

Features of Liver Injury in COVID-19 Pathophysiological, Biological and Clinical Particularities
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Pathophysiology and Histology
4. Biochemical Abnormalities in COVID-19
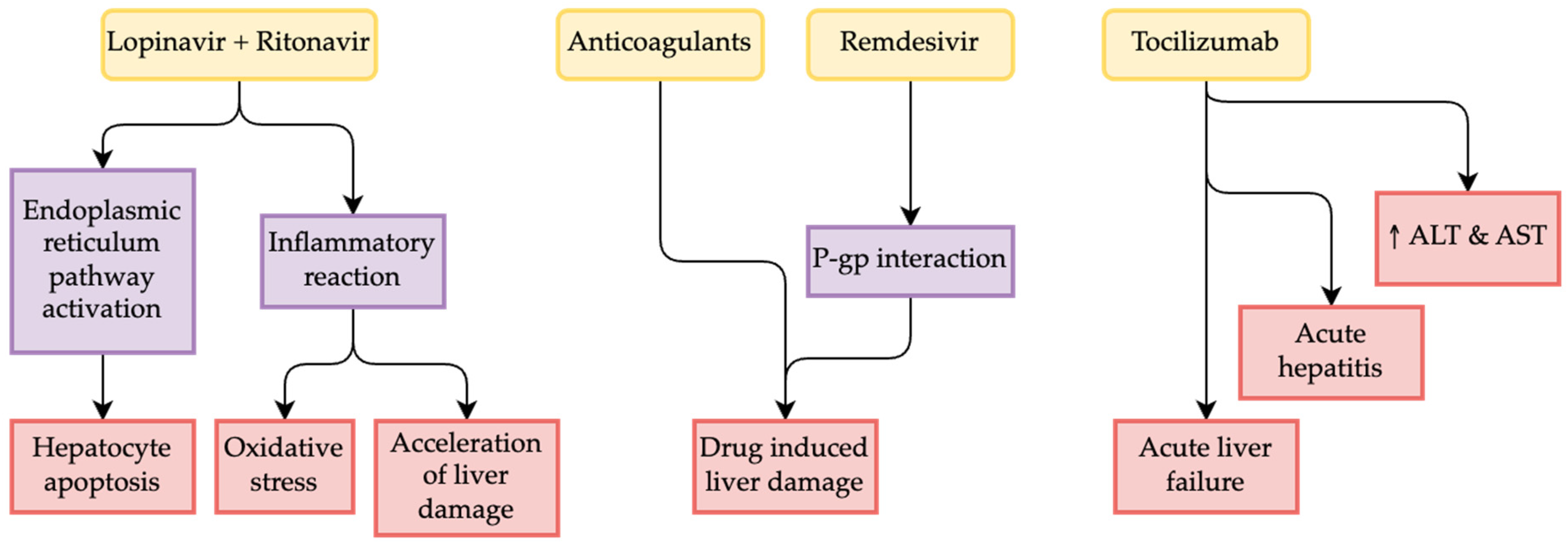
5. Drug-Induced Liver Damage
6. Clinical Correlations between SARS-CoV-2 Infection and Underlying Chronic Liver Disease
6.1. COVID-19 and Liver Cirrhosis
6.2. COVID-19 and MAFLD
6.3. COVID-19 and Chronic Hepatitis
6.4. COVID-19 and Autoimmune Hepatitis
6.5. COVID-19 and Vascular Diseases
7. COVID-19 and Cholangitis
8. COVID-19 and High-Risk Groups
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical Course and Outcomes of Critically Ill Patients with SARS-CoV-2 Pneumonia in Wuhan, China: A Single-Centered, Retrospective, Observational Study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marginean, C.M.; Popescu, M.; Vasile, C.M.; Cioboata, R.; Mitrut, P.; Popescu, I.A.S.; Biciusca, V.; Docea, A.O.; Mitrut, R.; Marginean, I.C.; et al. Challenges in the Differential Diagnosis of COVID-19 Pneumonia: A Pictorial Review. Diagnostics 2022, 12, 2823. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- McGrowder, D.A.; Miller, F.; Anderson Cross, M.; Anderson-Jackson, L.; Bryan, S.; Dilworth, L. Abnormal Liver Biochemistry Tests and Acute Liver Injury in COVID-19 Patients: Current Evidence and Potential Pathogenesis. Diseases 2021, 9, 50. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Long, X.; Zhang, B.; Zhang, W.; Chen, X.; Zhang, Z. ACE2 Expression in Pancreas May Cause Pancreatic Damage after SARS-CoV-2 Infection. Clin. Gastroenterol. Hepatol. 2020, 18, 2128–2130.e2. [Google Scholar] [CrossRef]
- Fan, Z.; Chen, L.; Li, J.; Cheng, X.; Yang, J.; Tian, C.; Zhang, Y.; Huang, S.; Liu, Z.; Cheng, J. Clinical Features of COVID-19-Related Liver Functional Abnormality. Clin. Gastroenterol. Hepatol. 2020, 18, 1561–1566. [Google Scholar] [CrossRef]
- Zhang, C.; Shi, L.; Wang, F.-S. Liver Injury in COVID-19: Management and Challenges. Lancet Gastroenterol. Hepatol. 2020, 5, 428–430. [Google Scholar] [CrossRef]
- Xu, L.; Liu, J.; Lu, M.; Yang, D.; Zheng, X. Liver Injury during Highly Pathogenic Human Coronavirus Infections. Liver Int. 2020, 40, 998–1004. [Google Scholar] [CrossRef] [Green Version]
- Albillos, A.; Lario, M.; Álvarez-Mon, M. Cirrhosis-Associated Immune Dysfunction: Distinctive Features and Clinical Relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef] [Green Version]
- Paizis, G.; Tikellis, C.; Cooper, M.E.; Schembri, J.M.; Lew, R.A.; Smith, A.I.; Shaw, T.; Warner, F.J.; Zuilli, A.; Burrell, L.M.; et al. Chronic Liver Injury in Rats and Humans Upregulates the Novel Enzyme Angiotensin Converting Enzyme 2. Gut 2005, 54, 1790–1796. [Google Scholar] [CrossRef] [Green Version]
- Chua, R.L.; Lukassen, S.; Trump, S.; Hennig, B.P.; Wendisch, D.; Pott, F.; Debnath, O.; Thürmann, L.; Kurth, F.; Völker, M.T.; et al. COVID-19 Severity Correlates with Airway Epithelium-Immune Cell Interactions Identified by Single-Cell Analysis. Nat. Biotechnol. 2020, 38, 970–979. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.G.K.; Allon, S.J.; Nyquist, S.K.; Mbano, I.M.; Miao, V.N.; Tzouanas, C.N.; Cao, Y.; Yousif, A.S.; Bals, J.; Hauser, B.M.; et al. SARS-CoV-2 Receptor ACE2 Is an Interferon-Stimulated Gene in Human Airway Epithelial Cells and Is Detected in Specific Cell Subsets across Tissues. Cell 2020, 181, 1016–1035.e19. [Google Scholar] [CrossRef] [PubMed]
- Zuo, T.; Liu, Q.; Zhang, F.; Lui, G.C.-Y.; Tso, E.Y.; Yeoh, Y.K.; Chen, Z.; Boon, S.S.; Chan, F.K.; Chan, P.K.; et al. Depicting SARS-CoV-2 Faecal Viral Activity in Association with Gut Microbiota Composition in Patients with COVID-19. Gut 2021, 70, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Lamers, M.M.; Beumer, J.; van der Vaart, J.; Knoops, K.; Puschhof, J.; Breugem, T.I.; Ravelli, R.B.G.; Paul van Schayck, J.; Mykytyn, A.Z.; Duimel, H.Q.; et al. SARS-CoV-2 Productively Infects Human Gut Enterocytes. Science 2020, 369, 50–54. [Google Scholar] [CrossRef]
