
Universal Health Coverage for Antiretroviral Treatment: A Review
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Theoretical Framework
- Coverage: who is covered? This concerned crude coverage in the current review;
- Financial protection: the proportion of the costs covered, and service costs covered by insurance or other methods. The effectiveness of financial protection is measured by catastrophic health expenditure and impoverishment;
- Equity in ART coverage: all people in need of service should be covered; the non-covered population is evidence of service disparity;
- Quality in ART care: in UHC, effective service coverage denotes the quality of services delivered to the people covered by services. Quality of care was assessed by any of methods in this review. Quality of care and equity are integrated definitions of UHC.
2.2. Identifying a Research Question
2.3. Searching, Selection, Charting and Presenting
3. Results
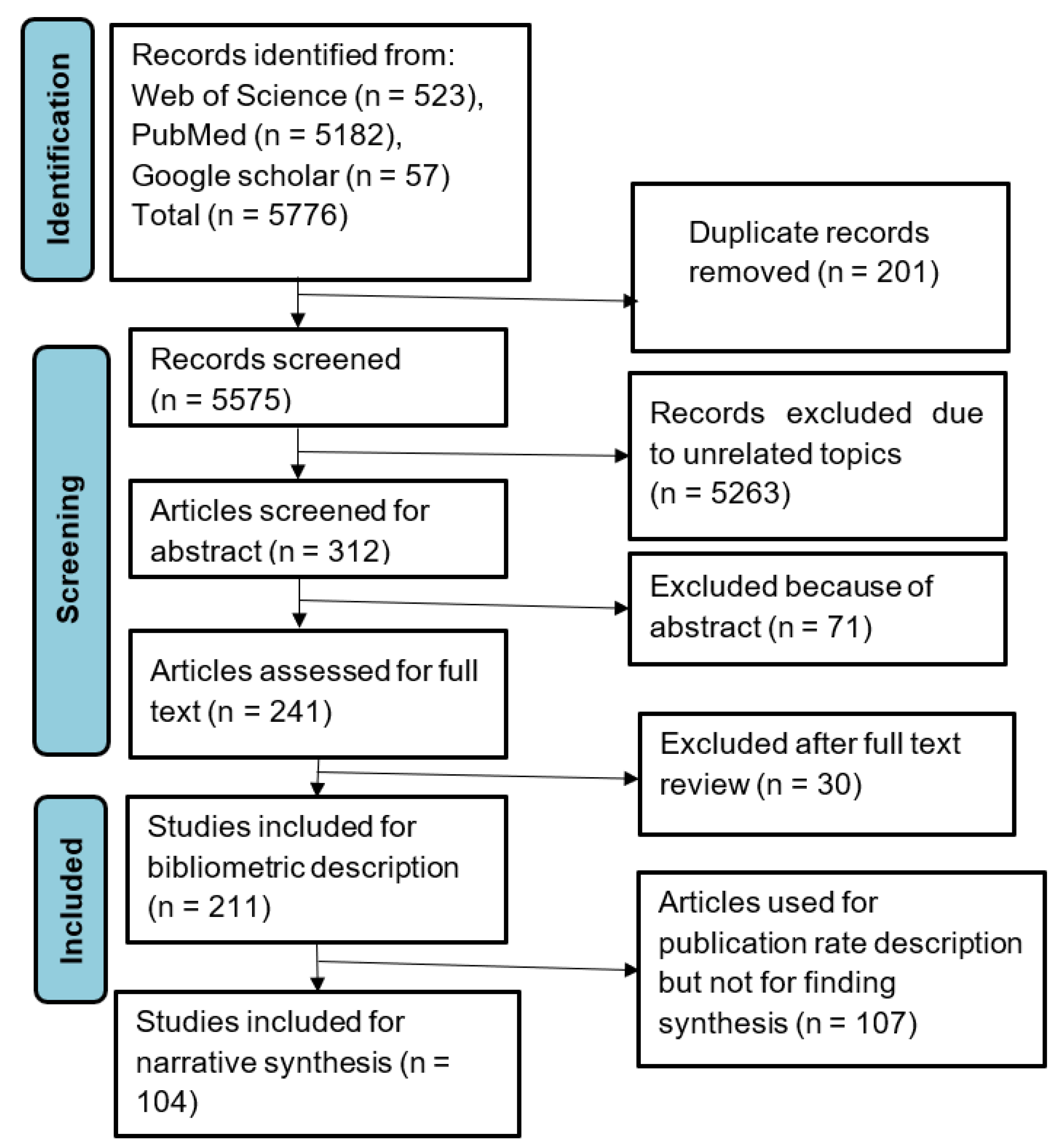
3.1. Search Results
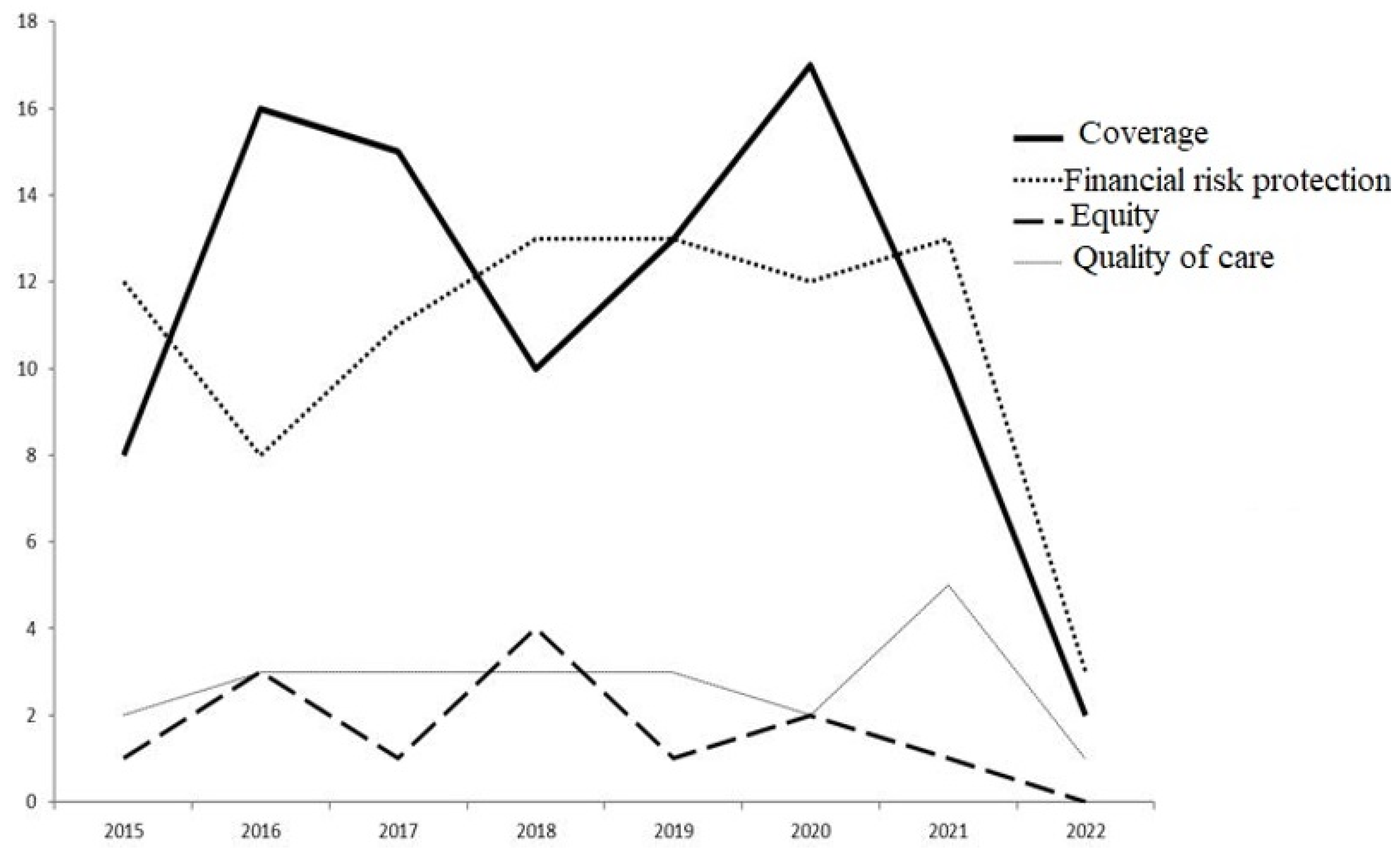
3.2. Main Findings
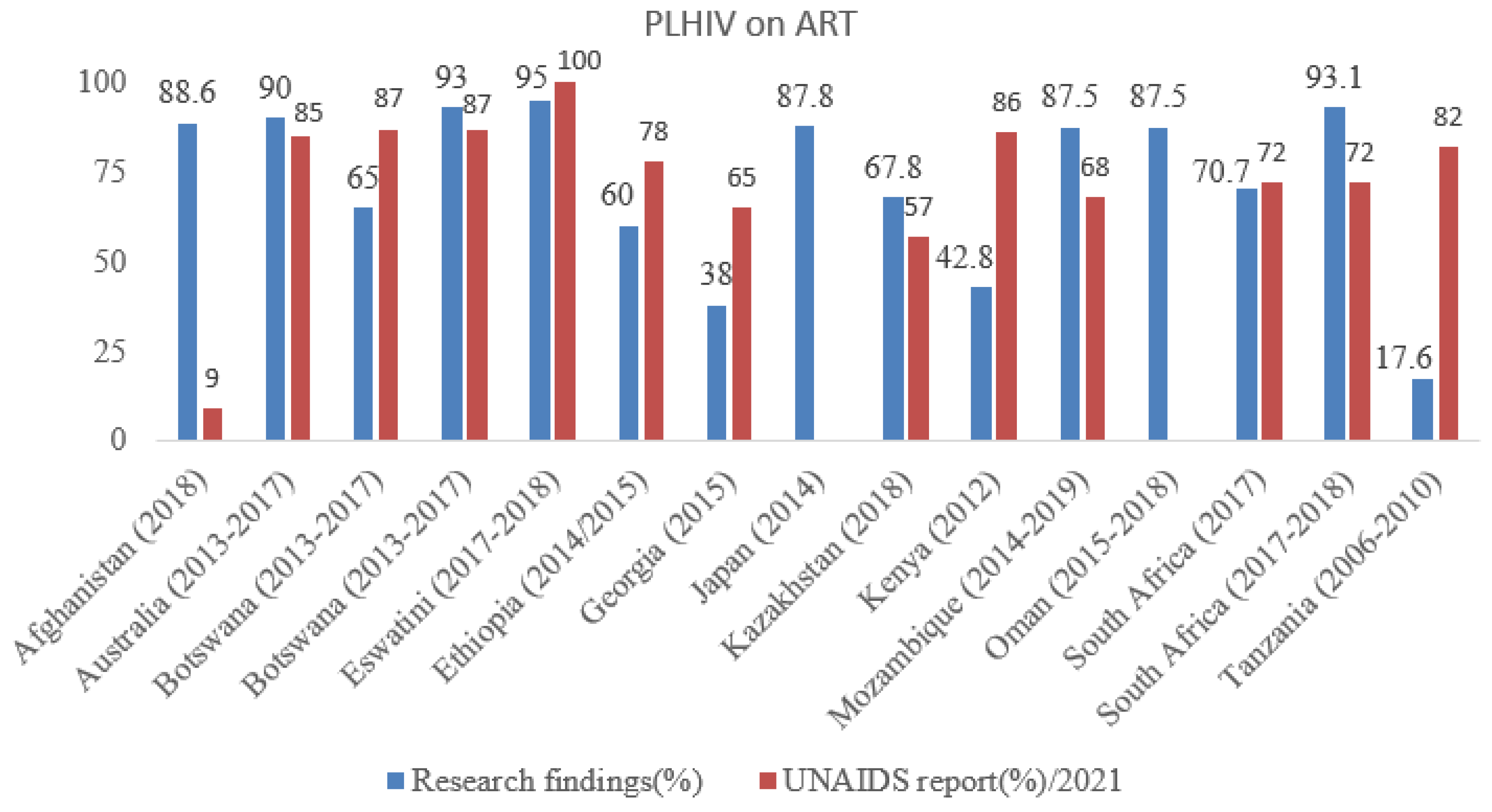
