
Post-Stroke Pneumonia in Real-World Practice: Background, Microbiological Examination, and Treatment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Collection and Definition of Acute Ischemic Stroke (AIS)
2.2. Definition of PSP
2.3. Collected Data
2.4. Microbiological Examination
2.5. Statistical Analysis
3. Results
3.1. PSP versus Non-PSP
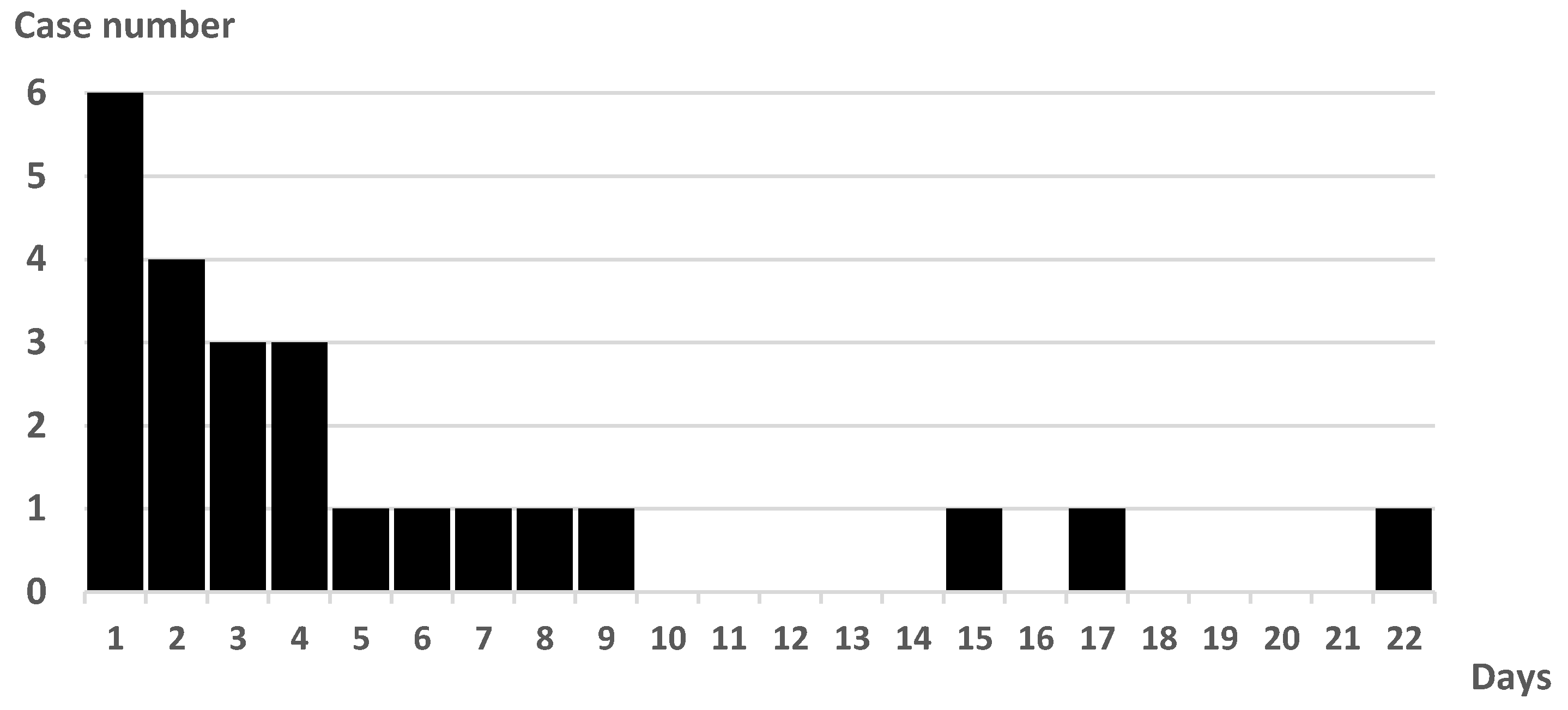
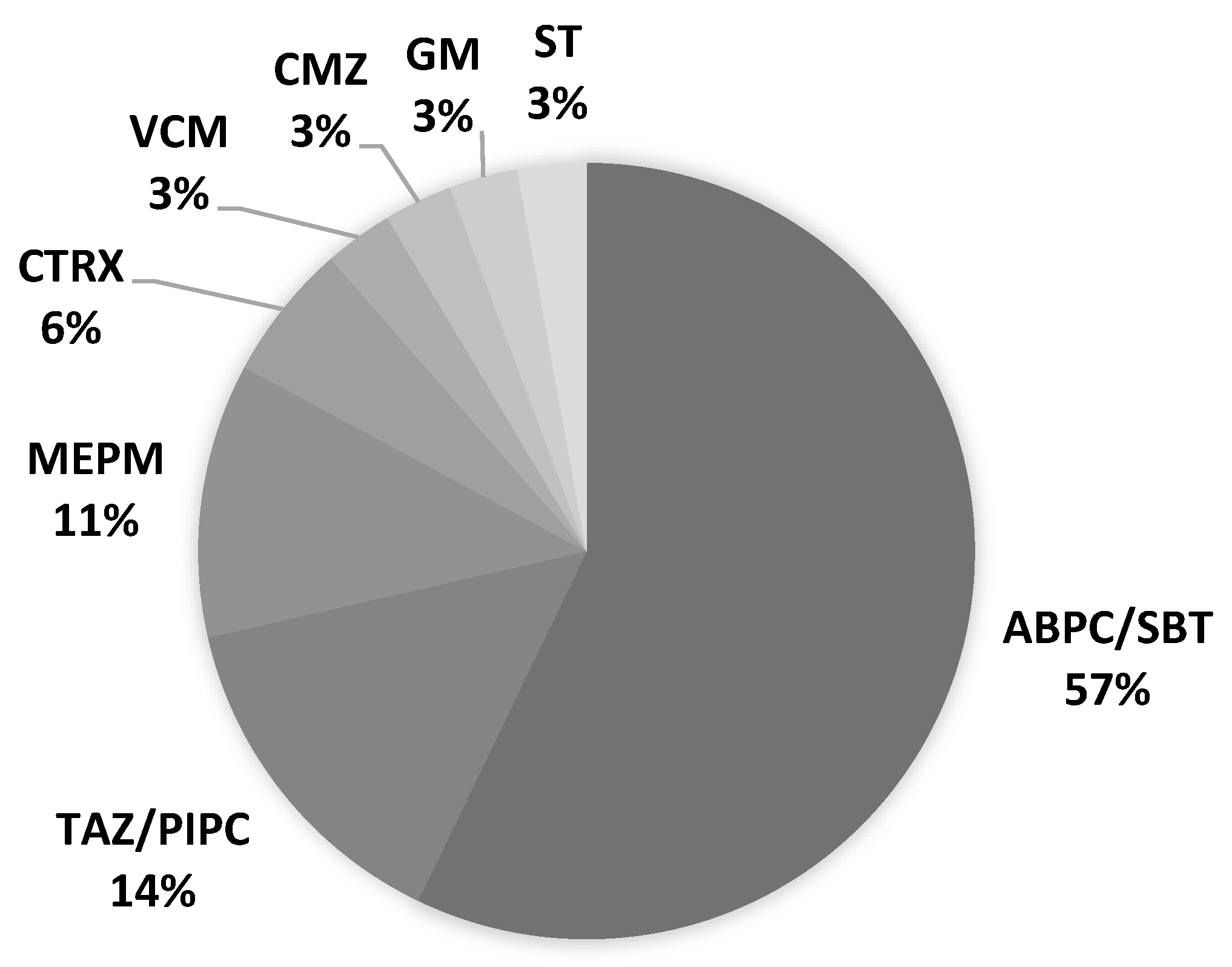
3.2. Details of PSP Cases
3.3. Good versus Poor Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, U.K.; Kodumuri, N.; Dave, M.; Lekshminarayanan, A.; Khan, N.; Kavi, T.; Kothari, R.; Lunagariya, A.; Jani, V. Stroke-Associated Pneumonia: A Retrospective Study of Risk Factors and Outcomes. Neurologist 2020, 25, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Matz, K.; Seyfang, L.; Dachenhausen, A.; Teuschl, Y.; Tuomilehto, J.; Brainin, M.; MD for the Austrian Stroke Unit Registry Collaborators. Post-stroke pneumonia at the stroke unit—A registry based analysis of contributing and protective factors. BMC Neurol. 2016, 16, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, S.; Malzahn, U.; Harms, H.; Koennecke, H.C.; Berger, K.; Kalic, M.; Walter, G.; Meisel, A.; Heuschmann, P.U. Development of a clinical score (A2DS2) to predict pneumonia in acute ischemic stroke. Stroke 2012, 43, 2617–2623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, U.; Knoblich, R.; Steinhagen, V.; Donat, M.; Benecke, R.; Kloth, A. Predictors of pneumonia in acute stroke patients admitted to a neurological intensive care unit. J. Neurol. 2007, 254, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Harms, H.; Grittner, U.; Dröge, H.; Meisel, A. Predicting post-stroke pneumonia: The PANTHERIS score. Acta Neurol. Scand. 2013, 128, 178–184. [Google Scholar] [CrossRef]
- Ji, R.; Shen, H.; Pan, Y.; Du, W.; Wang, P.; Liu, G.; Wang, Y.; Li, H.; Zhao, X.; Wang, Y. Risk score to predict hospital-acquired pneumonia after spontaneous intracerebral hemorrhage. Stroke 2014, 45, 2620–2628. [Google Scholar] [CrossRef] [Green Version]
- Ji, R.; Shen, H.; Pan, Y.; Wang, P.; Liu, G.; Wang, Y.; Li, H.; Wang, Y. Novel risk score to predict pneumonia after acute ischemic stroke. Stroke 2013, 44, 1303–1309. [Google Scholar] [CrossRef] [Green Version]
