

Local Delivery and Controlled Release Drugs Systems: A New Approach for the Clinical Treatment of Periodontitis Therapy

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
3. Drug Delivery System
4. LDDS and Periodontal Treatment
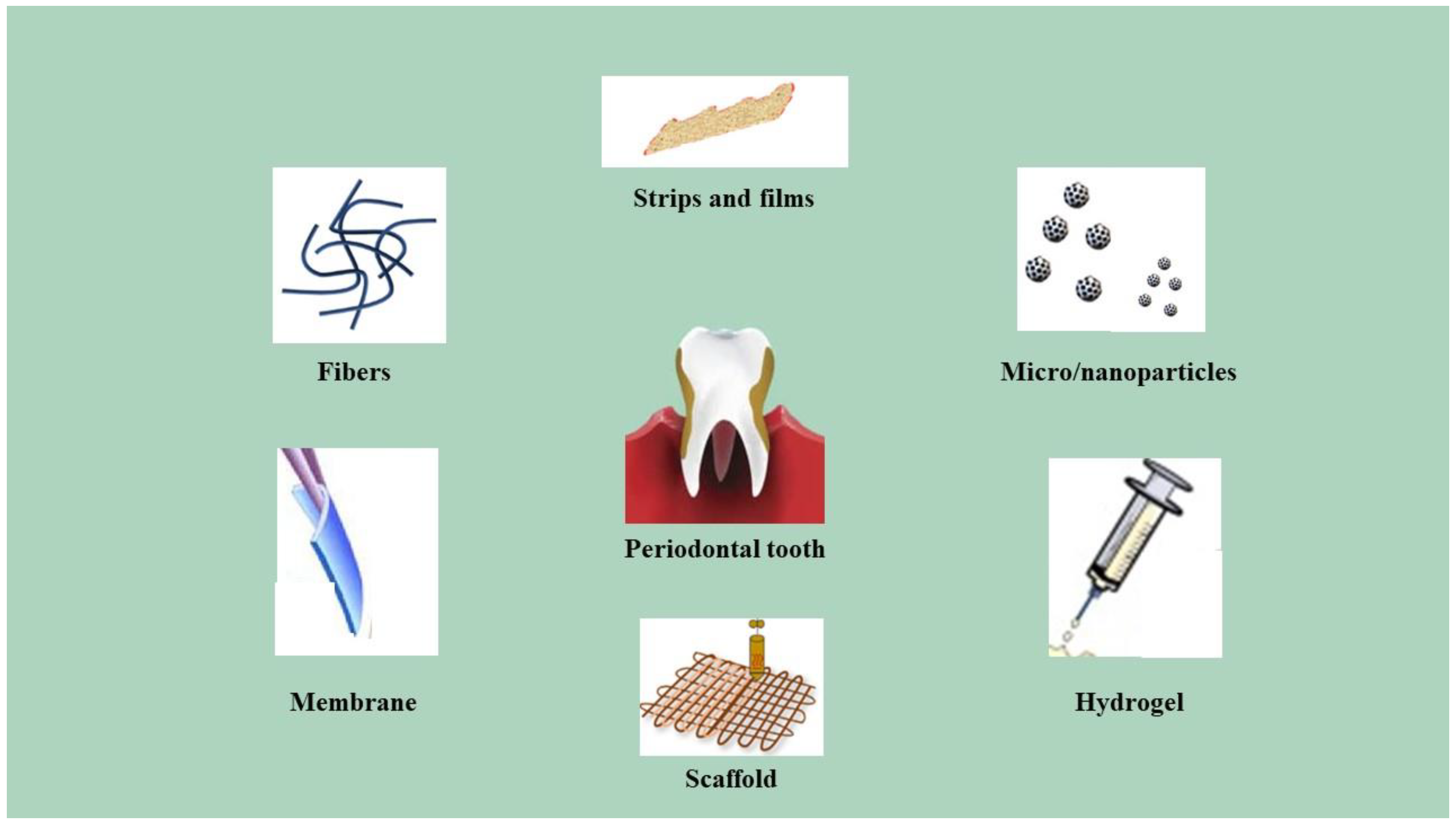
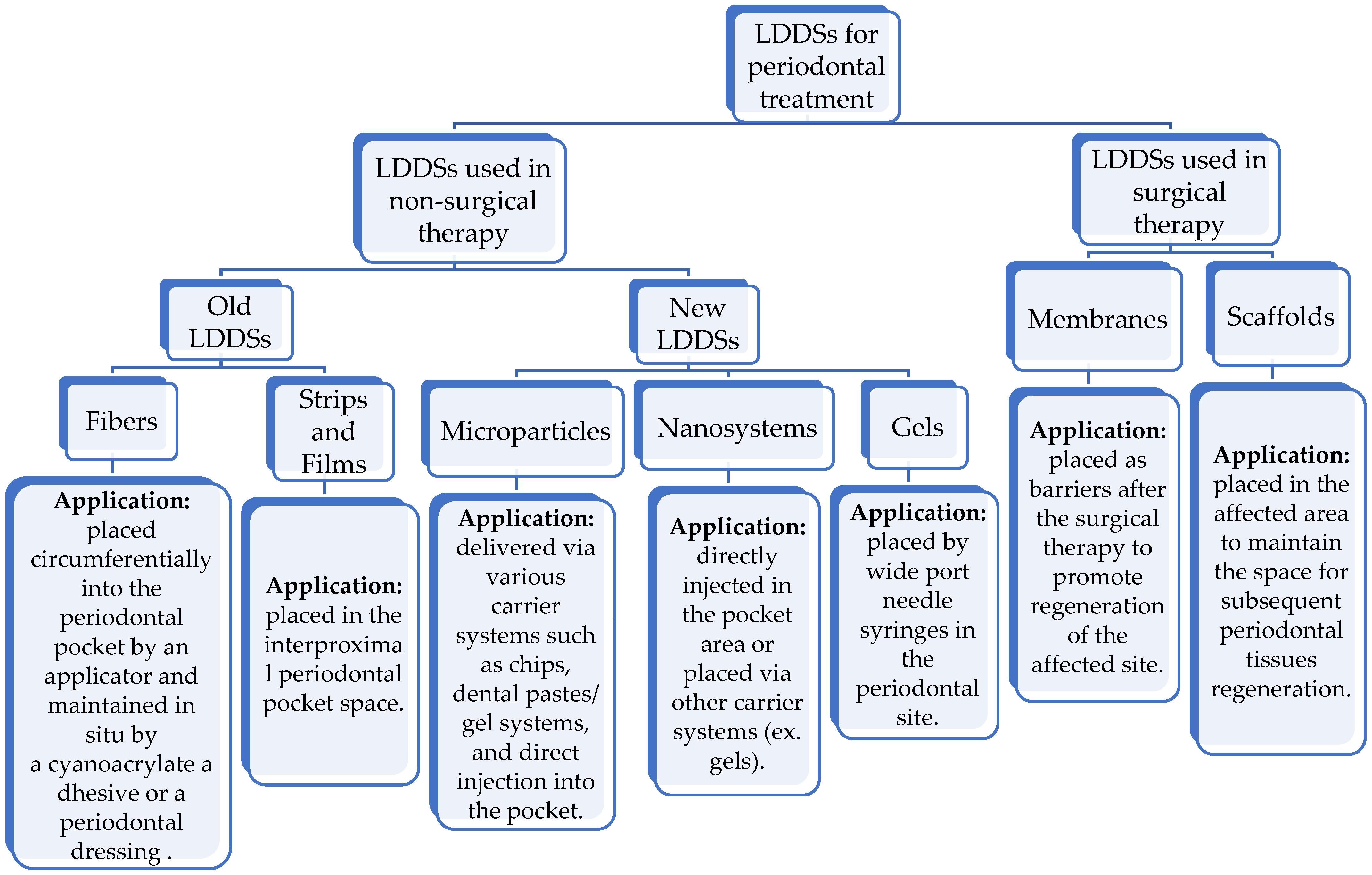
5. Types of LDDSs in Periodontitis Treatment
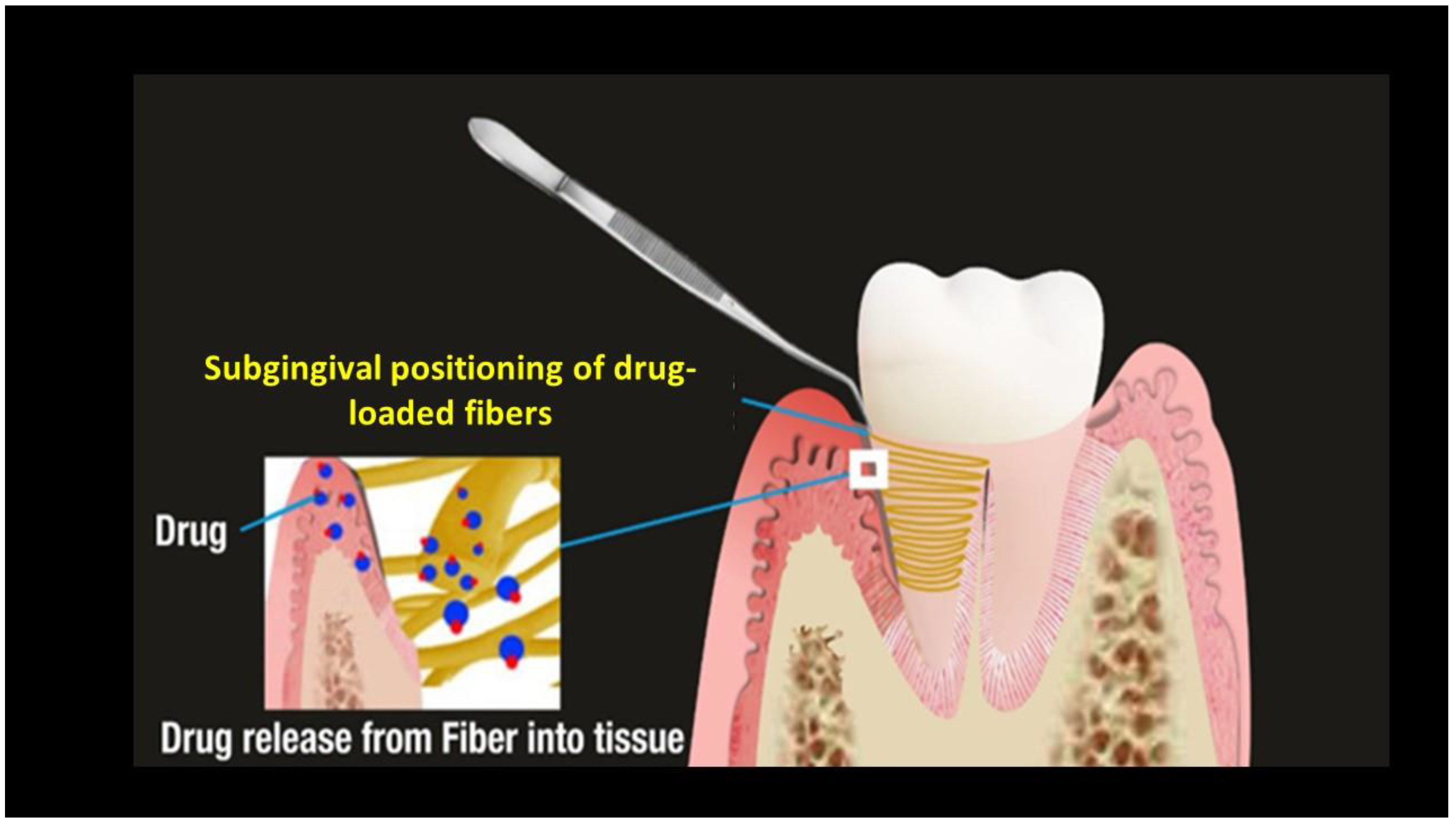
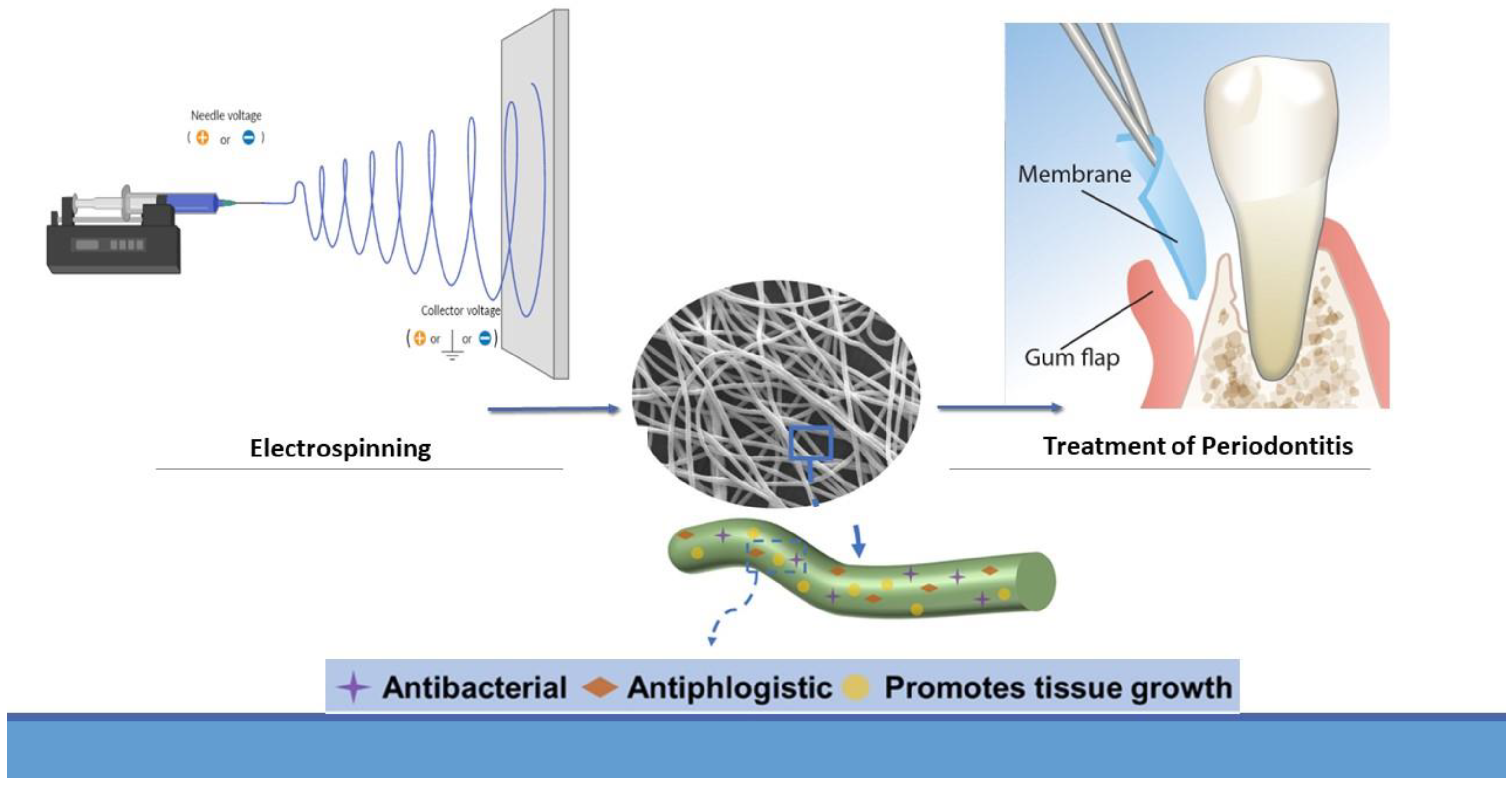
5.1. Fibers
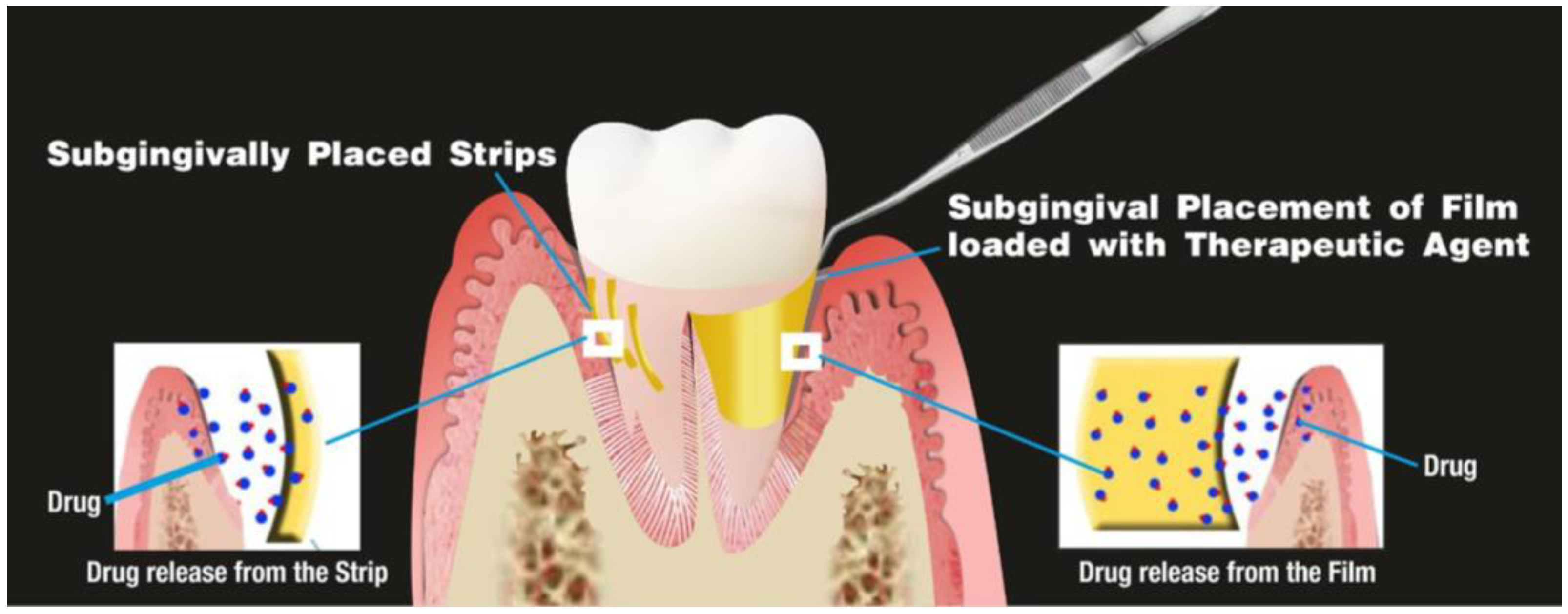
5.2. Strips and Films
5.3. Microparticles
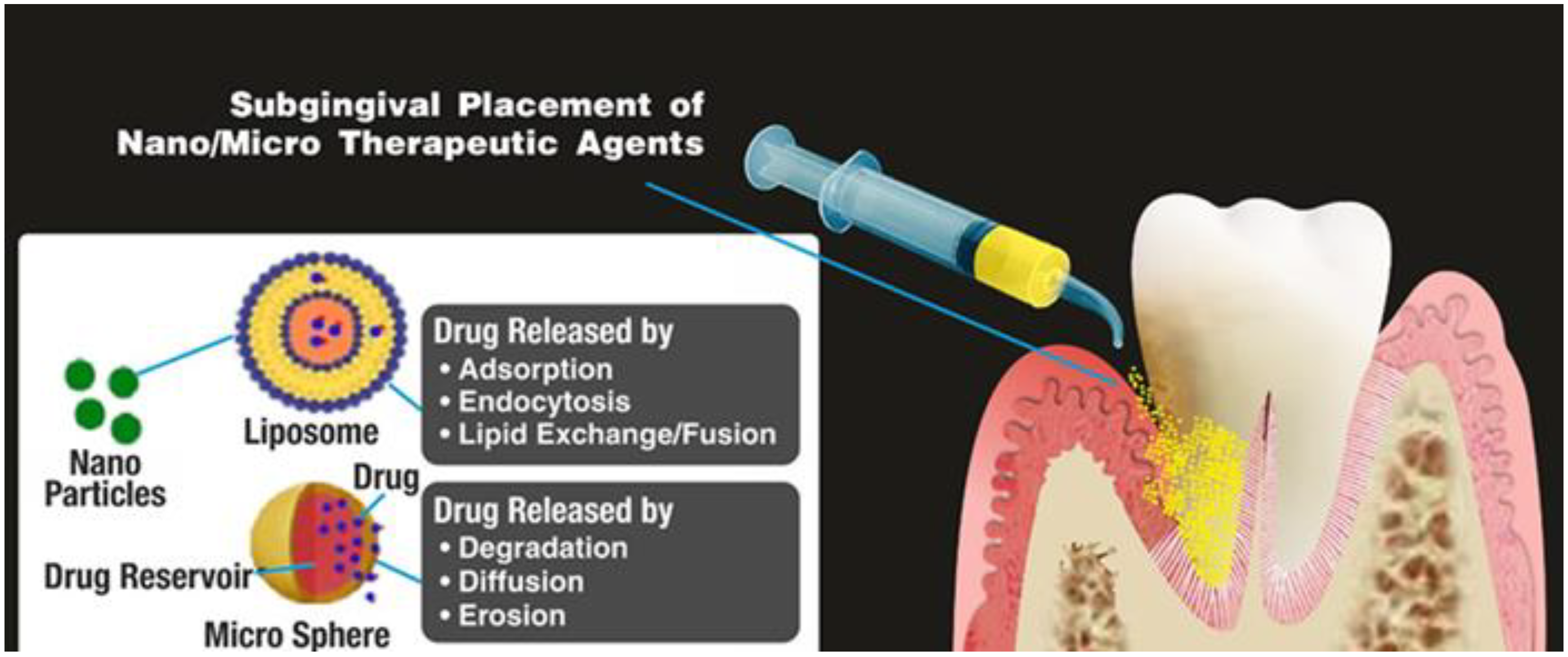
5.4. Nanosystems
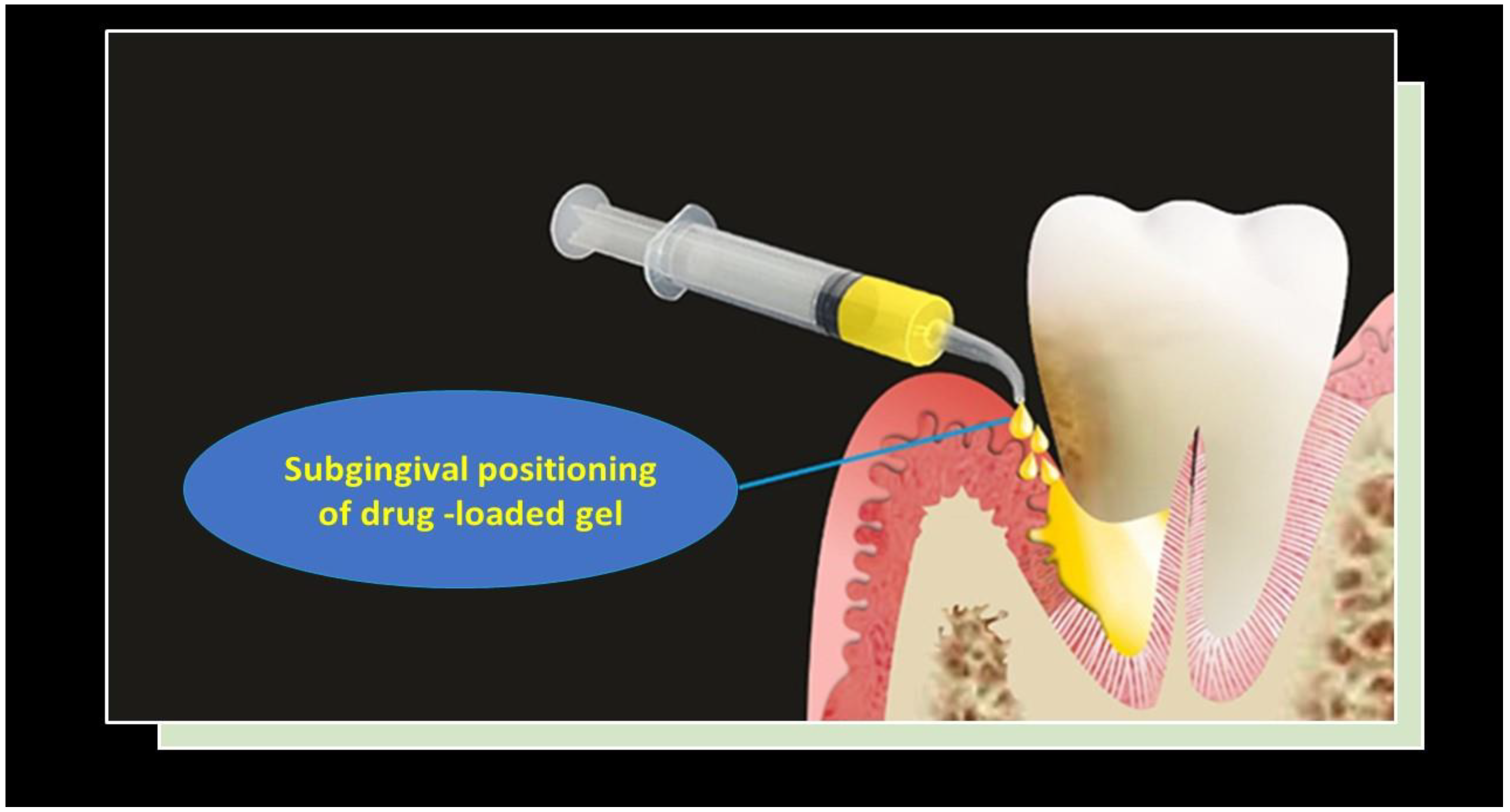
5.5. Gels
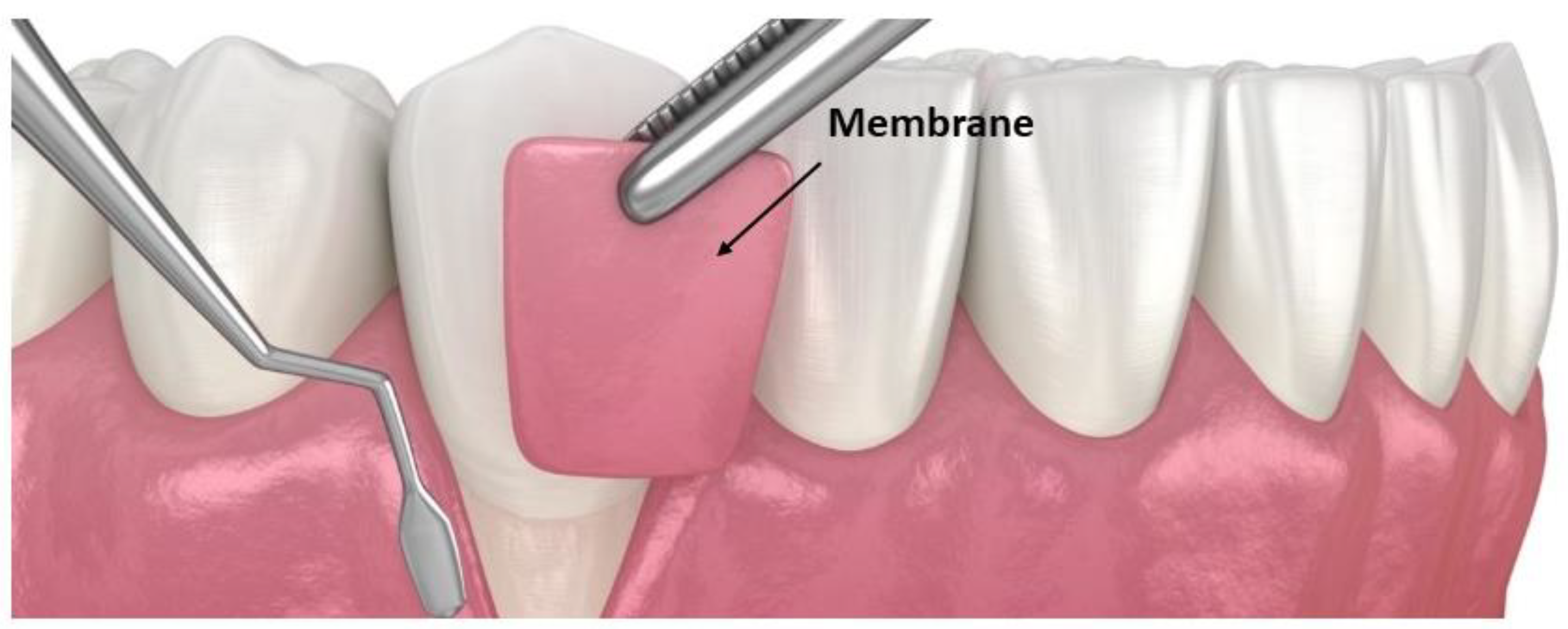
5.6. Membranes
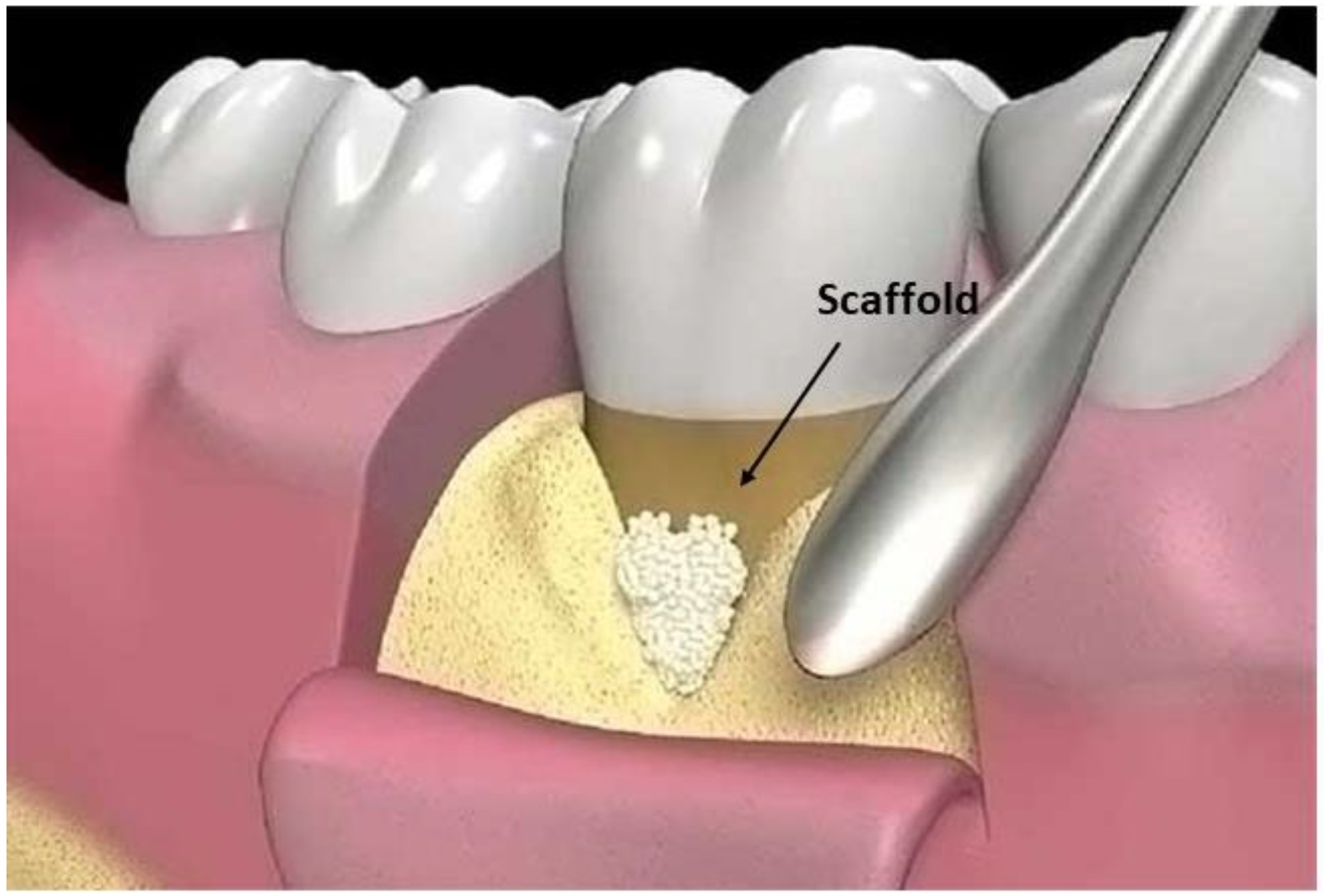
5.7. Scaffolds
6. LDDSs and Systemic Diseases in Periodontal Patients
7. New Perspectives
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Sanz, M.; Kebschull, M.; Jepsen, S.; Sculean, A.; Berglundh, T.; Papapanou, P.N.; Chapple, I.; Tonetti, M.S. Treatment of stage IV periodontitis: The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2022, 49 (Suppl. 24), 4–71. [Google Scholar] [CrossRef] [PubMed]
