
Long-Term Survivors in a Cohort of People Living with HIV Diagnosed between 1985 and 1994: Predictive Factors Associated with More Than 25 Years of Survival
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
- Epidemiological characteristics: sex, age, HIV exposure (IVDUs, MSMs, heterosexual transmission, transfusions).
- Clinical parameters: date of HIV diagnosis; baseline CD4+ T-cells count (cells/µL); CD8+ T-cells count (cells/µL); CD4+/CD8+ ratio; CD4+ nadir; HIV-RNA viral load (copies/mL), if available; HBsAg and HCV antibody test results; the first and the last recorded laboratory tests, including hemoglobin (g/dL), platelets count (×103/µL), creatinine (mg/dL), aspartate aminotransferase (UI/L), alanine aminotransferase (UI/L); date of most recent visit; antiretroviral therapy before the first cART; data of starting cART; AIDS-defining illnesses; AIDS presenter; date and cause of death.
2.2. Measurement of T-Cell Lymphocytes Subsets and HIV-RNA Plasma Viral Load
2.3. Inclusion Criteria
- All subjects with an ELISA antibody test positive for HIV, as confirmed with a Western Blot assay between 1 May 1985 and 31 December 1994.
- Age > 18 years.
2.4. Exclusion Criteria
- PLWH who were lost to follow-up or transferred to another ID center before completing the entire observation period (31 December 2019).
- Individuals who received the first diagnosis elsewhere.
2.5. Statistical Analysis
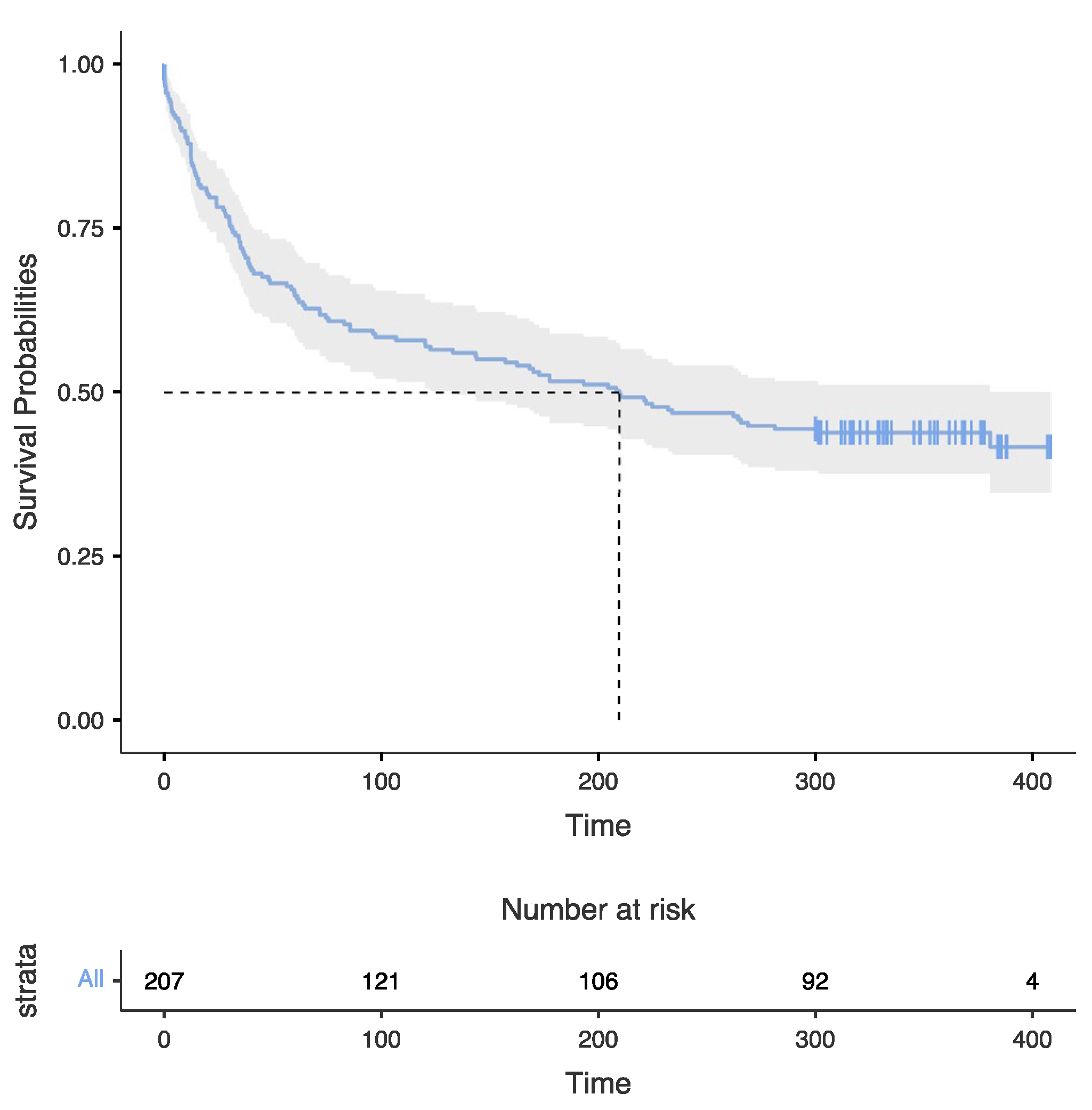
3. Results
3.1. Characteristics of the Population
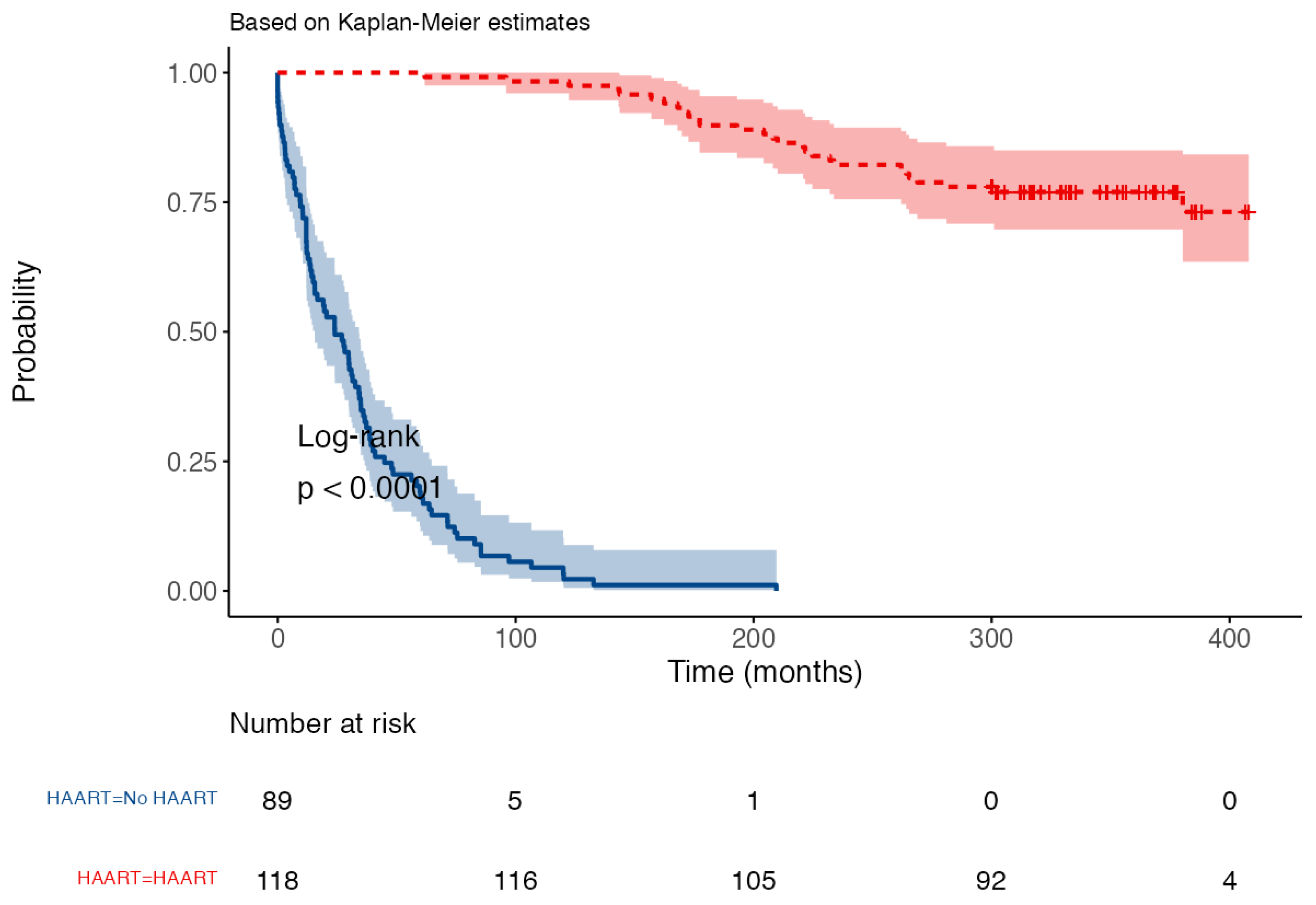
3.2. The “HAART Effect”
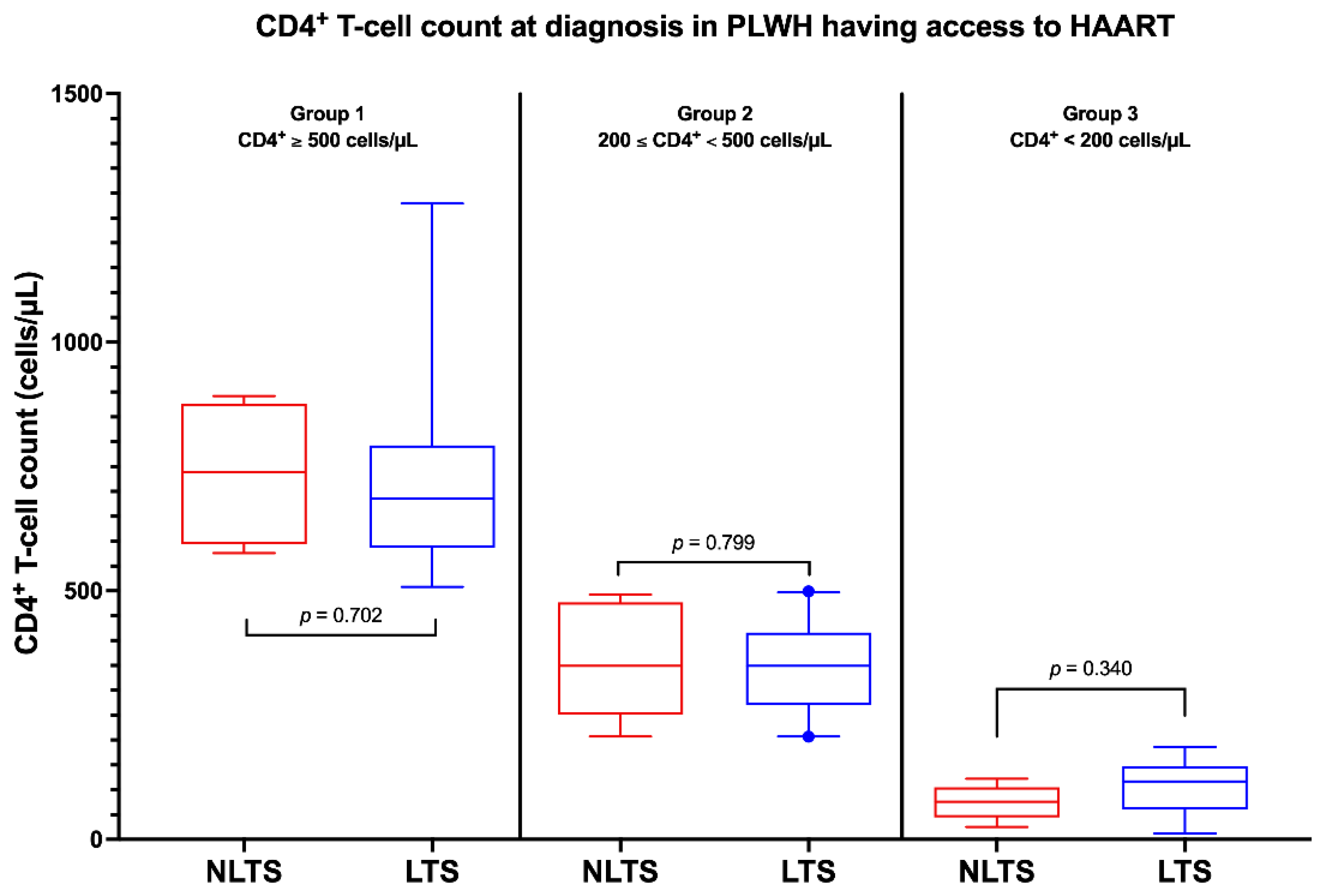
