
Optimizing Vancomycin Therapy in Critically Ill Children: A Population Pharmacokinetics Study to Inform Vancomycin Area under the Curve Estimation Using Novel Biomarkers

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dosing, PK Sampling, and Biomarker Measurement
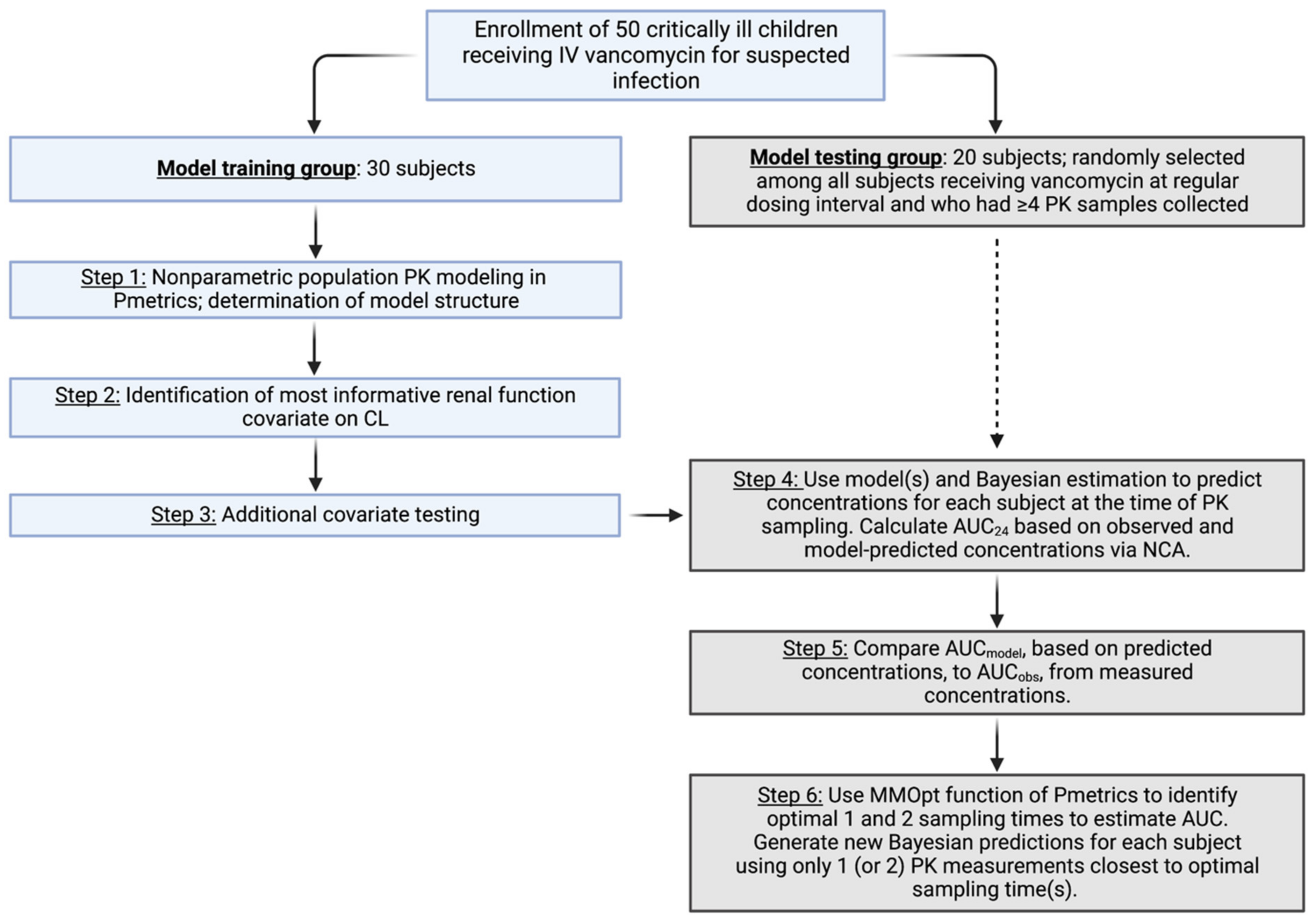
2.3. Population PK Model Training
2.4. Model Testing via Area under the Curve Comparisons
2.5. Area under the Curve Estimation from Optimal Sampling
3. Results
3.1. Study Population
3.2. Population PK Model Training
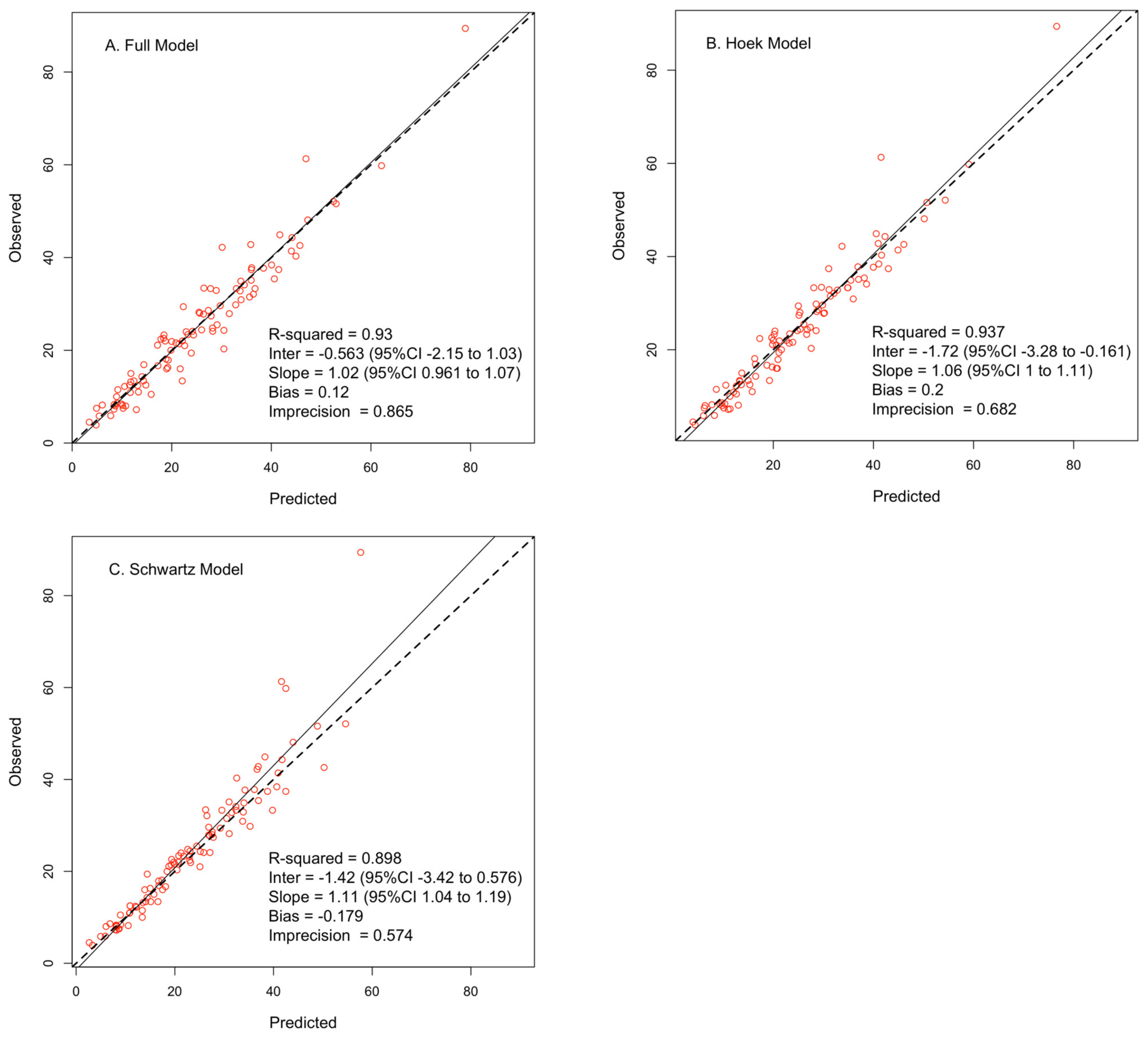
3.3. Area under the Curve Comparisons
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Weiss, S.L.; Fitzgerald, J.C.; Pappachan, J.; Wheeler, D.; Jaramillo-Bustamante, J.C.; Salloo, A.; Singhi, S.C.; Erickson, S.; Roy, J.A.; Bush, J.L.; et al. Global epidemiology of pediatric severe sepsis: The sepsis prevalence, outcomes, and therapies study. Am. J. Respir. Crit. Care Med. 2015, 191, 1147–1157. [Google Scholar] [CrossRef] [PubMed]
- Moise-Broder, P.A.; Forrest, A.; Birmingham, M.C.; Schentag, J.J. Pharmacodynamics of vancomycin and other antimicrobials in patients with Staphylococcus aureus lower respiratory tract infections. Clin. Pharmacokinet. 2004, 43, 925–942. [Google Scholar] [CrossRef]
- Kullar, R.; Davis, S.L.; Levine, D.P.; Rybak, M.J. Impact of vancomycin exposure on outcomes in patients with methicillin-resistant Staphylococcus aureus bacteremia: Support for consensus guidelines suggested targets. Clin. Infect. Dis. 2011, 52, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Song, K.H.; Kim, H.B.; Kim, H.S.; Lee, M.J.; Jung, Y.; Kim, G.; Hwang, J.H.; Kim, N.H.; Kim, M.; Kim, C.J.; et al. Impact of area under the concentration-time curve to minimum inhibitory concentration ratio on vancomycin treatment outcomes in methicillin-resistant Staphylococcus aureus bacteraemia. Int. J. Antimicrob. Agents 2015, 46, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.; Song, K.H.; Cho, J.; Kim, H.S.; Kim, N.H.; Kim, T.S.; Choe, P.G.; Chung, J.Y.; Park, W.B.; Bang, J.H.; et al. Area under the concentration-time curve to minimum inhibitory concentration ratio as a predictor of vancomycin treatment outcome in methicillin-resistant Staphylococcus aureus bacteraemia. Int. J. Antimicrob. Agents 2014, 43, 179–183. [Google Scholar] [CrossRef]
