
Parameters Associated with the Required Drug Dose of Intravenous Immunoglobulin in Stable Chronic Inflammatory Demyelinating Polyradiculoneuropathy

Abstract
:1. Background
2. Methods
2.1. Study Sample and Data Collection
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Broers, M.C.; Bunschoten, C.; Nieboer, D.; Lingsma, H.F.; Jacobs, B.C. Incidence and Prevalence of Chronic Inflammatory Demyelinating Polyradiculoneuropathy: A Systematic Review and Meta-Analysis. Neuroepidemiology 2019, 52, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Bunschoten, C.; Jacobs, B.C.; Van den Bergh, P.Y.K.; Cornblath, D.R.; van Doorn, P.A. Progress in diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy. Lancet Neurol. 2019, 18, 784–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalakas, M.C.; Latov, N.; Kuitwaard, K. Intravenous immunoglobulin in chronic inflammatory demyelinating polyradiculoneuropathy (CIDP): Mechanisms of action and clinical and genetic considerations. Expert Rev. Neurother. 2022, 22, 953–962. [Google Scholar] [CrossRef]
- Doneddu, P.E.; Cocito, D.; Manganelli, F.; Fazio, R.; Briani, C.; Filosto, M.; Benedetti, L.; Mazzeo, A.; Marfia, G.A.; Cortese, A.; et al. Atypical CIDP: Diagnostic criteria, progression and treatment response. Data from the Italian CIDP Database. J. Neurol. Neurosurg. Psychiatry 2019, 90, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Bergh, P.Y.K.V.D.; Doorn, P.A.; Hadden, R.D.M.; Avau, B.; Vankrunkelsven, P.; Allen, J.A.; Attarian, S.; Blomkwist-Markens, P.H.; Cornblath, D.R.; Eftimov, F.; et al. European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint Task Force-Second revision. Eur. J. Neurol. 2021, 28, 3556–3583. [Google Scholar] [CrossRef]
- Bromberg, M.B. What Is in the Literature. J. Clin. Neuromuscul. Dis. 2022, 24, 68–74. [Google Scholar] [CrossRef]
