
Intrafamilial Transmission of Pneumococcal Acute Spontaneous Peritonitis
 , , ,
, , ,
Abstract
:1. Introduction
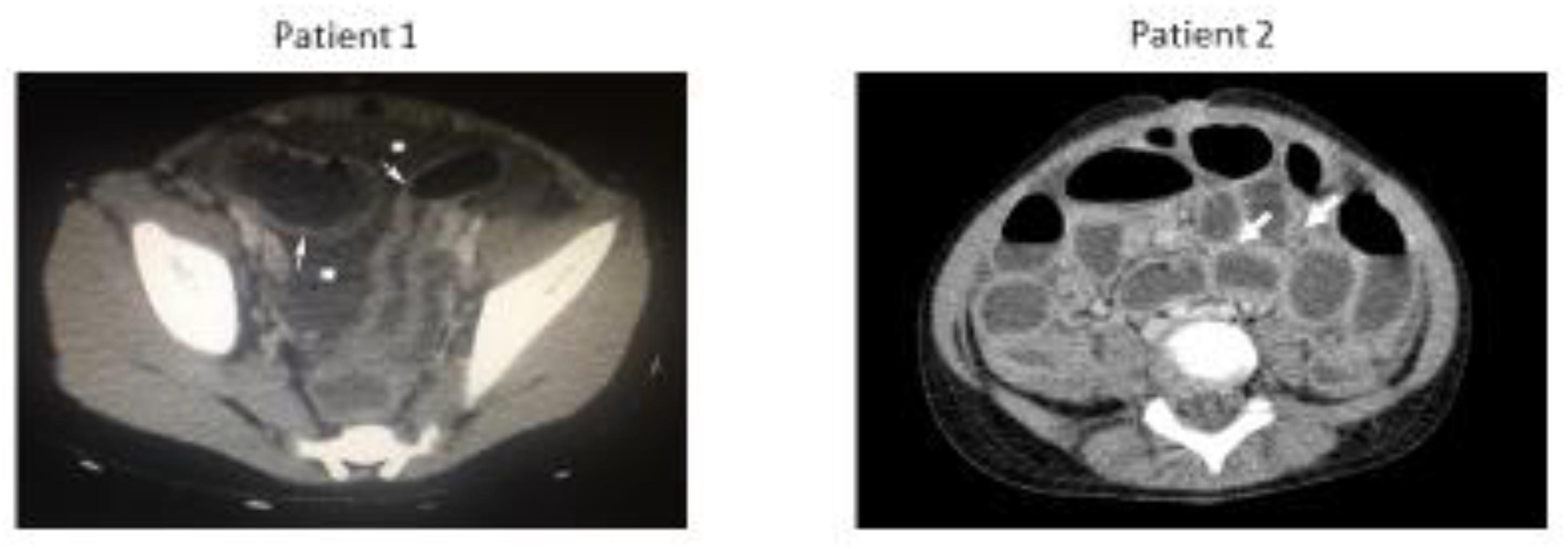
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Patient 1 (3-Year-Old) PspA Gene |
| AGCCTACTGTTGTAAGAGCAGAAGAAGCCCCCGTAGCTAGTCAGTCTAAAGCTGAAAAAGACTATGATGCAGCGAAGAGAGACGCTGAGAATGCGAAAAAAGCTTTAGAAGAAGCAAAACGTGCGCAGAAAAAATATGAGGATGATCAGAAGAAAACTGAGGAGAAAGCGAAAAAAGAGAAAGAAGCTTCTAAAGAGGAACAAGCTGCAAATCTGAAATATCAACAAGAGTTGGTTAAATATGCTAGTGAAAAAGATTCAGTAAAAAAAGCTAAAATTCTGAAAGAAGTGGAGGAAGCTGAGAAAGAGCATAAGAAAAAACGAGCAGAATTTGAGAAAGTTAGATCAGAGGTAATTCCTAGCGCGGAAGAGTTAAAAAAGACTAGACAAAAAGCAGAAGAGGCTAAAGCAAAAGAAGCAGAACTTATTAAAAAAGTAGAAGAAGCTGAGAAAAAAGTTACTGAAGCCAAACAAAAATTGGATGCTGAACGTGCTAAAGAAGTTGCTCTTCAAGCCAAAATCGCTGAGTTGGAAAATGAAGTTTATAGACTAGAAACAGAACTCAAAGGGATTGATGAATCTGACTCAGAAGATTATGTTAAAGAAGGTCTCCGTGCTCCTCTTCAATCTGAATTGGATGCCAAACGAACTAAACTATCAACACTTGAAGAGTTGAGTGATAAGATTGATGAGTTAGACGCTGAAATTGCAAAACTTGAAAAAAATGTAGAATATTTCAAAAAAACCGATGCTGAGCAAACTGAACAATACCTTGCTGCAGCTGAAAAAGACTTAGCTGATAAAAAAGCTGAATTGGAGAAAACTGAAGCTGACCTTAAGAAAGCAGTTAATGAGCCAGAAAAACCAGCTGAAGAAACTCCAGCTCCAGCACCAAAACCAGAAAAAACAGATGATCAACAAGCTGAAGAAGACTATGCTCGTAGATCAGAAGAAGAATATAACCGCTTGCCCCAACAGCAACCGCCAAAAGCAGAAAAACCAGCTCCAGCACCAAAACCAGAGCAACCAGTTCCT |
| Patient 2 (7-Year-Old) PspA Gene |
| AGCCTACTGTTGTAAGAGCAGAAGAAGCCCCCGTAGCTAGTCAGTCTAAAGCTGAAAAAGACTATGATGCAGCGAAGAGAGACGCTGAGAATGCGAAAAAAGCTTTAGAAGAAGCAAAACGTGCGCaGAAAAAATATGAGGATGATCAGAAGAAAACTGAGGAGAAAGCGAAAAAAGAGAAAGAAGCTTCTAAAGAGGAACAAGCTGCAAATCTGAAATATCAaCAAGAGTTGGTTAAATATGCTAGTGAAAAAGATTCAGTAAAAaAAGCTAAAATTCTGAAAGAAGTGGAGGAAGCTGAGAAAGAGCATAAGAAAAAACGAGCAGAATTTGAGAAAGTTAGATCAGAGGTAATTCCTAGCGCGGAAGAGTTAAAAAAGACTAGACAAAAAGCAGAAGAGGCTAAAGCAAAAGAAGCAGAACTTATTAAAAAAGTAGAAGAAGCTGAGAAAAAAGTTACTGAAGCCAAACAAAAATTGGATGCTGAACGTGCTAAAGAAGTTGCTCTTCAAGCCAAAATCGCTGAGTTGGAAAATGAAGTTTATAGACTAGAAACAGAACTCAAAGGGATTGATGAATCTGACTCAgAAGATTATGTTAAAGAAGGTCTCCGTGCTCCTCTTCAATCTGAATTGGATGCCAAACGAACTAAACTATCAACACTTGAAGAGTTGAGTGATAAGATTGATGAGTTAGACGCTGAAATTGCAAAACTTGAAAAAAATGTAGAATATTTCAAAAAAACCGATGCTGAGCAAACTGAACAATACCTTGCTGCAGCTGAAAAAGACTTAGCTGATAAAAAAGCTGAATTGGAGAAAACTGAAGCTGACCTTAAGAAAGCAGTTAATGAGCCAGAAAAACCAGCTGAAGAAACTCCAGCTCCAGCACCAAAACCAGAAAAAACAGATGATCAACAAGCTGAAGAAGACTATGCTCGTAGATCAGAAGAAGAATATAACCGCTTGCCCCAACAGCAACCGCCAAAAGCAGAAAAACCAGCTCCAGCACCAAAACCAGAGCAACCAGTTCCT |
| Patient 1 and Patient 2 PspA Protein 100% Alignment |
 |
References
- Oligbu, G.; Collins, S.; Sheppard, C.L.; Fry, N.K.; Slack, M.; Borrow, R.; Ladhani, S.N. Childhood Deaths Attributable to Invasive Pneumococcal Disease in England and Wales, 2006–2014. Clin. Infect. Dis. 2017, 65, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Oey, R.C.; van Buuren, H.R.; de Jong, D.M.; Erler, N.S.; de Man, R.A. Bacterascites: A study of clinical features, microbiological findings, and clinical significance. Liver Int. 2018, 38, 2199–2209. [Google Scholar] [CrossRef] [PubMed]
- Strutton, D.R.; Farkouh, R.A.; Earnshaw, S.R.; Hwang, S.; Theidel, U.; Kontodimas, S.; Klok, R.; Papanicolaou, S. Cost-effectiveness of 13-valent pneumococcal conjugate vaccine: Germany, Greece, and The Netherlands. J. Infect. 2012, 64, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Waisman, D.C.; Tyrrell, G.J.; Kellner, J.D.; Garg, S.; Marrie, T.J. Pneumococcal peritonitis: Still with us and likely to increase in importance. Can. J. Infect. Dis. Med. Microbiol. 2010, 21, e23–e27. [Google Scholar] [CrossRef] [PubMed]
- Lagos, R.; Muñoz, A.; Martin, O.S.; Maldonado, A.; Hormazabal, J.C.; Blackwelder, W.C.; Levine, M.M. Age- and Serotype-Specific Pediatric Invasive Pneumococcal Disease: Insights from Systematic Surveillance in Santiago, Chile, 1994–2007. J. Infect. Dis. 2008, 198, 1809–1817. [Google Scholar] [CrossRef] [PubMed]
- Wernette, C.M.; Frasch, C.E.; Madore, D.; Carlone, G.; Goldblatt, D.; Plikaytis, B.; Benjamin, W.; Quataert, S.A.; Hildreth, S.; Sikkema, D.J.; et al. Enzyme-Linked Immunosorbent Assay for Quantitation of Human Antibodies to Pneumococcal Polysaccharides. Clin. Vaccine Immunol. 2003, 10, 514–519. [Google Scholar] [CrossRef] [PubMed]