3.3. ART Coverage among PLHIV
3.4. ART Coverage among Key Population
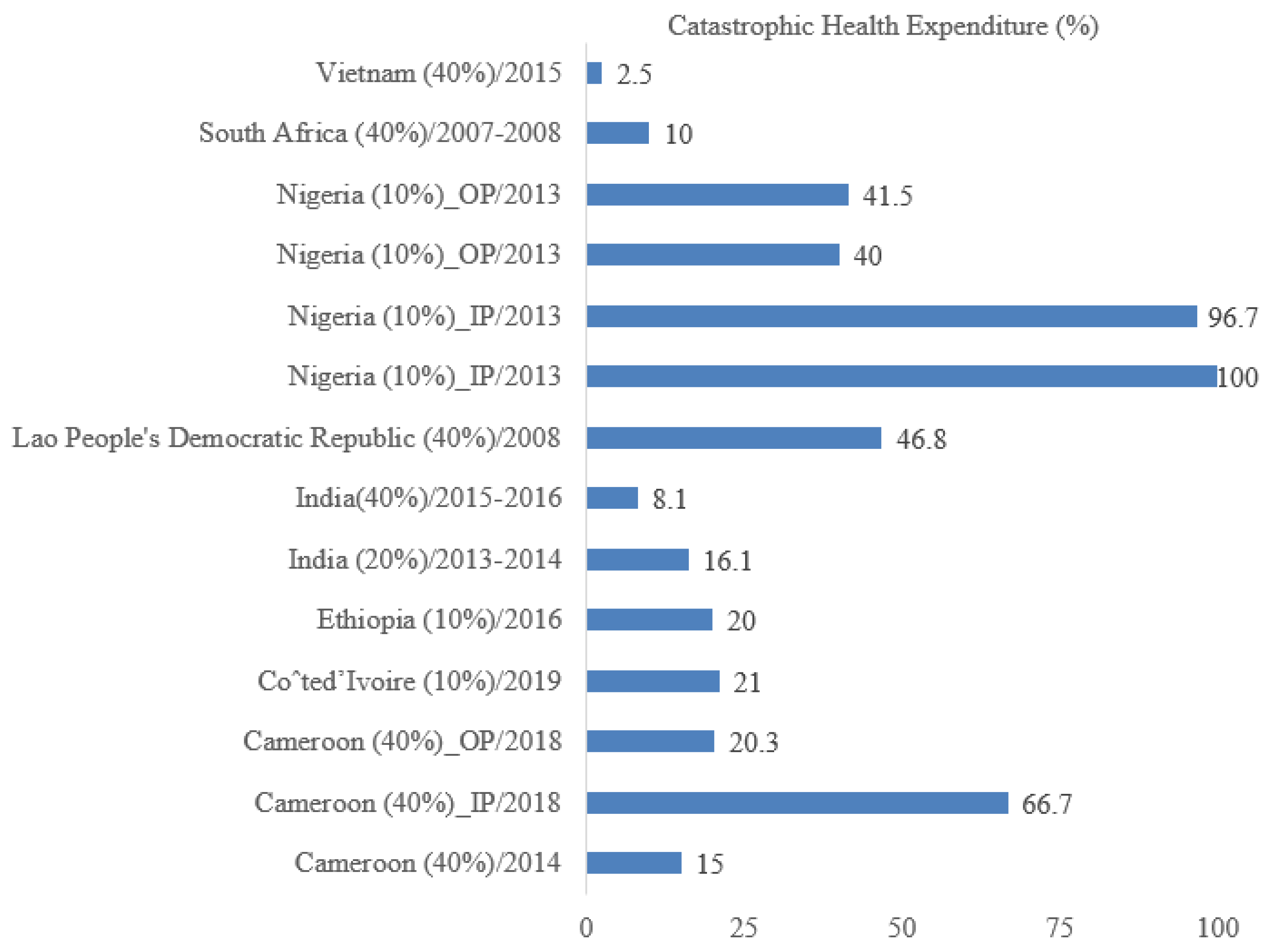
3.5. Catastrophic Health Expenditure
3.6. Strategies for ART Coverage and Quality of Care
3.7. Barriers for ART Coverage, Catastrophic Health Expenditure, and Quality of Care
3.8. Client (Sociodemographic- and Clinical-Related) Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Treating 3 Million by 2005: Making It Happen: The WHO Strategy: The WHO and UNAIDS Global Initiative to Provide Antiretroviral Therapy to 3 Million People with HIV/AIDS in Developing Countries by the End of 2005; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- UNAIDS. Global HIV & AIDS Statistics—Fact Sheet. 2021. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 12 June 2022).
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- United Nations. United Nations Sustainable Development Summit 2015. 2015. Available online: https://sustainabledevelopment.un.org/post2015/summit (accessed on 21 August 2022).
- World Health Organization. Universal Health Coverage: Moving towards Better Health: Action Framework for the Western Pacific Region. 2016. Available online: https://www.who.int/publications/i/item/9789290617563 (accessed on 3 May 2022).
- Ng, M.; Fullman, N.; Dieleman, J.L.; Flaxman, A.D.; Murray, C.J.; Lim, S.S. Effective coverage: A metric for monitoring universal health coverage. PLoS Med. 2014, 11, e1001730. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; The World Bank Group. Tracking Universal Health Coverage: 2017 Global Monitoring Report; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Universal Health Coverage (UHC) 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc) (accessed on 1 April 2022).
- World Health Organization. Standards for Quality HIV Care: A Tool for Quality Assessment, Improvement, and Accreditation; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- World Health Organization. Regional Office for The Eastern Mediterranean. Antiretroviral Therapy (ART) Coverage. 2019. Available online: https://rho.emro.who.int/Metadata/antiretroviral-therapy-art-coverage (accessed on 26 January 2022).
