
The Impact of Antimicrobial Resistance on Outcomes for Patients Undergoing Coronary Artery Bypass Graft and Valve Surgery: A Retrospective Cohort Study of Hospital Admissions Data from the National Inpatient Sample

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
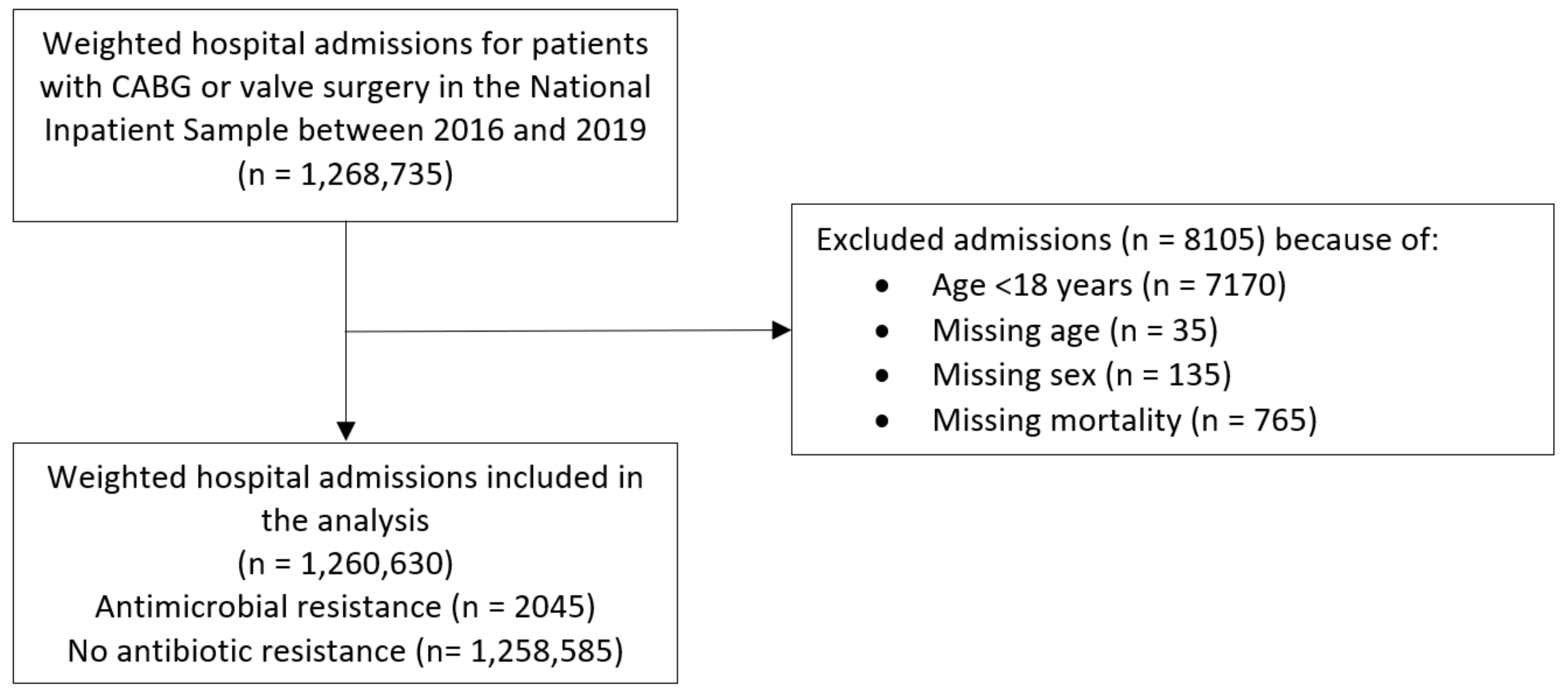
3. Results
4. Discussion
4.1. Key Findings
4.2. Key Considerations Regarding the Findings
4.3. Generalizability
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Variable | Source of Data | Detailed Codes/Description |
|---|---|---|
| Coronary artery bypass graft surgery | I10_PR1/25 | 021008, 021009, 02100A, 02100J, 02100K, 02100Z, 021108, 021109, 02110A, 02110J, 02110K, 02110Z, 021208, 021209, 02120A, 02120J, 02120K, 02120Z, 021308, 021309, 02130A, 02130J, 02130K, 02130Z |
| Valve surgery | I10_PR1/25 | 02RF0, 02RF3, 02RG0, 02RG3, 02RH0, 02RH3, 02RJ0, 02RJ3 |
| Antibiotic resistance | I10_DX1/40 | Z16 |
| Age | NIS Core | Derived from “AGE” variable. |
| Sex | NIS Core | Derived from “FEMALE” variable. |
| Race | NIS Core | Derived from “RACE” variable. |
| Rural | See comment | Derived from “PL_NCHS” variable in the NIS Core file where rural = micropolitan counties and not metropolitan or micropolitan counties. |
| Teaching hospital | See comment | Derived from “HOSP_LOCTEACH” variable in the NIS Hospital file where teaching hospitals are those which are urban teaching values. |
| Hospital region | NIS Hospital | Derived from “HOSP_REGION” variable. |
| Elective admission | NIS Core | Derived from “ELECTIVE” variable. |
| Weekend admission | NIS Core | Derived from “AWEEKEND” variable. |
| Primary expected payer | NIS Core | Derived from “PAY1” variable. |
| ZIP income quartile | NIS Core | Derived from “ZIPINC_QRTL” variable. |
| Hospital bed size | NIS Hospital | Derived from “HOSP_BEDSIZE” variable. |
| Smoking | I10_DX1/40 | Z72.0 |
| Alcohol misuse | I10_DX1/40 | F10.1 |
| Chronic kidney disease | I10_DX1/40 | N18 |
| Chronic lung disease | I10_DX1/40 | J40, J41, J42, J43, J44, J45, J46, J47 |
| Previous myocardial infarction | I10_DX1/40 | I25.2 |
| Previous stroke | I10_DX1/40 | I69 |
| Atrial fibrillation | I10_DX1/40 | I48 |
| Hypertension | I10_DX1/40 | I10, I11, I12, I13, I15, I16 |
| Hypercholesterolemia | I10_DX1/40 | E78.0, E78.1, E78.2, E78.3, E78.4, E78.5 |
| Diabetes mellitus | I10_DX1/40 | E08, E09, E10, E11, E13 |
| Cancer | I10_DX1/40 | C * |