- Panwar, M.; Gupta, S.H. Local Drug Delivery with Tetracycline Fiber: An Alternative to Surgical Periodontal Therapy. Med. J. Armed Forces India 2009, 65, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Vijayalashmi, R.; Ravindranath, S.M.; Jayakumar, N.D.; Padmalatha; Vargheese, S.H.; Kumaraswamy, K.L. Kinetics of drug release from a biodegradable local drug delivery system and its effect on Porphyromonas gingivalis isolates: An in vitro study. J. Indian Soc. Periodontol. 2013, 17, 429–434. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Liu, S.; Li, Z.; Xu, J.; Liu, Y.; Luo, E. Coaxial TP/APR electrospun nanofibers for programmed controlling inflammation and promoting bone regeneration in periodontitis-related alveolar bone defect models. Mater. Today Bio. 2022, 16, 100438. [Google Scholar] [CrossRef]
- Deasy, P.B.; Collins, A.E.; MacCarthy, D.J.; Russell, R.J. Use of strips containing tetracycline hydrochloride or metronidazole for the treatment of advanced periodontal disease. J. Pharm. Pharmacol. 1989, 41, 694–699. [Google Scholar] [CrossRef]
- Steinberg, D.; Friedman, M.; Soskolne, A.; Sela, M.N. A new degradable controlled release device for treatment of periodontal disease: In vitro release study. J. Periodontol. 1990, 61, 393–398. [Google Scholar] [CrossRef]
