
Evaluation of Therapeutic Effect of Buspirone in Improving Dysphagia in Patients with GERD and Ineffective Esophageal Motility: A Randomized Clinical Trial
 ,
,
Abstract
:1. Background
2. Methods and Materials
2.1. Study Design
2.2. Randomization and Blinding
2.3. Study Tools and Data Collection
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, J.H. Ineffective esophageal motility and the vagus: Current challenges and future prospects. Clin. Exp. Gastroenterol. 2016, 9, 291–299. [Google Scholar] [CrossRef] [Green Version]
- Kahrilas, P.J.; Bredenoord, A.J.; Fox, M.; Gyawali, C.P.; Roman, S.; Smout, A.J.; Pandolfino, J.E. The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol. Motil. 2015, 27, 160–174. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.C.; Chang, C.S.; Wu, C.Y.; Chen, G.H. Ineffective esophageal motility is a primary motility disorder in gastroesophageal reflux disease. Dig. Dis. Sci. 2002, 47, 652–656. [Google Scholar] [CrossRef]
- Bredenoord, A.J.; Fox, M.; Kahrilas, P.J.; Pandolfino, J.E.; Schwizer, W.; Smout, A.J.P.M. International High Resolution Manometry Working Group Chicago classification criteria of esophageal motility disorders defined in high resolution esophageal pressure topography. Neurogastroenterol. Motil. 2012, 24 (Suppl. 1), 57–65. [Google Scholar] [CrossRef] [Green Version]
- Pandolfino, J.E.; Fox, M.R.; Bredenoord, A.J.; Kahrilas, P.J. High-resolution manometry in clinical practice: Utilizing pressure topography to classify oesophageal motility abnormalities. Neurogastroenterol. Motil. 2009, 21, 796–806. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S.K.; Pandolfino, J.E.; Kwiatek, M.A.; Kahrilas, P.J. Oesophageal peristaltic transition zone defects: Real but few and far between. Neurogastroenterol. Motil. 2008, 20, 1283–1290. [Google Scholar] [CrossRef] [Green Version]