- Hughes, R.A.; Donofrio, P.; Bril, V.; Dalakas, M.C.; Deng, C.; Hanna, K.; Hartung, H.-P.; Latov, N.; Merkies, I.S.; A van Doorn, P. Intravenous immune globulin (10% caprylate-chromatography purified) for the treatment of chronic inflammatory demyelinating polyradiculoneuropathy (ICE study): A randomised placebo-controlled trial. Lancet Neurol. 2008, 7, 136–144. [Google Scholar] [CrossRef]
- Prevot, J.; Jolles, S. Global immunoglobulin supply: Steaming towards the iceberg? Curr. Opin. Allergy Clin. Immunol. 2020, 20, 557–564. [Google Scholar] [CrossRef]
- Turecek, P.L.; Hibbett, D.; Kreil, T.R. Plasma procurement and plasma product safety in light of the COVID-19 pandemic from the perspective of the plasma industry. Vox Sang 2022, 117, 780–788. [Google Scholar] [CrossRef]
- Oaklander, A.L.; Lunn, M.P.; Hughes, R.A.; van Schaik, I.N.; Frost, C.; Chalk, C.H. Treatments for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP): An overview of systematic reviews. Cochrane Database Syst. Rev. 2017, 1, CD010369. [Google Scholar] [CrossRef]
- Eftimov, F.; Winer, J.B.; Vermeulen, M.; de Haan, R.; van Schaik, I.N. Intravenous immunoglobulin for chronic inflammatory demyelinating polyradiculoneuropathy. Cochrane Database Syst. Rev. 2013, 2, CD001797. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, S.; Misawa, S.; Mori, M.; Tamura, N.; Kubota, M.; Hattori, T. Long term prognosis of chronic inflammatory demyelinating polyneuropathy: A five year follow up of 38 cases. J. Neurol. Neurosurg. Psychiatry 2006, 77, 66–70. [Google Scholar] [CrossRef]
- Terhoeven, P.; Seybold, J.; Utz, K.S.; Nickel, F.T.; Lee, D.H.; Linker, R.A. Longer-term effects of intravenous immunoglobulin treatment in chronic inflammatory demyelinating polyneuropathy: Who benefits? J. Neurol. Sci. 2020, 419, 117169. [Google Scholar] [CrossRef] [PubMed]
- Briani, C.; Cocito, D.; Campagnolo, M.; Doneddu, P.E.; Nobile-Orazio, E. Update on therapy of chronic immune-mediated neuropathies. Neurol. Sci. 2021, 43, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Gavrilova, N.; Kamaeva, E.; Ignatova, M.; Ryabkova, V.; Lukashenko, M.; Soprun, L.; Churilov, L.; Shoenfeld, Y. Intravenouse immunoglobuline in dysautonomia. Clin. Immunol. 2022, 240, 109039. [Google Scholar] [CrossRef]