- Le, J.; Ny, P.; Capparelli, E.; Lane, J.; Ngu, B.; Muus, R.; Romanowski, G.; Vo, T.; Bradley, J. Pharmacodynamic Characteristics of Nephrotoxicity Associated with Vancomycin Use in Children. J. Pediatr. Infect. Dis. Soc. 2015, 4, e109–e116. [Google Scholar] [CrossRef]
- Rybak, M.J.; Lomaestro, B.M.; Rotscahfer, J.C.; Moellering, R.C., Jr.; Craig, W.A.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Vancomycin Therapeutic Guidelines: A Summary of Consensus Recommendations from the Infectious Diseases Society of America, the American Society of Health-System Pharmacists, and the Society of Infectious Diseases Pharmacists. Clin. Infect. Dis. 2009, 49, 325–327. [Google Scholar] [CrossRef]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am. J. Health Syst. Pharm. 2020, 77, 835–864. [Google Scholar]
- Gyssens, I.C. Glycopeptides. In Fundamentals of Antimicrobial Pharmacokinetics and Pharmacodynamics; Vinks, A.A., Derendorf, H., Mouton, J.W., Eds.; Springer: New York, NY, USA, 2014; Volume 1, pp. 279–322. [Google Scholar]
- Fuchs, T.C.; Hewitt, P. Biomarkers for drug-induced renal damage and nephrotoxicity-an overview for applied toxicology. AAPS J. 2011, 13, 615–631. [Google Scholar] [CrossRef]
- Schwartz, G.J.; Munoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New equations to estimate GFR in children with CKD. J. Am. Soc. Nephrol. 2009, 20, 629–637. [Google Scholar] [CrossRef]
- Mussap, M.; Plebani, M. Biochemistry and clinical role of human cystatin C. Crit. Rev. Clin. Lab. Sci. 2004, 41, 467–550. [Google Scholar] [CrossRef]
- Roos, J.F.; Doust, J.; Tett, S.E.; Kirkpatrick, C.M. Diagnostic accuracy of cystatin C compared to serum creatinine for the estimation of renal dysfunction in adults and children—A meta-analysis. Clin. Biochem. 2007, 40, 383–391. [Google Scholar] [CrossRef]
- Larsson, A.; Malm, J.; Grubb, A.; Hansson, L.O. Calculation of glomerular filtration rate expressed in mL/min from plasma cystatin C values in mg/L. Scand. J. Clin. Lab. Investig. 2004, 64, 25–30. [Google Scholar] [CrossRef]
- Ataei, N.; Bazargani, B.; Ameli, S.; Madani, A.; Javadilarijani, F.; Moghtaderi, M.; Abbasi, A.; Shams, S.; Ataei, F. Early detection of acute kidney injury by serum cystatin C in critically ill children. Pediatr. Nephrol. 2014, 29, 133–138. [Google Scholar] [CrossRef]