- World Health Organization. Maintaining and Improving Quality of Care within HIV Clinical Services; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Pushing for High-Quality HIV Services in Low- and Middle-Income Countries. 2019. Available online: https://www.who.int/news/item/04–10–2019-pushing-for-high-quality-hiv-services-in-low--and-middle-income-countries (accessed on 7 June 2022).
- World Health Organization; World Bank Group. Monitoring Progress towards Universal Health Coverage at Country and Global Levels: Framework, Measures and Targets; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- UNAIDS. World Health Organization. Guidance on Ethics and Equitable Access to HIV Treatment and Care; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Joint United Nations Programme on HIV/AIDS. End Inequalities. End Aids. Global Aids Strategy 2021–2026. Available online: https://www.aidsdatahub.org/resource/end-inequalities-end-aids-global-aids-strategy-2021-2026 (accessed on 5 September 2022).
- Daudt, H.M.; van Mossel, C.; Scott, S.J. Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med. Res. Methodol. 2013, 13, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maulsby, C.H.; Ratnayake, A.; Hesson, D.; Mugavero, M.J.; Latkin, C.A. A scoping review of employment and HIV. AIDS Behav. 2020, 24, 2942–2955. [Google Scholar] [CrossRef] [PubMed]
- Saffier, I.P.; Kawa, H.; Harling, G. A scoping review of prevalence, incidence and risk factors for HIV infection amongst young people in Brazil. BMC Infect. Dis. 2017, 17, 675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Health Systems Financing: The Path to Universal Coverage; The World Health Report; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; Mclnerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Implement. 2021, 19, 3–10. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- UNAIDS. UNAIDS Data 2021 Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS. Available online: https://www.unaids.org/sites/default/files/media_asset/JC3032_AIDS_Data_book_2021_En.pdf (accessed on 11 October 2022).
- King, E.J.; Denebayeva, A.; Tukeyev, M.; Zhandybaeva, A.; Nurkerimova, A.; Nugmanova, Z. Factors associated with being on antiretroviral treatment among people living with HIV in Almaty, Kazakhstan. AIDS Care 2021, 33, 398–402. [Google Scholar] [CrossRef]
- Wirth, K.E.; Gaolathe, T.; Holme, M.P.; Mmalane, M.; Kadima, E.; Chakalisa, U.; Manyake, K.; Mbikiwa, A.M.; Simon, S.V.; Letlhogile, R.; et al. Population uptake of HIV testing, treatment, viral suppression, and male circumcision in Botswana: A cluster-randomized trial. Lancet HIV 2020, 7, e422. [Google Scholar] [CrossRef]
- Barnabas, R.V.; van Rooyen, H.; Tumwesigye, E.; Brantley, J.; Baeten, J.M.; van Heerden, A.; Turyamureeba, B.; Joseph, P.; Krows, M.; Thomas, K.K.; et al. Uptake of antiretroviral therapy and male circumcision after community-based HIV testing and strategies for linkage to care versus standard clinic referral: A multisite, open-label, randomised controlled trial in South Africa and Uganda. Lancet HIV 2016, 3, e212–e220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floyd, S.; Shanaube, K.; Yang, B.; Schaap, A.; Griffith, S.; Phiri, M.; Macleod, D.; Sloot, R.; Sabapathy, K.; Bond, V.; et al. HIV testing and treatment coverage achieved after 4 years across 14 urban and peri-urban communities in Zambia and South Africa: An analysis of findings from the HPTN 071 (PopART) trial. PLoS Med. 2020, 17, e1003067. [Google Scholar] [CrossRef] [PubMed]
- Shanaube, K.; Macleod, D.; Chaila, M.J.; Mackworth-Young, C.; Hoddinott, G.; Schaap, A.; Floyd, S.; Bock, P.; Hayes, R.; Fidler, S.; et al. HIV care cascade among adolescents in a “Test and Treat” community-based intervention: HPTN 071 (PopART) for youth study. J. Adolesc. Health 2021, 68, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Indravudh, P.P.; Fielding, K. Effect of community-led delivery of HIV self-testing on HIV testing and antiretroviral therapy initiation in Malawi: A cluster-randomised trial. PLoS Med. 2021, 18, e1003608. [Google Scholar] [CrossRef] [PubMed]
- Cornelius, L.J.; Erekaha, S.C.; Okundaye, J.N.; Sam-Agudu, N.A. A Socio-Ecological Examination of Treatment Access, Uptake and Adherence Issues Encountered By HIV-Positive Women in Rural North-Central Nigeria. J. Evid.-Inf. Soc. Work 2018, 15, 38–51. [Google Scholar] [CrossRef]
- Zelaya, C.E.; le Minh, N.; Lau, B.; Latkin, C.A.; Viet Ha, T.; Minh Quan, V.; Mo, T.T.; Sripaipan, T.; Davis, W.W.; Celentano, D.D.; et al. The Effect of a Multi-Level Intervention on the Initiation of Antiretroviral Therapy (ART) among HIV-Infected Men Who Inject Drugs and Were Diagnosed Late in Thai Nguyen, Vietnam. PLoS ONE 2016, 11, e0161718. [Google Scholar] [CrossRef] [Green Version]
- Karver, T.S.; Barrington, C.; Donastorg, Y.; Perez, M.; Gomez, H.; Page, K.R.; Celentano, D.; Smith, K.C.; Kerrigan, D. Exploring peer navigation and support in the quality of HIV care experiences of female sex workers in the Dominican Republic. BMC Health Serv. Res. 2022, 22, 56. [Google Scholar] [CrossRef]
