
HIV Infection Indicator Disease-Based Active Case Finding in a University Hospital: Results from the SHOT Project
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
Ethical Issues
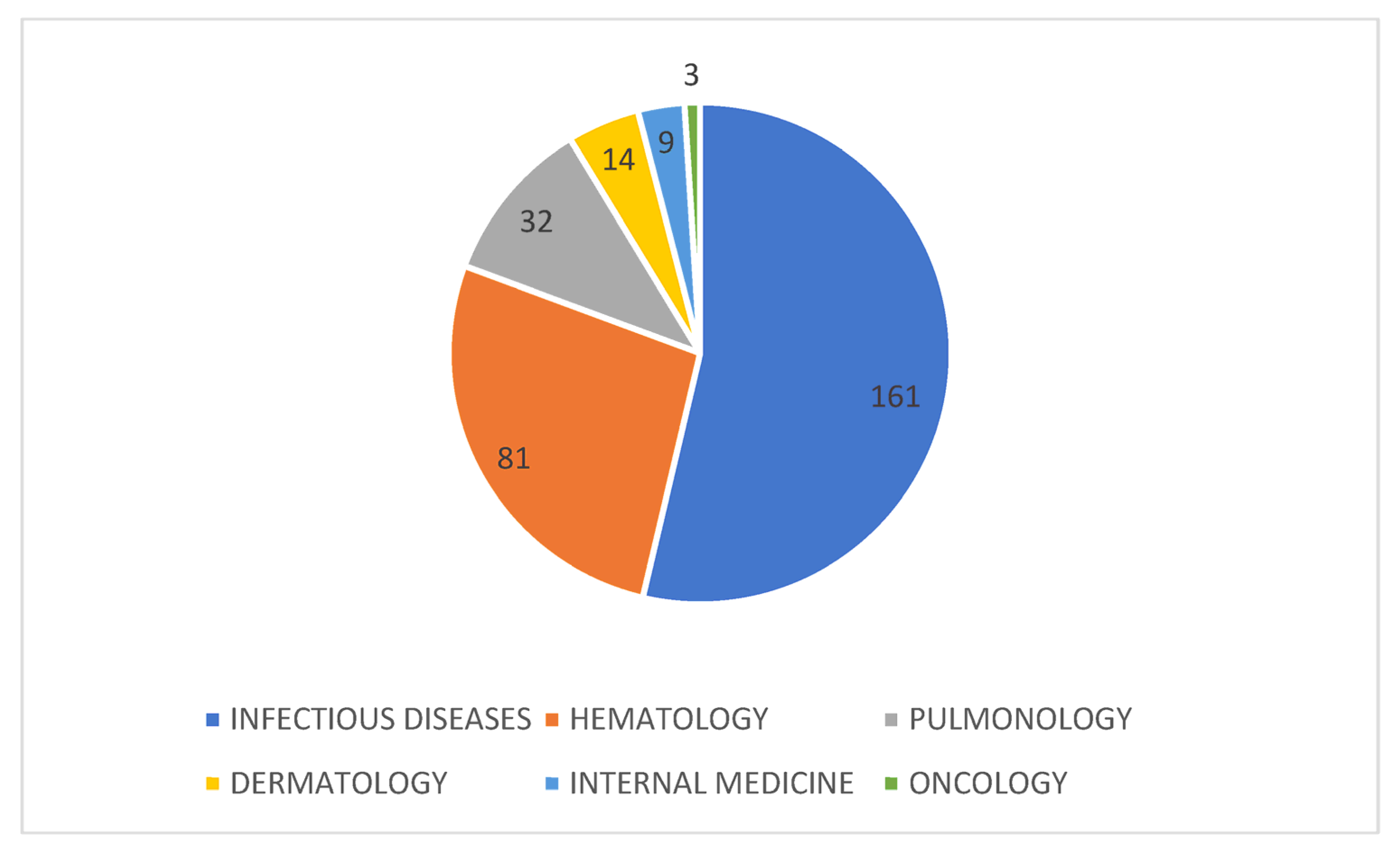
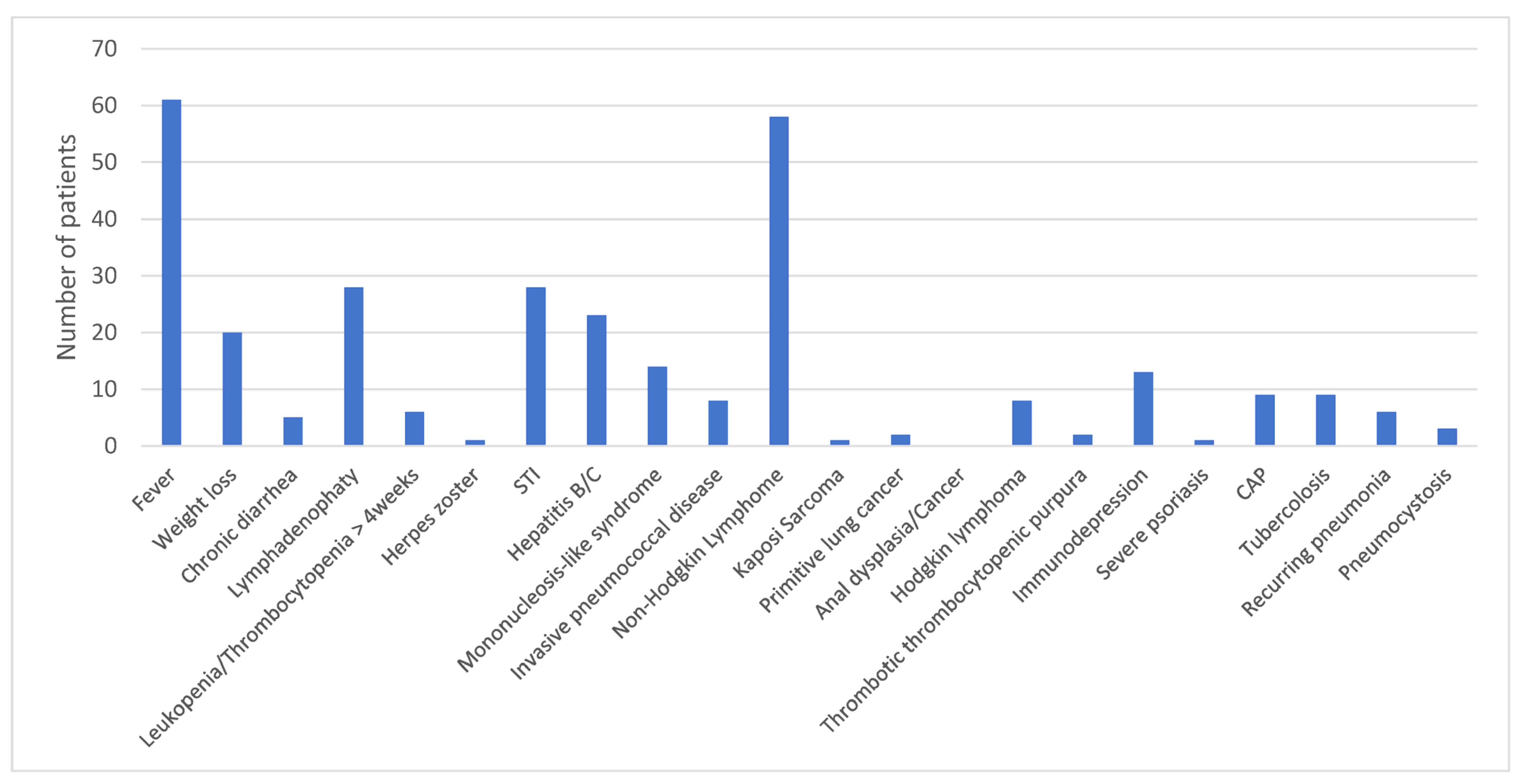
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fettig, J.; Swaminathan, M.; Murrill, C.S.; Kaplan, J.E. Global epidemiology of HIV. Infect. Dis. Clin. North Am. 2014, 28, 323–337. Available online: https://pubmed.ncbi.nlm.nih.gov/25151559/ (accessed on 10 November 2022). [CrossRef] [PubMed] [Green Version]
- WHO. Fact Sheets HIV. Available online: https://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed on 13 November 2022).
