
A Case of Advanced Hepatocellular Carcinoma with Bone Metastases Managed with Tyrosine Kinase Inhibitors and Aggressive Palliative Radiation Therapy: Role of Combination Therapy for Extending Survival
 , , , and
, , , and
Abstract
:1. Introduction
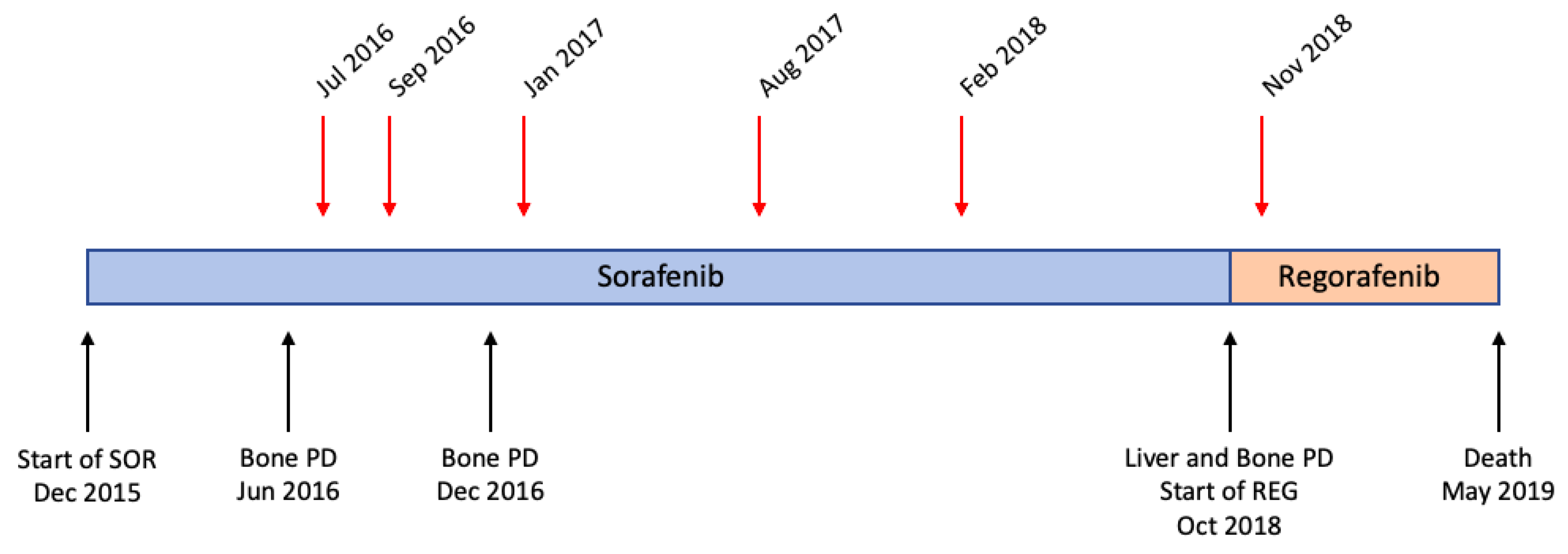
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Uka, K. Clinical features and prognosis of patients with extrahepatic metastases from hepatocellular carcinoma. World J. Gastroenterol. 2007, 13, 414. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatol. Baltim. Md. 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Aimar, G.; Marino, D.; Zichi, C.; Gamba, T.; Caglio, A.; De Vita, F.; Sperti, E.; Di Maio, M. Advanced hepatocellular carcinoma: Impact of systemic treatments on health-related quality of life and patient-reported outcomes. Liver Cancer Int. 2022, 3, 90–98. [Google Scholar] [CrossRef]
- Stefanini, B.; Tonnini, M.; Serio, I.; Renzulli, M.; Tovoli, F. Surveillance for hepatocellular carcinoma: Current status and future perspectives for improvement. Expert Rev. Anticancer Ther. 2022, 22, 371–381. [Google Scholar] [CrossRef]
- Schlageter, M.; Quagliata, L.; Matter, M.; Perrina, V.; Tornillo, L.; Terracciano, L. Clinicopathological Features and Metastatic Pattern of Hepatocellular Carcinoma: An Autopsy Study of 398 Patients. Pathobiology 2016, 83, 301–307. [Google Scholar] [CrossRef]
- Coleman, R.E.; Croucher, P.I.; Padhani, A.R.; Clézardin, P.; Chow, E.; Fallon, M.; Guise, T.; Colangeli, S.; Capanna, R.; Costa, L. Bone metastases. Nat. Rev. Dis. Primer 2020, 6, 83. [Google Scholar] [CrossRef]
- Huang, Z.; Wen, J.; Wang, Y.; Han, S.; Li, Z.; Hu, X.; Zhu, D.; Wang, Z.; Liang, J.; Chen, X.; et al. Bone metastasis of hepatocellular carcinoma: Facts and hopes from clinical and translational perspectives. Front. Med. 2022, 16, 551–573. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomised, phase 2, open-label trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef]
- Harrow, S.; Palma, D.A.; Olson, R.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Radiation for the Comprehensive Treatment of Oligometastases (SABR-COMET): Extended Long-Term Outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 611–616. [Google Scholar] [CrossRef]
- Kim, T.H.; Park, S.; Rim, C.H.; Choi, C.; Seong, J. Improved oncologic outcomes by ablative radiotherapy in patients with bone metastasis from hepatocellular carcinoma. J. Cancer Res. Clin. Oncol. 2021, 147, 2693–2700. [Google Scholar] [CrossRef]
- Hayashi, S.; Tanaka, H.; Hoshi, H. Palliative external-beam radiotherapy for bone metastases from hepatocellular carcinoma. World J. Hepatol. 2014, 6, 923–929. [Google Scholar] [CrossRef]
- Tovoli, F.; De Lorenzo, S.; Samolsky Dekel, B.G.; Piscaglia, F.; Benevento, F.; Brandi, G.; Bolondi, L. Oral oxycodone/naloxone for pain control in cirrhosis: Observational study in patients with symptomatic metastatic hepatocellular carcinoma. Liver Int. 2018, 38, 278–284. [Google Scholar] [CrossRef]
