
Kinetics of Anti-SARS-CoV-2 Antibody Response Following Two Doses of the BNT162b2 mRNA Vaccine: A Japanese Single-Center Primary Care Clinic Report Involving Volunteers and Patients with Autoimmune Disease
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measurement of Antibody Titers
2.4. Kinetic Graph
2.5. Antibody Data Comparison
2.6. Statistical Analysis
3. Results
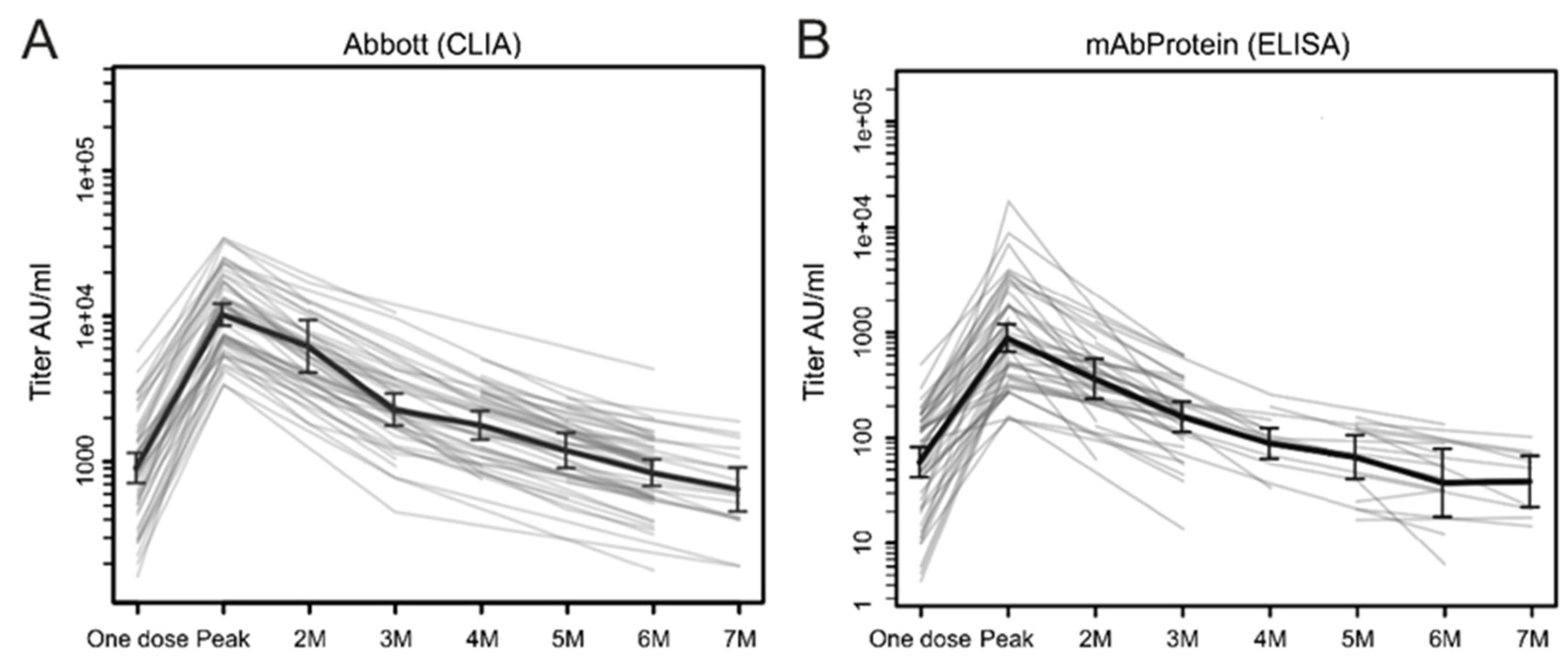
3.1. Kinetics of Antibody Response
3.2. Interindividual Differences in Antibody Titers
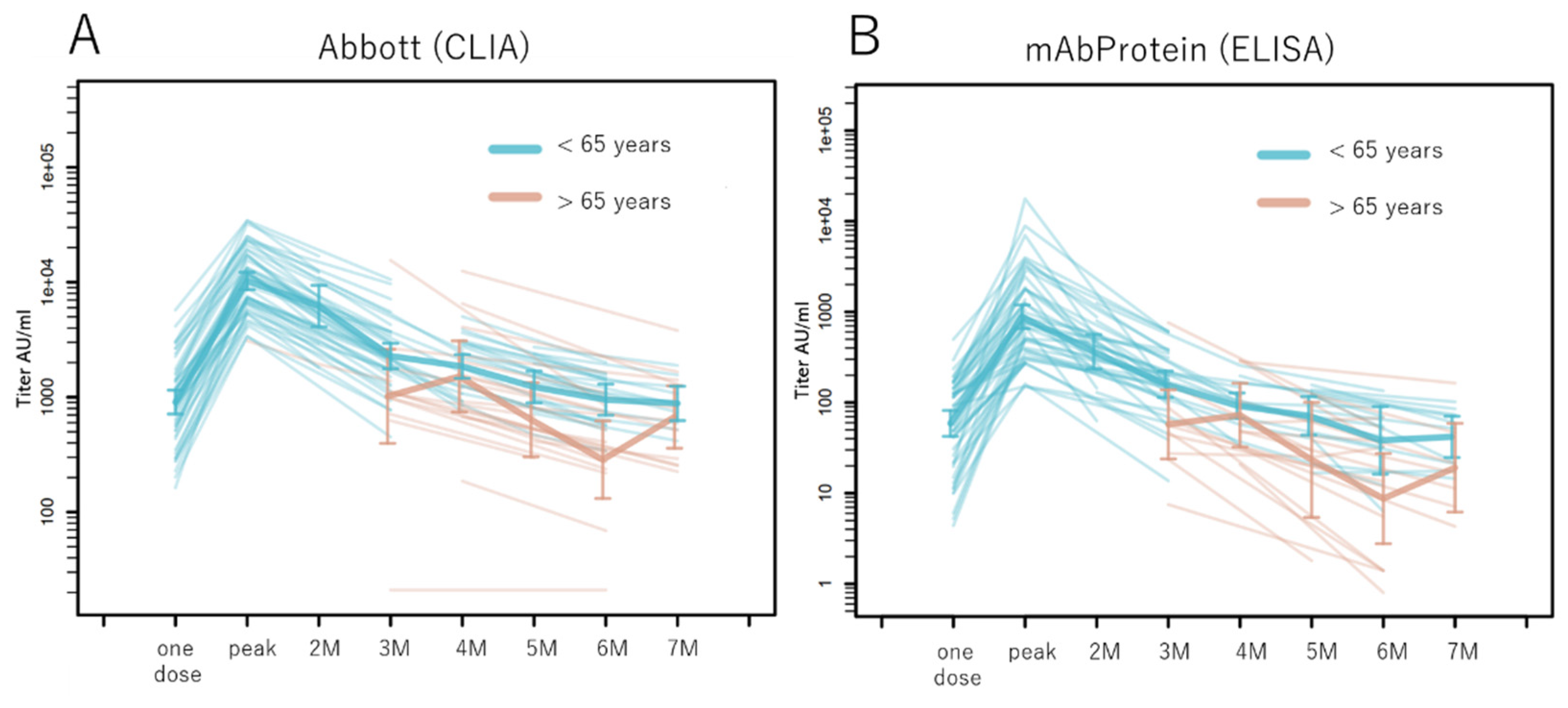
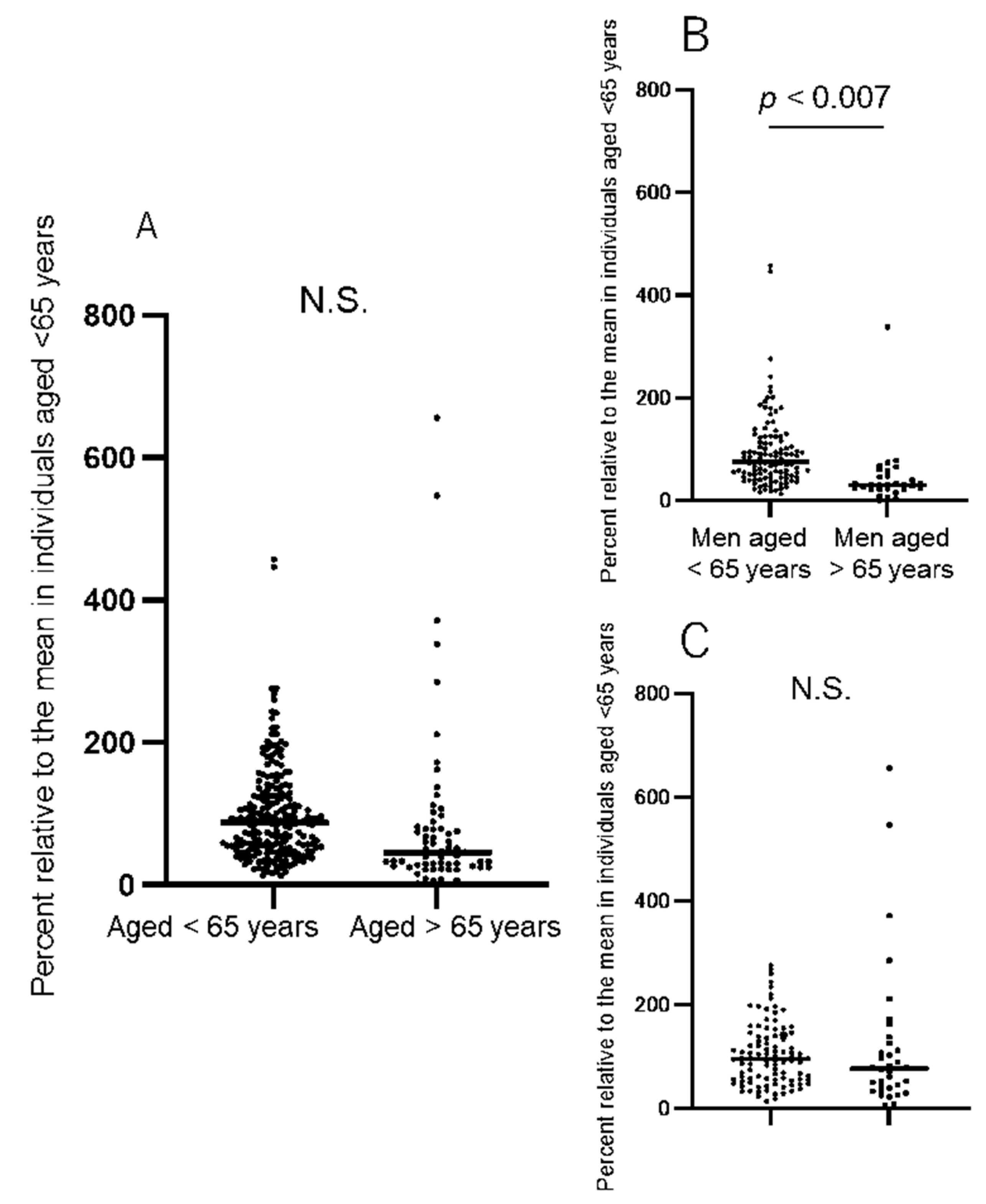
3.3. Antibody Titers in the Older Population
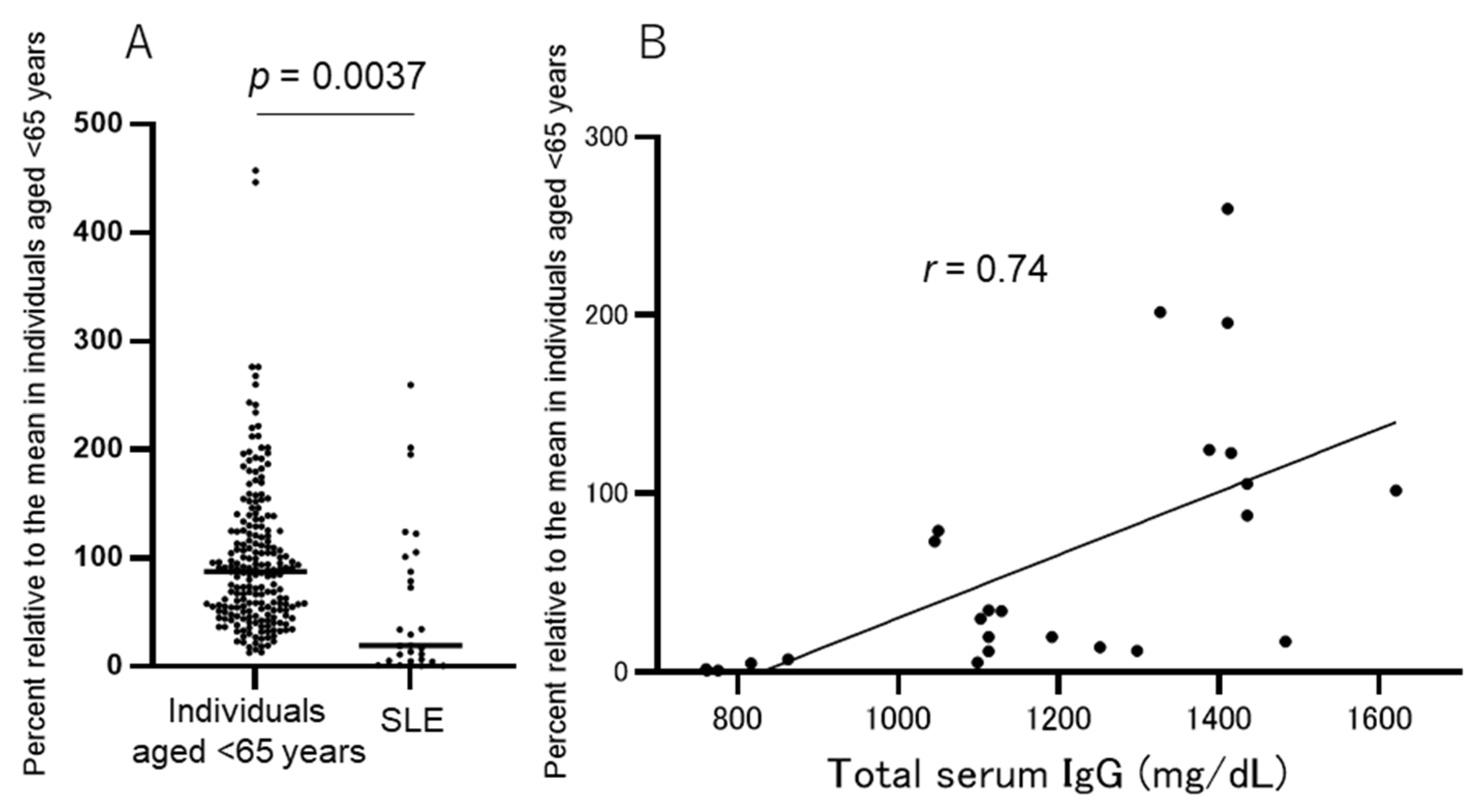
3.4. Immunosuppressed Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, T.; Ikeda, K.; Tanaka, S.; Tanigtiuchi, T.; Igari, H.; Onouchi, Y.; Kaneda, A.; Matsushita, K.; Matsushita, K.; Nakada, T.A.; et al. Antibody responses to BNT162b2 mRNA COVID-19 vaccine and their predictors among healthcare workers in a tertiary referral hospital in Japan. Clin. Microbiol. Infect. 2021, 27, 1861.e1–1861.e5. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Amano, M.; Uemura, Y.; Tsuchiya, K.; Matsushima, T.; Noda, K.; Shimizu, Y.; Fujiwara, A.; Takamatsu, Y.; Ichikawa, Y.; et al. Correlates of neutralizing/SARS-CoV-2-S1-binding antibody response with adverse effects and immune kinetics in BNT162b2-vaccinated individuals. Sci. Rep. 2021, 11, 22848. [Google Scholar] [CrossRef] [PubMed]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef] [PubMed]
- Đaković Rode, O.; Bodulić, K.; Zember, S.; Cetinić Balent, N.; Novokmet, A.; Čulo, M.; Rašić, Ž.; Mikulić, R.; Markotić, A. Decline of anti-SARS-CoV-2 IgG antibody levels 6 months after complete BNT162b2 vaccination in healthcare workers to levels observed following the first vaccine dose. Vaccines 2022, 10, 153. [Google Scholar] [CrossRef] [PubMed]
- Israel, A.; Merzon, E.; Schäffer, A.A.; Shenhar, Y.; Green, I.; Golan-Cohen, A.; Ruppin, E.; Magen, E.; Vinker, S. Elapsed time since BNT162b2 vaccine and risk of SARS-CoV-2 infection in a large cohort. medRxiv 2021. [Google Scholar] [CrossRef]
- Nachtigall, I.; Bonsignore, M.; Hohenstein, S.; Bollmann, A.; Günther, R.; Kodde, C.; Englisch, M.; Ahmad-Nejad, P.; Schröder, A.; Glenz, C.; et al. Effect of gender, age and vaccine on reactogenicity and incapacity to work after COVID-19 vaccination: A survey among health care workers. BMC Infect Dis. 2022, 22, 291. [Google