- Sabin, C.A.; Lundgren, J.D. The natural history of HIV infection. Curr. Opin. HIV AIDS 2013, 8, 311. Available online: https://pmc/articles/PMC4196796/ (accessed on 10 November 2022). [CrossRef] [PubMed]
- Boyd, M.A.; Boffito, M.; Castagna, A.; Estrada, V. Rapid initiation of antiretroviral therapy at HIV diagnosis: Definition, process, knowledge gaps. HIV Med. 2019, 20, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodger, A.J.; Cambiano, V.; Bruun, T.; Vernazza, P.; Collins, S.; Corbelli, G.M.; Degen, O.; Estrada, V.; Geretti, A.; Beloukas, A. Risk of HIV transmission through condomless sex in MSM couples with suppressive ART: The PARTNER2 Study extended results in gay men. AIDS 2018 Oral Abstract. J. Int. AIDS Soc. 2018, 21, 163. [Google Scholar]
- Rodger, A.J.; Cambiano, V.; Bruun, T.; Vernazza, P.; Collins, S.; van Lunzen, J.; Corbelli, G.M.; Estrada, V.; Geretti, A.M.; Beloukas, A.; et al. Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner is using suppressive antiretroviral therapy. J. Am. Med. Assoc. 2016, 316, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Rodger, A.J.; Cambiano, V.; Bruun, T.; Vernazza, P.; Collins, S.; Degen, O.; Corbelli, G.M.; Estrada, V.; Geretti, A.M.; Beloukas, A.; et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): Final results of a multicentre, prospective, observational study. Lancet 2019, 393, 2428–2438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, M.S.; McCauley, M.; Gamble, T.R. HIV treatment as prevention and HPTN 052. Curr. Opin. HIV AIDS 2012, 7, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Bavinton, B.R.; the Opposites Attract Study Group; Jin, F.; Prestage, G.; Zablotska, I.; Koelsch, K.K.; Phanuphak, N.; Grinsztejn, B.; Cooper, D.A.; Fairley, C.; et al. The Opposites Attract Study of viral load, HIV treatment and HIV transmission in serodiscordant homosexual male couples: Design and methods. BMC Public Health 2014, 14, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Group TISS. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, N.; Migone, C.; Calmy, A.; Kerschberger, B.; Kanters, S.; Nsanzimana, S.; Mills, E.J.; Meintjes, G.; Vitoria, M.; Doherty, M.; et al. Benefits and risks of rapid initiation of antiretroviral therapy. AIDS 2018, 32, 17–23. Available online: https://pubmed.ncbi.nlm.nih.gov/29112073/ (accessed on 10 November 2022). [CrossRef] [Green Version]
- UNAIDS 2025. Available online: https://aidstargets2025.unaids.org/assets/images/prevailing-against-pandemics_en.pdf (accessed on 10 November 2022).
- Global HIV & AIDS Statistics—Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 10 November 2022).
- Notiziario dell’Istituto superiore di Sanità: Aggiornamento delle nuove diagnosi di infezione da HIV e dei casi di AIDS in Italia. Available online: https://www.iss.it/documents/20126/5278313/COA+2022.pdf/b518925d-7663-cc23-610f-5f98b23a565d?t=1669622871324 (accessed on 10 November 2022).