- Iwuji, C.C.; Orne-Gliemann, J.; Larmarange, J. Uptake of Home-Based HIV Testing, Linkage to Care, and Community Attitudes about ART in Rural KwaZulu-Natal, South Africa: Descriptive Results from the First Phase of the ANRS 12249 TasP Cluster-Randomised Trial. PLoS Med. 2016, 13, e1002107. [Google Scholar] [CrossRef] [Green Version]
- Hayes, R.; Floyd, S.; Schaap, A.; Shanaube, K.; Bock, P.; Sabapathy, K.; Griffith, S.; Donnell, D.; Piwowar-Manning, E.; EI-Sadr, W.; et al. A universal testing and treatment intervention to improve HIV control: One-year results from intervention communities in Zambia in the HPTN 071 (PopART) cluster-randomised trial. PLoS Med. 2017, 14, e1002292. [Google Scholar] [CrossRef]
- Nascimento, L.; Paula, C.C.; Magnago, T.S.; Padoin, S.M.; Harzheim, E.; Silva, C.B. Quality of Primary Health Care for children and adolescents living with HIV. Proceedings of the National Academy of Sciences of the United States of America. Rev. Lat. Am. Enfermagem. 2016, 24, e2720. [Google Scholar] [CrossRef] [PubMed]
- Odayar, J.; Malaba, T.R.; Allerton, J.; Lesosky, M.; Myer, L. Delivery of antiretroviral therapy to HIV-infected women during the postpartum period: The Postpartum Adherence Clubs for Antiretroviral Therapy (PACART) trial. PLoS ONE 2019, 16, 100442. [Google Scholar] [CrossRef] [PubMed]
- Exavery, A. ART use and associated factors among HIV positive caregivers of orphans and vulnerable children in Tanzania. PLoS Med. 2020, 20, 1251. [Google Scholar] [CrossRef]
- Adeyinka, D.; Evans, M.; Ozigbu, C.; van Woerden, H.; Adeyinka, E.; Oladimeji, O.; Aimakhu, C.; Odoh, D.; Chamla, D. Understanding the influence of socioeconomic ernvironment on paediatric anti-retroviral treatment coverage: Towards closing treatment gaps in sub-Saharan Africa. Cent. Eur. J. Public Health 2017, 25, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeshiwas, Y.; Debie, A.; Worku, N.; Yazachew, L. Improving quality of service among antiretroviral therapy users through strategic problem-solving approach at bure primary hospital, northwest Ethiopia. Patient Prefer. Adherence 2021, 15, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- Visser, C.A.; Wolvaardt, J.E.; Cameron, D.; Marincowitz, G.J.O. Clinical mentoring to improve quality of care provided at three NIM-ART facilities: A mixed methods study. Afr. J. Prim. Health Care Fam. Med. 2018, 10, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Stecher, C. Physician network connections to specialists and HIV quality of care. Health Serv. Res. 2021, 56, 908–918. [Google Scholar] [CrossRef]
- Pilgrim, N.; Musheke, M.; Raymond, H.F.; Keating, R.; Mwale, J.; Banda, L.; Mulenga, D.; Phiri, L.; Geibel, S.; Tun, W. Quality of care and HIV service utilization among key populations in Zambia: A qualitative comparative analysis among female sex workers, men who have sex with men and people who use drugs. Aids Care-Psychol. Socio-Med. Asp. Aids/Hiv 2019, 31, 460–464. [Google Scholar] [CrossRef]
- Plazy, M.; Perriat, D.; Gumede, D.; Boyer, S.; Pillay, D.; Dabis, F.; Seeley, J.; Orne-Gliemann, J. Implementing universal HIV treatment in a high HIV prevalence and rural South African setting—Field experiences and recommendations of health care providers. PLoS ONE 2017, 12, e0186883. [Google Scholar] [CrossRef] [Green Version]
- Lazuardi, E.; Newman, C.E.; Anintya, I.; Rowe, E.; Wirawan, D.N.; Wisaksana, R.; Subronto, Y.W.; Kusmayanti, N.A.; Iskandar, S.; Kaldor, J. et al. Increasing HIV treatment access, uptake and use among men who have sex with men in urban Indonesia: Evidence from a qualitative study in three cities. Health Policy Plan. 2020, 35, 16–25. [Google Scholar]
- Li, C.Y.; Barrington, C.; Jiang, H.; Lei, G.; Golin, C.E.; Fisher, E.B.; Muessig, K.E. Challenges for accessing and maintaining good quality of HIV care among men who have sex with men living with HIV in China: A qualitative study with key stakeholders. Aids Care-Psychol. Socio-Med. Asp. Aids/Hiv 2020, 32, S119–S126. [Google Scholar] [CrossRef] [PubMed]
- Haacker, M.; Birungi, C. Poverty as a barrier to antiretroviral therapy access for people living with HIV/AIDS in Kenya. Afr. J. AIDS Res. 2018, 17, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Cholong, B.J.; Mayin, K.B.; Aloysius, N.M. The Determinants of Catastrophic Health Expenditure and Coping Strategies for Households with People Living With HIV/AIDS in the Nkambe District Hospital, Cameroon. Eur. J. Health Sci. 2022, 7, 36–48. [Google Scholar] [CrossRef]
- Bousmah, M.A.; Nishimwe, M.L. Free access to antiretroviral treatment and protection against the risk of catastrophic health expenditure in people living with HIV: Evidence from Cameroon. BMC Health Serv. Res. 2021, 21, 313. [Google Scholar] [CrossRef]
- McClarty, L.M.; Blanchard, J.F.; Becker, M.L. Leaving no one behind? An equity analysis of the HIV care cascade among a cohort of people living with HIV in Manitoba, Canada. BMC Public Health 2021, 21, 281. [Google Scholar] [CrossRef]