- Asilioglu, N.; Acikgoz, Y.; Paksu, M.S.; Gunaydin, M.; Ozkaya, O. Is serum cystatin C a better marker than serum creatinine for monitoring renal function in pediatric intensive care unit? J. Trop. Pediatr. 2012, 58, 429–434. [Google Scholar] [CrossRef]
- Di Nardo, M.; Ficarella, A.; Ricci, Z.; Luciano, R.; Stoppa, F.; Picardo, S.; Picca, S.; Muraca, M.; Cogo, P. Impact of severe sepsis on serum and urinary biomarkers of acute kidney injury in critically ill children: An observational study. Blood Purif. 2013, 35, 172–176. [Google Scholar] [CrossRef]
- Herrero-Morin, J.D.; Malaga, S.; Fernandez, N.; Rey, C.; Dieguez, M.A.; Solis, G.; Concha, A.; Medina, A. Cystatin C and beta2-microglobulin: Markers of glomerular filtration in critically ill children. Crit. Care 2007, 11, R59. [Google Scholar] [CrossRef]
- McCaffrey, J.; Coupes, B.; Chaloner, C.; Webb, N.J.; Barber, R.; Lennon, R. Towards a biomarker panel for the assessment of AKI in children receiving intensive care. Pediatr. Nephrol. 2015, 30, 1861–1871. [Google Scholar] [CrossRef]
- Downes, K.J.; Zane, N.R.; Zuppa, A.F. Effect of Cystatin C on Vancomycin Clearance Estimation in Critically Ill Children Using a Population Pharmacokinetic Modeling Approach. Ther. Drug Monit. 2020, 42, 848–855. [Google Scholar] [CrossRef]
- Wheeler, D.S.; Devarajan, P.; Ma, Q.; Harmon, K.; Monaco, M.; Cvijanovich, N.; Wong, H.R. Serum neutrophil gelatinase-associated lipocalin (NGAL) as a marker of acute kidney injury in critically ill children with septic shock. Crit. Care Med. 2008, 36, 1297–1303. [Google Scholar] [CrossRef]
- Haase, M.; Bellomo, R.; Devarajan, P.; Schlattmann, P.; Haase-Fielitz, A.; Group, N.M.-a.I. Accuracy of neutrophil gelatinase-associated lipocalin (NGAL) in diagnosis and prognosis in acute kidney injury: A systematic review and meta-analysis. Am. J. Kidney Dis. 2009, 54, 1012–1024. [Google Scholar] [PubMed]
- Kim, H.; Hur, M.; Cruz, D.N.; Moon, H.W.; Yun, Y.M. Plasma neutrophil gelatinase-associated lipocalin as a biomarker for acute kidney injury in critically ill patients with suspected sepsis. Clin. Biochem. 