| Dementia | I10_DX1/40 | F01, F02, F03, G30, G31 |
| Peripheral vascular disease | I10_DX1/40 | I73 |
| Liver failure | I10_DX1/40 | K72 |
| Obesity | I10_DX1/40 | E66.0, E66.1, E66.2, E66.8, E66.9 |
| Heart failure | I10_DX1/40 | I09.81, I11.0, I50 |
| Season | AMONTH Spring = March to May, Summer = June to August, Fall = September to November, Winter = December to February | |
| Central venous line | I10_PR1/25 | 02HV33Z, 02H633Z |
| Sepsis | I10_DX1/40 | A41 |
| Infection | I10_DX1/40 | A *, B * |
| Death | NIS Core | - |
| Length of stay | NIS Core | - |
| Cost | See comment | Defined by the product of the charge-to-cost ratio and total charge (“TOTCHG” in the NIS core file). |
| Discharge weight | NIS Core | - |
References
- Moffatt-Bruce, S.; Crestanello, J.; Way, D.P.; Williams, T.E., Jr. Providing cardiothoracic services in 2035: Signs of trouble ahead. J. Thorac. Cardiovasc. Surg. 2018, 155, 824–829. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Khera, R. Pumping the breaks on health care costs of cardiac surgery focusing on postacute cardiac spending. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e007253. [Google Scholar] [CrossRef]
- Kollef, M.H.; Sharpless, L.; Vlasnik, J.; Pasque, C.; Murphy, D.; Fraser, V.J. The impact of nosocomial infections on patient outcomes following cardiac surgery. Chest 1997, 112, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Massart, N.; Mansour, A.; Ross, J.T.; Piau, C.; Verhoye, J.P.; Tattevin, P.; Nesseler, N. Mortality due to hospital-acquired infection after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2022, 163, 2131–2140. [Google Scholar] [CrossRef]
- Jenney, A.W.; Harrington, G.A.; Spelman, D.W. Cost of surgical site infections following coronary artery bypass surgery. ANZ J. Surg. 2001, 71, 662–664. [Google Scholar] [CrossRef] [PubMed]
- Engelman, R.; Shahian, D.; Shemin, R.; Guy, T.S.; Bratzler, D.; Edwards, F.; Jacobs, M.; Fernando, H.; Bridges, C. The Society of Thoracic Surgeons Practice Guideline Series: Antibiotic prophylaxis in cardiac surgery, part II: Antibiotic choice. Ann. Thorac. Surg. 2007, 83, 1569–1576. [Google Scholar] [CrossRef]
- Lador, A.; Nasir, H.; Mansur, N.; Sharoni, E.; Biderman, P.; Leibovici, L.; Paul, M. Antibiotic prophylaxis in cardiac surgery: Systematic review and meta-analysis. J. Antimicrob. Chemother. 2012, 67, 541–550. [Google Scholar] [CrossRef]