- Kahrilas, P.J.; Ghosh, S.K.; Pandolfino, J.E. Esophageal motility disorders in terms of pressure topography: The Chicago Classification. J. Clin. Gastroenterol. 2008, 42, 627–635. [Google Scholar] [CrossRef] [Green Version]
- Pandolfino, J.E.; Roman, S.; Carlson, D.; Luger, D.; Bidari, K.; Boris, L.; Kwiatek, M.A.; Kahrilas, P.J. Distal esophageal spasm in high-resolution esophageal pressure topography: Defining clinical phenotypes. Gastroenterology 2011, 141, 469–475. [Google Scholar] [CrossRef] [Green Version]
- Pandolfino, J.E.; Leslie, E.; Luger, D.; Mitchell, B.; Kwiatek, M.A.; Kahrilas, P.J. The contractile deceleration point: An important physiologic landmark on oesophageal pressure topography. Neurogastroenterol. Motil. 2010, 22, 395. [Google Scholar] [CrossRef] [Green Version]
- Eduard, L.; Golubev, Y.; Puzikov, A. Serotonin Receptors Mediate Contractile Activity of Rat’s Esophagus In-Vivo. Arch. Organ. Transpl. 2017, 2, 019–022. [Google Scholar] [CrossRef]
- Scheerens, C.; Tack, J.; Rommel, N. Buspirone, a new drug for the management of patients with ineffective esophageal motility? United Eur. Gastroenterol J. 2015, 3, 261–265. [Google Scholar] [CrossRef]
- Hiestand, M.; Abdel-Jalil, A.; Castell, D.O. Manometric Subtypes of Ineffective Esophageal Motility. Clin. Translat. Gastroenterol. 2017, 8, 78. [Google Scholar] [CrossRef]
- Rohof, W.; Bredenoord, A.J. Chicago Classification of Esophageal Motility Disorders: Lessons Learned. Curr. Gastroenterol. Rep. 2017, 19, 37. [Google Scholar] [CrossRef] [Green Version]
