Negative Carbapenemase Detection Panel | CarbaNP | 53 |
| Imipenem/Relebactam Panel | IMR | 18 |
| Neisseria gonnorheae Panel | GC | 28 |
| Pseudomonas aeruginosa Panel | PSA | 28 |
| Staphylococcus with Borderline Oxacillin Susceptibility Panel | BOR | 24 |
| Vancomycin Intermediate Staphylococcus aureus Panel | VISA | 13 |
3. Results
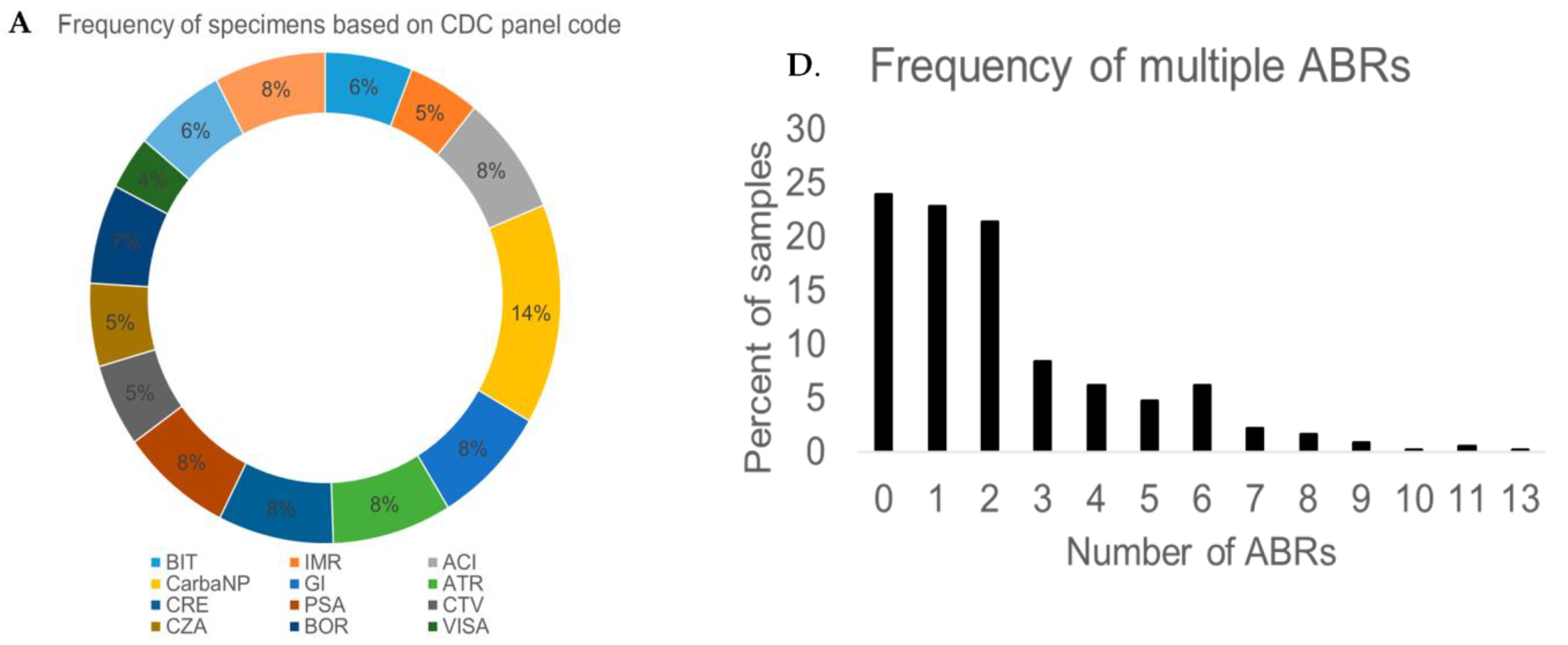
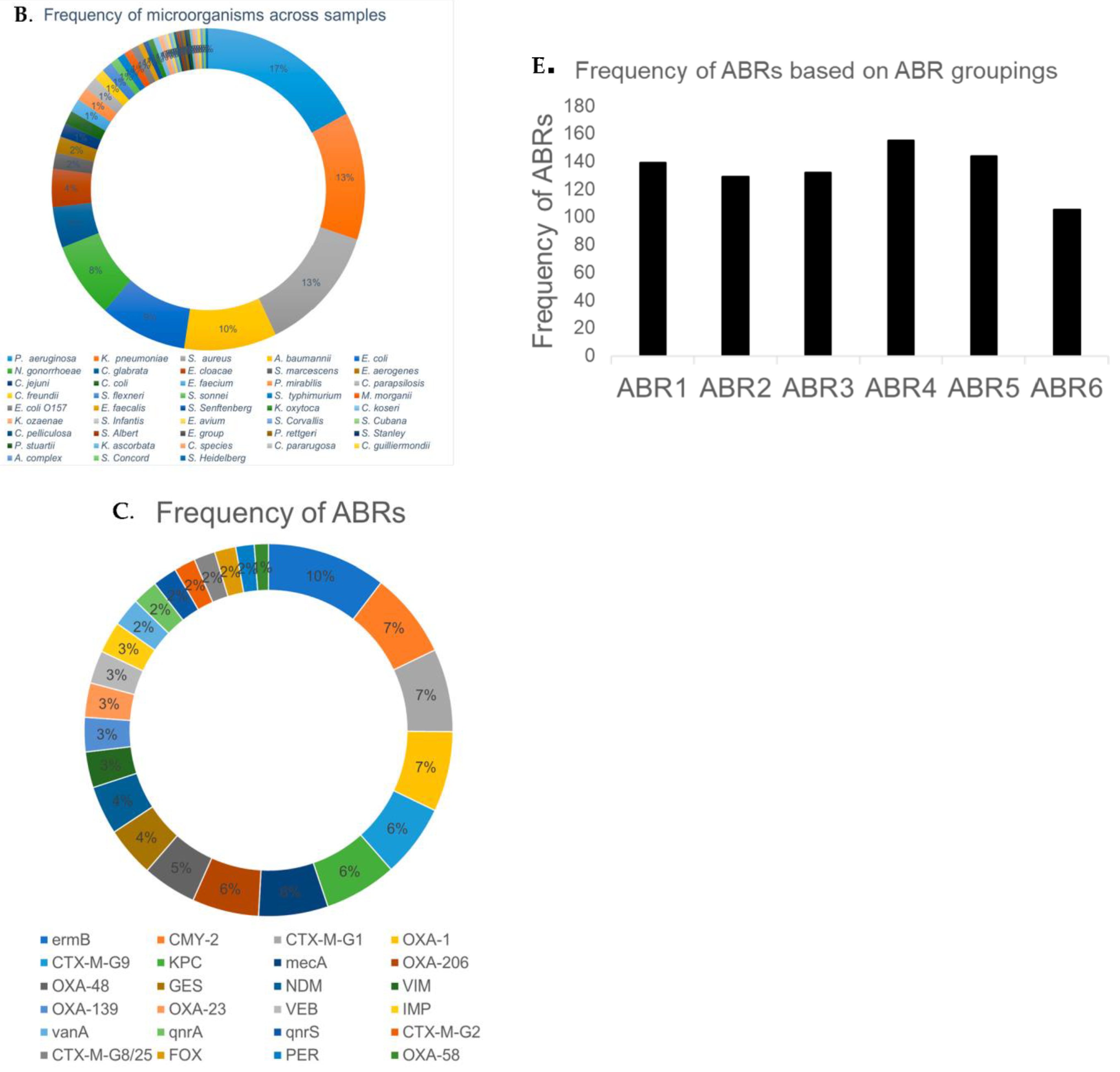
3.1. Classification and Analysis of Antibiotic Resistance Markers
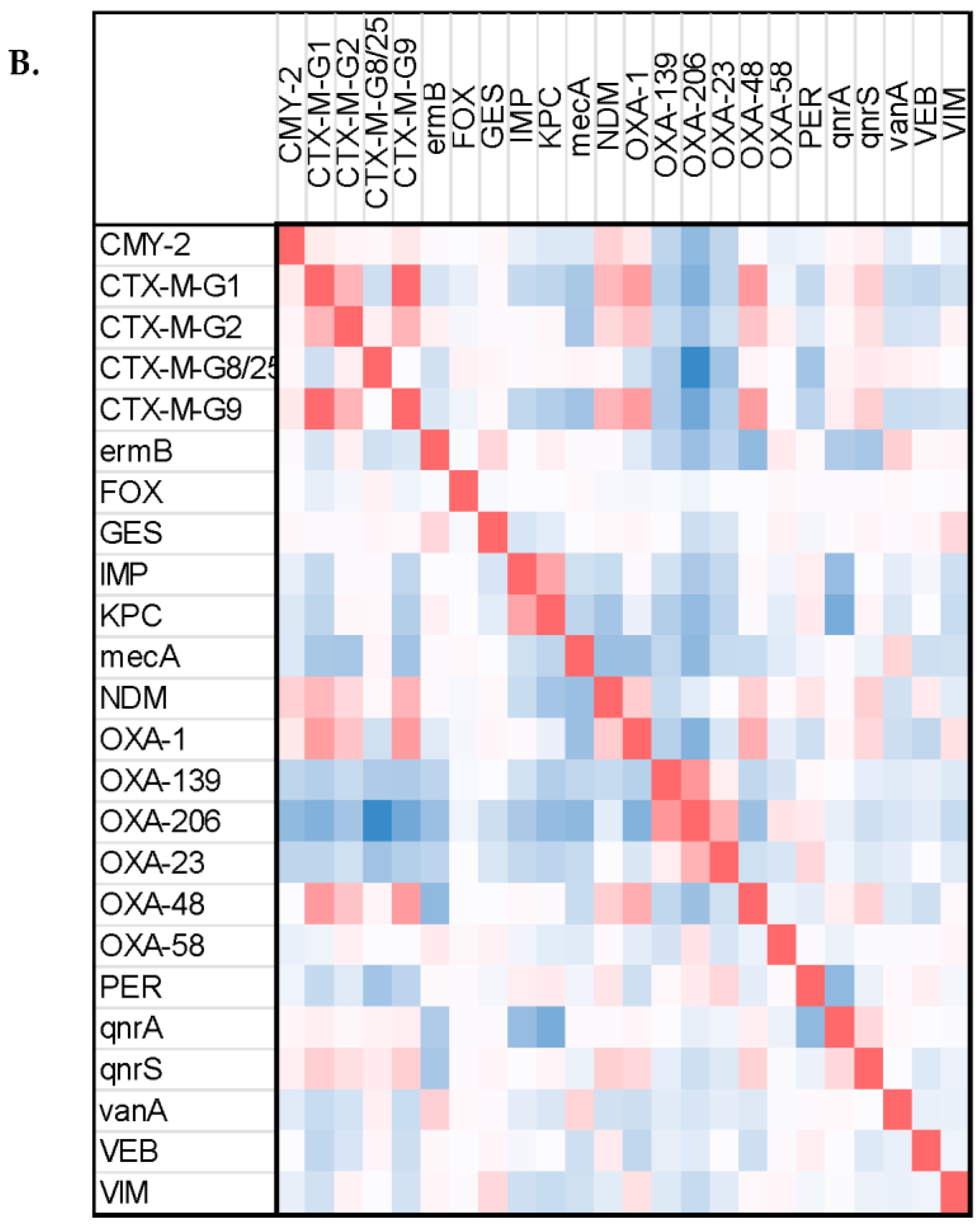
3.2. Correlation between Antibiotic Resistance Markers