- Cornblath, D.R.; van Doorn, P.; Hartung, H.-P.; Merkies, I.S.J.; Katzberg, H.D.; Hinterberger, D.; Clodi, E.; Kastrev, S.; Rizova, V.; Massie, R.; et al. Randomized trial of three IVIg doses for treating chronic inflammatory demyelinating polyneuropathy. Brain 2022, 145, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Adrichem, M.E.; Lucke, I.M.; Vrancken, A.F.J.E.; Goedee, H.S.; Wieske, L.; Dijkgraaf, M.G.W.; Voermans, N.C.; Notermans, N.C.; Faber, C.G.; Visser, L.H.; et al. Withdrawal of intravenous immunoglobulin in chronic inflammatory demyelinating polyradiculoneuropathy. Brain 2022, 145, 1641–1652. [Google Scholar] [CrossRef]
- Allen, J.A.; Lewis, R.A. Treatment of chronic inflammatory demyelinating polyneuropathy. Muscle Nerve 2022, 66, 552–557. [Google Scholar] [CrossRef]
- Hughes, R.; Willison, H.; Bergh, P.V.D.; Comi, G.; Illa, I.; Nobile-Orazio, E.; Van Doorn, P.; Dalakas, M.; Bojar, M.; Swan, A.; et al. Randomized controlled trial of intravenous immunoglobulin versus oral prednisolone in chronic inflammatory demyelinating polyradiculoneuropathy. Ann. Neurol. 2001, 50, 195–201. [Google Scholar] [CrossRef]
- Kleyweg, R.P.; van der Meche, F.G.; Schmitz, P.I. Interobserver agreement in the assessment of muscle strength and functional abilities in Guillain-Barre syndrome. Muscle Nerve 1991, 14, 1103–1109. [Google Scholar] [CrossRef]
- Bouchard, C.; Lacroix, C.; Plante, V.; Adams, D.; Chedru, F.; Guglielmi, J.M.; Said, G. Clinicopathologic findings and prognosis of chronic inflammatory demyelinating polyneuropathy. Neurology 1999, 52, 498. [Google Scholar] [CrossRef] [PubMed]
- Querol, L.; Crabtree, M.; Herepath, M.; Priedane, E.; Viejo, I.V.; Agush, S.; Sommerer, P. Systematic literature review of burden of illness in chronic inflammatory demyelinating polyneuropathy (CIDP). J. Neurol. 2021, 268, 3706–3716. [Google Scholar] [CrossRef] [PubMed]