- Rawat, A.; Uebel, K.; Moore, D.; Cingl, L.; Yassi, A. Patient Responses on Quality of Care and Satisfaction with Staff After Integrated HIV Care in South African Primary Health Care Clinics. J. Assoc. Nurses AIDS Care 2018, 29, 698–711. [Google Scholar] [CrossRef]
- Teeraananchai, S.; Kerr, S.J.; Khananuraksa, P.; Ruxrungtham, K.; Puthanakit, T. Rapid antiretroviral initiation among Thai youth living with HIV in the National AIDS programme in the era of treatment at any CD4 cell count: A national registry database study. J. Int. AIDS Soc. 2020, 23 (Suppl. S5), e25574. [Google Scholar] [CrossRef]
- Auld, A.F.; Shiraishi, R.W.; Mbofana, F.; Couto, A.; Fetogang, E.B.; El-Halabi, S.; Lebelonyane, R.; Pilatwe, P.T.; Humunime, N.; Okello, V.; et al. Lower levels of antiretroviral therapy enrollment among men with HIV compared with women—12 countries, 2002–2013. Morb. Mortal. Wkly. Rep. 2015, 64, 1281–1286. [Google Scholar] [CrossRef] [Green Version]
- Hoots, B.E.; Finlayson, T.J.; Wejnert, C.; Paz-Bailey, G.; Group, N.S. Early linkage to HIV care and antiretroviral treatment among men who have sex with men—20 cities, United States, 2008 and 2011. PLoS ONE 2015, 10, e0132962. [Google Scholar] [CrossRef] [Green Version]
- Landovitz, R.J.; Desmond, K.A.; Leibowitz, A.A. Antiretroviral Therapy: Racial Disparities among Publicly Insured Californians with HIV. J. Health Care Poor Underserved 2017, 28, 406–429. [Google Scholar] [CrossRef]
- Beer, L.; Bradley, H.; Mattson, C.L.; Johnson, C.H.; Hoots, B.; Shouse, R.L. Trends in racial and ethnic disparities in antiretroviral therapy prescription and viral suppression in the United States, 2009–2013. J. Acquir. Immune Defic. Syndr (1999) 2016, 73, 446. [Google Scholar] [CrossRef] [PubMed]
- Moyo, S.; Young, P.W.; Gouws, E.; Naidoo, I.; Wamicwe, J.; Mukui, I.; Marsh, K.; Igumbor, E.U.; Kim, A.A.; Rehle, T. Equity of antiretroviral treatment use in high HIV burden countries: Analyses of data from nationally-representative surveys in Kenya and South Africa. PLoS ONE 2018, 13, e0201899. [Google Scholar] [CrossRef]
- Onwujekwe, O.E.; Ibe, O.; Torpey, K.; Dada, S.; Uzochukwu, B.; Sanwo, O. Examining geographic and socio-economic differences in outpatient and inpatient consumer expenditures for treating HIV/AIDS in Nigeria. J. Int. AIDS Soc. 2016, 19, 20588. [Google Scholar] [CrossRef]
- Etiaba, E.; Onwujekwe, O.; Torpey, K.; Uzochukwu, B.; Chiegil, R. What Is the Economic Burden of Subsidized HIV/AIDS Treatment Services on Patients in Nigeria and Is This Burden Catastrophic to Households? PLoS ONE 2016, 11, e0167117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negin, J.; Randell, M.; Raban, M.Z.; Nyirenda, M.; Kalula, S.; Madurai, L.; Kowal, P. Health expenditure and catastrophic spending among older adults living with HIV. Glob. Public Health 2017, 12, 1282–1296. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, L.J.; Hull, M.W.; Samji, H.; Lima, V.D.; Yip, B.; Zhang, W.; Lourenço, L.; Colley, G.; Hogg, R.S.; Montaner, J.S.G. Is there a rural/urban gap in the quality of HIV care for treatment-naive HIV-positive individuals initiating antiretroviral therapy in British Columbia? Aids Care-Psychol. Socio-Med. Asp. Aids/Hiv 2017, 29, 1218–1226. [Google Scholar] [CrossRef]
- Shukla, M.; Agarwal, M.; Singh, J.; Tripathi, A.; Srivastava, A.; Singh, V.K. Catastrophic health expenditure amongst people living with HIV/AIDS availing antiretroviral treatment services at two tertiary care health facilities in district of northern India. Indian J. Community Med. Off. Publ. Indian Assoc. Prev. Soc. Med. 2015, 6, 323–328. [Google Scholar]
- Alvi, Y.; Faizi, N.; Khalique, N.; Ahmad, A. Assessment of out-of-pocket and catastrophic expenses incurred by patients with Human Immunodeficiency Virus (HIV) in availing free antiretroviral therapy services in India. Public Health 2020, 183, 16–22. [Google Scholar] [CrossRef]
- Barennes, H.; Frichittavong, A.; Gripenberg, M.; Koffi, P. Evidence of High Out of Pocket Spending for HIV Care Leading to Catastrophic Expenditure for Affected Patients in Lao People’s Democratic Republic. PLoS ONE 2015, 10, e0136664. [Google Scholar] [CrossRef]
- Furuoka, F.; Hoque, M.Z. Determinants of antiretroviral therapy coverage in Sub-Saharan Africa. J. Int. AIDS Soc. 2015, 3, e1496. [Google Scholar] [CrossRef] [Green Version]
- Mnyaka, O.R.; Mabunda, S.A. Barriers to the Implementation of the HIV Universal Test and Treat Strategy in Selected Primary Care Facilities in South Africa’s Eastern Cape Province. J. Prim. Care Community Health 2021, 12, 21501327211028706. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.; MacKellar, D. HIV testing and ART initiation among partners, family members, and high-risk associates of index clients participating in the CommLink linkage case management program, Eswatini, 2016–2018. PLoS ONE 2021, 16, e0261605. [Google Scholar] [CrossRef] [PubMed]
- Bachanas, P.; Alwano, M.G.; Lebelonyane, R.; Block, L.; Behel, S.; Raizes, E.; Ussery, G.; Wang, H.; Ussery, F.; Holme, M.P.; et al. Finding, treating and retaining persons with HIV in a high HIV prevalence and high treatment coverage country: Results from the Botswana Combination Prevention Project. PLoS ONE 2021, 16, e0250211. [Google Scholar] [CrossRef] [PubMed]