- Wu, L.; Chen, W.; Li, F.; Morrow, B.R.; Garcia-Godoy, F.; Hong, L. Sustained Release of Minocycline from Minocycline-Calcium-Dextran Sulfate Complex Microparticles for Periodontitis Treatment. J. Pharm. Sci. 2018, 107, 3134–3142. [Google Scholar] [CrossRef]
- Pichayakorn, W.; Boonme, P. Evaluation of cross-linked chitosan microparticles containing metronidazole for periodontitis treatment. Mater. Sci. Eng. C Mater. Biol. Appl. 2013, 33, 1197–1202. [Google Scholar] [CrossRef]
- Xu, S.; Zhou, Q.; Jiang, Z.; Wang, Y.; Yang, K.; Qiu, X.; Ji, Q. The effect of doxycycline-containing chitosan/carboxymethyl chitosan nanoparticles on NLRP3 inflammasome in periodontal disease. Carbohydr. Polym. 2020, 237, 116163. [Google Scholar] [CrossRef]
- Mou, J.; Liu, Z.; Liu, J.; Lu, J.; Zhu, W.; Pei, D. Hydrogel containing minocycline and zinc oxide-loaded serum albumin nanopartical for periodontitis application: Preparation, characterization and evaluation. Drug Deliv. 2019, 26, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Khorshidi, S.; Solouk, A.; Mirzadeh, H.; Mazinani, S.; Lagaron, J.M.; Sharifi, S.; Ramakrishna, S. A review of key challenges of electrospun scaffolds for tissue-engineering applications. J. Tissue Eng. Regen. Med. 2016, 10, 715–738. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, L.; Wang, Z.; Zheng, G.; Chen, Q.; Luo, E. Application of Electrospinning Strategy on Cartilage Tissue Engineering. Curr. Stem Cell Res. Ther. 2018, 13, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Kouidhi, B.; Al Qurashi, Y.M.; Chaieb, K. Drug resistance of bacterial dental biofilm and the potential use of natural compounds as alternative for prevention and treatment. Microb. Pathog. 2015, 80, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Lagha, A.B.; Grenier, D. Tea polyphenols protect gingival keratinocytes against TNF-α-induced tight junction barrier dysfunction and attenuate the inflammatory response of monocytes/macrophages. Cytokine 2019, 115, 64–75. [Google Scholar] [CrossRef]
- Joshi, D.; Garg, T.; Goyal, A.K.; Rath, G. Advanced drug delivery approaches against periodontitis. Drug Deliv. 2016, 23, 363–377. [Google Scholar] [CrossRef]