- Lunn, M.P.; Manji, H.; Choudhary, P.P.; Hughes, R.A.; Thomas, P.K. Chronic inflammatory demyelinating polyradiculoneuropathy: A prevalence study in south east England. J. Neurol. Neurosurg. Psychiatry 1999, 66, 677–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thirouin, J.; Petiot, P.; Antoine, J.; André-Obadia, N.; Convers, P.; Gavoille, A.; Bouhour, F.; Rheims, S.; Camdessanché, J. Usefulness and prognostic value of diagnostic tests in patients with possible chronic inflammatory demyelinating polyradiculoneuropathy. Muscle Nerve 2022, 66, 304–311. [Google Scholar] [CrossRef]
- Iijima, M.; Yamamoto, M.; Hirayama, M.; Tanaka, F.; Katsuno, M.; Mori, K.; Koike, H.; Hattori, N.; Arimura, K.; Nakagawa, M.; et al. Clinical and electrophysiologic correlates of IVIg responsiveness in CIDP. Neurology 2005, 64, 1471–1475. [Google Scholar] [CrossRef]
- Hahn, A.F.; Bolton, C.F.; Zochodne, D.; Feasby, T.E. Intravenous immunoglobulin treatment in chronic inflammatory demyelinating polyneuropathy. A double-blind, placebo-controlled, cross-over study. Brain 1996, 119, 1067–1077. [Google Scholar] [CrossRef] [Green Version]
- Rajabally, Y.A.; Seow, H.; Wilson, P. Dose of intravenous immunoglobulins in chronic inflammatory demyelinating polyneuropathy. J. Peripher. Nerv. Syst. 2006, 11, 325–329. [Google Scholar] [CrossRef]
- Alonge, P.; Di Stefano, V.; Lupica, A.; Gangitano, M.; Torrente, A.; Pignolo, A.; Maggio, B.; Iacono, S.; Gentile, F.; Brighina, F. Clinical and Neurophysiological Follow-Up of Chronic Inflammatory Demyelinating Polyneuropathy Patients Treated with Subcutaneous Immunoglobulins: A Real-Life Single Center Study. Brain Sci. 2022, 13, 10. [Google Scholar] [CrossRef]
- Ricciardi, D.; Amitrano, F.; Coccia, A.; Todisco, V.; Trojsi, F.; Tedeschi, G.; Cirillo, G. Neurophysiological Hallmarks of Axonal Degeneration in CIDP Patients: A Pilot Analysis. Brain Sci. 2022, 12, 1510. [Google Scholar] [CrossRef]