- De Vito, A.; Colpani, A.; Zauli, B.; Meloni, M.C.; Fois, M.; Fiore, V.; Pintus, G.A.; Nardi, V.G.; Babudieri, S.; Madeddu, G. How Little Do We Know about HIV and STIs Prevention? Results from a Web-Based Survey among the General Population. Healthcare 2022, 10, 1059. Available online: https://www.mdpi.com/2227-9032/10/6/1059/html (accessed on 10 November 2022). [CrossRef] [PubMed]
- Fast-Track Cities: Ending the Aids Epidemic. Available online: https://www.unaids.org/sites/default/files/media_asset/20141201_Paris_Declaration_en.pdf (accessed on 10 November 2022).
- Ziersch, A.; Walsh, M.; Baak, M.; Rowley, G.; Oudih, E.; Mwanri, L. “It is not an acceptable disease”: A qualitative study of HIV-related stigma and discrimination and impacts on health and wellbeing for people from ethnically diverse backgrounds in Australia. BMC Public Heal. 2021, 21, 1–15. [Google Scholar] [CrossRef] [PubMed]
- ECDC. Public health guidance on HIV, hepatitis B and C testing in the EU/EEA: An integrated approach [Internet]. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/hiv-hep-testing-guidance_0.pdf (accessed on 10 November 2022).
- Istituto Superiore di Sanità. Aggiornamento Delle Nuove Diagnosi di Infezione da HIV e Dei Casi di AIDS in Italia al 31 Dicembre 2018. 2019. Available online: https://www.iss.it/documents/20126/45616/AGGIORNAMENTO_HIV_2018.pdf/14e3206f-bd4d-0054-4568-4508556f61d2?t=1581096394022 (accessed on 10 November 2022).
- García García, A.; Martínez Sanz, J.; Vivancos Gallego, M.; Cano, C.; Romero, B.; Sánchez Conde, M.; Vélez Díaz-Pallarés, M.; González Vázquez, M.; Gea Rodríguez, F.; Galán Montemayor, J.; et al. HIV Testing Taining for Non-HIV-Specialists in a Tertiary Hospital: Changes in Attitudes and Rates of HIV Screening. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9585422/ (accessed on 13 November 2022).
- Desai, S.; Tavoschi, L.; Sullivan, A.K.; Combs, L.; Raben, D.; Delpech, V. HIV testing strategies employed in health care settings in the European Union/European Economic Area (EU/EEA): Evidence from a systematic review. HIV Med. 2020, 21, 163–179. Available online: https://pubmed.ncbi.nlm.nih.gov/31729150/ (accessed on 10 November 2022). [CrossRef] [PubMed]
- Madeddu, G.; de Vito, A.; Cozzi-Lepri, A.; Cingolani, A.; Maggiolo, F.; Perno, C.F.; Robertaf, G.; Giuliag, M.; Annalisah, S.; Antonella d’Arminio, M.; et al. Time spent with HIV-RNA ≤ 200 copies/mL in a cohort of people with HIV during the U=U era. AIDS 2021, 35, 1103–1112. Available online: https://journals.lww.com/aidsonline/Fulltext/2021/06010/Time_spent_with_HIV_RNA___200_copies_ml_in_a.11.aspx (accessed on 10 November 2022). [CrossRef]
- Sullivan, A.K.; Raben, D.; Reekie, J.; Rayment, M.; Mocroft, A.; Esser, S.; Leon, A.; Begovac, J.; Brinkman, K.; Zangerle, R.; et al. Feasibility and effectiveness of indicator condition-guided testing for HIV: Results from HIDES I (HIV indicator diseases across Europe study). PLoS ONE 2013, 8, e52845. Available online: https://pubmed.ncbi.nlm.nih.gov/23341910/ (accessed on 10 November 2022). [CrossRef] [PubMed]