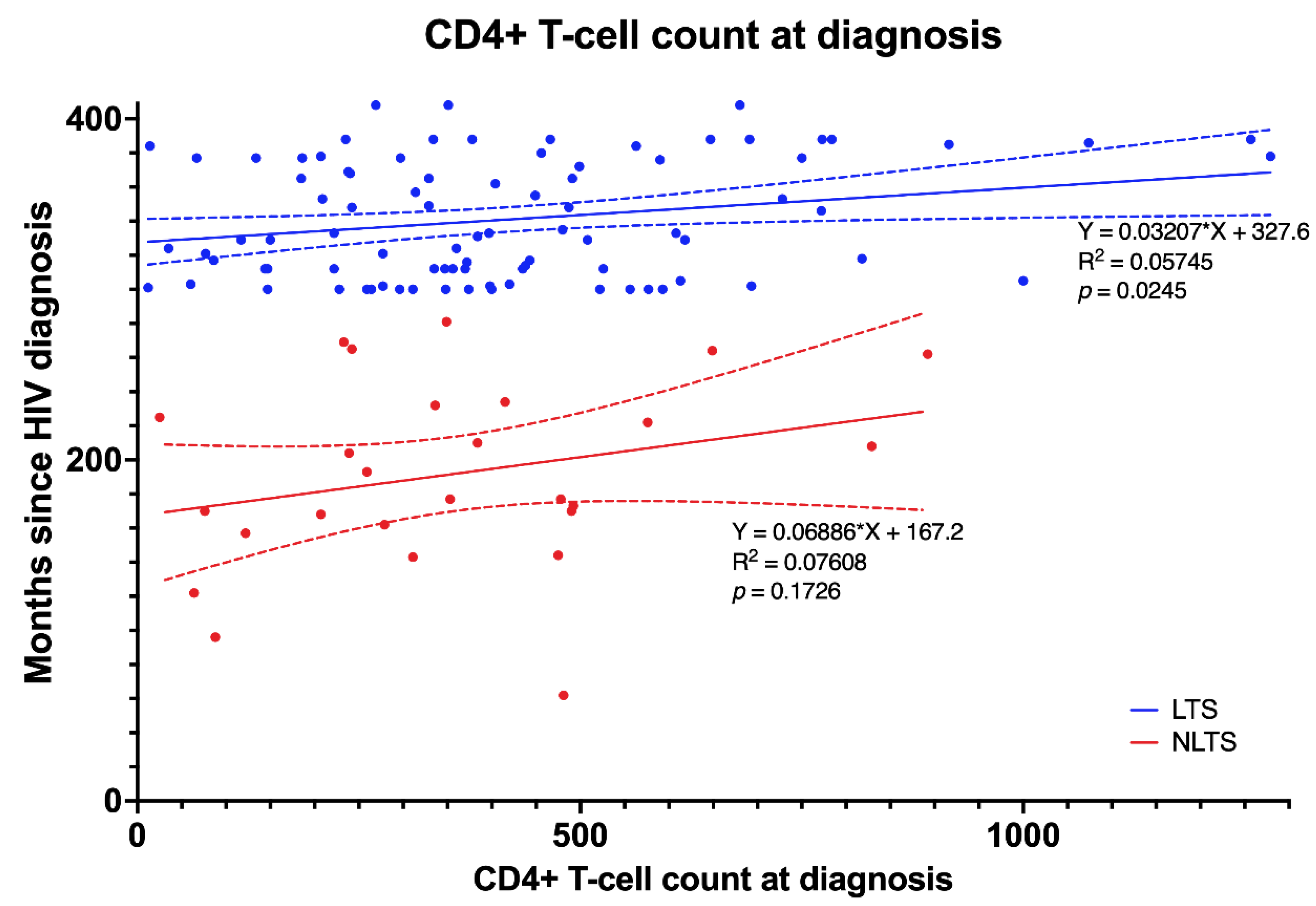
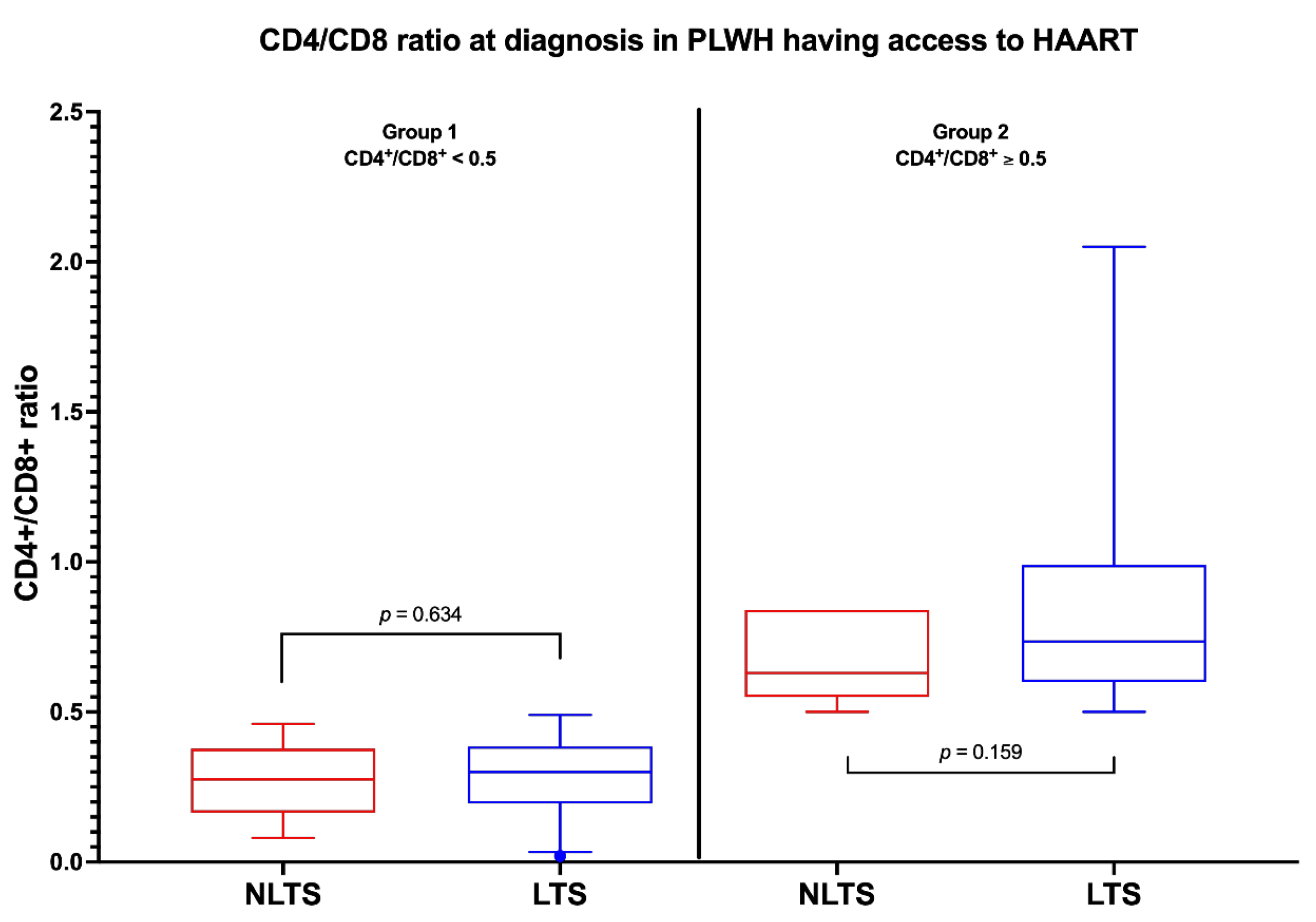
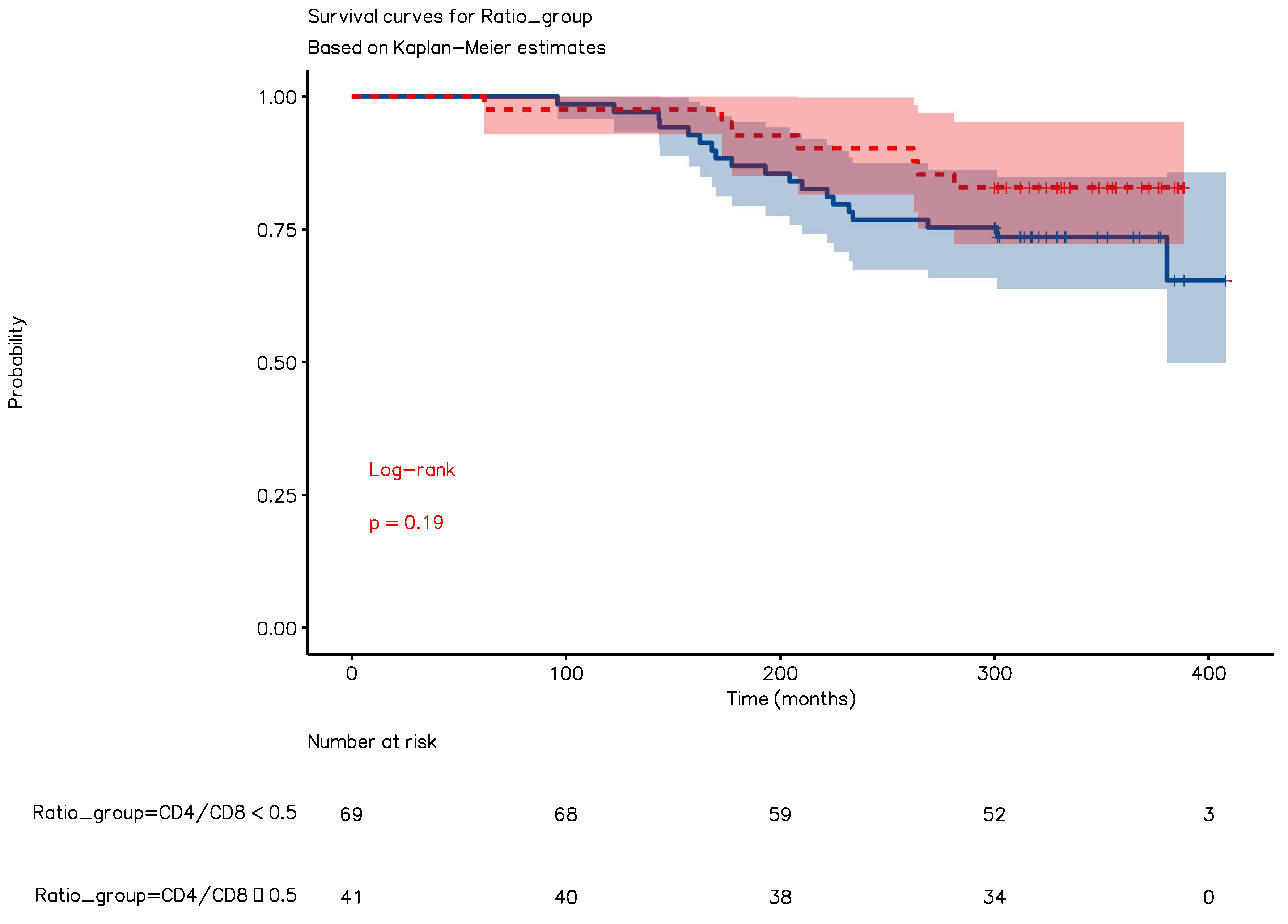
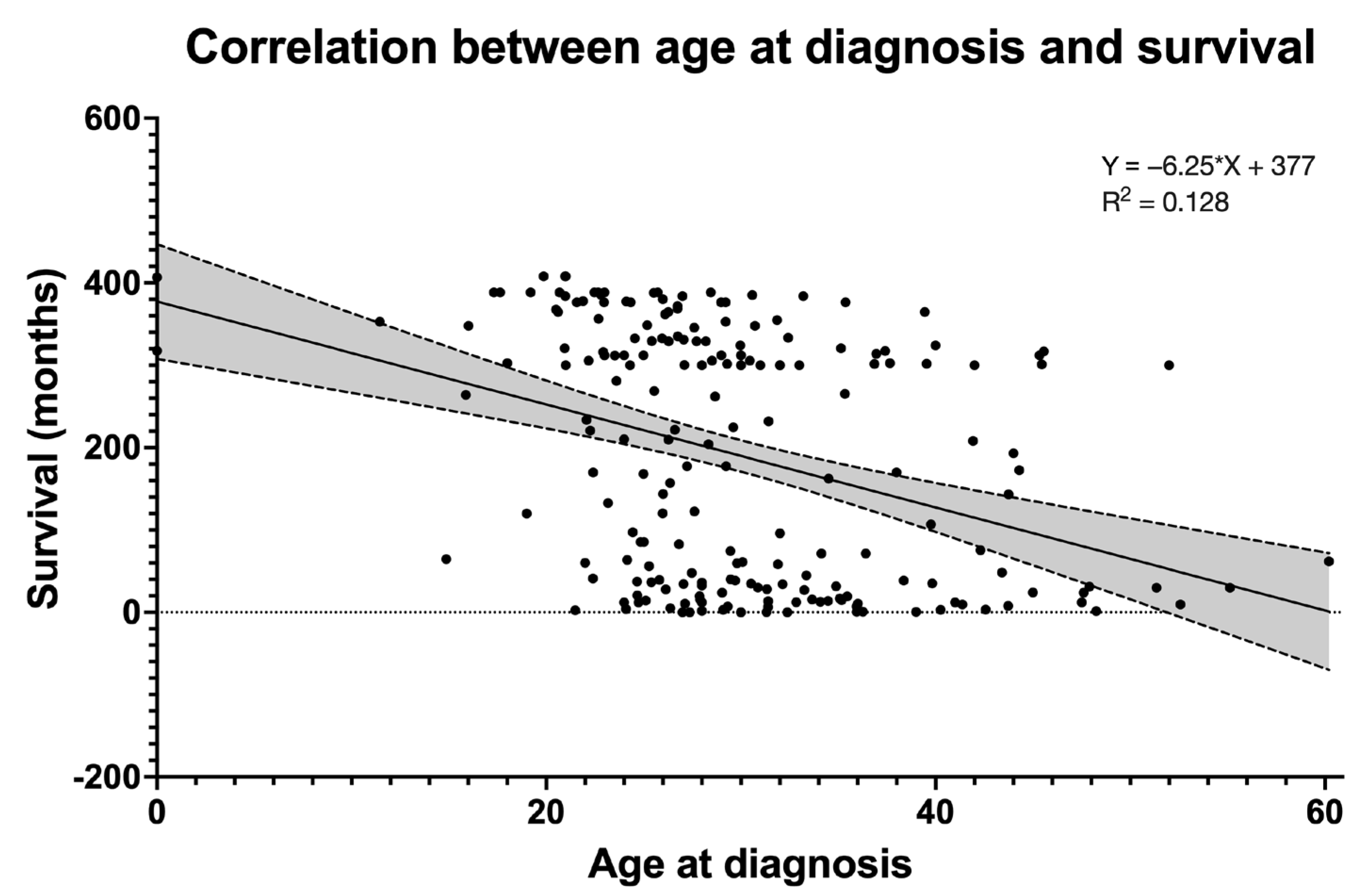
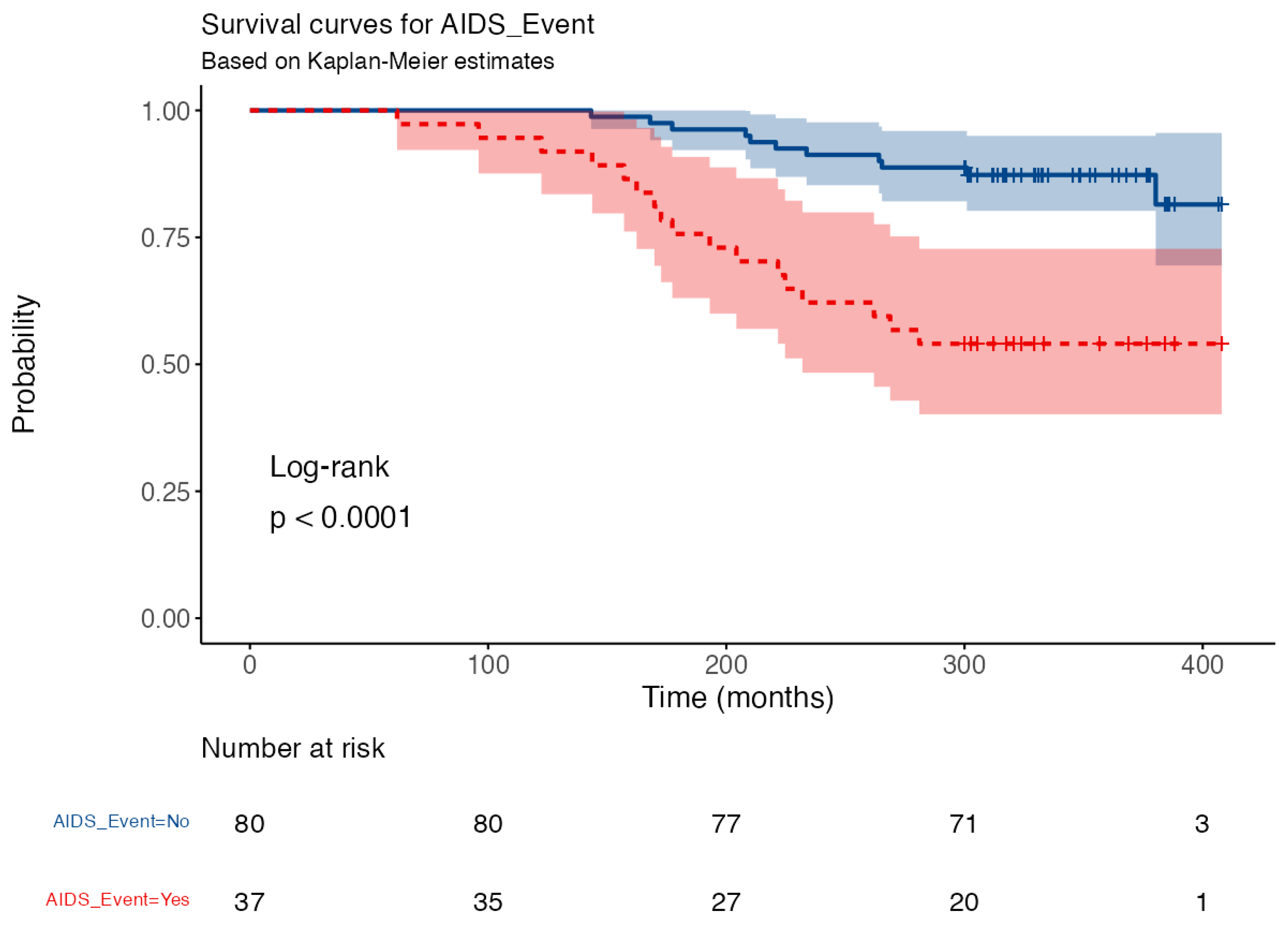
3.3. People Living with HIV Who Had Access to HAART
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNAIDS. UNAIDS Fact Sheet 2022. Available online: https://www.unaids.org/en/resources/documents/2022/UNAIDS_FactSheet (accessed on 9 December 2022).
- Ceccarelli, M.; Condorelli, F.; Rullo, E.V.; Pellicanò, G.F. Editorial—Improving Access and Adherence to Screening Tests for Cancers: A New, Though Old, Challenge in the HIV Epidemics. World Cancer Res. J. 2018, 5, e1030. [Google Scholar]
- D’Andrea, F.; Ceccarelli, M.; Rullo, E.V.; Facciolà, A.; D’Aleo, F.; Cacopardo, B.; Iacobello, C.; Costa, A.; Altavilla, G.; Pellicanò, G.F.; et al. Cancer Screening in HIV-Infected Patients: Early Diagnosis in a High-Risk Population. World Cancer Res. J. 2018, 5, e1130. [Google Scholar]
- Ceccarelli, M.; Rullo, E.V.; Marino, M.A.; D’Aleo, F.; Pellicanò, G.F.; D’Andrea, F.; Marino, A.; Cacopardo, B.; Celesia, B.M.; Rocca, G.L.; et al. Non-AIDS Defining Cancers: A Comprehensive Update on Diagnosis and Management. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3849–3875. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, F.; Ceccarelli, M.; Facciolà, A.; Nunnari, G.; Pellicanò, G.F.; Rullo, E.V. Breast Cancer in Women Living with HIV. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1158–1164. [Google Scholar] [CrossRef]