- McElhiney, J.; Lohse, M.R.; Arora, A.S.; Peloquin, J.M.; Geno, D.M.; Kuntz, M.M.; Enders, F.B.; Fredericksen, M.; Abdalla, A.A.; Khan, Y.; et al. The Mayo Dysphagia Questionnaire-30: Documentation of Reliability and Validity of a Tool for Interventional Trials in Adults with Esophageal Disease. Dysphagia 2010, 25, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Boland, K.; Abdul-Hussein, M.; Tutuian, R.; Castell, D.O. Characteristics of Consecutive Esophageal Motility Diagnoses after a Decade of Change. J. Clin. Gastroenterol. 2016, 50, 301–306. [Google Scholar] [CrossRef]
- Jandee, S.; Geeraerts, A.; Geysen, H.; Rommel, N.; Tack, J.; Vanuytsel, T. Management of ineffective esophageal hypomotility. Front. Pharmacol. 2021, 12, 638915. [Google Scholar] [CrossRef]
- Denaxas, K.; Ladas, S.D.; Karamanolis, G.P. Evaluation and management of esophageal manifestations in systemic sclerosis. Ann. Gastroenterol. 2018, 31, 165–170. [Google Scholar] [CrossRef]
- Di Stefano, M.; Papathanasopoulos, A.; Blondeau, K.; Vos, R.; Boecxstaens, V.; Farre, R.; Rommel, N.; Tack, J. Effect of buspirone, a 5-HT1A receptor agonist, on esophageal motility in healthy volunteers. Dis. Esophagus 2012, 1, 470–476. [Google Scholar] [CrossRef]
- Karamanolis, G.P.; Panopoulos, S.; Denaxas, K.; Karlaftis, A.; Zorbala, A.; Kamberoglou, D.; Ladas, S.D.; Sfikakis, P.P. The 5-HT1A receptor agonist buspirone improves esophageal motor function and symptoms in systemic sclerosis: A 4-week, open-label trial. Arthritis Res. Ther. 2016, 18, 195. [Google Scholar] [CrossRef] [Green Version]
- Karamanolis, G.; Panopoulos, S.; Karlaftis, A.; Denaxas, K.; Kamberoglou, D.; Sfikakis, P.P.; Ladas, S.D. Beneficial effect of the 5-HT1A receptor agonist buspirone on esophageal dysfunction associated with systemic sclerosis: A pilot study. United Eur Gastroenterol. J. 2015, 3, 266–271. [Google Scholar] [CrossRef]