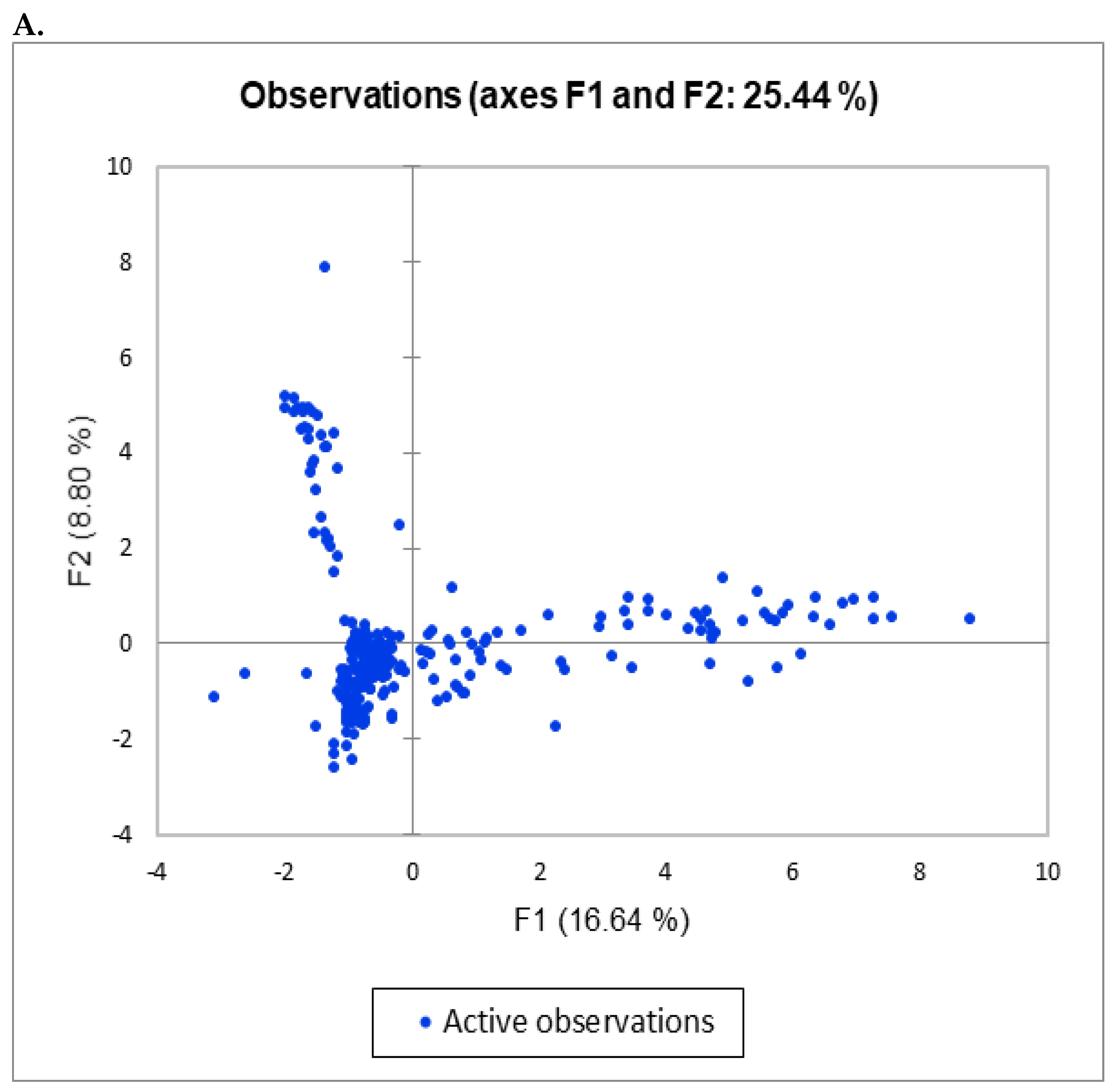
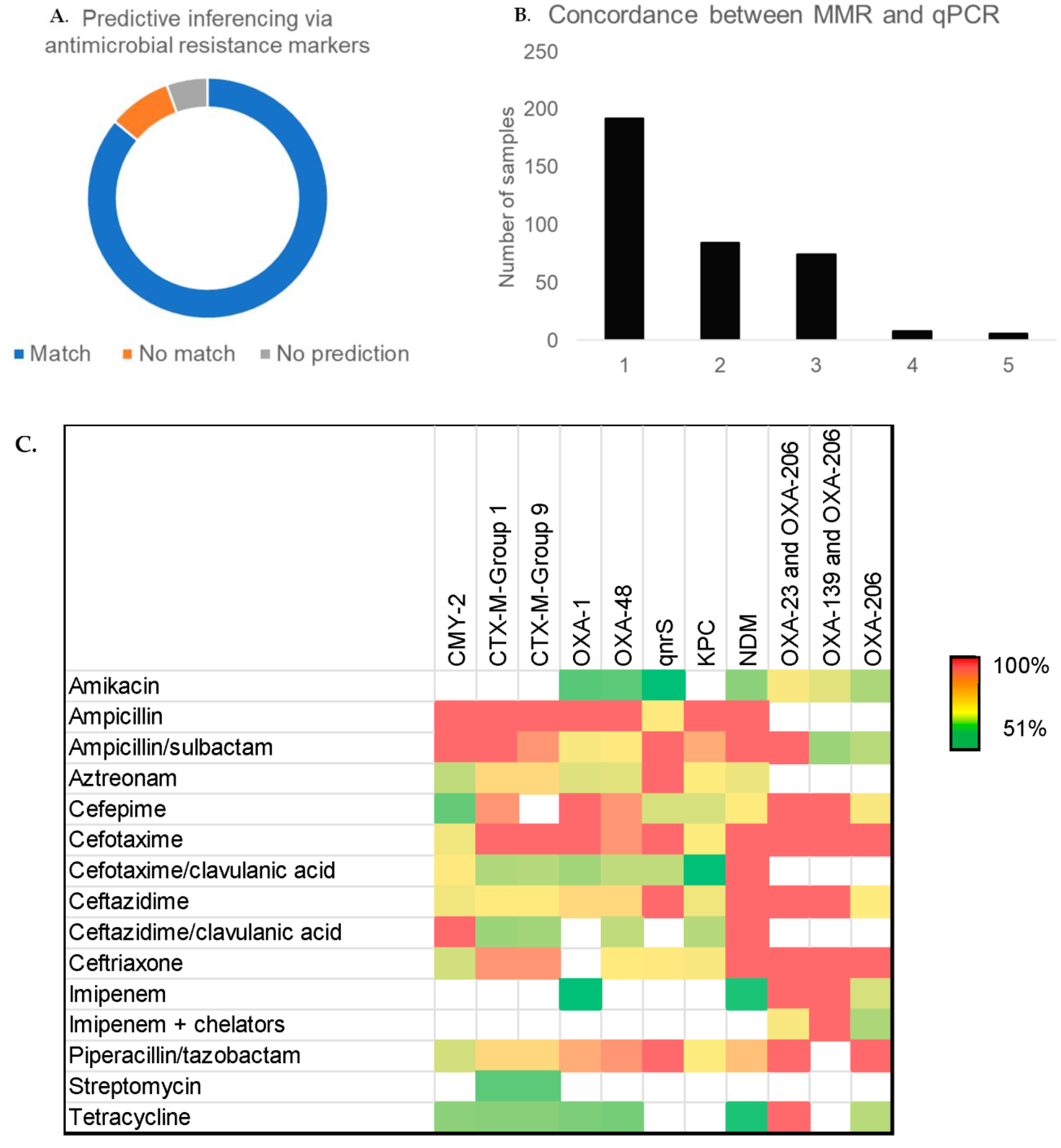
3.3. Accuracy of Model for Predictive Inferencing via Antimicrobial Resistance Markers
3.4. Concordance between CDC-Tested Methods and Multiplex qPCR
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stamm, W.E.; Norrby, S.R. Urinary Tract Infections: Disease Panorama and Challenges. J. Infect. Dis. 2001, 183 (Suppl. S1), S1–S4. [Google Scholar] [CrossRef]
- Schappert, S.M.; A Rechtsteiner, E. Ambulatory medical care utilization estimates for 2007. Vital Health Stat. 13 2011, 169, 1–38. [Google Scholar]