- Pinzone, M.R.; Ceccarelli, M.; Rullo, E.V.; Maresca, M.; Bruno, R.; Condorelli, F.; Rosa, M.D.; Madeddu, G.; Focà, E.; Calcagno, A.; et al. Circulating Angiopoietin-like Protein 2 Levels Are Associated with Decreased Renal Function in HIV+ Subjects on CART: A Potential Marker of Kidney Disease. Biom. Rep. 2019, 10, 140–144. [Google Scholar] [CrossRef]
- Marino, A.; Zafarana, G.; Ceccarelli, M.; Cosentino, F.; Moscatt, V.; Bruno, G.; Bruno, R.; Benanti, F.; Cacopardo, B.; Celesia, B.M. Immunological and Clinical Impact of DAA-Mediated HCV Eradication in a Cohort of HIV/HCV Coinfected Patients: Monocentric Italian Experience. Diagnostics 2021, 11, 2336. [Google Scholar] [CrossRef]
- Levy, J.A. HIV Pathogenesis and Long-Term Survival. Aids 1993, 7, 1401–1410. [Google Scholar] [CrossRef]
- McManus, H.; O’Connor, C.C.; Boyd, M.; Broom, J.; Russell, D.; Watson, K.; Roth, N.; Read, P.J.; Petoumenos, K.; Law, M.G.; et al. Long-Term Survival in HIV Positive Patients with up to 15 Years of Antiretroviral Therapy. PLoS ONE 2012, 7, e48839. [Google Scholar] [CrossRef] [Green Version]
- Rutherford, G.W. Long Term Survival in HIV-1 Infection. BMJ 1994, 309, 283. [Google Scholar] [CrossRef] [Green Version]
- Vuppula, S.; Tyungu, D.; Kaul, A.; Chandwani, S.; Rigaud, M.; Borkowsky, W. Thirty-Year Perspective of the Long-Term Survival, CD4 Percentage and Social Achievements of Perinatally HIV-Infected Children as a Function of Their Birth Era. Pediatric. Infect. Dis. J. 2017, 36, 198–201. [Google Scholar] [CrossRef]