- Qian, Q.; Fan, L.; Liu, W.; Li, J.; Yue, J.; Wang, M.; Ke, X.; Yin, Y.; Chen, Q.; Jiang, C. Direct Evidence of Active SARS-CoV-2 Replication in the Intestine. Clin. Infect. Dis. 2021, 73, 361–366. [Google Scholar] [CrossRef]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of Antibody Immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef]
- Berlin, D.A.; Gulick, R.M.; Martinez, F.J. Severe COVID-19. N. Engl. J. Med. 2020, 383, 2451–2460. [Google Scholar] [CrossRef]
- Chai, X.; Hu, L.; Zhang, Y.; Han, W.; Lu, Z.; Ke, A.; Zhou, J.; Shi, G.; Fang, N.; Fan, J.; et al. Specific ACE2 Expression in Cholangiocytes May Cause Liver Damage after 2019-NCoV Infection. bioRxiv 2020, bioRxiv:2020.02.03.931766. [Google Scholar]
- Li, Y.; Xiao, S.-Y. Hepatic Involvement in COVID-19 Patients: Pathology, Pathogenesis, and Clinical Implications. J. Med. Virol. 2020, 92, 1491–1494. [Google Scholar] [CrossRef]
- Yao, X.H.; Li, T.Y.; He, Z.C.; Ping, Y.F.; Liu, H.W.; Yu, S.C.; Mou, H.M.; Wang, L.H.; Zhang, H.R.; Fu, W.J.; et al. A pathological report of three COVID-19 cases by minimal invasive autopsies. Zhonghua Bing Li Xue Za Zhi 2020, 49, 411–417. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.; Lely, A.; Navis, G.; van Goor, H. Tissue Distribution of ACE2 Protein, the Functional Receptor for SARS Coronavirus. A First Step in Understanding SARS Pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Onabajo, O.O.; Banday, A.R.; Stanifer, M.L.; Yan, W.; Obajemu, A.; Santer, D.M.; Florez-Vargas, O.; Piontkivska, H.; Vargas, J.M.; Ring, T.J.; et al. Interferons and Viruses Induce a Novel Truncated ACE2 Isoform and Not the Full-Length SARS-CoV-2 Receptor. Nat. Genet. 2020, 52, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.; Altayar, O.; Siddique, S.M.; Davitkov, P.; Feuerstein, J.D.; Lim, J.K.; Falck-Ytter, Y.; El-Serag, H.B.; AGA Institute. AGA Institute Rapid Review of the Gastrointestinal and Liver Manifestations of COVID-19, Meta-Analysis of International Data, and Recommendations for the Consultative Management of Patients with COVID-19. Gastroenterology 2020, 159, 320–334.e27. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Jabri, A.; Satlin, M.J.; Campion, T.R.; Nahid, M.; Ringel, J.B.; et al. Clinical Characteristics of Covid-19 in New York City. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef]
- Youssef, M.; Hussein, M.H.; Attia, A.S.; Elshazli, R.M.; Omar, M.; Zora, G.; Farhoud, A.S.; Elnahla, A.; Shihabi, A.; Toraih, E.A.; et al. COVID-19 and Liver Dysfunction: A Systematic Review and Meta-Analysis of Retrospective Studies. J. Med. Virol. 2020, 92, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Hundt, M.A.; Deng, Y.; Ciarleglio, M.M.; Nathanson, M.H.; Lim, J.K. Abnormal Liver Tests in COVID-19: A Retrospective Observational Cohort Study of 1827 Patients in a Major U.S. Hospital Network. Hepatology 2020, 72, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Elmunzer, B.J.; Spitzer, R.L.; Foster, L.D.; Merchant, A.A.; Howard, E.F.; Patel, V.A.; West, M.K.; Qayed, E.; Nustas, R.; Zakaria, A.; et al. Digestive Manifestations in Patients Hospitalized with Coronavirus Disease 2019. Clin. Gastroenterol. Hepatol. 2021, 19, 1355–1365.e4. [Google Scholar] [CrossRef]
- Fu, Y.; Zhu, R.; Bai, T.; Han, P.; He, Q.; Jing, M.; Xiong, X.; Zhao, X.; Quan, R.; Chen, C.; et al. Clinical Features of Patients Infected with Coronavirus Disease 2019 with Elevated Liver Biochemistries: A Multicenter, Retrospective Study. Hepatology 2021, 73, 1509–1520. [Google Scholar] [CrossRef]