- Esposito, E.; Cortesi, R.; Cervellati, F.; Menegatti, E.; Nastruzzi, C. Biodegradable microparticles for sustained delivery of tetracycline to the periodontal pocket: Formulatory and drug release studies. J. Microencapsul. 1997, 14, 175–187. [Google Scholar] [CrossRef]
- Moreira, A.L.; Novaes, A.B., Jr.; Grisi, M.F.; Taba, M., Jr.; Souza, S.L.; Palioto, D.B.; de Oliveira, P.G.; Casati, M.Z.; Casarin, R.C.; Messora, M.R. Antimicrobial photodynamic therapy as an adjunct to non-surgical treatment of aggressive periodontitis: A split-mouth randomized controlled trial. J. Periodontol. 2015, 86, 376–386. [Google Scholar] [CrossRef]
- Zazo, H.; Colino, C.I.; Lanao, J.M. Current applications of nanoparticles in infectious diseases. J. Control. Release 2016, 224, 86–102. [Google Scholar] [CrossRef]
- Shahzad, M.; Millhouse, E.; Culshaw, S.; Edwards, C.A.; Ramage, G.; Combet, E. Selected dietary (poly)phenols inhibit periodontal pathogen growth and biofilm formation. Food Funct. 2015, 6, 719–729. [Google Scholar] [CrossRef]
- Işılay Özdoğan, A.; Akca, G.; Şenel, S. Development and in vitro evaluation of chitosan based system for local delivery of atorvastatin for treatment of periodontitis. Eur. J. Pharm. Sci. 2018, 124, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.; Ahmad, F.J.; Bedi, S.; Sharma, S.; Umar, S.; Ansari, M.A. A novel Nanoformulation Development of Eugenol and their treatment in inflammation and periodontitis. Saudi Pharm. J. 2019, 27, 778–790. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Shao, J.; Jansen, J.A.; Walboomers, X.F.; Yang, F. A Novel Thermoresponsive Gel as a Potential Delivery System for Lipoxin. J. Dent. Res. 2019, 98, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Luo, W.; Ng, T.W.; Leung, P.C.; Zhang, C.; Leung, K.C.; Jin, L. Nanoparticle-encapsulated baicalein markedly modulates pro-inflammatory response in gingival epithelial cells. Nanoscale 2017, 9, 12897–12907. [Google Scholar] [CrossRef]
- Xu, X.; Gu, Z.; Chen, X.; Shi, C.; Liu, C.; Liu, M.; Wang, L.; Sun, M.; Zhang, K.; Liu, Q.; et al. An injectable and thermosensitive hydrogel: Promoting periodontal regeneration by controlled-release of aspirin and erythropoietin. Acta Biomater. 2019, 86, 235–246. [Google Scholar] [CrossRef]
- Gunjiganur Vemanaradhya, G.; Emani, S.; Mehta, D.S.; Bhandari, S. Effect of 1.2% of simvastatin gel as a local drug delivery system on Gingival Crevicular Fluid interleukin-6 & interleukin-8 levels in non surgical treatment of chronic periodontitis patients. Arch. Oral Biol. 2017, 82, 55–61. [Google Scholar] [CrossRef]