- Wood, E.; Hogg, R.S.; Yip, B.; Harrigan, P.R.; O’Shaughnessy, M.V.; Montaner, J.S.G. Effect of Medication Adherence on Survival of HIV-Infected Adults Who Start Highly Active Antiretroviral Therapy When the CD4+ Cell Count Is 0.200 to 0.350 × 109 Cells/L. Ann. Intern. Med. 2003, 139, 810. [Google Scholar] [CrossRef] [PubMed]
- Colford, J.M.; Ngo, L.; Tager, I. Factors Associated with Survival in Human Immunodeficiency Virus-Infected Patients with Very Low CD4 Counts. Am. J. Epidemiol. 1994, 139, 206–218. [Google Scholar] [CrossRef] [PubMed]
- Marino, A.; Scuderi, D.; Locatelli, M.E.; Gentile, A.; Pampaloni, A.; Cosentino, F.; Ceccarelli, M.; Celesia, B.M.; Benanti, F.; Nunnari, G.; et al. Modification of Serum Brain-Derived Neurotrophic Factor Levels Following Anti-HCV Therapy with Direct Antiviral Agents: A New Marker of Neurocognitive Disorders. Hepat. Mon. 2020, 20, e95101. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.Y.; Feeney, E.R.; Chung, R.T. HCV and HIV Co-Infection: Mechanisms and Management. Nat. Rev. Gastroentero. 2014, 11, 362–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apolonio, E.G.; Hoover, D.R.; He, Y.; Saah, A.J.; Lyter, D.W.; Detels, R.; Kaslow, R.A.; Phair, J.P. Prognostic Factors in Human Immunodeficiency Virus-Positive Patients with a CD4+ Lymphocyte Count < 50/MicroL. J. Infect. Dis. 1995, 171, 829–836. [Google Scholar] [CrossRef]
- Antiretroviral Therapy Cohort Collaboration. Life Expectancy of Individuals on Combination Antiretroviral Therapy in High-Income Countries: A Collaborative Analysis of 14 Cohort Studies. Lancet Lond. Engl. 2008, 372, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Crum, N.F.; Riffenburgh, R.H.; Wegner, S.; Agan, B.K.; Tasker, S.A.; Spooner, K.M.; Armstrong, A.W.; Fraser, S.; Wallace, M.R.; Triservice AIDS Clinical Consortium. Comparisons of Causes of Death and Mortality Rates Among HIV-Infected Persons. Jaids. J. Acquir. Immune. Defic. Syndr. 