- Mao, R.; Qiu, Y.; He, J.-S.; Tan, J.-Y.; Li, X.-H.; Liang, J.; Shen, J.; Zhu, L.-R.; Chen, Y.; Iacucci, M.; et al. Manifestations and Prognosis of Gastrointestinal and Liver Involvement in Patients with COVID-19: A Systematic Review and Meta-Analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 667–678. [Google Scholar] [CrossRef]
- Phipps, M.M.; Barraza, L.H.; LaSota, E.D.; Sobieszczyk, M.E.; Pereira, M.R.; Zheng, E.X.; Fox, A.N.; Zucker, J.; Verna, E.C. Acute Liver Injury in COVID-19: Prevalence and Association with Clinical Outcomes in a Large U.S. Cohort. Hepatology 2020, 72, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Hajifathalian, K.; Krisko, T.; Mehta, A.; Kumar, S.; Schwartz, R.; Fortune, B.; Sharaiha, R.Z. Gastrointestinal and Hepatic Manifestations of 2019 Novel Coronavirus Disease in a Large Cohort of Infected Patients From New York: Clinical Implications. Gastroenterology 2020, 159, 1137–1140.e2. [Google Scholar] [CrossRef]
- Cholankeril, G.; Podboy, A.; Aivaliotis, V.I.; Tarlow, B.; Pham, E.A.; Spencer, S.P.; Kim, D.; Hsing, A.; Ahmed, A. High Prevalence of Concurrent Gastrointestinal Manifestations in Patients with Severe Acute Respiratory Syndrome Coronavirus 2: Early Experience From California. Gastroenterology 2020, 159, 775–777. [Google Scholar] [CrossRef]
- Bernal-Monterde, V.; Casas-Deza, D.; Letona-Giménez, L.; de la Llama-Celis, N.; Calmarza, P.; Sierra-Gabarda, O.; Betoré-Glaria, E.; Martínez-de Lagos, M.; Martínez-Barredo, L.; Espinosa-Pérez, M.; et al. SARS-CoV-2 Infection Induces a Dual Response in Liver Function Tests: Association with Mortality during Hospitalization. Biomedicines 2020, 8, 328. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Khan, A. Clinical Characteristics and Outcomes of Coronavirus Disease 2019 among Patients with Preexisting Liver Disease in the United States: A Multicenter Research Network Study. Gastroenterology 2020, 159, 768–771.e3. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Guo, Y.; Zhuang, X.; Huang, L.; Zhang, X.; Wei, F.; Yang, B. Abnormal Liver-Related Biomarkers in COVID-19 Patients and the Role of Prealbumin. Saudi J. Gastroenterol. 2020, 26, 272–278. [Google Scholar] [CrossRef]
- Sonzogni, A.; Previtali, G.; Seghezzi, M.; Grazia Alessio, M.; Gianatti, A.; Licini, L.; Morotti, D.; Zerbi, P.; Carsana, L.; Rossi, R.; et al. Liver Histopathology in Severe COVID 19 Respiratory Failure Is Suggestive of Vascular Alterations. Liver Int. 2020, 40, 2110–2116. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Yang, L.; Han, Y.; Nilsson-Payant, B.E.; Gupta, V.; Wang, P.; Duan, X.; Tang, X.; Zhu, J.; Zhao, Z.; Jaffré, F.; et al. A Human Pluripotent Stem Cell-Based Platform to Study SARS-CoV-2 Tropism and Model Virus Infection in Human Cells and Organoids. Cell Stem Cell 2020, 27, 125–136.e7. [Google Scholar] [CrossRef]
- Papic, N.; Pangercic, A.; Vargovic, M.; Barsic, B.; Vince, A.; Kuzman, I. Liver Involvement during Influenza Infection: Perspective on the 2009 Influenza Pandemic. Influenza Other Respir. Viruses 2012, 6, e2–e5. [Google Scholar] [CrossRef] [Green Version]
- Farcas, G.A.; Poutanen, S.M.; Mazzulli, T.; Willey, B.M.; Butany, J.; Asa, S.L.; Faure, P.; Akhavan, P.; Low, D.E.; Kain, K.C. Fatal Severe Acute Respiratory Syndrome Is Associated with Multiorgan Involvement by Coronavirus. J. Infect. Dis. 2005, 191, 193–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Liu, S.; Liu, H.; Li, W.; Lin, F.; Jiang, L.; Li, X.; Xu, P.; Zhang, L.; Zhao, L.; et al. SARS-CoV-2 Infection of the Liver Directly Contributes to Hepatic Impairment in Patients with COVID-19. J. Hepatol. 2020, 73, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Wang, Y.; Shao, C.; Huang, J.; Gan, J.; Huang, X.; Bucci, E.; Piacentini, M.; Ippolito, G.; Melino, G. COVID-19 Infection: The Perspectives on Immune Responses. Cell Death Differ. 2020, 27, 1451–1454. [Google Scholar] [CrossRef] [Green Version]