2013, 46, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Sampaio de Souza Garms, D.; Cardoso Eid, K.Z.; Burdmann, E.A.; Marcal, L.J.; Antonangelo, L.; Dos Santos, A.; Ponce, D. The Role of Urinary Biomarkers as Diagnostic and Prognostic Predictors of Acute Kidney Injury Associated with Vancomycin. Front. Pharmacol. 2021, 12, 705636. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, N.J.; Prozialeck, W.C.; Lodise, T.P.; Venkatesan, N.; O’Donnell, J.N.; Pais, G.; Cluff, C.; Lamar, P.C.; Neely, M.N.; Gulati, A.; et al. Evaluation of Vancomycin Exposures Associated with Elevations in Novel Urinary Biomarkers of Acute Kidney Injury in Vancomycin-Treated Rats. Antimicrob. Agents Chemother. 2016, 60, 5742–5751. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T.C.; Frick, K.; Emde, B.; Czasch, S.; von Landenberg, F.; Hewitt, P. Evaluation of novel acute urinary rat kidney toxicity biomarker for subacute toxicity studies in preclinical trials. Toxicol. Pathol. 2012, 40, 1031–1048. [Google Scholar] [CrossRef]
- Pais, G.M.; Avedissian, S.N.; O’Donnell, J.N.; Rhodes, N.J.; Lodise, T.P.; Prozialeck, W.C.; Lamar, P.C.; Cluff, C.; Gulati, A.; Fitzgerald, J.C.; et al. Comparative Performance of Urinary Biomarkers for Vancomycin-Induced Kidney Injury According to Timeline of Injury. Antimicrob. Agents Chemother. 2019, 63. [Google Scholar] [CrossRef]
- Neely, M.N.; van Guilder, M.G.; Yamada, W.M.; Schumitzky, A.; Jelliffe, R.W. Accurate detection of outliers and subpopulations with Pmetrics, a nonparametric and parametric pharmacometric modeling and simulation package for R. Ther. Drug Monit. 2012, 34, 467–476. [Google Scholar] [CrossRef]
- R Foundation for Statistical Computing Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- RStudio. RStudio: Integrated Development Environment for R; RStudio, Inc.: Boston, MA, USA, 2019. [Google Scholar]
- Yamada, W.M.; Neely, M.N.; Bartroff, J.; Bayard, D.S.; Burke, J.V.; Guilder, M.V.; Jelliffe, R.W.; Kryshchenko, A.; Leary, R.; Tatarinova, T.; et al. An Algorithm for Nonparametric Estimation of a Multivariate Mixing Distribution with Applications to Population Pharmacokinetics. Pharmaceutics 2020, 13, 42. [Google Scholar] [CrossRef]
- Hoek, F.J.; Kemperman, F.A.; Krediet, R.T. A comparison between cystatin C, plasma creatinine and the Cockcroft and Gault formula for the estimation of glomerular filtration rate. Nephrol. Dial. Transplant. 2003, 18, 2024–2031. [Google Scholar] [CrossRef]