2006, 41, 194–200. [Google Scholar] [CrossRef]
- Elkbuli, A.; Polcz, V.; Dowd, B.; McKenney, M.; Prado, G. HIV Prevention Intervention for Substance Users: A Review of the Literature. Subst. Abus. Treat. Prev. Policy 2019, 14, 1. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.J.; Jordan, A.E.; Frank, M.; Hagan, H. Spontaneous Viral Clearance of Hepatitis C Virus (HCV) Infection among People Who Inject Drugs (PWID) and HIV-Positive Men Who Have Sex with Men (HIV+ MSM): A Systematic Review and Meta-Analysis. BMC Infect. Dis. 2016, 16, 471. [Google Scholar] [CrossRef] [Green Version]
- Celesia, B.M.; Marino, A.; Vecchio, R.F.D.; Bruno, R.; Palermo, F.; Gussio, M.; Nunnari, G.; Cacopardo, B. Is It Safe and Cost Saving to Defer the CD4+ Cell Count Monitoring in Stable Patients on Art with More than 350 or 500 Cells/Μl? Mediterr. J. Hematol. Infect. Dis. 2019, 11, e2019063. [Google Scholar] [CrossRef]
- HIV-CAUSAL Collaboration; Ray, M.; Logan, R.; Sterne, J.A.C.; Hernández-Díaz, S.; Robins, J.M.; Sabin, C.; Bansi, L.; van Sighem, A.; de Wolf, F.; et al. The Effect of Combined Antiretroviral Therapy on the Overall Mortality of HIV-Infected Individuals. Aids 2010, 24, 123–137. [Google Scholar] [CrossRef] [Green Version]