- Kwon, H.M.; Jeong, S.W.; Lee, S.H.; Yoon, B.W. The pneumonia score: A simple grading scale for prediction of pneumonia after acute stroke. Am. J. Infect. Control 2006, 34, 64–68. [Google Scholar] [CrossRef]
- Chumbler, N.R.; Williams, L.S.; Wells, C.K.; Lo, A.C.; Nadeau, S.; Peixoto, A.J.; Gorman, M.; Boice, J.L.; Concato, J.; Bravata, D.M. Derivation and validation of a clinical system for predicting pneumonia in acute stroke. Neuroepidemiology 2010, 34, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.J.; Bray, B.D.; Hoffman, A.; Meisel, A.; Heuschmann, P.U.; Wolfe, C.D.; Tyrrell, P.J.; Rudd, A.G. Can a novel clinical risk score improve pneumonia prediction in acute stroke care? A UK multicenter cohort study. J. Am. Heart Assoc. 2015, 4, e001307. [Google Scholar] [CrossRef]
- Hassan, A.; Khealani, B.A.; Shafqat, S.; Aslam, M.; Salahuddin, N.; Syed, N.A.; Baig, S.M.; Wasay, M. Stroke-associated pneumonia: Microbiological data and outcome. Singap. Med. J. 2006, 47, 204–207. [Google Scholar]
- Finlayson, O.; Kapral, M.; Hall, R.; Asllani, E.; Selchen, D.; Saposnik, G. Risk factors, inpatient care, and outcomes of pneumonia after ischemic stroke. Neurology 2011, 77, 1338–1345. [Google Scholar] [CrossRef] [PubMed]
- Katzan, I.L.; Dawson, N.V.; Thomas, C.L.; Votruba, M.E.; Cebul, R.D. The cost of pneumonia after acute stroke. Neurology 2007, 68, 1938–1943. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.; Spreckelsen, N.V.; Zhang, X.; Stavrinou, P.; Timmer, M.; Dohmen, C.; Goldbrunner, R.; Cao, F.; Zhang, Q.; Ran, Q.; et al. Should preventive antibiotics be used in patients with acute stroke? A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2017, 12, e0186607. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, S. Prophylactic Antibiotic Therapy for Preventing Poststroke Infection. Neurotherapeutics 2016, 13, 783–790. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.J.; Kishore, A.K.; Vail, A.; Chamorro, A.; Garau, J.; Hopkins, S.J.; Di Napoli, M.; Kalra, L.; Langhorne, P.; Montaner, J.; et al. Diagnosis of Stroke-Associated Pneumonia: Recommendations from the Pneumonia in Stroke Consensus Group. Stroke 2015, 46, 2335–2340. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Geckler, R.W.; Gremillion, D.H.; McAllister, C.K.; Ellenbogen, C. Microscopic and bacteriological comparison of paired sputa and transtracheal aspirates. J. Clin. Microbiol. 1977, 6, 396–399. [Google Scholar] [CrossRef]
- Horner, J.; Buoyer, F.G.; Alberts, M.J.; Helms, M.J. Dysphagia following brain-stem stroke: Clinical correlates and outcome. Arch. Neurol. 1991, 48, 1170–1173. [Google Scholar] [CrossRef]
- Arboix, A.; Massons, J.; García-Eroles, L.S.; Targa, C.; Oliveres, M.; Comes, E. Clinical Predictors of Prolonged Hospital Stay after Acute Stroke: Relevance of Medical Complications. Int. J. Clin. Med. 2012, 6, 502–507. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.E.; Kent, D.M.; Bulsara, K.R.; Leung, L.Y.; Lichtman, J.H.; Reeves, M.J.; Towfighi, A.; Whiteley, W.N.; Zahuranec, D.B. Effect of Dysphagia Screening Strategies on Clinical Outcomes After Stroke: A Systematic Review for the 2018 Guidelines for the Early Management of Patients with Acute Ischemic Stroke. Stroke 2018, 49, e123–e128. [Google Scholar] [CrossRef] [PubMed]
- Eltringham, S.A.; Kilner, K.; Gee, M.; Sage, K.; Bray, B.D.; Pownall, S.; Smith, C.J. Impact of Dysphagia Assessment and Management on Risk of Stroke-Associated Pneumonia: A Systematic Review. Cerebrovasc. Dis. 2018, 46, 99–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Solh, A.A.; Pietrantoni, C.; Bhat, A.; Aquilina, A.T.; Okada, M.; Grover, V.; Gifford, N. Microbiology of severe aspiration pneumonia in institutionalized elderly. Am. J. Respir. Crit. Care Med. 2003, 167, 1650–1654. [Google Scholar] [CrossRef] [PubMed]
- Arai, T.; Sekizawa, K.; Ohrui, T.; Fujiwara, H.; Yoshimi, N.; Matsuoka, H.; Sasaki, H. ACE inhibitors and protection against pneumonia in elderly patients with stroke. Neurology 2005, 64, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Harada, J.; Sekizawa, K. Angiotensin-converting enzyme inhibitors and pneumonia in elderly patients with intracerebral hemorrhage. J. Am. Geriatr. Soc. 2006, 54, 175–176. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, Y.; Origasa, H. Post-stroke pneumonia prevention by angiotensin-converting enzyme inhibitors: Results of a meta-analysis of five studies in Asians. Adv. Ther. 2012, 29, 900–912. [Google Scholar] [CrossRef]