- Pottel, H.; Delanaye, P.; Schaeffner, E.; Dubourg, L.; Eriksen, B.O.; Melsom, T.; Lamb, E.J.; Rule, A.D.; Turner, S.T.; Glassock, R.J.; et al. Estimating glomerular filtration rate for the full age spectrum from serum creatinine and cystatin C. Nephrol. Dial. Transplant. 2017, 32, 497–507. [Google Scholar] [CrossRef]
- Chen, I.H.; Nicolau, D.P. Augmented Renal Clearance and How to Augment Antibiotic Dosing. Antibiotics 2020, 9, 393. [Google Scholar] [CrossRef]
- Straney, L.; Clements, A.; Parslow, R.C.; Pearson, G.; Shann, F.; Alexander, J.; Slater, A.; ANZICS Paediatric Study Group; Paediatric Intensive Care Audit Network. Paediatric Index of Mortality 3: An Updated Model for Predicting Mortality in Pediatric Intensive Care. Pediatr. Crit. Care Med. 2013, 14, 673–681. [Google Scholar] [CrossRef]
- Back, H.M.; Lee, J.B.; Han, N.; Goo, S.; Jung, E.; Kim, J.; Song, B.; An, S.H.; Kim, J.T.; Rhie, S.J.; et al. Application of Size and Maturation Functions to Population Pharmacokinetic Modeling of Pediatric Patients. Pharmaceutics 2019, 11, 259. [Google Scholar] [CrossRef]
- Rowland, M.; Tozer, T.N. Appendix A: Assessment of Area. In Clinical Pharmacokinetics: Concepts and Applications, 2nd ed.; Lea & Febiger: Malvern, PA, USA, 1989. [Google Scholar]
- Bayard, D.S.; Neely, M. Experiment design for nonparametric models based on minimizing Bayes Risk: Application to voriconazole. J. Pharm. Pharm. 2017, 44, 95–111. [Google Scholar] [CrossRef]
- Oh, Y.; Park, S.; Park, E.; Lee, J.; Lee, H.; Kim, J.; Cho, J. Correlation between vancomycin clearance and cystatin C-based glomerular filtration rate in paediatric patients. Br. J. Clin. Pharmacol. 2021, 87, 3190–3196. [Google Scholar] [CrossRef]
- Hasson, D.; Menon, S.; Gist, K.M. Improving acute kidney injury diagnostic precision using biomarkers. Pract. Lab. Med. 2022, 30, e00272. [Google Scholar] [CrossRef]
- Hirai, K.; Ishii, H.; Shimoshikiryo, T.; Shimomura, T.; Tsuji, D.; Inoue, K.; Kadoiri, T.; Itoh, K. Augmented Renal Clearance in Patients with Febrile Neutropenia is Associated with Increased Risk for Subtherapeutic Concentrations of Vancomycin. Ther. Drug Monit. 2016, 38, 706–710. [Google Scholar] [CrossRef]
- Goutelle, S.; Woillard, J.B.; Neely, M.; Yamada, W.; Bourguignon, L. Nonparametric Methods in Population Pharmacokinetics. J. Clin. Pharmacol. 2022, 62, 142–157. [Google Scholar] [CrossRef]