- Raben, D.D.; Mocroft, A.; Rayment, M.M.; Mitsura, V.; Hadziosmanovic, V.; Sthoeger, Z.M.; Palfreeman, A.A.; Morris, S.S.; Kutsyna, G.G.; Vassilenko, A.A.; et al. Auditing HIV Testing Rates across Europe: Results from the HIDES 2 Study. PLoS ONE 2015, 10, e0140845. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0140845 (accessed on 10 November 2022). [CrossRef] [PubMed]
- Bogers, S.J.; van der Loeff, M.F.S.; Boyd, A.; Davidovich, U.; van der Valk, M.; Brinkman, K.; Sigaloff, K.; Branger, J.; Bokhizzou, N.; de Bree, G.J.; et al. Improving indicator-condition guided testing for HIV in the hospital setting (PROTEST 2·0): A multicenter, interrupted time-series analysis. Lancet Reg. Health Eur. 2022, 23, 100515. Available online: http://www.thelancet.com/article/S2666776222002113/fulltext (accessed on 13 November 2022). [CrossRef]
- Cayuelas Redondo, L.; Ruíz, M.; Kostov, B.; Sequeira, E.; Noguera, P.; Herrero, M.A.; Menacho, I.; Barba, O.; Clusa, T.; Rifa, B.; et al. Indicator condition-guided HIV testing with an electronic prompt in primary healthcare: A before and after evaluation of an intervention. Sex Transm. Infect. 2019, 95, 238–243. Available online: https://pubmed.ncbi.nlm.nih.gov/30679391/ (accessed on 10 November 2022). [CrossRef] [PubMed]
- Tincati, C.; Barbanotti, D.; Bini, T.; Tavelli, A.; Ravizza, M.; Marconi, A.; Cattaneo, M.; Chiumello, D.A.; Cerri, A.; Priori, A.; et al. High HIV prevalence following screening of subjects withHIV indicator conditions in a hospital setting. HIV Med. 2019, 20, 252–253. [Google Scholar]
- European AIDS Clinical Society. EACS Guidelines 11.0. 2021. Available online: https://www.eacsociety.org/media/guidelines-11.1_final_09-10.pdf (accessed on 10 November 2022).
- SIMIT, Salute M della. Linee Guida Italiane sull’utilizzo della Terapia Antiretrovirale e la gestione diagnostico-clinica delle persone con infezione da HIV-1. 2017. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2696_allegato.pdf (accessed on 10 November 2022).
- Fabbiani, M.; Gagliardini, R.; Ciccarelli, N.; Roldan, E.Q.; Latini, A.; D’Ettorre, G.; Antinori, A.; Castagna, A.; Orofino, G.; Francisci, D.; et al. Atazanavir/ritonavir with lamivudine as maintenance therapy in virologically suppressed HIV-infected patients: 96 week outcomes of a randomized trial. J. Antimicrob. Chemother. 2018, 73, 1955–1964. Available online: https://pubmed.ncbi.nlm.nih.gov/29668978/ (accessed on 10 November 2022). [CrossRef] [PubMed] [Green Version]
- De Vito, A.; Caruana, G.; Clark, F.; Nunnari, G.; Pellicanò, G.; Angioni, G.; Freedman, A.; Babudieri, S.; Madeddu, G. Efficacy, safety and tolerability of dolutegravir-based combination antiretroviral therapy in clinical practice in HIV-infected patients: Results from a multicenter study—Infectious Diseases & Tropical Medicine. Infect. Dis. Trop. Med. 2019, 5, e565. Available online: https://www.infectiousjournal.com/article/565 (accessed on 10 November 2022).