- He, J.; Shi, S.; Ye, L.; Ma, G.; Pan, X.; Huang, Y.; Zeng, Z.-C. A randomized trial of conventional fraction versus hypofraction radiotherapy for bone metastases from hepatocellular carcinoma. J. Cancer 2019, 10, 4031–4037. [Google Scholar] [CrossRef]
- Seong, J.; Koom, W.S.; Park, H.C. Radiotherapy for painful bone metastases from hepatocellular carcinoma. Liver Int. Off. J. Int. Assoc. Study Liver 2005, 25, 261–265. [Google Scholar] [CrossRef]
- He, J.; Zeng, Z.C.; Tang, Z.Y.; Fan, J.; Zhou, J.; Zeng, M.S.; Wang, J.-H.; Sun, J.; Chen, B.; Pan, B.-S. Clinical features and prognostic factors in patients with bone metastases from hepatocellular carcinoma receiving external beam radiotherapy. Cancer 2009, 115, 2710–2720. [Google Scholar] [CrossRef]
- Guo, X.; Xu, Y.; Wang, X.; Lin, F.; Wu, H.; Duan, J.; Xiong, Y.; Han, X.; Baklaushev, V.; Xiong, S.; et al. Advanced Hepatocellular Carcinoma with Bone Metastases: Prevalence, Associated Factors, and Survival Estimation. Med. Sci. Monit. 2019, 25, 1105–1112. [Google Scholar] [CrossRef]
- Van den Brande, R.; Cornips, E.M.; Peeters, M.; Ost, P.; Billiet, C.; Van de Kelft, E. Epidemiology of spinal metastases, metastatic epidural spinal cord compression and pathologic vertebral compression fractures in patients with solid tumors: A systematic review. J. Bone Oncol. 2022, 35, 100446. [Google Scholar] [CrossRef] [PubMed]
- Dawson, L.A.; Winter, K.; Knox, J.; Zhu, A.X.; Krishnan, S.; Guha, C.; Kachnic, L.A.; Gillin, M.; Hong, T.S.; Craig, T.; et al. NRG/RTOG 1112: Randomized Phase III Study of Sorafenib vs. Stereotactic Body Radiation Therapy (SBRT) Followed by Sorafenib in Hepatocellular Carcinoma (HCC) (NCT01730937). Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 1057. [Google Scholar] [CrossRef]
- Li, H.; Wu, Z.; Chen, J.; Su, K.; Guo, L.; Xu, K.; Gu, T.; Jiang, Y.; Wang, P.; Zeng, H.; et al. External radiotherapy combined with sorafenib has better efficacy in unresectable hepatocellular carcinoma: A systematic review and meta-analysis. Clin. Exp. Med. 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Tovoli, F.; Ielasi, L.; Casadei-Gardini, A.; Granito, A.; Foschi, F.G.; Rovesti, G.; Negrini, G.; Orsi, G.; Renzulli, M.; Piscaglia, F. Management of adverse events with tailored sorafenib dosing prolongs survival of hepatocellular carcinoma patients. J. Hepatol. 2019, 71, 1175–1183. [Google Scholar] [CrossRef]
- Raoul, J.L.; Adhoute, X.; Penaranda, G.; Perrier, H.; Castellani, P.; Oules, V.; Bourlière, M. Sorafenib: Experience and Better Manage-ment of Side Effects Improve Overall Survival in Hepatocellular Carcinoma Patients: A Real-Life Retrospective Analysis. Liver Cancer 2019, 8, 457–467. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Lond. Engl. 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Granito, A.; Forgione, A.; Marinelli, S.; Renzulli, M.; Ielasi, L.; Sansone, V.; Benevento, F.; Piscaglia, F.; Tovoli, F. Experience with regorafenib in the treatment of hepatocellular carcinoma. Ther. Adv. Gastroenterol. 2021, 14, 17562848211016960. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Ielasi, L.; Tovoli, F.; Piscaglia, F. Lenvatinib mesylate to treat hepatocellular carcinoma. Drugs Today 2019, 55, 305–313. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Tovoli, F.; Dadduzio, V.; De Lorenzo, S.; Rimassa, L.; Masi, G.; Iavarone, M.; Marra, F.; Garajova, I.; Brizzi, M.P.; Daniele, B.; et al. Real-Life Clinical Data of Cabozantinib for Unresectable Hepatocellular Carcinoma. Liver Cancer 2021, 10, 370–379. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Tovoli, F.; Pallotta, D.P.; Sansone, V.; Iavarone, M.; De Giorgio, M.; Ielasi, L.; Di Costanzo, G.G.; Giuffrida, P.; Sacco, R.; Pressiani, T.; et al. Outcomes of Sorafenib for Recurrent Hepatocellular Carcinoma After Liver Transplantation in the Era of Combined and Sequential Treatments. Transplantation 2023, 107, 156–161. [Google Scholar] [CrossRef]
- Ielasi, L.; Sansone, V.; Granito, A.; Benevento, F.; De Lorenzo, S.; Tovoli, F. An update of treatments of hepatocellular carcinoma in patients refractory to sorafenib. Drugs Today Barc. Spain 1998 2018, 54, 615–627. [Google Scholar] [CrossRef]
- Jose, A.; Bavetta, M.G.; Martinelli, E.; Bronte, F.; Giunta, E.F.; Manu, K.A. Hepatocellular Carcinoma: Current Therapeutic Algorithm for Localized and Advanced Disease. J. Oncol. 2022, 2022, 3817724. [Google Scholar] [CrossRef]
- Xiang, L.; Gilkes, D.M. The Contribution of the Immune System in Bone Metastasis Pathogenesis. Int. J. Mol. Sci. 2019, 20, 999. [Google Scholar] [CrossRef]
- Wang, K.; Gu, Y.; Liao, Y.; Bang, S.; Donnelly, C.R.; Chen, O.; Tao, X.; Mirando, A.J.; Hilton, M.J.; Ji, R.R. PD-1 blockade inhibits osteoclast formation and murine bone cancer pain. J. Clin. Investig. 2020, 130, 3603–3620. [Google Scholar] [CrossRef]


{kind=link}
| Date | Site | Single Dose | Sessions | Total Dose |
|---|---|---|---|---|
| Jul 2016 | 5th left rib | 4 Gy | 5 | 20 Gy |
| Sep 2016 | Left clavicle | 4 Gy | 5 | 20 Gy |
| Sep 2016 | L4 vertebra | 4 Gy | 5 | 20 Gy |
| Jan 2017 | L2 vertebra | 4 Gy | 5 | 20 Gy |
| Aug 2017 | D5 vertebra | 4 Gy | 5 | 20 Gy |
| Feb 2018 | D5 vertebra | 4 Gy | 3 | 12 Gy |
| Nov 2018 | 10th right rib | 4 Gy | 5 | 20 Gy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ielasi, L.; Stefanini, B.; Piscaglia, F.; Granito, A.; Tovoli, F. A Case of Advanced Hepatocellular Carcinoma with Bone Metastases Managed with Tyrosine Kinase Inhibitors and Aggressive Palliative Radiation Therapy: Role of Combination Therapy for Extending Survival. Gastroenterol. Insights 2023, 14, 38-44. https://doi.org/10.3390/gastroent14010005
Ielasi L, Stefanini B, Piscaglia F, Granito A, Tovoli F. A Case of Advanced Hepatocellular Carcinoma with Bone Metastases Managed with Tyrosine Kinase Inhibitors and Aggressive Palliative Radiation Therapy: Role of Combination Therapy for Extending Survival. Gastroenterology Insights. 2023; 14(1):38-44. https://doi.org/10.3390/gastroent14010005
Chicago/Turabian StyleIelasi, Luca, Bernardo Stefanini, Fabio Piscaglia, Alessandro Granito, and Francesco Tovoli. 2023. "A Case of Advanced Hepatocellular Carcinoma with Bone Metastases Managed with Tyrosine Kinase Inhibitors and Aggressive Palliative Radiation Therapy: Role of Combination Therapy for Extending Survival" Gastroenterology Insights 14, no. 1: 38-44. https://doi.org/10.3390/gastroent14010005