- Aggarwal, N.; Thota, P.N.; Rocio, L.; Gabbard, S. A randomized double-blind placebo-controlled crossover-style trial of buspirone in functional dysphagia and ineffective esophageal motility. Neurogastroenterol. Motil. 2017, 30, e13213. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.T.; Yazaki, E.; Sifrim, D. High-resolution manometry: Esophageal disorders not addressed by the “Chicago Classification”. J. Neurogastroenterol. Motility 2012, 18, 365. [Google Scholar] [CrossRef] [PubMed]
- Shetler, K.P.; Bikhtii, S.; Triadafilopoulos, G. Ineffective esophageal motility: Clinical, manometric, and outcome characteristics in patients with and without abnormal esophageal acid exposure. Dis. Esophagus 2017, 30, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Taghvaei, T.; Elyasi, F.; Rahbar, Z.; Neyestani, F. Effectiveness of Buspirone in Patients with Functional Dyspepsia: A Randomized, Double-Blind, Placebo-Controlled Study. Middle East J. Dig. Dis. (MEJDD) 2021, 13, 302–313. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | 45.33 ± 11.16 * | |
|---|---|---|
| Swallowing Disorder Questionnaire before treatment | 1.70 ± 0.95 | |
| MAYO score before treatment | 12.17 ± 6.01 | |
| Resting LES pressure before treatment | 10.53 ± 5.08 | |
| DCI before treatment | 283.97 ± 196.77 | |
| Integrated relaxation pressure before treatment | 4.14 ± 2.93 | |
| Swallowing Disorder Questionnaire after treatment | 0.93 ± 0.87 | |
| MAYO score after treatment | 8.60 ± 5.39 | |
| Resting LES pressure after treatment | 14.87 ± 8.66 | |
| DCI after treatment | 509.60 ± 448.36 | |
| Integrated relaxation pressure after treatment | 4.62 ± 4.09 | |
| Group | Pantoprazol | 15(50%) ** |
| Pantoprazol + Buspirone | 15(50%) | |
| Age grouping | <40 | 11(36.7%) |
| >40 | 19(63.3%) | |
| Gender | Male | 11(36.7%) |
| Female | 19(63.3%) | |
| Solid Swallowing disorder before treatment | No | 7(23.3%) |
| Yes | 23(76.7%) | |
