
Cholangioscopy-Assisted Laser Lithotripsy for Treatment of Postcholecystectomy Mirizzi Syndrome: Case Series
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Selection
2.2. Technique Description
3. Case Reports
3.1. Case 1
3.2. Case 2
3.3. Case 3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALAT | alanine aminotransferase |
| AP | alkaline phosphatase |
| ASAT | aspartate aminotransferase |
| CA | cholangioscopy-assisted |
| CA-EHL | cholangioscopy-assisted electrohydraulic lithotripsy |
| CA-LL | cholangioscopy-assisted laser lithotripsy |
| CBD | common bile duct |
| CD | cystic duct |
| CHD | common hepatic duct |
| CDS | cystic duct stone |
| CT | computer tomography |
| EHL | electrohydraulic lithotripsy |
| ERCP | endoscopic retrograde cholangiopancreatography |
| ES | endoscopic sphincterotomy |
| ESWL | extracorporeal shockwave lithotripsy |
| EUS | endoscopic ultrasonography |
| GGT | gamma-glutamyl transpeptidase |
| IOC | intraoperative cholangiography |
| LL | laser lithotripsy |
| LC | laparoscopic cholecystectomy |
| MRCP | magnetic resonance cholangiopancreatography |
| MS | Mirizzi syndrome |
| pMS | postcholecystectomy Mirrizi syndrome |
| SOC | single-operator cholangioscopy |
| US | ultrasonography |
References
- Turner, M.A.; Fulcher, A.S. The Cystic Duct: Normal Anatomy and Disease Processes. Radiographics 2001, 21, 3–22. [Google Scholar] [CrossRef]
- Kehr, H. Die in Neiner Klinik Geubte Technik de Gallenstein Operationen, mit Einen Hinweis auf die Indikationen und die Dauerersolge; JF Lehman: Munich, Germany, 1905. [Google Scholar]
- Ruge, E. Deitrage zur chirurgischen anatomie der grossen galenwege (Ductus hepaticus, choledochus, und pancreaticus). Arch. Clin. Chir. 1908, 78, 47. [Google Scholar]
- Mirizzi, P.L. Sindrome del conducto heptico. J. Int. Chir. 1948, 8, 731–777. [Google Scholar]
- Jones, M.W.; Kashyap, S.; Ferguson, T. Gallbladder Imaging; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Yonetci, N.; Kutluana, U.; Yilmaz, M.; Sungurtekin, U.; Tekin, K. The incidence of Mirizzi syndrome in patients undergoing endoscopic retrograde cholangiopancreatography. Hepatobiliary Pancreat. Dis. Int. 2008, 7, 520–524. [Google Scholar]
- Valderrama-Treviño, A.I.; Granados-Romero, J.J.; Espejel-Deloiza, M.; Chernitzky-Camaño, J.; Mera, B.B.; Estrada-Mata, A.G.; Ceballos-Villalva, J.C.; Campos, J.A.; Argüero-Sánchez, R. Updates in Mirizzi syndrome. Hepatobiliary Surg. Nutr. 2017, 6, 170–178. [Google Scholar] [CrossRef] [Green Version]
- Antoniou, S.; Antoniou, G.A.; Makridis, C. Laparoscopic treatment of Mirizzi syndrome: A systematic review. Surg. Endosc. 2009, 24, 33–39. [Google Scholar] [CrossRef]