- Caldeira, D.; Alarcao, J.; Vaz-Carneiro, A.; Costa, J. Risk of pneumonia associated with use of angiotensin converting enzyme inhibitors and angiotensin receptor blockers: Systematic review and meta-analysis. BMJ 2012, 345, e4260. [Google Scholar] [CrossRef] [Green Version]
- Osawa, A.; Maeshima, S.; Tanahashi, N. Efficacy of cilostazol in preventing aspiration pneumonia in acute cerebral infarction. J. Stroke Cerebrovasc. Dis. 2013, 22, 857–861. [Google Scholar] [CrossRef]
- Nakamura, Y.; Nakajima, H.; Kimura, F.; Unoda, K.; Arawaka, S. Preventive Effect of Cilostazol on Pneumonia in Patients with Acute Cerebral Infarction. J. Stroke Cerebrovasc. Dis. 2018, 27, 2354–2359. [Google Scholar] [CrossRef]
- El Solh, A.A.; Saliba, R. Pharmacologic prevention of aspiration pneumonia: A systematic review. Am. J. Geriatr. Pharmacother. 2007, 5, 352–362. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PSP n = 24 | Non-PSP n = 257 | Total n = 281 | p Value | |
|---|---|---|---|---|
| Age | 77 (65–94) | 73 (39–99) | 73 (39–99) | 0.060 |
| Male | 17 (70.8%) | 172 (66.9%) | 199 (72.4%) | 0.822 |
| Independent before stroke | 17 (70.8%) | 228 (88.7%) | 245 (89.1%) | 0.021 * |
| Past medical history | ||||
| Hypertension | 20 (83.3%) | 160 (62.3%) | 180 (65.5%) | 0.045 * |
| Diabetes mellitus | 9 (37.5%) | 71 (27.6%) | 80 (29.1%) | 0.345 |
| Smoking habit | 15 (62.5%) | 147 (57.2%) | 162 (58.9%) | 0.671 |
| Stroke | 4 (16.7%) | 57 (22.2%) | 61 (22.2%) | 0.371 |
| Neurological findings | ||||
| GCS | 14 (9–15) | 15 (5–15) | 29 (10.5%) | <0.001 * |
| Hemiparesis | 12 (50.0%) | 133 (51.8%) | 145 (52.7%) | 1.000 |
| Dysarthria | 14 (58.3%) | 95 (37.0%) | 109 (39.6%) | 0.049 * |
| Facial weakness | 9 (37.5%) | 58 (22.6%) | 67 (24.4%) | 0.130 |
| NIHSS | 4 (0–18) | 2 (0–34) | 2 (0–34) | 0.007 * |
| Types of ischemic stroke | ||||
| Large artery | 1 (4.2%) | 30 (11.7%) | 31 (11.3%) | 0.331 |
| Cardio embolism | 8 (33.3%) | 65 (25.3%) | 73 (26.5%) | |