| Liquid Swallowing disorder before treatment | No | 16(53.3%) |
| Yes | 14(46.7%) | |
| Solid Swallowing disorder after treatment | No | 11(36.7%) |
| Yes | 19(63.3%) | |
| Liquid Swallowing disorder after treatment | No | 22(73.3%) |
| Yes | 8(26.7%) | |
| Age (Mean ± SD) | p | |
|---|---|---|
| Pantoprazole | 46.46 ± 13.16 | |
| Pantoprazole + Buspirone | 44.20 ± 9.04 | 0.58 |
| Swallowing Disorder Questionnaire before treatment | ||
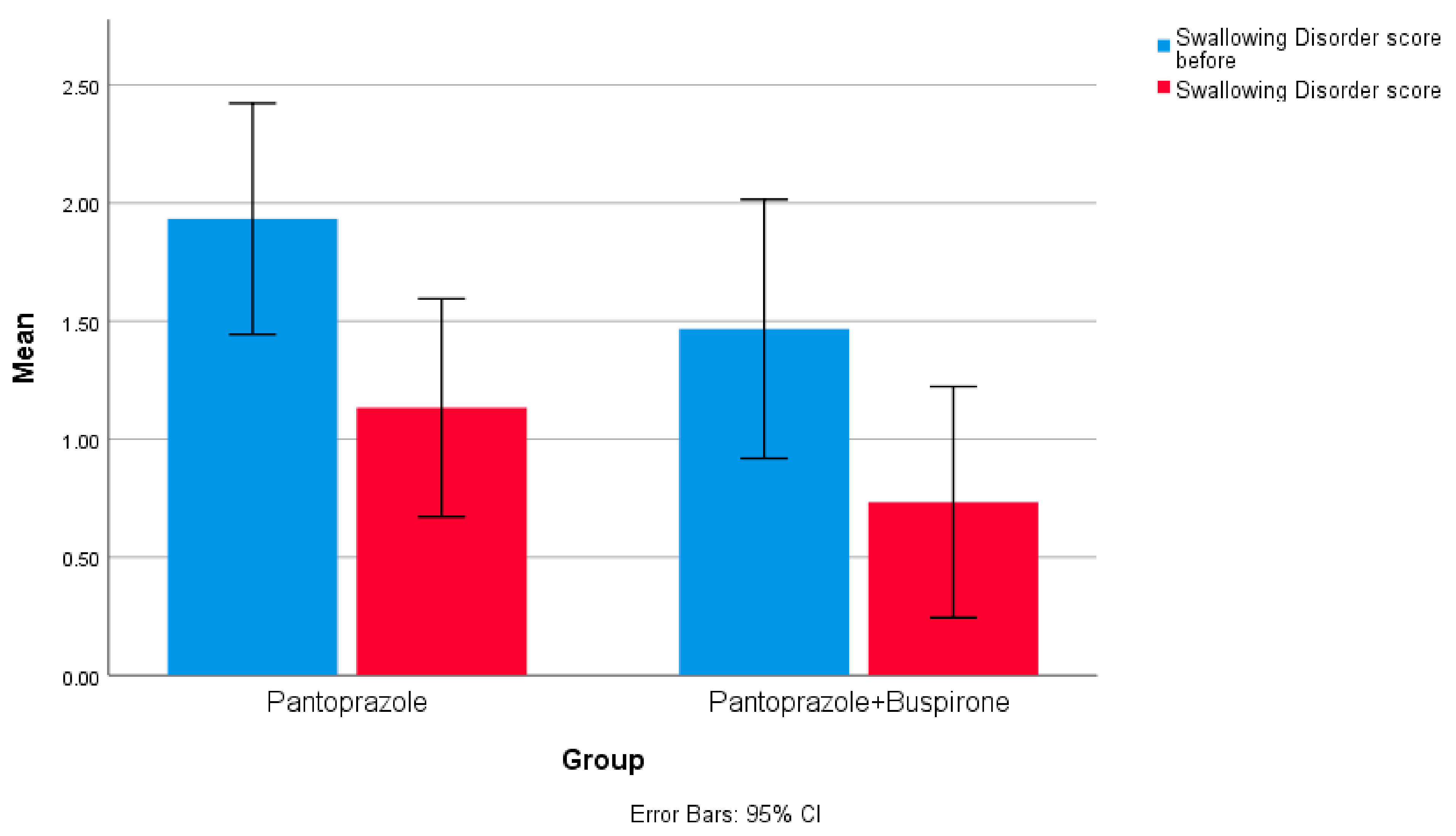
| Pantoprazole | 1.93 ± 0.88 | |
| Pantoprazole + Buspirone | 1.46 ± 0.99 | 0.18 |
| Swallowing Disorder Questionnaire after treatment | ||
| Pantoprazole | 1.13 ± 0.83 | |
| Pantoprazole + Buspirone | 0.88 ± 0.73 | 0.21 |
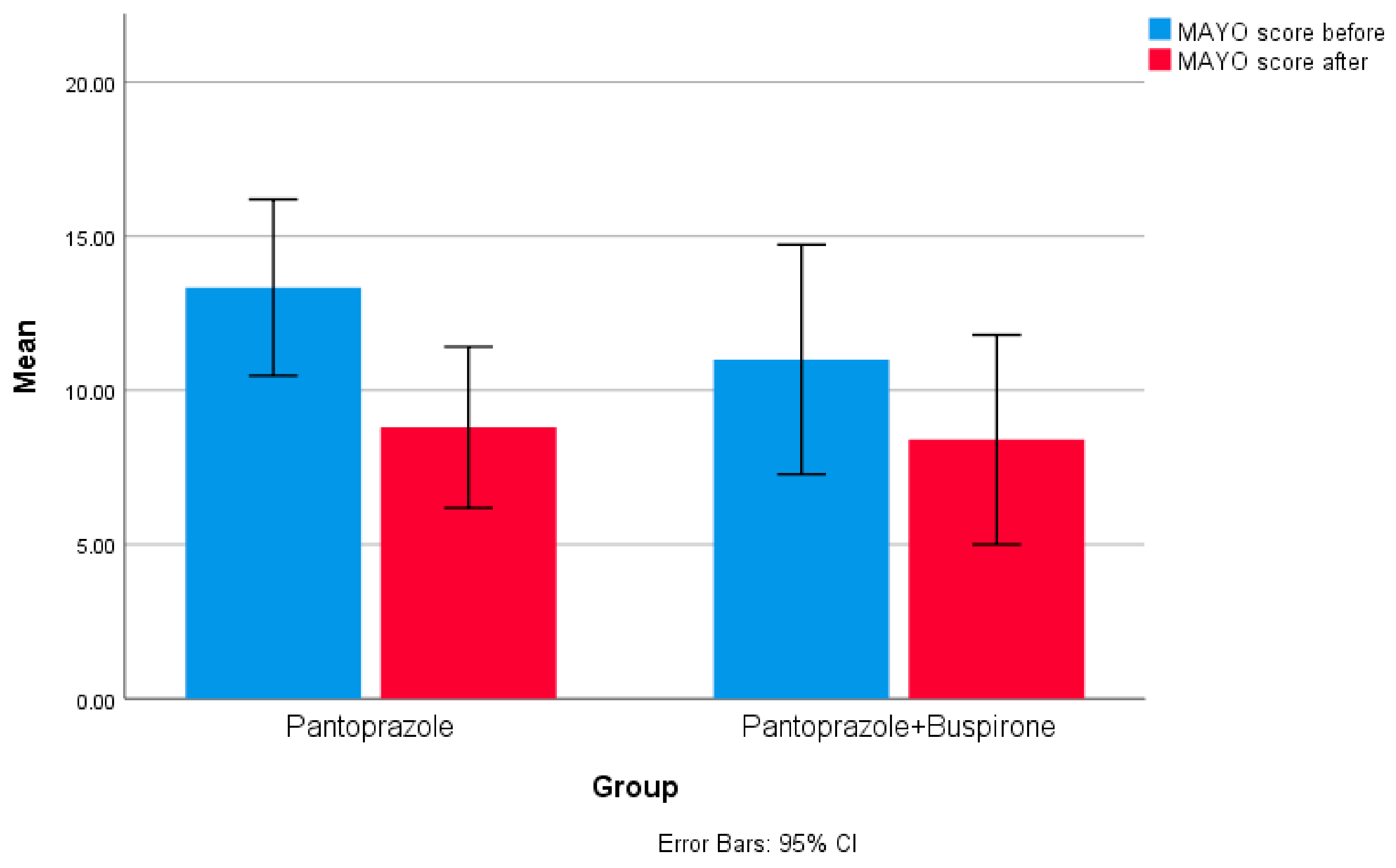
| MAYO score before treatment | ||
| Pantoprazole | 13.33 ± 5.16 | |
| Pantoprazole + Buspirone | 11.00 ± 6.72 | 0.29 |
| MAYO score after treatment | ||
| Pantoprazole | 8.80 ± 4.72 | |
| Pantoprazole + Buspirone | 8.40 ± 6.13 | 0.84 |
| Resting LES pressure before treatment | ||
| Pantoprazole | 9.40 ± 5.08 | |
| Pantoprazole + Buspirone | 11.66 ± 4.99 | 0.22 |
| Resting LES pressure after treatment | ||
| Pantoprazole | 15.00 ± 9.97 | |
| Pantoprazole + Buspirone | 14.73 ± 7.47 | 0.93 |
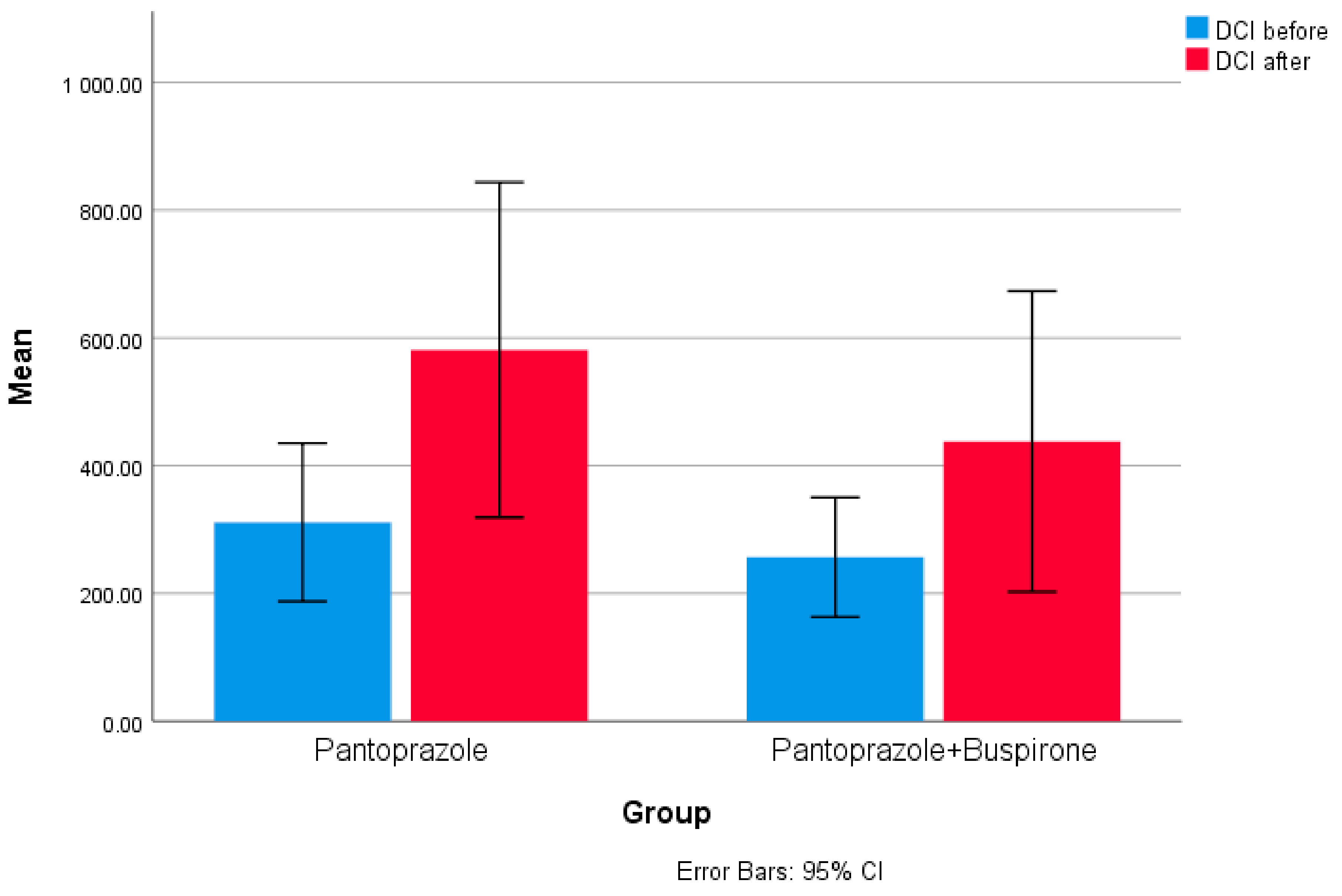
| DCI before treatment | ||
| Pantoprazole | 311.33 ± 223.74 | |
| Pantoprazole + Buspirone | 256.60 ± 168.92 | 0.45 |
| DCI after treatment | ||
| Pantoprazole | 581.26 ± 473.86 | |
| Pantoprazole + Buspirone | 437.93 ± 425.27 | 0.39 |
| Integrated relaxation pressure before treatment | ||
| Pantoprazole | 3.66 ± 2.79 | |
| Pantoprazole + Buspirone | 4.61 ± 3.08 | 0.38 |
| Integrated relaxation pressure after treatment | ||
| Pantoprazole | 4.82 ± 3.90 | |
| Pantoprazole + Buspirone | 5.00 ± 4.40 | 0.9 |