- Fong, I.W.; Baker, C.B.; McKee, D.C. The value of prophylactic antibiotics in aorta-coronary bypass operations: A double-blind randomized trial. J. Thorac. Cardiovasc. Surg. 1979, 78, 908–913. [Google Scholar] [CrossRef]
- Zanetti, G.; Goldie, S.J.; Platt, R. Clinical consequences and cost of limiting use of vancomycin for perioperative prophylaxis: Example of coronary artery bypass surgery. Emerg. Infect. Dis. 2001, 7, 820–827. [Google Scholar] [CrossRef]
- Gelijns, A.C.; Moskowitz, A.J.; Acker, M.A.; Argenziano, M.; Geller, N.L.; Puskas, J.D.; Perrault, L.P.; Smith, P.K.; Kron, I.L.; Michler, R.E.; et al. Management practices and major infections after cardiac surgery. J. Am. Coll. Cardiol. 2014, 64, 372–381. [Google Scholar] [CrossRef]
- World Health Organization. Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 24 December 2022).
- Antimicrobial Resistance Collaborators. Global burden on bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Johnston, K.J.; Thorpe, K.E.; Jacob, J.T.; Murphy, D.J. The incremental cost of infections associated with multidrug-resistant organisms in the inpatient hospital setting—A national estimate. Health Serv. Res. 2019, 54, 782–792. [Google Scholar] [CrossRef]
- The Expert Panel on The Potential Socio-Economic Impacts of Antimicrobial Resistance in Canada. When Antibiotics Fail. 2019. Available online: https://cca-reports.ca/reports/the-potential-socio-economic-impacts-of-antimicrobial-resistance-in-canada/ (accessed on 24 December 2022).
- Pierce, G.N.; Resch, C.; Mourin, M.; Dibrov, P.; Dibrov, E.; Ravandi, A. Bacteria and growing threat of multidrug resistance for invasive cardiac interventions. Rev. Cardiovasc. Med. 2022, 23, 15. [Google Scholar] [CrossRef]
- Healthcare Cost & Untilization Project. Overview of the National (Nationwide) Inpatient Sample (NIS). Available online: https://www.hcup-us.ahrq.gov/nisoverview.jsp (accessed on 24 December 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Mubashir, T.; Balogh, J.; Breland, E.; Rumpel, D.; Waheed, M.A.; Lai, H.; Napolitano, C.A. Risk factors and outcome of protein-calorie malnutrition in chronic heart failure patients undergoing elective cardiac surgery. Cureus 2022, 14, e30378. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Antimicrobial Resistance. Available online: https://ahpsr.who.int/publications/i/item/global-action-plan-on-antimicrobial-resistance (accessed on 24 December 2022).