- Xu, X.-Q.; Hong, T.; Li, B.-L.; Liu, W.; He, X.-D.; Zheng, C.-J. Mirizzi Syndrome: Our Experience with 27 Cases in PUMC Hospital. Chin. Med. Sci. J. 2013, 28, 172–177. [Google Scholar] [CrossRef]
- Kwak, N.; Yeoun, D.; Arroyo-Mercado, F.; Mubarak, G.; Cheung, D.; Vignesh, S. Outcomes and risk factors for ERCP-related complications in a predominantly black urban population. BMJ Open Gastroenterol. 2020, 7, e000462. [Google Scholar] [CrossRef]
- Yeh, C.; Wang, S.; Liu, K.; Yeh, T.; Tsai, C.; Tseng, J.; Wu, C.; Liu, N.; Chu, Y.; Jan, Y. Surgical outcome of Mirizzi syndrome: Value of endoscopic retrograde cholangiopancreatography and laparoscopic procedures. J. Hepato-Biliary-Pancreatic Sci. 2021, 28, 760–769. [Google Scholar] [CrossRef]
- Klekowski, J.; Piekarska, A.; Góral, M.; Kozula, M.; Chabowski, M. The Current Approach to the Diagnosis and Classification of Mirizzi Syndrome. Diagnostics 2021, 11, 1660. [Google Scholar] [CrossRef] [PubMed]
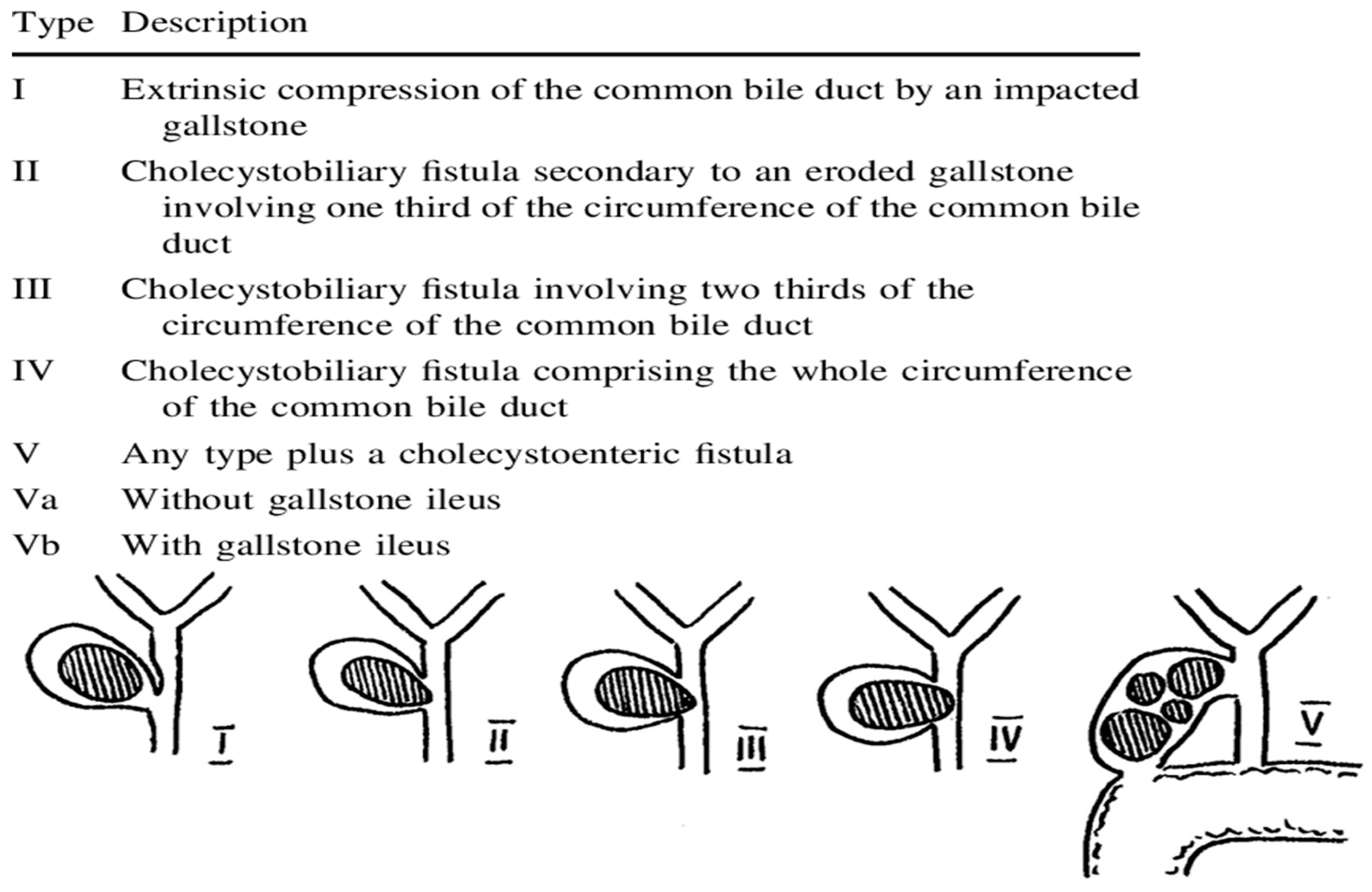
- Csendes, A.; Diaz, J.C.; Burdiles, P.; Maluenda, F.; Nava, O. Mirizzi syndrome and cholecystobiliary fistula: A unifying classification. Br. J. Surg. 1989, 76, 1139–1143. [Google Scholar] [CrossRef] [PubMed]
- McSherry, C.K.; Ferstenberg, H.; Virship, M. The Mirizzi syndrome: Suggested classification and surgical therapy. Surg. Gas-troenterol. 1982, 1, 219–225. [Google Scholar]
- Ahlawat, S.K.; Singhania, R.; Al-Kawas, F.H. Mirizzi syndrome. Curr. Treat. Options Gastroenterol. 2007, 10, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Binmoeller, K.F.; Thonke, F.; Soehendra, N. Endoscopic treatment of Mirizzi’s syndrome. Gastrointest. Endosc. 1993, 39, 532–536. [Google Scholar] [CrossRef]
- Tsuyuguchi, T.; Saisho, H.; Ishihara, T.; Yamaguchi, T.; Onuma, E.K. Long-term follow-up after treatment of Mirizzi syndrome by peroral cholangioscopy. Gastrointest. Endosc. 2000, 52, 639–644. [Google Scholar] [CrossRef]
- Jones, J.D.; Pawa, R. Single-Operator Peroral Cholangioscopy for Extraction of Cystic Duct Stones in Postcholecystectomy Mirizzi Syndrome. Case Rep. Gastrointest. Med. 2017, 2017, 1710501. [Google Scholar] [CrossRef]
- Kodali, V.P.; Petersen, B.T. Endoscopic therapy of postcholecystectomy Mirizzi syndrome. Gastrointest. Endosc. 1996, 44, 86–90. [Google Scholar] [CrossRef]
- Doykov, M. Application of a mini-percutaneous nephrolithotomy with a single aspiration shaft for the treatment of kidney stones larger than 20 mm. Clin. Urol. 2021, 1, 17–23. [Google Scholar]
- Doykov, M. Minimally Invasive Percutaneous Nephrolithotomy Combined with Holmium: YAG Laser for Treatment of Large Renal Stones Merit Research. J. Med. Med. Sci. 2022, 10, 244–248. [Google Scholar]
- Doykov, M. Mini-invasive percutaneous techniques for treatment of kidney stone disease. Med. Mag. 2022, 107, 36–38. [Google Scholar]