- McCartney, J.E.; Fraser, J. Pneumococcal peritonitis. Br. J. Surg. 1922, 9, 479–489. [Google Scholar] [CrossRef]
- Fuchs, I.; Dagan, R.; Givon-Lavi, N.; Greenberg, D. Serotype Childhood Invasive Pneumococcal Disease has Unique Characteristics Compared to Disease Caused by Other Streptococcus pneumoniae Serotypes. Pediatr. Infect. Dis. J. 2013, 32, 614–618. [Google Scholar] [CrossRef] [PubMed]
- Von Mollendorf, C.; Cohen, C.; Tempia, S.; Meiring, S.; De Gouveia, L.; Quan, V.; Lengana, S.; Karstaedt, A.; Dawood, H.; Seetharam, S.; et al. Epidemiology of Serotype 1 Invasive Pneumococcal Disease, South Africa, 2003–2013. Emerg. Infect. Dis. 2016, 22, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Brandenburg, L.-O.; Tauber, S.C. Do Innate Immune Gene Variations Contribute to Susceptibility and Severity of Pneumococcal Meningitis? Ebiomedicine 2016, 10, 9–10. [Google Scholar] [CrossRef] [PubMed]

| Laboratory Values Upon Hospital Admission | Patient 1 | Patient 2 | |
|---|---|---|---|
| WBC | ×10³/μL | 3.8 | 21.69 |
| Neutrophils | % | 84 | 95.6 |
| Lymphocytes | % | 8 | 2.2 |
| Monocytes | % | 3 | 0.8 |
| Hemoglobulin (HGb) | g/dL | 9.4 | 11.5 |
| Hematocrit (HCT) | % | 29.5 | 34.2 |
| Platelets (PLTs) | ×10³/μL | 343 | 241 |
| C-reactive protein | mg/L | 475 | 321 |
| Procalcitonin (PCT) | ng/mL | 26.12 | |
| Glucose | mg/dL | 109 | 84 |
| Urea | mg/dL | 10 | 29 |
| Creatinine | mg/dL | 0.25 | 0.40 |
| SGOT(AST) | U/L | 43 | 13 |
| SGPT(ALT) | U/L | 6 | 6 |
| γ-GT | U/L | 7 | 10 |
| ALP | U/L | 66 | 140 |
| Total Billirubin | mg/dL | 0.26 | 0.18 |
| Direct Billirubin | mg/dL | 0.12 | 0.09 |
| Total Protein | g/dL | 5.2 | 7.2 |
| Albumin | g/dL | 3.2 | 4.0 |
| Potassium | mmol/L | 3.6 | 3.9 |
| Sodium | mmol/L | 130 | 129 |
| Calcium | mg/dL | 8.6 | 10.1 |
| Signs and Symptoms Upon Hospital Admission | Patient 1 | Patient 2 | |
| Level of | yes | yes | |
| Tachypnoea & Tachycardia | yes | yes | |