- Hamasaeed, P.A. Resistance to bacterial infection, complication occurring after cardiac surgery. Cell. Mol. Biol. 2020, 66, 20–25. [Google Scholar] [CrossRef]
- Ko, R.E.; Huh, K.; Kim, D.H.; Na, S.J.; Chung, C.R.; Cho, Y.H.; Jeon, K.; Suh, G.Y.; Yang, J.H. Nosocomial infections in in-hospital cardiac arrest patients who undergo extracorporeal cardiopulmonary resuscitation. PLoS ONE 2020, 15, e0243838. [Google Scholar] [CrossRef]
- Bhatt, P.J.; Ali, M.; Rana, M.; Patel, G.; Sullivan, T.; Murphy, J.; Pinney, S.; Anyanwu, A.; Huprikar, S.; Taimur, S. Infections due to multidrug-resistant organisms following heart transplantation: Epidemiology, microbiology, and outcomes. Transpl. Infect. Dis. 2020, 22, e13215. [Google Scholar] [CrossRef]
- Zhou, Y.; Cai, J.; Wang, X.; Du, S.; Zhang, J. Distribution and resistance of pathogens in infected patients within 1 year after heart transplantation. Int. J. Infect. Dis. 2020, 103, 132–137. [Google Scholar] [CrossRef]
- Crnich, C.J.; Safdar, N.; Robinson, J.; Zimmerman, D. Longitudinal trends in antibiotic resistance in US nursing homes, 2000–2004. Infect. Control Hosp. Epidemiol. 2007, 28, 1006–1008. [Google Scholar] [CrossRef]
- Menz, B.D.; Charani, E.; Gordon, D.L.; Leather, A.J.M.; Moonesinghe, S.R.; Phillips, C.J. Surgical antibiotic prophylaxis in an era of antibiotic resistance: Common resistant bacteria and wider considerations for practice. Infect. Drug Resist. 2021, 14, 5235–5252. [Google Scholar] [CrossRef] [PubMed]
- Chokshi, A.; Sifri, Z.; Cennimo, D.; Horng, H. Global contributors to antibiotic resistance. J. Glob. Infect. Dis. 2019, 11, 36–42. [Google Scholar] [PubMed]

| Variable | No Antimicrobial Resistance | Antimicrobial Resistance | p-Value |
|---|---|---|---|
| Total | 1,258,585 | 2045 | - |
| Mean age [IQR] | 69 [61 to 76] | 68 [58 to 76] | 0.73 |
| Female | 31.5% | 52.8% | <0.001 |
| Race/ethnicity | <0.001 | ||
| White | 80.0% | 69.5% | |
| African American | 6.7% | 7.8% | |
| Hispanic | 7.3% | 13.7% | |
| Asian or Pacific Islander | 2.7% | 3.1% | |
| Native American | 0.5% | 0.8% | |
| Other | 2.8% | 5.2% | |
| Nicotine dependence | 1.1% | 1.2% | 0.82 |
| Alcohol misuse | 1.6% | 2.7% | 0.083 |
| Weekend admission | 9.1% | 17.4% | <0.001 |
| Season | 0.24 | ||
| Spring | 25.9% | 24.0% | |
| Summer | 25.0% | 26.7% | |
| Fall | 24.9% | 28.1% | |
| Winter | 24.3% | 21.3% | |
| Elective admission | 58.5% | 34.4% | <0.001 |
| Primary expected payer | <0.001 | ||
| Medicare | 61.3% | 58.7% | |
| Medicaid | 7.0% | 13.9% | |
| Private insurance | 26.6% | 21.5% | |
| Self-pay | 2.3% | 2.9% | |
| No charge | 0.2% | 0% | |
| Other | 2.7% | 2.9% | |
| Year | 0.009 | ||
| 2016 | 24.1% | 19.6% | |
| 2017 | 24.7% | 24.5% | |
| 2018 | 25.0% | 23.0% | |
| 2019 | 26.2% | 33.0% | |
| Hospital region | 0.15 | ||
| Northeast | 18.5% | 15.7% | |
| Midwest | 23.4% | 20.8% | |
| South | 40.0% | 42.8% | |
| West | 18.1% | 20.8% | |