- Lagana, S.M.; Kudose, S.; Iuga, A.C.; Lee, M.J.; Fazlollahi, L.; Remotti, H.E.; Del Portillo, A.; De Michele, S.; de Gonzalez, A.K.; Saqi, A.; et al. Hepatic Pathology in Patients Dying of COVID-19: A Series of 40 Cases Including Clinical, Histologic, and Virologic Data. Mod. Pathol. 2020, 33, 2147–2155. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients with Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef]
- Manolis, A.S.; Manolis, T.A.; Manolis, A.A.; Papatheou, D.; Melita, H. COVID-19 Infection: Viral Macro- and Micro-Vascular Coagulopathy and Thromboembolism/Prophylactic and Therapeutic Management. J. Cardiovasc. Pharm. 2021, 26, 12–24. [Google Scholar] [CrossRef]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.D.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef]
- Middeldorp, S.; Coppens, M.; van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Müller, M.C.A.; Bouman, C.C.S.; Beenen, L.F.M.; Kootte, R.S.; Heijmans, J.; et al. Incidence of Venous Thromboembolism in Hospitalized Patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1995–2002. [Google Scholar] [CrossRef]
- Olry, A.; Meunier, L.; Délire, B.; Larrey, D.; Horsmans, Y.; Le Louët, H. Drug-Induced Liver Injury and COVID-19 Infection: The Rules Remain the Same. Drug Saf. 2020, 43, 615–617. [Google Scholar] [CrossRef]
- Weber, S.; Hellmuth, J.C.; Scherer, C.; Muenchhoff, M.; Mayerle, J.; Gerbes, A.L. Liver Function Test Abnormalities at Hospital Admission Are Associated with Severe Course of SARS-CoV-2 Infection: A Prospective Cohort Study. Gut 2021, 70, 1925–1932. [Google Scholar] [CrossRef]
- Cai, Q.; Huang, D.; Yu, H.; Zhu, Z.; Xia, Z.; Su, Y.; Li, Z.; Zhou, G.; Gou, J.; Qu, J.; et al. COVID-19: Abnormal Liver Function Tests. J. Hepatol. 2020, 73, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Ponziani, F.R.; Del Zompo, F.; Nesci, A.; Santopaolo, F.; Ianiro, G.; Pompili, M.; Gasbarrini, A.; “Gemelli against COVID-19” group. Liver Involvement Is Not Associated with Mortality: Results from a Large Cohort of SARS-CoV-2-Positive Patients. Aliment. Pharm. 2020, 52, 1060–1068. [Google Scholar] [CrossRef]
- Yip, T.C.-F.; Lui, G.C.-Y.; Wong, V.W.-S.; Chow, V.C.-Y.; Ho, T.H.-Y.; Li, T.C.-M.; Tse, Y.-K.; Hui, D.S.-C.; Chan, H.L.-Y.; Wong, G.L.-H. Liver Injury Is Independently Associated with Adverse Clinical Outcomes in Patients with COVID-19. Gut 2021, 70, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Li, G.; Chen, L.; Shu, C.; Song, J.; Wang, W.; Wang, Y.; Chen, Q.; Jin, G.; Liu, T.; et al. Association of Liver Abnormalities with In-Hospital Mortality in Patients with COVID-19. J. Hepatol. 2021, 74, 1295–1302. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zheng, L.; Liu, L.; Zhao, M.; Xiao, J.; Zhao, Q. Liver Impairment in COVID-19 Patients: A Retrospective Analysis of 115 Cases from a Single Centre in Wuhan City, China. Liver Int. 2020, 40, 2095–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, S.A.; Eid, K.M.; Anyiam, F.E.; Wadaaallah, H.; Muhamed, M.A.M.; Morsi, M.H.; Dahman, N.B.H. Liver Injury with COVID-19: Laboratory and Histopathological Outcome-Systematic Review and Meta-Analysis. Egypt. Liver J. 2022, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.K.; Singh, A.; Zhang, Q.; Bai, X.; Zhang, W.; Yadav, R.K.; Singh, A.; Zhiwei, L.; Adhikari, V.P.; Liang, T. Involvement of Liver in COVID-19: Systematic Review and Meta-Analysis. Gut 2021, 70, 807–809. [Google Scholar] [CrossRef]
- Lei, F.; Liu, Y.-M.; Zhou, F.; Qin, J.-J.; Zhang, P.; Zhu, L.; Zhang, X.-J.; Cai, J.; Lin, L.; Ouyang, S.; et al. Longitudinal Association Between Markers of Liver Injury and Mortality in COVID-19 in China. Hepatology 2020, 72, 389–398. [Google Scholar] [CrossRef]