- Soni, A.; Raj, S.; Kashyap, L.; Upadhyay, A.; Agrahari, V.C.; Sharma, A. Comparative effect of 1.2% atorvastatin gel and 1.2% rosuvastatin as a local drug delivery in treatment of intra-bony defects in chronic periodontitis. Indian J. Dent. Res. 2022, 33, 180–183. [Google Scholar] [CrossRef]
- Manjunatha, V.A.; Vemanaradhya, G.G.; Gowda, T.M. Clinical and antioxidant efficacy of 4% mangosteen gel as a local drug delivery in the treatment of chronic periodontitis: A placebo-controlled, split-mouth trial. Dent. Med. Probl. 2022, 59, 111–119. [Google Scholar] [CrossRef]
- Nyman, S.; Lindhe, J.; Karring, T.; Rylander, H. New attachment following surgical treatment of human periodontal disease. J. Clin. Periodontol. 1982, 9, 290–296. [Google Scholar] [CrossRef]
- Sheikh, Z.; Qureshi, J.; Alshahrani, A.M.; Nassar, H.; Ikeda, Y.; Glogauer, M.; Ganss, B. Collagen based barrier membranes for periodontal guided bone regeneration applications. Odontology 2017, 105, 1–12. [Google Scholar] [CrossRef]