| Hospital bed size | 0.54 | ||
| Small | 10.2% | 11.5% | |
| Medium | 24.2% | 25.2% | |
| Large | 65.6% | 63.3% | |
| Rural hospital | 19.4% | 15.3% | 0.037 |
| Teaching hospital | 84.1% | 86.1% | 0.27 |
| Hypertension | 85.6% | 81.2% | 0.011 |
| Hypercholesterolemia | 72.8% | 59.4% | <0.001 |
| Obesity | 24.5% | 24.5% | 0.97 |
| Diabetes mellitus | 41.4% | 44.7% | 0.17 |
| Previous myocardial infarction | 14.2% | 11.7% | 0.15 |
| Heart failure | 40.4% | 54.8% | <0.001 |
| Atrial fibrillation | 39.3% | 48.9% | <0.001 |
| Previous stroke | 10.0% | 12.7% | 0.062 |
| Peripheral vascular disease | 6.9% | 5.1% | 0.15 |
| Chronic kidney disease | 22.8% | 37.2% | <0.001 |
| Liver failure | 1.6% | 7.1% | <0.001 |
| Chronic lung disease | 22.9% | 27.1% | 0.039 |
| Cancer | 3.0% | 3.4% | 0.59 |
| Dementia | 1.8% | 2.4% | 0.31 |
| Surgery type | <0.001 | ||
| Coronary artery bypass only | 56.0% | 44.7% | |
| Valve surgery only | 36.1% | 45.0% | |
| Coronary artery bypass and valve surgery | 7.9% | 10.3% | |
| Central line insertion | 9.1% | 28.4% | <0.001 |
| Sepsis | 2.8% | 20.8% | <0.001 |
| Infection | 23.1% | 88.8% | <0.001 |
| In-hospital mortality | 2.4% | 7.1% | <0.001 |
| Length of stay [IQR] | 7 [5 to 11] | 15 [10 to 23] | <0.001 |
| Cost [IQR] | USD 43,740 [33,283 to 59,767] | USD 69,135 [49,905 to 105,786] | <0.001 |
| Variable | Odds Ratio (95%CI) | p-Value |
|---|---|---|
| Female | 2.13 (1.72–2.62) | <0.001 |
| Race vs. White | ||
| Hispanic | 1.57 (1.14–2.16) | 0.005 |
| Other | 1.88 (1.18–2.99) | 0.008 |
| Alcohol misuse | 1.97 (1.07–3.63) | 0.031 |
| Elective admission | 0.70 (0.55–0.88) | 0.003 |
| Year vs. 2016 | ||
| 2019 | 1.42 (1.06–1.91) | 0.019 |
| Atrial fibrillation | 1.27 (1.03–1.57) | 0.027 |
| Chronic kidney disease | 1.47 (1.17–1.84) | 0.001 |
| Central line insertion | 1.56 (1.22–1.98) | <0.001 |
| Sepsis | 1.50 (1.13–2.00) | 0.005 |
| Infection | 18.33 (13.24–25.37) | <0.001 |
| Variable | Odds Ratio (95% CI) or Coefficient [95% CI] | p-Value |
|---|---|---|
| In-hospital mortality | ||
| Unadjusted | 3.11 (2.13–4.54) | <0.001 |
| Model 1 | 2.75 (1.85–4.11) | <0.001 |
| Model 2 | 2.26 (1.50–3.41) | <0.001 |
| Model 3 | 1.38 (0.86–2.21) | 0.18 |
| Length of stay | ||
| Unadjusted | 11.24 [10.44 to 12.05] | <0.001 |
| Model 1 | 10.82 [9.99 to 11.64] | <0.001 |
| Model 2 | 9.02 [8.25 to 9.80] | <0.001 |
| Model 3 | 7.65 [6.91 to 8.39] | <0.001 |
| Cost | ||
| Unadjusted | USD 42,278 [38,377 to 46,180] | <0.001 |
| Model 1 | USD 39,211 [35,228 to 43,193] | <0.001 |
| Model 2 | USD 33,090 [29,219 to 36,961] | <0.001 |
| Model 3 | USD 25,240 [21,626 to 28,854] | <0.001 |
| Subgroup | In-Hospital Mortality Odds Ratio (95% CI) | Length of Stay Coefficient [95% CI] | Cost Coefficient [95% CI] |
|---|---|---|---|
| No infection | 3.46 (1.00–11.98), p = 0.05 | 11.2 [9.7 to 12,6], p < 0.001 | USD 45,348 [38,638 to 52,059], p < 0.001 |