- Bangash, M.N.; Patel, J.M.; Parekh, D.; Murphy, N.; Brown, R.M.; Elsharkawy, A.M.; Mehta, G.; Armstrong, M.J.; Neil, D. SARS-CoV-2: Is the Liver Merely a Bystander to Severe Disease? J. Hepatol. 2020, 73, 995–996. [Google Scholar] [CrossRef]
- David, S.; Hamilton, J.P. Drug-Induced Liver Injury. US Gastroenterol. Hepatol. Rev. 2010, 6, 73–80. [Google Scholar]
- Björnsson, E.S. Hepatotoxicity by Drugs: The Most Common Implicated Agents. Int. J. Mol. Sci. 2016, 17, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe COVID-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Muhović, D.; Bojović, J.; Bulatović, A.; Vukčević, B.; Ratković, M.; Lazović, R.; Smolović, B. First Case of Drug-Induced Liver Injury Associated with the Use of Tocilizumab in a Patient with COVID-19. Liver Int. 2020, 40, 1901–1905. [Google Scholar] [CrossRef] [PubMed]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012.
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Hahn, K.J.; Morales, S.J.; Lewis, J.H. Enoxaparin-Induced Liver Injury: Case Report and Review of the Literature and FDA Adverse Event Reporting System (FAERS). Drug Saf. Case Rep. 2015, 2, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrara, F.; Granata, G.; Pelliccia, C.; La Porta, R.; Vitiello, A. The Added Value of Pirfenidone to Fight Inflammation and Fibrotic State Induced by SARS-CoV-2: Anti-Inflammatory and Anti-Fibrotic Therapy Could Solve the Lung Complications of the Infection? Eur. J. Clin. Pharm. 2020, 76, 1615–1618. [Google Scholar] [CrossRef]
- Hu, T.Y.; Frieman, M.; Wolfram, J. Insights from Nanomedicine into Chloroquine Efficacy against COVID-19. Nat. Nanotechnol. 2020, 15, 247–249. [Google Scholar] [CrossRef] [Green Version]
- Feng, G.; Zheng, K.I.; Yan, Q.-Q.; Rios, R.S.; Targher, G.; Byrne, C.D.; Poucke, S.V.; Liu, W.-Y.; Zheng, M.-H. COVID-19 and Liver Dysfunction: Current Insights and Emergent Therapeutic Strategies. J. Clin. Transl. Hepatol. 2020, 8, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Abbott, C.E.; Xu, R.; Sigal, S.H. Colchicine-Induced Hepatotoxicity. ACG Case Rep. J. 2017, 4, e120. [Google Scholar] [CrossRef]
- Vitiello, A.; Ferrara, F. Remdesivir versus Ritonavir/Lopinavir in COVID-19 Patients. Ir. J. Med. Sci. 2021, 190, 1249–1250. [Google Scholar] [CrossRef]
- Mehta, K.G.; Patel, T.; Chavda, P.D.; Patel, P. Efficacy and Safety of Colchicine in COVID-19: A Meta-Analysis of Randomised Controlled Trials. RMD Open 2021, 7, e001746. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.-C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and Azithromycin as a Treatment of COVID-19: Results of an Open-Label Non-Randomized Clinical Trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef] [PubMed]
- Cortegiani, A.; Ingoglia, G.; Ippolito, M.; Giarratano, A.; Einav, S. A Systematic Review on the Efficacy and Safety of Chloroquine for the Treatment of COVID-19. J. Crit. Care 2020, 57, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Covid-19: Six Million Doses of Hydroxychloroquine Donated to US despite Lack of Evidence. BMJ 2020, 368, m1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makin, A.J.; Wendon, J.; Fitt, S.; Portmann, B.C.; Williams, R. Fulminant Hepatic Failure Secondary to Hydroxychloroquine. Gut 1994, 35, 569–570. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.M.; Monogue, M.L.; Jodlowski, T.Z.; Cutrell, J.B. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 323, 1824–1836. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, G.X.; Lenhart, G.; Becker, M.W.; Schwambach, K.H.; Tovo, C.V.; Blatt, C.R. Drug-Induced Liver Injury and COVID-19: A Review for Clinical Practice. World J. Hepatol. 