- Jin, Z.; Wei, Y.; Tang, X.; Shen, S.; Yang, J.; Jin, H.; Zhang, X. Single-operator peroral cholangioscope in treating difficult biliary stones: A systematic review and meta-analysis. Dig. Endosc. 2018, 31, 256–269. [Google Scholar] [CrossRef]
- Buxbaum, J.; Sahakian, A.; Ko, C.; Jayaram, P.; Lane, C.; Yu, C.Y.; Kankotia, R.; Laine, L. Randomized trial of cholangioscopy-guided laser lithotripsy versus conventional therapy for large bile duct stones (with videos). Gastrointest. Endosc. 2017, 87, 1050–1060. [Google Scholar] [CrossRef] [Green Version]
- Angsuwatcharakon, P.; Kulpatcharapong, S.; Ridtitid, W.; Boonmee, C.; Piyachaturawat, P.; Kongkam, P.; Pareesri, W.; Rerknimitr, R. Digital cholangioscopy-guided laser versus mechanical lithotripsy for large bile duct stone removal after failed papillary large-balloon dilation: A randomized study. Endoscopy 2019, 51, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, U.; Hasan, M.K.; Kommaraju, K.; Zhu, X.; Hebert-Magee, S.; Hawes, R.H.; Vargo, J.J.; Varadarajulu, S.; Parsi, M.A. Digital, single-operator cholangiopancreatoscopy in the diagnosis and management of pancreatobiliary disorders: A multicenter clinical experience (with video). Gastrointest. Endosc. 2016, 84, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Salgado-Garza, G.; Hernandez-Arriaga, P.; Gonzalez-Urquijo, M.; Díaz-Elizondo, J.A.; Flores-Villalba, E.; Rojas-Méndez, J.; Rodarte-Shade, M. Single-operator cholangioscopy and electrohydraulic lithotripsy for the treatment of Mirizzi syndrome. Ann. Med. Surg. 2021, 62, 274–277. [Google Scholar] [CrossRef]
- Pawa, R.; Dorrell, R.; Pawa, S. Endoscopic management of cystic duct stones and Mirizzi’s syndrome: Experience at an academic medical center. Endosc. Int. Open 2022, 10, E135–E144. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, S.; Bathini, R.; Sharma, A.; Maydeo, A. Usefulness of single-operator cholangioscopy-guided laser lithotripsy in patients with Mirizzi syndrome and cystic duct stones: Experience at a tertiary care center. Gastrointest. Endosc. 2016, 84, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Sepe, P.S.; Berzin, T.M.; Sanaka, S.; Patel, N.; Sawhney, M.S.; Chuttani, R.; Pleskow, D.K. Single-operator cholangioscopy for the extraction of cystic duct stones (with video). Gastrointest. Endosc. 2012, 75, 206–210. [Google Scholar] [CrossRef]
- Shim, C.S.; Moon, J.H.; Cho, Y.D.; Kim, Y.S.; Hong, S.J.; Kim, J.O.; Cho, J.Y.; Kim, Y.S.; Lee, J.S.; Lee, M.S. The role of extracorporeal shock wave lithotripsy combined with endoscopic management of impacted cystic duct stones in patients with high surgical risk. Hepato-Gastroenterology 2005, 52, 1026–1029. [Google Scholar]