- Mateo-Urdiales, A.; Johnson, S.; Nachega, J.B.; Eshun-Wilson, I. Rapid Initiation of Antiretroviral Therapy for People Living with HIV. Cochrane Db. Syst. Rev. 2019, 6, CD012962. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Li, J.; Zhou, S.; Xia, X.; Xie, Z.; Liu, P.; Xu, Y.; Qian, Y.; Zhang, H.; Ma, L.; et al. Prognosis of HIV Patients Receiving Antiretroviral Therapy According to CD4 Counts: A Long-Term Follow-up Study in Yunnan, China. Sci. Rep. 2017, 7, 9595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; May, M.; Chêne, G.; Phillips, A.N.; Ledergerber, B.; Dabis, F.; Costagliola, D.; Monforte, A.D.; de Wolf, F.; Reiss, P.; et al. Prognosis of HIV-1-Infected Patients Starting Highly Active Antiretroviral Therapy: A Collaborative Analysis of Prospective Studies. Lancet 2002, 360, 119–129. [Google Scholar] [CrossRef]
- Goedert, J.J.; Biggar, R.J.; Melbye, M.; Mann, D.L.; Wilson, S.; Gail, M.H.; Grossman, R.J.; DiGioia, R.A.; Sanchez, W.C.; Weiss, S.H.; et al. Effect of T4 Count and Cofactors on the Incidence of AIDS in Homosexual Men Infected With Human Immunodeficiency Virus. JAMA 1987, 257, 331–334. [Google Scholar] [CrossRef]
- Polk, B.F.; Fox, R.; Brookmeyer, R.; Kanchanaraksa, S.; Kaslow, R.; Visscher, B.; Rinaldo, C.; Phair, J. Predictors of the Acquired Immunodeficiency Syndrome Developing in a Cohort of Seropositive Homosexual Men. N. Engl. J. Med. 1987, 316, 61–66. [Google Scholar] [CrossRef]
- Croxford, S.; Kitching, A.; Desai, S.; Kall, M.; Edelstein, M.; Skingsley, A.; Burns, F.; Copas, A.; Brown, A.E.; Sullivan, A.K.; et al. Mortality and Causes of Death in People Diagnosed with HIV in the Era of Highly Active Antiretroviral Therapy Compared with the General Population: An Analysis of