| Infection | 0.81 (0.50–1.30), p = 0.38 | 3.8 [2.6 to 5.1], p < 0.001 | USD 8361 [2070 to 14,652], p = 0.009 |
| No sepsis | 1.21 (0.65–2.24), p = 0.55 | 6.5 [5.8 to 7.2], p < 0.001 | USD 23,384 [20,045 to 26,723], p < 0.001 |
| Sepsis | 0.63 (0.32–1.24), p = 0.18 | 2.4 [−2.1 to 6.9], p = 0.30 | −USD 10,509 [−34,031 to 13,013], p = 0.38 |
| No central line insertion | 1.59 (0.88–2.85), p = 0.12 | 5.9 [5.1 to 6.6], p < 0.001 | USD 19,803 [16,151 to 23,456], p < 0.001 |
| Central line insertion | 0.84 (0.40–1.79), p = 0.65 | 8.7 [6.3 to 11.1], p < 0.001 | USD 24,572 [12,588 to 36,556], p < 0.001 |
| CABG surgery | 1.23 (0.65–2.32), p = 0.52 | 7.9 [7.0 to 8.8], p < 0.001 | USD 25,271 [20,808 to 29,733], p < 0.001 |
| Valve surgery | 1.54 (0.88–2.70), p = 0.13 | 6.0 [4.8 to 7.1], p < 0.001 | USD 18,672 [12,968 to 24,376], p < 0.001 |
| No infection | 3.46 (1.00–11.98), p = 0.05 | 11.2 [9.7 to 12,6], p < 0.001 | USD 45,348 [38,638 to 52,059], p < 0.001 |
| Infection | 0.81 (0.50–1.30), p = 0.38 | 3.8 [2.6 to 5.1], p < 0.001 | USD 8361 [2070 to 14,652], p = 0.009 |
| No sepsis | 1.21 (0.65–2.24), p = 0.55 | 6.5 [5.8 to 7.2], p < 0.001 | USD 23,384 [20,045 to 26,723], p < 0.001 |
| Sepsis | 0.63 (0.32–1.24), p = 0.18 | 2.4 [−2.1 to 6.9], p = 0.30 | −USD 10,509 [−34,031 to 13,013], p = 0.38 |
| No central line insertion | 1.59 (0.88–2.85), p = 0.12 | 5.9 [5.1 to 6.6], p < 0.001 | USD 19,803 [16,151 to 23,456], p < 0.001 |
| Central line insertion | 0.84 (0.40–1.79), p = 0.65 | 8.7 [6.3 to 11.1], p < 0.001 | USD 24,572 [12,588 to 36,556], p < 0.001 |
| CABG surgery | 1.23 (0.65–2.32), p = 0.52 | 7.9 [7.0 to 8.8], p < 0.001 | USD 25,271 [20,808 to 29,733], p < 0.001 |
| Valve surgery | 1.54 (0.88–2.70), p = 0.13 | 6.0 [4.8 to 7.1], p < 0.001 | USD 18,672 [12,968 to 24,376], p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said, K.A.; Will, M.; Qureshi, A.I.; Kwok, C.S. The Impact of Antimicrobial Resistance on Outcomes for Patients Undergoing Coronary Artery Bypass Graft and Valve Surgery: A Retrospective Cohort Study of Hospital Admissions Data from the National Inpatient Sample. Microbiol. Res. 2023, 14, 580-590. https://doi.org/10.3390/microbiolres14020040
Said KA, Will M, Qureshi AI, Kwok CS. The Impact of Antimicrobial Resistance on Outcomes for Patients Undergoing Coronary Artery Bypass Graft and Valve Surgery: A Retrospective Cohort Study of Hospital Admissions Data from the National Inpatient Sample. Microbiology Research. 2023; 14(2):580-590. https://doi.org/10.3390/microbiolres14020040
Chicago/Turabian StyleSaid, Kirellos Abbas, Maximillian Will, Adnan I. Qureshi, and Chun Shing Kwok. 2023. "The Impact of Antimicrobial Resistance on Outcomes for Patients Undergoing Coronary Artery Bypass Graft and Valve Surgery: A Retrospective Cohort Study of Hospital Admissions Data from the National Inpatient Sample" Microbiology Research 14, no. 2: 580-590. https://doi.org/10.3390/microbiolres14020040