- Zilberberg, M.D.; Nathanson, B.H.; Sulham, K.; Shorr, A.F. Descriptive epidemiology and outcomes of emergency department visits with complicated urinary tract infections in the United States, 2016–2018. J. Am. Coll. Emerg. Physicians Open 2022, 3, e12694. [Google Scholar] [CrossRef]
- KKobayashi, M.; Shapiro, D.J.; Hersh, A.L.; Sanchez, G.V.; Hicks, L.A. Outpatient Antibiotic Prescribing Practices for Uncomplicated Urinary Tract Infection in Women in the United States, 2002–2011. Open Forum Infect. Dis. 2016, 3, ofw159. [Google Scholar] [CrossRef]
- Shapiro, D.J.; Hicks, L.A.; Pavia, A.T.; Hersh, A.L. Antibiotic prescribing for adults in ambulatory care in the USA, 2007–09. J. Antimicrob. Chemother. 2014, 69, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.Y.; Seed, P.; Schofield, P.; Ibrahim, S.; Ashworth, M. Which practices are high antibiotic prescribers? A cross-sectional analysis. Br. J. Gen. Pr. 2009, 59, e315–e320. [Google Scholar] [CrossRef] [PubMed]
- Broyles, M.R. Impact of Procalcitonin-Guided Antibiotic Management on Antibiotic Exposure and Outcomes: Real-world Evidence. Open Forum. Infect. Dis. 2017, 4, ofx213. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Muller, B.; Christ-Crain, M.; Stolz, D.; Tamm, M.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; Briel, M.; et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst. Rev. 2017, 10, CD007498. [Google Scholar] [CrossRef] [PubMed]
- de Jong, E.; van Oers, J.A.; Beishuizen, A.; Vos, P.; Vermeijden, W.J.; Haas, L.E.; Loef, B.G.; Dormans, T.; van Melsen, G.C.; de Lange, D.W.; et al. Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: A randomised, controlled, open-label trial. Lancet Infect. Dis. 2016, 16, 819–827. [Google Scholar] [CrossRef]
- Department of Health and Human Services; Centers for Disease Control and Prevention. Antibiotic Resistance Trends in the United States. 2013. Available online: https://www.cdc.gov/drugresistance/pdf/arthreats-2013–508.pdf (accessed on 12 March 2023).
- Centers for Disease Control and Prevention; National Center for Emerging and Zoonotic Infectious Diseases; Division of Healthcare Quality Promotion. Antibiotic/Antimi-Crobial Resistance (AR/AMR). Available online: https://www.cdc.gov/drugresistance/about.html (accessed on 12 March 2023).