- Walsh, R.M.; Ponsky, J.L.; Dumot, J. Retained gallbladder/cystic duct remnant calculi as a cause of postcholecystectomy pain. Surg. Endosc. Other Interv. Tech. 2002, 16, 981–984. [Google Scholar] [CrossRef]
- Palanivelu, C.; Rangarajan, M.; Jategaonkar, P.A.; Madankumar, M.V.; Anand, N.V. Laparoscopic Management of Remnant Cystic Duct Calculi: A Retrospective Study. Ann. R. Coll. Surg. Engl. 2009, 91, 25–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kar, A.; Gulati, S.; Mohammed, S.; Valappil, M.V.; Sarala, B.B.; Ghatak, S.; Bhattacharyya, A. Surgical Management of Cystic Duct Stump Stone or Gall Bladder Remnant Stone. Indian J. Surg. 2018, 80, 284–287. [Google Scholar] [CrossRef]
- Moon, J.H.; Cha, S.W.; Ryu, C.B.; Kim, Y.S.; Hong, S.J.; Cheon, Y.K.; Cho, Y.D.; Kim, Y.S.; Lee, J.S.; Lee, M.S.; et al. Endoscopic treatment of retained bileduct stones by using a balloon catheter for electro-hydraulic lithotripsy without cholangioscopy. Gastrointest. Endosc. 2004, 60, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Goenka, M.K.; Shah, B.B.; Rodge, G.A.; Rai, V.K.; Afzalpurkar, S.; Agarwal, R.; Goenka, U. Efficacy and safety of cholangioscopy guided laser lithotripsy for difficult bile duct stones—A prospective study from a tertiary care centre in Eastern India. Arab. J. Gastroenterol. 2021, 22, 111–114. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Sex | Type of MS | Diagnostc Method | Number of ERCP/CA-LL Sessions | Duration of CA-LL Procedure (min) | Technical/Clinical Success | Adverse Events | Follow-Up (Months) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 66 | female | 1 | ERCP | 4/2 | 270 (180 + 90) | Yes/Yes | No | 13 |
| 2 | 44 | male | 1 | ERCP | 3/1 | 84 | Yes/Yes | Mild cholangitis | 17 |
| 3 | 37 | female | 1 | ERCP | 3/1 | 40 | Yes/Yes | No | 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hristov, B.; Doykov, D.; Andonov, V.; Radev, D.; Kraev, K.; Uchikov, P.; Kostov, G.; Valova, S.; Tilkiyan, E.; Doykova, K. Cholangioscopy-Assisted Laser Lithotripsy for Treatment of Postcholecystectomy Mirizzi Syndrome: Case Series. Gastroenterol. Insights 2023, 14, 121-130. https://doi.org/10.3390/gastroent14010009
Hristov B, Doykov D, Andonov V, Radev D, Kraev K, Uchikov P, Kostov G, Valova S, Tilkiyan E, Doykova K. Cholangioscopy-Assisted Laser Lithotripsy for Treatment of Postcholecystectomy Mirizzi Syndrome: Case Series. Gastroenterology Insights. 2023; 14(1):121-130. https://doi.org/10.3390/gastroent14010009
Chicago/Turabian StyleHristov, Bozhidar, Daniel Doykov, Vladimir Andonov, Deyan Radev, Krasimir Kraev, Petar Uchikov, Gancho Kostov, Siyana Valova, Eduard Tilkiyan, and Katya Doykova. 2023. "Cholangioscopy-Assisted Laser Lithotripsy for Treatment of Postcholecystectomy Mirizzi Syndrome: Case Series" Gastroenterology Insights 14, no. 1: 121-130. https://doi.org/10.3390/gastroent14010009