- Leroux, S.; Biran, V.; van den Anker, J.; Gotta, V.; Zhao, W.; Zhang, D.; Jacqz-Aigrain, E.; Pfister, M. Serum Creatinine and Serum Cystatin C are Both Relevant Renal Markers to Estimate Vancomycin Clearance in Critically Ill Neonates. Front. Pharmacol. 2021, 12, 634686. [Google Scholar] [CrossRef]
- Thomas, S.N.; Stieglitz, H.M.; Hackenmueller, S.; Suh-Lailam, B.; Pyle-Eilola, A.L. Use of Cotton Balls in Diapers for Collection of Urine Samples Impacts the Analysis of Routine Chemistry Tests: An Evaluation of Cotton Balls, Diapers, and Chemistry Analyzers. J. Pediatr. 2022, 245, 179–183.e8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Model Training Group (n = 30) | Model Testing Group (n = 20) | p-Value a |
|---|---|---|---|
| At start of vancomycin | |||
| Age in years, median (IQR) | 9.8 (3.8–11.2) | 10.2 (2.9–13.2) | 0.68 |
| Weight in kg, median (IQR) | 25.9 (13.9–41.8) | 37.6 (14.4–57.5) | 0.33 |
| Female sex, n (%) | 11 (37) | 5 (25) | 0.54 |
| Serum creatinine in mg/dL, median (IQR) | 0.40 (0.23–0.60) | 0.40 (0.19–0.43) | 0.22 |
| eGFRSchwartz in mL/min/1.73 m2, median (IQR) | 117 (97–154) | 154 (126–185) | 0.06 |
| Receipt of vasopressors, n (%) | 18 (60) | 6 (30) | 0.05 |
| Vancomycin dose in mg/kg/dose, median (IQR) | 14.7 (11.9–15.0) | 14.5 (11.8–14.8) | 0.60 |
| At PK sampling | |||
| Serum creatinine in mg/dL, median (IQR) | 0.30 (0.20–0.48) | 0.35 (0.19–0.50) | 0.92 |
| eGFRSchwartz in mL/min/1.73 m2, median (IQR) | 164 (114–222) | 156 (134–184) | 0.95 |
| eGFRHoek in mL/min/1.73 m2, median (IQR) | 143 (110–197) | 130 (96–156) | 0.64 |
| Receipt of vasopressors, n (%) | 14 (47) | 7 (35) | 0.56 |
| PIM3 probability of death, median (IQR) | 1.3% (0.5–4.3) | 1.3% (0.4–4.1) | 0.96 |
| Vancomycin dose in mg/kg/dose, median (IQR) | 13.2 (10.0–14.8) | 15.0 (14.5–15.7) | 0.005 |
| Duration of vancomycin therapy prior to PK sampling (in hours), median (IQR) | 36.4 (30.8–41.4) | 36.1 (32.1–41.9) | 0.68 |
| Parameter | Weighted Parameter Estimate | CV% | Shrinkage % | |
|---|---|---|---|---|
| Median | 95th Percentile | |||
| CL0 | 3.31 | 2.53–4.22 | 39.5 | 54.7 |
| CLWT | 0.75 | - | - | |
| CLHOEK | 0.85 | 0.22–0.90 | 62.8 | 55.6 |
| CLNGAL | 0.94 | 0.86–1.00 | 10.9 | 50.5 |