| Small vessel | 2 (8.3%) | 62 (24.1%) | 64 (23.3%) | |
| Other determined | 4 (16.7%) | 17 (6.6%) | 21 (7.6%) | |
| Two or more causes | 0 (0%) | 17 (6.6%) | 17 (6.2%) | |
| Negative evaluation | 9 (37.5%) | 66 (25.7%) | 75 (27.3%) | |
| Lesion location ** | ||||
| Supratentorial | 19 (79.2%) | 199 (77.4%) | 218 (77.6%) | 0.540 |
| Infratentorial | 10 (41.7%) | 59 (23.0%) | 69 (24.6%) | 0.042 * |
| ISAN score | 8 (4–15) | 5 (0–20) | 13 (4.7%) | <0.001 |
| Risk group | ||||
| Low risk (0–5) | 9 (37.5%) | 156 (60.7%) | 165 (60%) | 0.006 * |
| Medium risk (6–10) | 7 (29.2%) | 75 (29.2%) | 82 (29.8%) | |
| High risk (11–14) | 7 (29.2%) | 22 (8.6%) | 29 (10.5%) | |
| Very high risk (15-) | 1 (4.2%) | 4 (1.6%) | 5 (1.8%) | |
| Complication of UTI | 4 (16.7%) | 26 (10.1%) | 30 (10.7%) | 0.244 |
| Prescription at discharge | ||||
| Cilostazol | 2 (8.3%) | 36 (14.0%) | 38 (13.8%) | 0.341 |
| ACE-I | 4 (16.7%) | 13 (5.1%) | 17 (6.2%) | 0.046 * |
| Outcome at discharge | ||||
| mRS 0 | 64 (24.9%) | 2 (8.3%) | 66 | <0.001 |
| 1 | 73 (28.4%) | 3 (12.5%) | 76 | |
| 2 | 41 (16%) | 1 (4.2%) | 42 | |
| 3 | 28 (10.9%) | 4 (16.7%) | 32 | |
| 4 | 35 (13.6%) | 2 (8.3%) | 37 | |
| 5 | 13 (5.1%) | 9 (37.5%) | 22 | |
| 6 | 3 (1.2%) | 3 (12.5%) | 6 | |
| mRS > 3 | 18 (75.0%) | 78 (30.3%) | 96 (34.1%) | <0.001 * |
| Duration of admission | 46 (9–181) | 20 (5–145) | 23 (5–181) | <0.001 * |
| Meal at discharge (survival cases) | ||||
| Normal meal | 4 (19.0%) | 180 (70.9%) | 184 (66.9%) | <0.001 * |
| Soft meal | 7 (33.3%) | 58 (22.8%) | 65 (23.6%) | 0.341 |
| Tube feeding (nasogastric tube) | 7 (33.3%) | 12 (4.7%) | 19 (6.9%) | 0.046 * |
| Tube feeding (gastric fistula) | 0 (0%) | 1 (0.4%) | 1 (0.4%) | <0.001 * |
| Intravenous hyperalimentation | 3 (14.3%) | 3 (1.2%) | 6 (2.2%) | <0.001 * |
| Good Outcome (mRS < 3) n = 184 | Poor Outcome (mRS ≥ 3) n = 97 | p Value | |
|---|---|---|---|
| Age | 71 (39–95) | 79 (46–99) | <0.001 * |
| Male | 135 (73.4%) | 54 (55.7%) | 0.002 * |
| Independent before stroke | 184 (100%) | 61 (62.9%) | <0.001 * |
| Past medical history | |||
| Hypertension | 117 (63.2%) | 63 (65.6%) | 0.793 |