- Marukutira, T.; Gray, R.T.; Douglass, C.; El-Hayek, C.; Moreira, C.; Asselin, J.; Donovan, B.; Vickers, T.; Spelman, T.; Crowe, S.; et al. Gaps in the HIV diagnosis and care cascade for migrants in Australia, 2013–2017: A cross-sectional study. PLoS Med. 2020, 17, e1003044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soumah, A.; Avettand-Fenoel, V.; Veber, F.; Moshous, D.; Mahlaoui, N.; Blanche, S.; Frange, P. High rates of antiretroviral coverage and virological suppression in HIV-1-infected children and adolescents. BMJ Open 2020, 50, 269–273. [Google Scholar] [CrossRef]
- KPMG. Ending the Epidemic: An Assessment of HIV Policy in France and Recommendation to Improve the Lives of Those Living with, and at Risk of HIV; KPMG: Amstelveen, The Netherlands, 2019. [Google Scholar]
- Elgalib, A.; Shah, S.; Al-Habsi, Z.; Al-Fouri, M.; Lau, R.; Al-Kindi, H.; Al-Rawahi, B.; Al-Abri, S. The cascade of HIV care in Oman, 2015–2018: A population-based study from the Middle East. Int. J. Infect. Dis. 2020, 90, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Harooni, M.Z.; Atarud, A.A.; Ehsan, E.; Alokozai, A.; McFarland, W.; Mirzazadeh, A. Gaps in the continuum of care among people living with HIV in Afghanistan. Int. J. STD AIDS 2021, 33, 282–288. [Google Scholar] [CrossRef]
- Miyazaki, N.; Sugiura, W.; Gatanaga, H.; Watanabe, D.; Yamamoto, Y.; Yokomaku, Y.; Yoshimura, K.; Matsushita, S.; the Japanese HIV-MDR Study Group. The Prevalence of High Antiretroviral Coverage and Viral Suppression in Japan: An Excellent Profile for a Downstream Human Immunodeficiency Virus Care Spectrum. Jpn. J. Infect. Dis. 2017, 70, 158–160. [Google Scholar] [CrossRef] [Green Version]
- Pathmanathan, I.; Nelson, R.; de Louvado, A.; Thompson, R.; Pals, S.; Casavant, I.; Cardoso, M.J.A.; Ujamaa, D.; Bonzela, J.; Mikusova, S.; et al. High Coverage of Antiretroviral Treatment with Annual Home-Based HIV Testing, Follow-up Linkage Services, and Implementation of Test and Start: Findings From the Chokwe Health Demographic Surveillance System, Mozambique, 2014–2019. Jaids-J. Acquir. Immune Defic. Syndr. 2021, 86, E97–E105. [Google Scholar] [CrossRef]
- Wu, C.; Zhang, B.; Dai, Z.; Zheng, Q.; Duan, Z.; He, Q.; Zhu, C. Impact of immediate initiation of antiretroviral therapy among men who have sex with men infected with HIV in Chengdu, southwest China: Trends analysis, 2008–2018. BMC Public Health 2021, 21, 689. [Google Scholar] [CrossRef]
- Chkhartishvili, N.; Chokoshvili, O.; Dvali, N.; Abutidze, A.; Sharvadze, L.; Tsertsvadze, T. Significant Improvements Are Needed in HIV Care Continuum to Meet 90–90–90 Targets in Georgia. J. Int. Assoc. Provid. AIDS Care 2016, 15, 451–454. [Google Scholar] [CrossRef] [PubMed]
- Levira, F.; Agnarson, A.M.; Masanja, H.; Zaba, B.; Ekström, A.M.; Thorson, A. Antiretroviral treatment coverage in a rural district in Tanzania—A modeling study using empirical data. BMC Public Health 2015, 15, 195. [Google Scholar] [CrossRef] [PubMed]
- Mathews, C.; Cheyip, M.; Beauclair, R.; Puren, A.; Lombard, C.; Jonas, K.; Ayalew, K.A.; Govindasamy, D.; Kuo, C.; Dietrich., J.J.; et al. HIV care coverage among HIV-positive adolescent girls and young women in South Africa: Results from the HERStory Study. S. Afr. Med. J. 2021, 111, 460–468. [Google Scholar] [CrossRef]
- Ruegsegger, L.M.; Stockton, M.; Go, V.F.; Piscalko, H.; Davis, D.; Hoffman, I.F.; Hosseinipour, M.C.; Zalira, E.; Lungu, T.; Bula, A.; et al. Stigma, Social Support, and Sexual Behavior among Female Sex Workers at risk for HIV in Malawi. AIDS Educ. Prev. Off. Publ. Int. Soc. AIDS Educ. 2021, 33, 290. [Google Scholar] [CrossRef] [PubMed]
- Ferraz, D.; Couto, M.T.; Zucchi, E.M.; Calazans, G.J.; dos Santos, L.A.; Mathias, A.; Grangeiro, A. AIDS-and sexuality-related stigmas underlying the use of post-exposure prophylaxis for HIV in Brazil: Findings from a multicentric study. Sex. Reprod. Health Matters 2019, 27, 107–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdella, S.; Demissie, M.; Worku, A.; Dheresa, M.; Berhane, Y. HIV prevalence and associated factors among female sex workers in Ethiopia, east Africa: A cross-sectional study using a respondent-driven sampling technique. EClinicalMedicine 2022, 51, 101540. [Google Scholar] [CrossRef]
- Sharma, M.; Smith, J.A.; Farquhar, C.; Ying, R.; Cherutich, P.; Golden, M.; Wamuti, B.; Bukusi, D.; Spiegel, H.; Barnabas, R.V. Assisted partner notification services are cost-effective for decreasing HIV burden in western Kenya. Aids 2018, 32, 233–241. [Google Scholar] [CrossRef]
- Iryawan, A.R.; Stoicescu, C.; Sjahrial, F.; Nio, K.; Dominich, A. The impact of peer support on testing, linkage to and engagement in HIV care for people who inject drugs in Indonesia: Qualitative perspectives from a community-led study. Harm Reduct. J. 2022, 19, 16. [Google Scholar] [CrossRef] [PubMed]
- Corina, M. Four takeaways from the AIDS 2022 Conference: Clinton Health Access Initiative. 2022. Available online: https://www.clintonhealthaccess.org/blog/4-takeaways-from-aids-2022/ (accessed on 19 September 2022).