| VC0 | 3.50 | 2.72–7.09 | 49.2 | 59.5 |
| VC-WT | 1 | - | - | |
| Q0 | 7.09 | 4.76–7.97 | 32.6 | 60.9 |
| QWT | 0.75 | - | - | |
| VP0 | 7.75 | 6.63–13.80 | 39.0 | 49.1 |
| VP-WT | 1 | - | - | |
| Full Model | Hoek Model | Schwartz Model | |
|---|---|---|---|
| All available PK samples | |||
| AUC24, median (range) | 475 (325–857) | 488 (338–907) | 501 (319–710) |
| Median bias b | 2.3% | 1.8% | −2.4% |
| Median imprecision c | 6.2% | 7.0% | 6.2% |
| Number of subjects with AUCmodel within 20% of AUCobs | 18 (90%) | 17 (85%) | 19 (95%) |
| Correlation between AUCmodel and AUCobs | 0.939 | 0.926 | 0.893 |
| Two optimally timed PK samples | |||
| AUC24, median (range) | 487 (316–968) | 482 (333–832) | 471 (332–714) |
| Median bias b | 2.0% | 1.8% | −1.2% |
| Median imprecision c | 13.4% | 6.0% | 6.8% |
| Number of subjects with AUCmodel within 20% of AUCobs | 15 (75%) | 18 (90%) | 17 (85%) |
| Correlation between AUCmodel and AUCobs | 0.876 | 0.928 | 0.860 |
| Single optimally timed PK sample | |||
| AUC24, median (range) | 526 (284–968) | 523 (283–830) | 466 (353–700) |
| Median bias b | 3.7% | 2.5% | −0.9% |
| Median imprecision c | 13.4% | 11.4% | 7.0% |
| Number of subjects with AUCmodel within 20% of AUCobs | 13 (65%) | 17 (85%) | 17 (85%) |
| Correlation between AUCmodel and AUCobs | 0.817 | 0.891 | 0.825 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Downes, K.J.; Zuppa, A.F.; Sharova, A.; Neely, M.N. Optimizing Vancomycin Therapy in Critically Ill Children: A Population Pharmacokinetics Study to Inform Vancomycin Area under the Curve Estimation Using Novel Biomarkers. Pharmaceutics 2023, 15, 1336. https://doi.org/10.3390/pharmaceutics15051336
Downes KJ, Zuppa AF, Sharova A, Neely MN. Optimizing Vancomycin Therapy in Critically Ill Children: A Population Pharmacokinetics Study to Inform Vancomycin Area under the Curve Estimation Using Novel Biomarkers. Pharmaceutics. 2023; 15(5):1336. https://doi.org/10.3390/pharmaceutics15051336
Chicago/Turabian StyleDownes, Kevin J., Athena F. Zuppa, Anna Sharova, and Michael N. Neely. 2023. "Optimizing Vancomycin Therapy in Critically Ill Children: A Population Pharmacokinetics Study to Inform Vancomycin Area under the Curve Estimation Using Novel Biomarkers" Pharmaceutics 15, no. 5: 1336. https://doi.org/10.3390/pharmaceutics15051336