Scholar] [CrossRef] [PubMed]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent immune response to the Biontech/Pfizer BNT162b2 coronavirus disease 2019 vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.; Ursini, F.; Gragnani, L.; Raimondo, V.; Giuggioli, D.; Foti, R.; Caminiti, M.; Olivo, D.; Cuomo, G.; Visentini, M.; et al. Impaired immunogenicity to COVID-19 vaccines in autoimmune systemic diseases. High prevalence of non-response in different patients’ subgroups. J. Autoimmun. 2021, 125, 102744. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann. Rheum. Dis. 2021, 80, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Izmirly, P.M.; Kim, M.Y.; Samanovic, M.; Fernandez-Ruiz, R.; Ohana, S.; Deonaraine, K.K.; Engel, A.J.; Masson, M.; Xie, X.; Cornelius, A.R.; et al. Evaluation of immune response and disease status in systemic lupus erythematosus patients following SARS-CoV-2 vaccination. Arthritis. Rheumatol. 2022, 74, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Evans, J.P.; Reisinger, S.; Woyach, J.; Liscynesky, C.; El Boghdadly, Z.E.; Rubinstein, M.P.; Chakravarthy, K.; Saif, L.; Oltz, E.M.; et al. Impaired neutralizing antibody response to COVID-19 mRNA vaccines in cancer patients. Cell Biosci. 2021, 11, 197. [Google Scholar] [CrossRef] [PubMed]