- Stelmach, R.D.; Rabkin, M.; Abo, K.; Ahoba, I.; Gildas Anago, M.; Boccanera, R.; Brou, H.; Flueckiger, R.; Hartsough, K.; Msukwa, M.; et al. Financial burdens of HIV and chronic disease on people living with HIV in Côte d’Ivoire: A cross-sectional out-of-pocket expenditure study. PLoS ONE 2021, 16, e0255074. [Google Scholar] [CrossRef]
- Assebe, L.F.; Negussie, E.K.; Jbaily, A.; Tolla, M.T.T.; Johansson, K.A. Financial burden of HIV and TB among patients in Ethiopia: A cross-sectional survey. BMJ Open 2020, 10, e036892. [Google Scholar] [CrossRef]
- Julien, A.; Anthierens, S.; van Rie, A.; West, R.; Maritze, M.; Twine, R.; Kahn, K.; Lippman, S.S.; Pettifor, A.; Leslie, H.H. Health Care Providers’ Challenges to High-Quality HIV Care and Antiretroviral Treatment Retention in Rural South Africa. Qual. Health Res. 2021, 31, 722–735. [Google Scholar] [CrossRef] [PubMed]
- Aves, T.; Kredo, T.; Welch, V.; Mursleen, S.; Ross, S.; Zani, B.; Motaze, N.V.; Quinlan, L.; Mbugbaw, L. Equity issues were not fully addressed in Cochrane human immunodeficiency virus systematic reviews. J. Clin. Epidemiol. 2017, 81, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Dover, D.C.; Belon, A.P. The health equity measurement framework: A comprehensive model to measure social inequities in health. Int. J. Equity Health 2019, 18, 36. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strategies | Coverage | Quality of Care |
|---|---|---|
| Diagnosed after the country’s change in treatment approach [25] | ✓ | |
| Community-based HIV prevention and treatment interventions (test and treat) [26,27,28,29,30] | ✓ | |
| Peer (group) and community support [31,32,33] | ✓ | ✓ |
| Home-based care, including door-to-door communication [32,34,35] | ✓ | |
| Family health strategy [36] | ✓ | |
| Being a member of adherence clubs of HIV-positive people [37] | ✓ | |
| Health insurance [38] | ✓ | |
| Food security [38] | ✓ | |
| Government expenditure on health [39] | ✓ | |
| Effective governance [39] | ✓ | |
| Virology testing by 2 months of age [39] | ✓ | |
| Density of healthcare workers per 10,000 population [39] | ✓ | |
| Presence of laws to combat barriers [31] | ✓ | |
| Ensuring regular internal mentorship [40,41] | ✓ | ✓ |
| Availing supplies [40] | ✓ | |
| Providing refresher training [40] | ✓ | |
| Physician network connectedness [42] | ✓ | |
| Comfort in the clinic [43] | ✓ |
| Barriers | Coverage | Catastrophic Health Expenditure | Quality of Care |
|---|---|---|---|
| Logistical problems [44] | ✓ | ||
| ART shortage [31,44,45] | ✓ | ||
| Workload [41,44,46] | ✓ | ✓ | |
| Shortage of trained health force [41,46] | ✓ | ||
| Poverty [47] | ✓ | ||
| Stigma and discrimination [31,43,46] | ✓ | ✓ | |
| Long waiting times in ART clinic [31] | ✓ | ||
| Transportation unavailability [31] | ✓ | ||
| Cost problems [31] | ✓ | ||
| Clients fear of unwanted disclosure [45] | ✓ | ||
| Mode of transportation (motor cycle) than private car [48] | ✓ | ||
| Implementation of the free ART policy in middle income [49] | ✓ | ||
| Lack of confidentiality [43] | ✓ | ||
| Legal prosecution [43] | ✓ | ||
| Poor infrastructure [41] | ✓ | ||
| Unclear division of responsibility between health care providers [46] | ✓ | ||
| Limited training opportunity [46] | ✓ | ||
| Strict auditing [46] | ✓ |
| Determinants | More Covered (Inequity) | High Catastrophic Health Expenditure | Poor Quality of Care |
|---|---|---|---|
| Caregivers aged 40–49 years [38] | ✓ | ||
| Older [50,51] | ✓ | ✓ | |
| Age 15–19 years [52] | ✓ | ||
| Age 18–25 and 36–45 years [51] | ✓ | ✓ | |
| Female [51,52,53] | ✓ | ✓ | |
| White vs. Black [50,54,55,56] | ✓ | ||
| Urban dwellers [38,57] | ✓ | ||
| Rural residence [58,59,60,61] | ✓ | ✓ | |
| Lives far distance from health care settings [62,63,64] | ✓ | ||
| Divorced adult [48] | ✓ | ||
| Non-immigrants vs. immigrants [50] | ✓ | ||
| Educated [38] | ✓ | ||
| Being unemployed [63] | ✓ | ||
| Lower socioeconomic class [59,62,63,64] | ✓ | ||
| Belonged to nuclear family [63] | ✓ | ||
| Non-disabled vs. disabled [38] | ✓ | ||
| Live in high HIV burden area [65] | ✓ | ||
| Acquired HIV through sexual transmission rather than injection drug users [25] | ✓ | ||
| Diagnosed in later clinical stages [25] | ✓ | ||
| Had a CD4 cell count lower than 200 [63] | ✓ | ||
| Attending clinic more than 10 years [51] | ✓ | ||
| Visiting clinics every 3 months [51] | ✓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Endalamaw, A.; Gilks, C.F.; Ambaw, F.; Habtewold, T.D.; Assefa, Y. Universal Health Coverage for Antiretroviral Treatment: A Review. Infect. Dis. Rep. 2023, 15, 1-15. https://doi.org/10.3390/idr15010001
Endalamaw A, Gilks CF, Ambaw F, Habtewold TD, Assefa Y. Universal Health Coverage for Antiretroviral Treatment: A Review. Infectious Disease Reports. 2023; 15(1):1-15. https://doi.org/10.3390/idr15010001
Chicago/Turabian StyleEndalamaw, Aklilu, Charles F Gilks, Fentie Ambaw, Tesfa Dejenie Habtewold, and Yibeltal Assefa. 2023. "Universal Health Coverage for Antiretroviral Treatment: A Review" Infectious Disease Reports 15, no. 1: 1-15. https://doi.org/10.3390/idr15010001