- Cosentino, G.; Di Stefano, V.; Presti, R.L.; Montana, M.; Todisco, M.; Gastaldi, M.; Cortese, A.; Alfonsi, E.; Tassorelli, C.; Fierro, B.; et al. Expression pattern of matrix metalloproteinases-2 and -9 and their tissue inhibitors in patients with chronic inflammatory demyelinating polyneuropathy. Neurol. Sci. 2021, 42, 4297–4300. [Google Scholar] [CrossRef]
- Kapoor, M.; Carr, A.; Foiani, M.; Heslegrave, A.; Zetterberg, H.; Malaspina, A.; Compton, L.; Hutton, E.; Rossor, A.; Reilly, M.M.; et al. Association of plasma neurofilament light chain with disease activity in chronic inflammatory demyelinating polyradiculoneuropathy. Eur. J. Neurol. 2022, 29, 3347–3357. [Google Scholar] [CrossRef] [PubMed]
- Wieske, L.; Smyth, D.; Lunn, M.P.; Eftimov, F.; Teunissen, C.E. Fluid Biomarkers for Monitoring Structural Changes in Polyneuropathies: Their Use in Clinical Practice and Trials. Neurotherapeutics 2021, 18, 2351–2367. [Google Scholar] [CrossRef] [PubMed]
- Kuitwaard, K.; De Gelder, J.; Tio-Gillen, A.P.; Hop, W.C.J.; Van Gelder, T.; Van Toorenenbergen, A.W.; Van Doorn, P.A.; Jacobs, B.C. Pharmacokinetics of intravenous immunoglobulin and outcome in Guillain-Barre syndrome. Ann. Neurol. 2009, 66, 597–603. [Google Scholar] [CrossRef] [PubMed]
- van Doorn, P.A.; Kuitwaard, K.; Jacobs, B.C. Serum IgG levels as biomarkers for optimizing IVIg therapy in CIDP. J. Peripher. Nerv. Syst. 2011, 16, 38–40. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Drug Dose, p-Value | ||
|---|---|---|
| Age, median, (iqr) | 64 (57–70) | <0.001 ** |
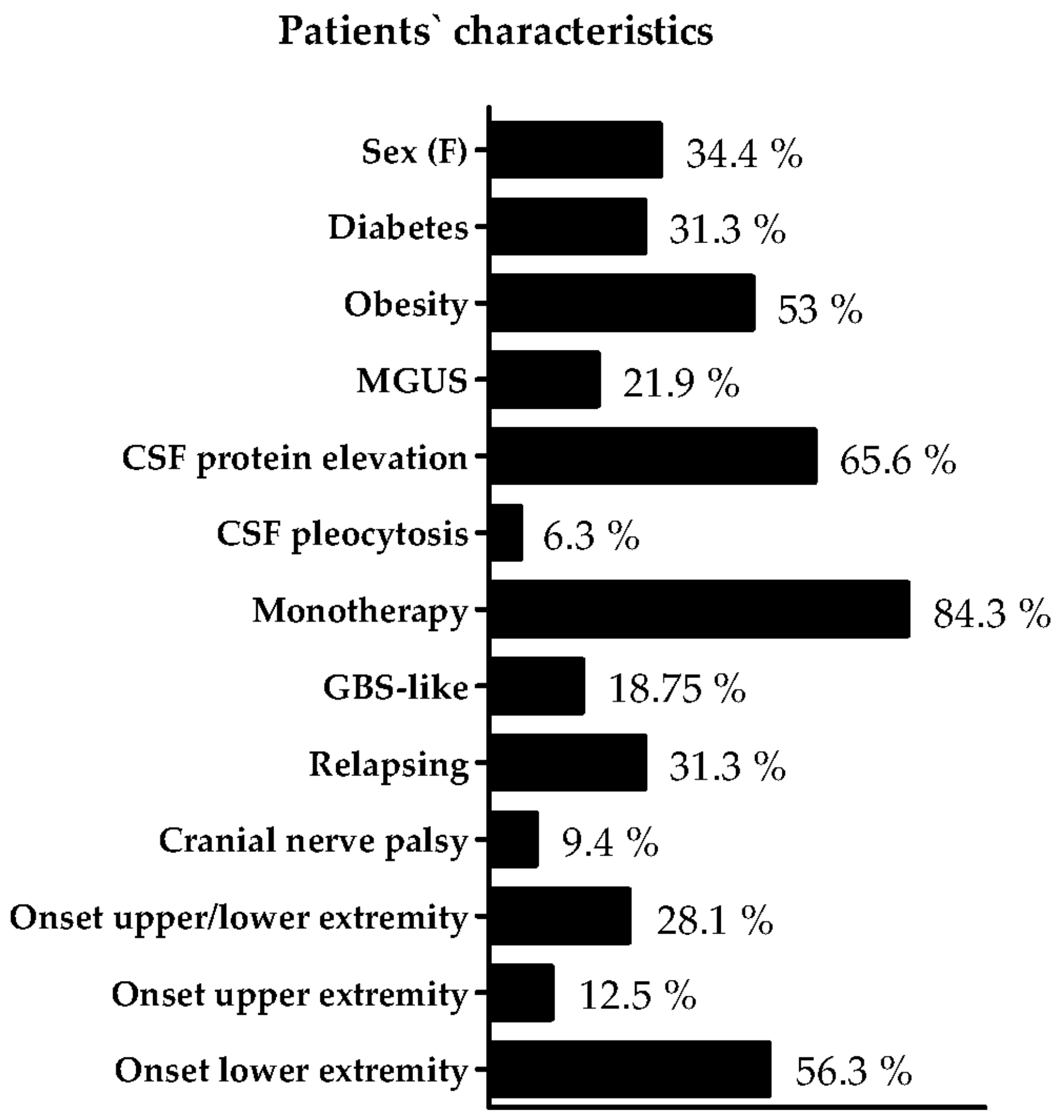
| Sex, female n, (%) | 11 (34.4) | 0.207 |
| Diabetes, n, (%) | 10 (31.3) | 0.350 |
| Obesity, n, (%) | 17 (53) | 0.358 |
| MGUS, n (%) | 7 (21.9) | 0.183 |
| MGUS IgM | 3 (9.4) | 0.631 |
| MGUS IgA | 2 (6.3) | - |
| MGUS IgG | 4 (12.5) | 0.110 |
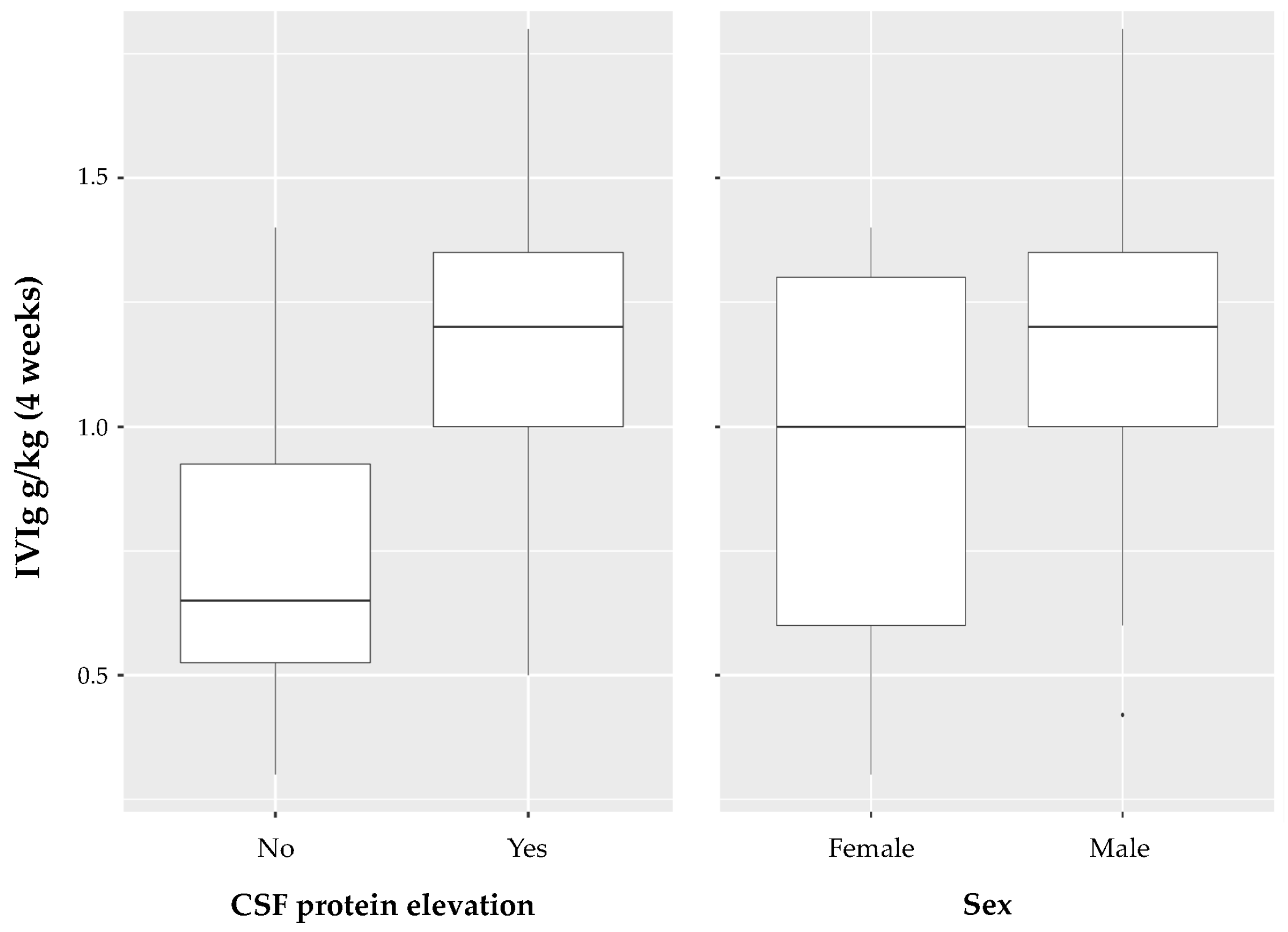
| CSF protein elevation, n, (%) | 21 (65.6) | 0.049 * |
| CSF pleocytosis, n, (%) | 2 (6.3) | - |
| IVIg monotherapy, n, (%) | 27 (84.3) | 0.107 |
| GBS like, n, (%) | 6 (18.75) | 0.147 |
| Relapsing, n, (%) | 10 (31.3) | 0.412 |
| Cranial nerve palsy, n, (%) | 3 (9.4) | 0.909 |
| Upper and lower extremity, n, (%) | 9 (28.1) | 0.606 |