a National Observational Cohort. Lancet Public Health 2017, 2, e35–e46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Group, I.S.S.; Lundgren, J.D.; Babiker, A.G.; Gordin, F.; Emery, S.; Grund, B.; Sharma, S.; Avihingsanon, A.; Cooper, D.A.; Fätkenheuer, G.; et al. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Population (n = 210) | N | % |
|---|---|---|---|
| Sex | M * | 158 | 75.24% |
| F * | 52 | 24.76% | |
| Age (median, IQR *) | 28 (25–34) years | ||
| Year of HIV * diagnosis | 1983–1989 | 95 | 45.24% |
| 1990–1994 | 115 | 54.76% | |
| HCV * positivity | Yes | 101 | 48.10% |
| No | 100 | 47.62% | |
| Not known | 9 | 4.29% | |
| HBV * positivity | Yes | 5 | 2.38% |
| No | 196 | 93.33% | |
| Not known | 9 | 4.29% | |
| Risk factors | IDUs * | 100 | 47.62% |
| MSMs * | 42 | 20% | |
| Heterosexual transmission | 50 | 23.81% | |
| Multiple transfusions | 13 | 6.19% | |
| Not known | 5 | 2.38% | |
| AIDS * presenter | Yes | 69 | 32.86% |
| No | 139 | 66.19% | |
| Not known | 2 | 0.95% | |
| AIDS * during the period of interest | Yes | 116 | 55.24% |
| No | 92 | 43.81% | |
| Not known | 2 | 0.95% | |
| CD4+ at diagnosis, cell/µL, median, IQR | 234 (IQR 54–439) | ||
| CD4+ nadir at diagnosis, cell/µL, median, IQR | 35 (IQR 14–94) | ||
| N | % | ||
|---|---|---|---|
| LTS * | 93 | 44.29 | |
| NLTS * | 116 | 55.24 | |
| Not known | 1 | 0.48 | |
| Cause of death | AIDS *-related | 98 | 83.05 |
| HCV *-related | 9 | 7.63 | |
| Non-AIDS * malignancy | 4 | 3.39 | |
| Cardiovascular diseases | 4 | 3.39 | |
| Overdose | 3 | 2.54 | |