| Diabetes mellitus | 57 (31.0%) | 23 (23.7%) | 0.126 |
| Smoking habit | 113 (61.4%) | 49 (50.5%) | 0.052 |
| Stroke | 40 (21.6%) | 21 (21.9%) | 0.961 |
| Neurological findings | |||
| GCS | 15 (13–15) | 15 (5–15) | <0.001 |
| Hemiparesis | 71 (38.6%) | 74 (76.3%) | <0.001 * |
| Dysarthria | 62 (33.7%) | 47 (48.5%) | 0.011 * |
| Facial weakness | 35 (19.0%) | 32 (33.0%) | 0.007 * |
| NIHSS | 1 (0–10) | 4 (0–34) | <0.001 * |
| Types of ischemic stroke | |||
| Large artery | 14 (7.6%) | 17 (17.5%) | 0.002 * |
| Cardio embolism | 45 (24.5%) | 28 (28.9%) | |
| Small vessel | 52 (28.3%) | 12 (12.4%) | |
| Other determined | 15 (8.2%) | 6 (6.2%) | |
| Two or more causes | 7 (3.8%) | 10 (10.3%) | |
| Negative evaluation | 52 (28.3%) | 23 (23.7%) | |
| Complication of UTI | 9 (4.9%) | 21 (21.6%) | <0.001 * |
| Outcome at discharge | |||
| Duration of hospitalization | 16 (5–104) | 37 (9–181) | <0.001 * |
| Meal at discharge | |||
| Normal meal | 159 (86.4%) | 24 (24.7%) | <0.001 * |
| Soft meal | 24 (13%) | 41 (42.3%) | |
| Tube feeding (nasogastric tube) | 0 (0%) | 19 (19.6%) | |
| Tube feeding (gastric fistula) | 0 (0%) | 1 (1%) | |
| Intravenous hyperalimentation | 0 (0%) | 6 (6.2%) |
| Variables | p Value | aOR (95% CI) |
|---|---|---|
| PSP | 0.002 | 6.903 (2.080–22.915) |
| NIHSS | <0.001 | 1.885 (1.563–2.273) |
| Sex (Female) | <0.001 | 2.876 (1.473–5.613) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akimoto, T.; Hara, M.; Ishihara, M.; Ogawa, K.; Nakajima, H. Post-Stroke Pneumonia in Real-World Practice: Background, Microbiological Examination, and Treatment. Neurol. Int. 2023, 15, 69-77. https://doi.org/10.3390/neurolint15010006
Akimoto T, Hara M, Ishihara M, Ogawa K, Nakajima H. Post-Stroke Pneumonia in Real-World Practice: Background, Microbiological Examination, and Treatment. Neurology International. 2023; 15(1):69-77. https://doi.org/10.3390/neurolint15010006
Chicago/Turabian StyleAkimoto, Takayoshi, Makoto Hara, Masaki Ishihara, Katsuhiko Ogawa, and Hideto Nakajima. 2023. "Post-Stroke Pneumonia in Real-World Practice: Background, Microbiological Examination, and Treatment" Neurology International 15, no. 1: 69-77. https://doi.org/10.3390/neurolint15010006