| Only upper extremity, n, (%) | 4 (12.5) | 0.455 |
| Only lower extremity, n, (%) | 18 (56.3) | 0.705 |
| Disease duration (median, iqr) | 10 (4.8–14.3) | <0.001 ** |
| Delay onset/diagnosis (median, iqr) | 1 (0–3.5) | <0.001 ** |
| INCAT Score, median (iqr) | 2 (1–4.6) | 0.013 * |
| MRC SS, median (iqr) | 58 (53.8–60) | <0.001 ** |
| Univariable Model | Multivariable Model | |||
|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | |
| Age | 0.01 (0.00–0.02) | 0.0175 * | 0.01 (0.0–0.02) | 0.149 |
| Sex, male | 0.19 (−0.09–0.02) | 0.182 | 0.32 (0.02–0.62) | 0.037 |
| CSF protein elevation | 0.42 (0.09–0.74) | 0.0141 * | 0.33 (0.02–0.65) | 0.036 |
| Diabetes | 0.11 (−0.18–0.40) | 0.437 | ||
| Obesity | 0.12 (−0.15–0.39) | 0.356 | ||
| MGUS | 0.23 (−0.09–0.55) | 0.157 | ||
| GBS like | −0.22 (−0.56–0.13) | 0.214 | ||
| Relapsing | −0.1 (−0.4–0.19) | 0.483 | ||
| INCAT score | 0.07 (0.01–0.12) | 0.014 * | ||
| MRC SS | −0.03 (−0.05–0.00) | 0.027 * | −0.02 (−0.05–0.0) | 0.080 |
| Delay onset/diagnosis | 0.01 (−0.01–0.04) | 0.303 | −0.02 (−0.05–0.01) | 0.172 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feyen, L.; Schaub, C.; Zimmermann, J.; Nitsch, L. Parameters Associated with the Required Drug Dose of Intravenous Immunoglobulin in Stable Chronic Inflammatory Demyelinating Polyradiculoneuropathy. Neurol. Int. 2023, 15, 405-414. https://doi.org/10.3390/neurolint15010027
Feyen L, Schaub C, Zimmermann J, Nitsch L. Parameters Associated with the Required Drug Dose of Intravenous Immunoglobulin in Stable Chronic Inflammatory Demyelinating Polyradiculoneuropathy. Neurology International. 2023; 15(1):405-414. https://doi.org/10.3390/neurolint15010027
Chicago/Turabian StyleFeyen, Ludger, Christina Schaub, Julian Zimmermann, and Louisa Nitsch. 2023. "Parameters Associated with the Required Drug Dose of Intravenous Immunoglobulin in Stable Chronic Inflammatory Demyelinating Polyradiculoneuropathy" Neurology International 15, no. 1: 405-414. https://doi.org/10.3390/neurolint15010027