2021, 13, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Noor, M.T.; Manoria, P. Immune Dysfunction in Cirrhosis. J. Clin. Transl. Hepatol. 2017, 5, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Fan, V.S.; Dominitz, J.A.; Eastment, M.C.; Locke, E.R.; Green, P.; Berry, K.; O’Hare, A.M.; Shah, J.A.; Crothers, K.; Ioannou, G.N. Risk Factors for Testing Positive for Severe Acute Respiratory Syndrome Coronavirus 2 in a National United States Healthcare System. Clin. Infect. Dis. 2021, 73, e3085–e3094. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Liang, P.S.; Locke, E.; Green, P.; Berry, K.; O’Hare, A.M.; Shah, J.A.; Crothers, K.; Eastment, M.C.; Fan, V.S.; et al. Cirrhosis and Severe Acute Respiratory Syndrome Coronavirus 2 Infection in US Veterans: Risk of Infection, Hospitalization, Ventilation, and Mortality. Hepatology 2021, 74, 322–335. [Google Scholar] [CrossRef]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.-A.; et al. Outcomes Following SARS-CoV-2 Infection in Patients with Chronic Liver Disease: An International Registry Study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef]
- Nagarajan, R.; Krishnamoorthy, Y.; Rajaa, S.; Hariharan, V.S. COVID-19 Severity and Mortality among Chronic Liver Disease Patients: A Systematic Review and Meta-Analysis. Prev. Chronic Dis. 2022, 19, E53. [Google Scholar] [CrossRef]
- Wang, Y.; Hu, M.; Yang, H. Cirrhosis Is an Independent Predictor for COVID-19 Mortality: A Meta-Analysis of Confounding Cofactors-Controlled Data. J. Hepatol. 2023, 78, e28–e31. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Garcia-Tsao, G.; Wong, F.; Biggins, S.W.; Kamath, P.S.; McGeorge, S.; Chew, M.; Pearson, M.; Shaw, J.; Kalluri, A.; et al. Cirrhosis Is Associated with High Mortality and Readmissions over 90 Days Regardless of COVID-19: A Multicenter Cohort. Liver Transpl. 2021, 27, 1343–1347. [Google Scholar] [CrossRef]
- Bushman, D.; Davidson, A.; Pathela, P.; Greene, S.K.; Weiss, D.; Reddy, V.; New York City Fatal Case-Control Study Team; Latash, J. Risk Factors for Death among Hospitalized Patients Aged 21–64 Years Diagnosed with COVID-19—New York City, March 13–April 9, 2020. J. Racial Ethn. Health Disparities 2022, 9, 1584–1599. [Google Scholar] [CrossRef]
- Castilla, J.; Guevara, M.; Miqueleiz, A.; Baigorria, F.; Ibero-Esparza, C.; Navascués, A.; Trobajo-Sanmartín, C.; Martínez-Baz, I.; Casado, I.; Burgui, C.; et al. Risk Factors of Infection, Hospitalization and Death from SARS-CoV-2: A Population-Based Cohort Study. J. Clin. Med. 2021, 10, 2608. [Google Scholar] [CrossRef]
- Simon, T.G.; Hagström, H.; Sharma, R.; Söderling, J.; Roelstraete, B.; Larsson, E.; Ludvigsson, J.F. Risk of Severe COVID-19 and Mortality in Patients with Established Chronic Liver Disease: A Nationwide Matched Cohort Study. BMC Gastroenterol. 2021, 21, 439. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.-F.; Schattenberg, J.M.; et al. A New Definition for Metabolic Dysfunction-Associated Fatty Liver Disease: An International Expert Consensus Statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Stan, I.S.; Biciuşcă, V.; Durand, P.; Petrescu, A.M.; Oancea, D.M.; Ciuciulete, A.R.; Petrescu, M.; Udriştoiu, I.; Camen, G.C.; Bălteanu, M.A.; et al. Diagnostic and Prognostic Significance of Hepatic Steatosis in Patients with Chronic Hepatitis C. Rom. J. Morphol. Embryol. 2021, 62, 765–775. [Google Scholar] [CrossRef]
- Bucurica, S.; Ionita Radu, F.; Bucurica, A.; Socol, C.; Prodan, I.; Tudor, I.; Sirbu, C.A.; Plesa, F.C.; Jinga, M. Risk of New-Onset Liver Injuries Due to COVID-19 in Preexisting Hepatic Conditions—Review of the Literature. Medicina 2023, 59, 62. [Google Scholar] [CrossRef]
- Asemota, J.; Aduli, F. The Impact of Nonalcoholic Fatty Liver Disease on the Outcomes of Coronavirus Disease 2019 Infection. Clin. Liver Dis. 2022, 19, 29–31. [Google Scholar] [CrossRef]