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; Dellinger, R.P.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar]
- Price, T.K.; Dune, T.; Hilt, E.E.; Thomas-White, K.J.; Kliethermes, S.; Brincat, C.; Brubaker, L.; Wolfe, A.J.; Mueller, E.R.; Schreckenberger, P.C. The Clinical Urine Culture: Enhanced Techniques Improve Detection of Clinically Relevant Microorganisms. J. Clin. Microbiol. 2016, 54, 1216–1222. [Google Scholar] [CrossRef]
- Wojno, K.J.; Baunoch, D.; Luke, N.; Opel, M.; Korman, H.; Kelly, C.; Jafri, S.M.A.; Keating, P.; Hazelton, D.; Hindu, S.; et al. Multiplex PCR Based Urinary Tract Infection (UTI) Analysis Compared to Traditional Urine Culture in Identifying Significant Pathogens in Symptomatic Patients. Urology 2020, 136, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Croxall, G.; Weston, V.; Joseph, S.; Manning, G.; Cheetham, P.; McNally, A. Increased human pathogenic potential of Escherichia coli from polymicrobial urinary tract infections in comparison to isolates from monomicrobial culture samples. J. Med Microbiol. 2011, 60 Pt 1, 102–109. [Google Scholar] [CrossRef]
- Hilt, E.E.; McKinley, K.; Pearce, M.M.; Rosenfeld, A.B.; Zilliox, M.J.; Mueller, E.R.; Brubaker, L.; Gai, X.; Wolfe, A.J.; Schreckenberger, P.C. Urine Is Not Sterile: Use of Enhanced Urine Culture Techniques To Detect Resident Bacterial Flora in the Adult Female Bladder. J. Clin. Microbiol. 2014, 52, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Fasolino, T. New and emerging technologies for the diagnosis of urinary tract infections. J. Lab. Med. 2022, 46, 3–15. [Google Scholar] [CrossRef]
- Lutgring, J.D.; Machado, M.-J.; Benahmed, F.H.; Conville, P.; Shawar, R.M.; Patel, J.; Brown, A.C. FDA-CDC Antimicrobial Resistance Isolate Bank: A Publicly Available Resource to Support Research, Development, and Regulatory Requirements. J. Clin. Microbiol. 2018, 56. [Google Scholar] [CrossRef] [PubMed]
- Wielders, C.L.C.; Fluit, A.C.; Brisse, S.; Verhoef, J.; Schmitz, F.J. mecA Gene Is Widely Disseminated in Staphylococcus aureus Population. J. Clin. Microbiol. 2002, 40, 3970–3975. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Hiramatsu, K. Acquisition of methicillin resistance and progression of multiantibiotic resistance in methicil-lin-resistant Staphylococcus aureus. Yonsei Med. J. 1998, 39, 526–533. [Google Scholar] [CrossRef]
- Poirel, L.; Nordmann, P. Carbapenem resistance in Acinetobacter baumannii: Mechanisms and epidemiology. Clin. Microbiol. Infect. 2006, 12, 826–836. [Google Scholar] [CrossRef] [PubMed]
- Vollstedt, A.; Baunoch, D.; Wojno, K.J.; Luke, N.; Cline, K.; Belkoff, L.; Sirls, L. Multisite prospective comparison of multiplex polymerase chain reaction testing with urine culture for diagnosis of urinary tract infections in symptomatic patients. J. Sur. Urol. 2020, 1, JSU-102. [Google Scholar]
- Vollstedt, A.; Baunoch, D.; Wolfe, A.; Luke, N.; Wojno, K.J.; Cline, K.; Belkoff, L.; Milbank, A.; Sherman, N.; Sirls, L.; et al. Bacterial interactions as detected by pooled antibiotic susceptibility testing (P-AST) in polymicrobial urine specimens. J. Sur. Urol. 2020, 1, JSU-101. [Google Scholar] [CrossRef]
- Pietsch, M.; RESET Study Group; Irrgang, A.; Roschanski, N.; Michael, G.B.; Hamprecht, A.; Rieber, H.; Käsbohrer, A.; Schwarz, S.; Rösler, U.; et al. Whole genome analyses of CMY-2-producing Escherichia coli isolates from humans, animals and food in Germany. BMC Genom. 2018, 19, 601. [Google Scholar] [CrossRef] [PubMed]