| Year of Diagnosis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1983 | 1985 | 1986 | 1987 | 1988 | 1989 | 1990 | 1991 | 1992 | 1993 | 1994 | ||
| No AIDS * | NLTS * | 0 | 10 | 4 | 6 | 4 | 3 | 8 | 5 | 7 | 1 | 1 |
| LTS * | 1 | 17 | 8 | 8 | 6 | 2 | 11 | 9 | 11 | 8 | 9 | |
| AIDS * | NLTS * | 1 | 3 | 4 | 2 | 5 | 10 | 7 | 14 | 13 | 6 | 1 |
| LTS * | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 2 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cosentino, F.; Marino, A.; Anile, L.; Moscatt, V.; Gussio, M.; Boscia, V.; Bruno, R.; Nunnari, G.; Pulvirenti, A.; Privitera, G.F.; et al. Long-Term Survivors in a Cohort of People Living with HIV Diagnosed between 1985 and 1994: Predictive Factors Associated with More Than 25 Years of Survival. Infect. Dis. Rep. 2023, 15, 70-83. https://doi.org/10.3390/idr15010008
Cosentino F, Marino A, Anile L, Moscatt V, Gussio M, Boscia V, Bruno R, Nunnari G, Pulvirenti A, Privitera GF, et al. Long-Term Survivors in a Cohort of People Living with HIV Diagnosed between 1985 and 1994: Predictive Factors Associated with More Than 25 Years of Survival. Infectious Disease Reports. 2023; 15(1):70-83. https://doi.org/10.3390/idr15010008
Chicago/Turabian StyleCosentino, Federica, Andrea Marino, Laura Anile, Vittoria Moscatt, Maria Gussio, Vincenzo Boscia, Roberto Bruno, Giuseppe Nunnari, Alfredo Pulvirenti, Grete Francesca Privitera, and et al. 2023. "Long-Term Survivors in a Cohort of People Living with HIV Diagnosed between 1985 and 1994: Predictive Factors Associated with More Than 25 Years of Survival" Infectious Disease Reports 15, no. 1: 70-83. https://doi.org/10.3390/idr15010008