- Adenote, A.; Dumic, I.; Madrid, C.; Barusya, C.; Nordstrom, C.W.; Rueda Prada, L. NAFLD and Infection, a Nuanced Relationship. Can. J. Gastroenterol. Hepatol. 2021, 2021, 5556354. [Google Scholar] [CrossRef]
- Singer, C.E.; Vasile, C.M.; Popescu, M.; Popescu, A.I.S.; Marginean, I.C.; Iacob, G.A.; Popescu, M.D.; Marginean, C.M. Role of Iron Deficiency in Heart Failure—Clinical and Treatment Approach: An Overview. Diagnostics 2023, 13, 304. [Google Scholar] [CrossRef]
- Pantic, I.; Lugonja, S.; Rajovic, N.; Dumic, I.; Milovanovic, T. Colonic Diverticulosis and Non-Alcoholic Fatty Liver Disease: Is There a Connection? Medicina 2022, 58, 38. [Google Scholar] [CrossRef]
- Ronderos, D.; Omar, A.M.S.; Abbas, H.; Makker, J.; Baiomi, A.; Sun, H.; Mantri, N.; Choi, Y.; Fortuzi, K.; Shin, D.; et al. Chronic Hepatitis-C Infection in COVID-19 Patients Is Associated with in-Hospital Mortality. World J. Clin. Cases 2021, 9, 8749–8762. [Google Scholar] [CrossRef]
- Afify, S.; Eysa, B.; Hamid, F.A.; Abo-Elazm, O.M.; Edris, M.A.; Maher, R.; Abdelhalim, A.; Abdel Ghaffar, M.M.; Omran, D.A.; Shousha, H.I. Survival and Outcomes for Co-Infection of Chronic Hepatitis C with and without Cirrhosis and COVID-19: A Multicenter Retrospective Study. World J. Gastroenterol. 2021, 27, 7362–7375. [Google Scholar] [CrossRef]
- Kang, S.H.; Cho, D.-H.; Choi, J.; Baik, S.K.; Gwon, J.G.; Kim, M.Y. Association between Chronic Hepatitis B Infection and COVID-19 Outcomes: A Korean Nationwide Cohort Study. PLoS ONE 2021, 16, e0258229. [Google Scholar] [CrossRef]
- Yang, S.; Wang, S.; Du, M.; Liu, M.; Liu, Y.; He, Y. Patients with COVID-19 and HBV Coinfection Are at Risk of Poor Prognosis. Infect. Dis. 2022, 11, 1229–1242. [Google Scholar] [CrossRef]
- Kushner, T.; Cafardi, J. Chronic Liver Disease and COVID-19: Alcohol Use Disorder/Alcohol-Associated Liver Disease, Nonalcoholic Fatty Liver Disease/Nonalcoholic Steatohepatitis, Autoimmune Liver Disease, and Compensated Cirrhosis. Clin. Liver Dis. 2020, 15, 195–199. [Google Scholar] [CrossRef]
- Efe, C.; Dhanasekaran, R.; Lammert, C.; Ebik, B.; Higuera-de la Tijera, F.; Aloman, C.; Rıza Calışkan, A.; Peralta, M.; Gerussi, A.; Massoumi, H.; et al. Outcome of COVID-19 in Patients with Autoimmune Hepatitis: An International Multicenter Study. Hepatology 2021, 73, 2099–2109. [Google Scholar] [CrossRef]
- Marjot, T.; Buescher, G.; Sebode, M.; Barnes, E.; Barritt, A.S.; Armstrong, M.J.; Baldelli, L.; Kennedy, J.; Mercer, C.; Ozga, A.-K.; et al. SARS-CoV-2 Infection in Patients with Autoimmune Hepatitis. J. Hepatol. 2021, 74, 1335–1343. [Google Scholar] [CrossRef]
- Efe, C.; Lammert, C.; Taşçılar, K.; Dhanasekaran, R.; Ebik, B.; Higuera-de la Tijera, F.; Calışkan, A.R.; Peralta, M.; Gerussi, A.; Massoumi, H.; et al. Effects of Immunosuppressive Drugs on COVID-19 Severity in Patients with Autoimmune Hepatitis. Liver Int. 2022, 42, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Satyapriya, S.; Tahaseen, S.M.; Singh, K.; Kumar, A. Severe Progression of Autoimmune Hepatitis in a Young COVID-19 Adult Patient: A Case Report. J. Acute Dis. 2022, 11, 161. [Google Scholar] [CrossRef]
- Baiges, A.; Cerda, E.; Amicone, C.; Téllez, L.; Alvarado-Tapias, E.; Puente, A.; Fortea, J.I.; Llop, E.; Rocha, F.; Orts, L.; et al. Impact of SARS-CoV-2 Pandemic on Vascular Liver Diseases. Clin. Gastroenterol. Hepatol. 2022, 20, 1525–1533.e5. [Google Scholar] [CrossRef] [PubMed]
- Roth, N.C.; Kim, A.; Vitkovski, T.; Xia, J.; Ramirez, G.; Bernstein, D.; Crawford, J.M. Post-COVID-19 Cholangiopathy: A Novel Entity. Am. J. Gastroenterol. 2021, 116, 1077–1082. [Google Scholar] [CrossRef]
- Zhao, B.; Ni, C.; Gao, R.; Wang, Y.; Yang, L.; Wei, J.; Lv, T.; Liang, J.; Zhang, Q.; Xu, W.; et al. Recapitulation of SARS-CoV-2 Infection and Cholangiocyte Damage with Human Liver Ductal Organoids. Protein Cell 2020, 11, 771–775. [Google Scholar] [CrossRef] [Green Version]