| Dehydration (by clinical findings) | severe | moderate | |
| Auscultation of the Chest (findings) | left lower lobe: reduced breathing sounds | No abnormality detected (NAD) | |
| Palpitation of the Abdomen (findings) | Tenderness; generalized abdominal wall guarding; mild abdominal distension | significant abdominal distension;tenderness; generalized abdominal wall guarding | |
| Auscultation of the Abdomen (findings) | Scarce bowel sounds | Absent bowel sounds | |
| Patient | Protective Antibody Levels against IPD [6] | Serotype 1 | Serotype 3 | Serotype 9V | Serotype 19A |
|---|---|---|---|---|---|
| 1 (3-year-old) | >0.5 mg/L | 5.08 mg/L | 0.41 mg/L | 16.21 mg/L | 20.32 mg/L |
| 2 (7-year-old) | >0.5 mg/L | 7.32 mg/L | 0.85 mg/L | 8.01 mg/L | 11.73 mg/L |
| Immunoglobulins and Complement Factors | Patient 1 (Normal Range for Age) | Patient 2 (Normal Range for Age) | |
|---|---|---|---|
| IgG (nephelometry) | mg/dL | 2090.00 (955–1995) | 1810.00 (891–2042) |
| IgA (nephelometry) | mg/dL | 185 (85–214) | 163 (52–331) |
| IgM (nephelometry) | mg/dL | 148 (65–372) | 139 (63–275) |
| C3 (nephelometry) | mg/dL | 196 (90–180) | 147 (90–180) |
| C4 (nephelometry) | mg/dL | 57 (10–40) | 30 (10–40) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadatou, I.; Moudaki, A.; Mentessidou, A.; Tsakogiannis, D.; Georgiadou, E.; Spoulou, V. Intrafamilial Transmission of Pneumococcal Acute Spontaneous Peritonitis. Infect. Dis. Rep. 2023, 15, 299-306. https://doi.org/10.3390/idr15030030
Papadatou I, Moudaki A, Mentessidou A, Tsakogiannis D, Georgiadou E, Spoulou V. Intrafamilial Transmission of Pneumococcal Acute Spontaneous Peritonitis. Infectious Disease Reports. 2023; 15(3):299-306. https://doi.org/10.3390/idr15030030
Chicago/Turabian StylePapadatou, Ioanna, Angeliki Moudaki, Anastasia Mentessidou, Dimitrios Tsakogiannis, Elissavet Georgiadou, and Vana Spoulou. 2023. "Intrafamilial Transmission of Pneumococcal Acute Spontaneous Peritonitis" Infectious Disease Reports 15, no. 3: 299-306. https://doi.org/10.3390/idr15030030