- Rossetti, B.; Baldin, G.; Sterrantino, G.; Rusconi, S.; De Vito, A.; Giacometti, A.; Gagliardini, R.; Colafigli, M.; Capetti, A.; D’Ettorre, G.; et al. Efficacy and safety of dolutegravir-based regimens in advanced HIV-infected naïve patients: Results from a multicenter cohort study. Antivir. Res. 2019, 169, 104552. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient | Sex | Age | Risk Factor | Reason for Testing | Opportunistic Infections | Stage | Basal HIV-RNA (Copies/mL) | CD4 Cells/mm3 | CD4 % | CD4/CD8 | First-Line Therapy | Date of Negativization | LTFU |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Female | 29 | HE | Fever | None | B3 | 2,000,000 | 54.00 | 5.62 | 0.12 | TDF/FTC + ATV/r | 10 February 2018 | Yes |
| 2 | Female | 41 | HE | Pharyngotonsillitis; Rash | None | A1 | 9420 | 1357.00 | 52.15 | 1.63 | TDF/TAF + DTG | 27 September 2019 | No |
| 3 | Male | 43 | MSM | Bilateral pneumonia | PjP | C3 | 6480 | 56.00 | 3.14 | 0.04 | TDF/FTC + DTG | 8 November 2017 | No |
| 4 | Female | 42 | HE | Bilateral pneumonia | PjP | C3 | 1,940,000 | 80.00 | 5.2 | 0.19 | TDF/FTC + DTG | Died | No |
| 5 | Male | 40 | MSM | Bilateral pneumonia | PjP | A2 | 150,000 | 308.00 | 23.00 | 0.42 | TDF/FTC + DTG | 25 July 2017 | No |
| 6 | Male | 40 | IDU | Bilateral pneumonia | PjP | C3 | 739,000 | 14.00 | 0.48 | 0.01 | TDF/FTC + DTG | 17 July 2017 | No |
| 7 | Female | 57 | HE | Pleural Empyema | None | B2 | 139,000 | 317.00 | 10.72 | 0.14 | TAF/FTC + RAL | 21 March 2019 | No |
| 8 | Male | 72 | HE | Fever; Asthenia | HZV | C3 | 462,000 | 162.00 | 17.97 | 0.62 | TDF/FTC + RAL | 16 March 2018 | No |
| 9 | Male | 66 | HE | Fever; Asthenia | None | B1 | 765,000 | 924.00 | 9.77 | 1.39 | TDF/FTC + DRV/r | 12 September 2017 | Yes |
| 10 | Male | 28 | MSM | Bilateral pneumonia | PCP; Invasive Pneumococcal Disease; CMV; Esophageal Candidiasis; Perianal HSV | C3 | 150,000 | 29.00 | 3.89 | 0.07 | TDF/FTC + DTG | 1 June 2017 | No |
| 11 | Male | 73 | MSM | Stomatitis | None | B2 | 73,100 | 246.00 | 20.00 | 0.38 | TDF/TAF + RAL | 2 October 2019 | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Vito, A.; Colpani, A.; Mameli, M.S.; Bagella, P.; Fiore, V.; Fozza, C.; Montesu, M.A.; Fois, A.G.; Filigheddu, F.; Manzoni, N.; et al. HIV Infection Indicator Disease-Based Active Case Finding in a University Hospital: Results from the SHOT Project. Infect. Dis. Rep. 2023, 15, 94-101. https://doi.org/10.3390/idr15010010
De Vito A, Colpani A, Mameli MS, Bagella P, Fiore V, Fozza C, Montesu MA, Fois AG, Filigheddu F, Manzoni N, et al. HIV Infection Indicator Disease-Based Active Case Finding in a University Hospital: Results from the SHOT Project. Infectious Disease Reports. 2023; 15(1):94-101. https://doi.org/10.3390/idr15010010
Chicago/Turabian StyleDe Vito, Andrea, Agnese Colpani, Maria Sabrina Mameli, Paola Bagella, Vito Fiore, Claudio Fozza, Maria Antonia Montesu, Alessandro Giuseppe Fois, Fabiana Filigheddu, Noemi Manzoni, and et al. 2023. "HIV Infection Indicator Disease-Based Active Case Finding in a University Hospital: Results from the SHOT Project" Infectious Disease Reports 15, no. 1: 94-101. https://doi.org/10.3390/idr15010010