- Demaret, J.; Corroyer-Simovic, B.; Alidjinou, E.K.; Goffard, A.; Trauet, J.; Miczek, S.; Vuotto, F.; Dendooven, A.; Huvent-Grelle, D.; Podvin, J.; et al. Impaired functional T-cell response to SARS-CoV-2 after two doses of BNT162b2 mRNA vaccine in older people. Front. Immunol. 2021, 12, 778679. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Morell, A.; Terry, W.D.; Waldmann, T.A. Metabolic properties of IgG subclasses in man. J. Clin. Investig. 1970, 49, 673–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Ramirez, S.I.; Ramirez, S.I.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- Wajnberg, A.; Amanat, F.; Firpo, A.; Altman, D.R.; Bailey, M.J.; Mansour, M.; McMahon, M.; Meade, P.; Mendu, D.R.; Muellers, K.; et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science 2020, 370, 1227–1230. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Klein, S.L.; Garibaldi, B.T.; Li, H.; Wu, C.; Osevala, N.M.; Li, T.; Margolick, J.B.; Pawelec, G.; Leng, S.X. Aging in COVID-19: Vulnerability, immunity and intervention. Ageing Res. Rev. 2021, 65, 101205. [Google Scholar] [CrossRef] [PubMed]
- Deepak, P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, A.B.; El-Qunni, A.A.; Haile, A.; Huang, K.; Kinnett, B.; Liebeskind, M.J.; et al. Glucocorticoids and B cell depleting agents substantially impair immunogenicity of mRNA vaccines to SARS-CoV-2. medRxiv 2021. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Timing of Blood Sampling after the Second Dose | n | Abbott (CLIA) | mAbProtein (ELISA) | ||
|---|---|---|---|---|---|
| Mean ± SD (AU/mL) | Median (95% CI) (AU/mL) | Mean ± SD (AU/mL) | Median (95% CI) (AU/mL) | ||
| The same day (time point 0) | 50 | 1253 ± 1098 | 917 (720–1202) | 96.4 ± 89.4 | 77.2 (61.1–101.6) |
| 2–3 W after (peak point) | 53 | 12,406 ± 8014 | 10,983 (7171–13,045) | 1356.5 ± 1461.2 | 759.1 (512.3–931.7) |
| 2 M after (42–67 days) | 18 | 6030 ± 4332 | 5302 (2941–7337) | 363.8 ± 226.1 | 366.9 (201–524.3) |
| 3 M after (68–97 days) | 56 | 2322 ± 1751 | 2129 (1638–2409) | 163.9 ± 121 | 145.4 (117–172) |
| 4 M after (98–125 days) | 18 | 2305 ± 1204 | 2304 (1208–3061) | 98.2 ± 59.7 | 91.3 (60.4–153) |
| 5 M after (126–153 days) | 16 | 1296 ± 656 | 1083 (768–1734) | 83.7 ± 50.7 | 81.5 (59–133.3) |
| 6 M after (154–181 days) | 51 | 945 ± 662 | 888 (585–990) | 48.7 ± 34.6 | 42.7 (32.5–55) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugiura, T.; Sugiura, H.; Kato, H.; Nariai, Y.; Mizumoto, Y.; Hanada, K.; Takahashi, R.; Hinotubo, Y.; Tanaka, N.; Sasaki, M.; et