- Pinkerton, S.D.; Bogart, L.M.; Howerton, D.; Snyder, S.; Becker, K.; Asch, S.M. Cost of Rapid HIV Testing at 45 U.S. Hospitals. AIDS Patient Care STDs 2010, 24, 409–413. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibiotic Resistance | Targeted Drug Classes |
|---|---|
| ABR1 CTX M Group 1 CTX M Group 2 CTX M Group 8/25 CTX M Group 9 | Class A beta-lactamase resistance (cephalosporins, penicillins, aztreonam) |
| ABR2 OXA-1 OXA-48 qnrA qnrS | Class D oxacillinases resistance (cloxacillin, oxacillin, penicillins, carbapenems, extended spectrum cephalosporins, B-lactamase inhibitors) Fluoroquinolones resistance (ciprofloxacin, gemifloxacin, levofloxacin, moxifloxacin, norfloxacin, ofloxacin) |
| ABR3 KPC IMP-1 VIM NDM | Class A beta-lactamase resistance (carbapenems, cephalosporins, penicillins, b-lactamase inhibitors, aztreonam) Class B metallo-beta-lactamase resistance (carbapenems, cephalosporins, penicillins, b-lactamase inhibitors) |
| ABR4 PER VEB GES ermB | Minor ESBL Resistance: (Extended spectrum cephalosporins, penicillins, aztreonam, Carbapenems, cephamycins, extended spectrum cephalosporins, penicillins) Macrolides resistance (erythromycin, clindamycin, azithromycin) |
| ABR5 FOX mecA vanA CMY-2 | AmpC beta- lactamase resistance (cephalosporins, penicillins, b-lactamase inhibitors) Methicillin resistance Vancomycin resistance Cephamycin/cephalosporin resistance |
| ABR6 OXA-23 OXA-139 OXA-206 OXA-58 | Oxacillinases resistance |
| ABR Gene Target | Amplicon Length (bp) | Fluorophore | Excitation (nm) | Emission (nm) |
|---|---|---|---|---|
| CTX-M-Group 1 | 185 | FAM | 495 | 520 |
| CTX-M-Group 2 | 111 | HEX | 538 | 555 |
| CTX-M-Group 8/25 | 145 | ROX | 588 | 608 |
| CTX-M-Group 9 | 85 | Cy5 | 648 | 668 |
| OXA-1 | 109 | FAM | 495 | 520 |
| OXA-48 | 100 | HEX | 538 | 555 |
| qnrA | 107 | ROX | 588 | 608 |
| qnrS | 100 | Cy5 | 648 | 668 |
| KPC | 115 | FAM | 495 | 520 |
| IMP | 102 | HEX | 538 | 555 |
| VIM | 108 | ROX | 588 | 608 |
| NDM | 130 | Cy5 | 648 | 668 |
| PER | 92 | FAM | 495 | 520 |
| VEB | 97 | HEX | 538 | 555 |
| GES | 96 | ROX | 588 | 608 |
| ermB | 105 | Cy5 | 648 | 668 |
| FOX | 129 | FAM | 495 | 520 |
| mecA | 128 | HEX | 538 | 555 |
| vanA | 119 | ROX | 588 | 608 |
| CMY-2 | 124 | Cy5 | 648 | 668 |
| OXA-23 | 81 | FAM | 495 | 520 |
| OXA-139 | 106 | HEX | 538 | 555 |
| OXA-206 | 106 | ROX | 588 | 608 |
| OXA-58 | 93 | Cy5 | 648 | 668 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harris, M.; Fasolino, T.; Davis, N.J.; Ivankovic, D.; Brownlee, N. Multiplex Detection of Antimicrobial Resistance Genes for Rapid Antibiotic Guidance of Urinary Tract Infections. Microbiol. Res. 2023, 14, 591-602. https://doi.org/10.3390/microbiolres14020041
Harris M, Fasolino T, Davis NJ, Ivankovic D, Brownlee N. Multiplex Detection of Antimicrobial Resistance Genes for Rapid Antibiotic Guidance of Urinary Tract Infections. Microbiology Research. 2023; 14(2):591-602. https://doi.org/10.3390/microbiolres14020041
Chicago/Turabian StyleHarris, Mohammed, Tracy Fasolino, Nicole J. Davis, Diana Ivankovic, and Noel Brownlee. 2023. "Multiplex Detection of Antimicrobial Resistance Genes for Rapid Antibiotic Guidance of Urinary Tract Infections" Microbiology Research 14, no. 2: 591-602. https://doi.org/10.3390/microbiolres14020041