- Colmenero, J.; Rodríguez-Perálvarez, M.; Salcedo, M.; Arias-Milla, A.; Muñoz-Serrano, A.; Graus, J.; Nuño, J.; Gastaca, M.; Bustamante-Schneider, J.; Cachero, A.; et al. Epidemiological Pattern, Incidence, and Outcomes of COVID-19 in Liver Transplant Patients. J. Hepatol. 2021, 74, 148–155. [Google Scholar] [CrossRef]
- Nasa, P.; Alexander, G. COVID-19 and the Liver: What Do We Know so Far? World J. Hepatol. 2021, 13, 522–532. [Google Scholar] [CrossRef]
- Rabiee, A.; Sadowski, B.; Adeniji, N.; Perumalswami, P.V.; Nguyen, V.; Moghe, A.; Latt, N.L.; Kumar, S.; Aloman, C.; Catana, A.M.; et al. Liver Injury in Liver Transplant Recipients with Coronavirus Disease 2019 (COVID-19): U.S. Multicenter Experience. Hepatology 2020, 72, 1900–1911. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; HLH Across Speciality Collaboration, UK. COVID-19: Consider Cytokine Storm Syndromes and Immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Nasa, P.; Juneja, D.; Jain, R.; Nasa, R. COVID-19 and Hemolysis, Elevated Liver Enzymes and Thrombocytopenia Syndrome in Pregnant Women-Association or Causation? World J. Virol. 2022, 11, 310–320. [Google Scholar] [CrossRef]
- Gao, Y.-D.; Ding, M.; Dong, X.; Zhang, J.-J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.-L.; Fu, W.; Li, W.; et al. Risk Factors for Severe and Critically Ill COVID-19 Patients: A Review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Ana, A.; Das, J.K.; Salam, R.A.; Padhani, Z.A.; Irfan, O.; Bhutta, Z.A. A Systematic Review and Meta-Analysis of Data on Pregnant Women with Confirmed COVID-19: Clinical Presentation, and Pregnancy and Perinatal Outcomes Based on COVID-19 Severity. J. Glob. Health 2021, 11, 05018. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical Manifestations, Risk Factors, and Maternal and Perinatal Outcomes of Coronavirus Disease 2019 in Pregnancy: Living Systematic Review and Meta-Analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- van Lieshout, L.C.E.W.; Koek, G.H.; Spaanderman, M.A.; van Runnard Heimel, P.J. Placenta Derived Factors Involved in the Pathogenesis of the Liver in the Syndrome of Haemolysis, Elevated Liver Enzymes and Low Platelets (HELLP): A Review. Pregnancy Hypertens. 2019, 18, 42–48. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Romero, R. SARS-CoV-2 Infection during Pregnancy and Risk of Preeclampsia: A Systematic Review and Meta-Analysis. Am. J. Obs. Gynecol. 2022, 226, 68–89.e3. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| OR | 95% CI | p | |
|---|---|---|---|
| Unadjusted | 5.77 | 1.19–27.91 | 0.029 |
| Model I | 6.25 | 1.23–31.71 | 0.027 |
| Model II | 6.32 | 1.16–34.54 | 0.033 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marginean, C.M.; Cinteza, E.; Vasile, C.M.; Popescu, M.; Biciusca, V.; Docea, A.O.; Mitrut, R.; Popescu, M.S.; Mitrut, P. Features of Liver Injury in COVID-19 Pathophysiological, Biological and Clinical Particularities. Gastroenterol. Insights 2023, 14, 156-169. https://doi.org/10.3390/gastroent14020012
Marginean CM, Cinteza E, Vasile CM, Popescu M, Biciusca V, Docea AO, Mitrut R, Popescu MS, Mitrut P. Features of Liver Injury in COVID-19 Pathophysiological, Biological and Clinical Particularities. Gastroenterology Insights. 2023; 14(2):156-169. https://doi.org/10.3390/gastroent14020012
Chicago/Turabian StyleMarginean, Cristina Maria, Eliza Cinteza, Corina Maria Vasile, Mihaela Popescu, Viorel Biciusca, Anca Oana Docea, Radu Mitrut, Marian Sorin Popescu, and Paul Mitrut. 2023. "Features of Liver Injury in COVID-19 Pathophysiological, Biological and Clinical Particularities" Gastroenterology Insights 14, no. 2: 156-169. https://doi.org/10.3390/gastroent14020012