| Variables | Mean Differences(md) | Statistic Test | p | |
|---|---|---|---|---|
| Pantoprazole | Swallowing Disorder Questionnaire | 0.800 | z = −2.200 | 0.028 |
| MAYO score | 4.533 | z = −2.621 | 0.009 | |
| Resting LES pressure | −5.600 | z = −2.378 | 0.017 | |
| DCI | −269.933 | z = −2.698 | 0.007 | |
| Integrated relaxation pressure | −1.162 | z = −1.294 | 0.196 | |
| Pantoprazole + Buspirone | Swallowing Disorder Questionnaire | 0.733 | z = −2.810 | 0.005 |
| MAYO score | 2.600 | z = −2.422 | 0.015 | |
| Resting LES pressure | −3.066 | z = −2.451 | 0.014 | |
| DCI | −181.333 | z = −2.272 | 0.023 | |
| Integrated relaxation pressure | −0.390 | z = −0.377 | 0.706 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alborzi Avanaki, F.; Baghereslami, E.; Varpaei, H.A.; Farhadi, N.; Aletaha, N.; Allameh, F.; Taher, M. Evaluation of Therapeutic Effect of Buspirone in Improving Dysphagia in Patients with GERD and Ineffective Esophageal Motility: A Randomized Clinical Trial. Gastroenterol. Insights 2023, 14, 1-12. https://doi.org/10.3390/gastroent14010001
Alborzi Avanaki F, Baghereslami E, Varpaei HA, Farhadi N, Aletaha N, Allameh F, Taher M. Evaluation of Therapeutic Effect of Buspirone in Improving Dysphagia in Patients with GERD and Ineffective Esophageal Motility: A Randomized Clinical Trial. Gastroenterology Insights. 2023; 14(1):1-12. https://doi.org/10.3390/gastroent14010001
Chicago/Turabian StyleAlborzi Avanaki, Foroogh, Elham Baghereslami, Hesam Aldin Varpaei, Narges Farhadi, Najmeh Aletaha, Farshad Allameh, and Mohammad Taher. 2023. "Evaluation of Therapeutic Effect of Buspirone in Improving Dysphagia in Patients with GERD and Ineffective Esophageal Motility: A Randomized Clinical Trial" Gastroenterology Insights 14, no. 1: 1-12. https://doi.org/10.3390/gastroent14010001