al. Kinetics of Anti-SARS-CoV-2 Antibody Response Following Two Doses of the BNT162b2 mRNA Vaccine: A Japanese Single-Center Primary Care Clinic Report Involving Volunteers and Patients with Autoimmune Disease. Infect. Dis. Rep. 2023, 15, 24-33. https://doi.org/10.3390/idr15010003
Sugiura T, Sugiura H, Kato H, Nariai Y, Mizumoto Y, Hanada K, Takahashi R, Hinotubo Y, Tanaka N, Sasaki M, et al. Kinetics of Anti-SARS-CoV-2 Antibody Response Following Two Doses of the BNT162b2 mRNA Vaccine: A Japanese Single-Center Primary Care Clinic Report Involving Volunteers and Patients with Autoimmune Disease. Infectious Disease Reports. 2023; 15(1):24-33. https://doi.org/10.3390/idr15010003
Chicago/Turabian StyleSugiura, Tomoko, Hiroaki Sugiura, Hiroaki Kato, Yuko Nariai, Yuuki Mizumoto, Kozue Hanada, Rieko Takahashi, Yukari Hinotubo, Naoko Tanaka, Mutsumi Sasaki, and et al. 2023. "Kinetics of Anti-SARS-CoV-2 Antibody Response Following Two Doses of the BNT162b2 mRNA Vaccine: A Japanese Single-Center Primary Care Clinic Report Involving Volunteers and Patients with Autoimmune Disease" Infectious Disease Reports 15, no. 1: 24-33. https://doi.org/10.3390/idr15010003