- Wei, Y.; Deng, Y.; Ma, S.; Ran, M.; Jia, Y.; Meng, J.; Han, F.; Gou, J.; Yin, T.; He, H.; et al. Local drug delivery systems as therapeutic strategies against periodontitis: A systematic review. J. Control. Release 2021, 333, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Rajeshwari, H.R.; Dhamecha, D.; Jagwani, S.; Rao, M.; Jadhav, K.; Shaikh, S.; Puzhankara, L.; Jalalpure, S. Local drug delivery systems in the management of periodontitis: A scientific review. J. Control. Release 2019, 307, 393–409. [Google Scholar] [CrossRef]
- Qasim, S.S.B.; Nogueria, L.P.; Fawzy, A.S.; Daood, U. The Effect of Cross-linking Efficiency of Drug-Loaded Novel Freeze Gelated Chitosan Templates for Periodontal Tissue Regeneration. AAPS PharmSciTech 2020, 21, 173. [Google Scholar] [CrossRef]
- Liao, Y.; Li, H.; Shu, R.; Chen, H.; Zhao, L.; Song, Z.; Zhou, W. Mesoporous Hydroxyapatite/Chitosan Loaded with Recombinant-Human Amelogenin Could Enhance Antibacterial Effect and Promote Periodontal Regeneration. Front. Cell Infect. Microbiol. 2020, 10, 180. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; Santonocito, S.; Viglianisi, G.; Tatullo, M.; Isola, G. Impact of Oral Mesenchymal Stem Cells Applications as a Promising Therapeutic Target in the Therapy of Periodontal Disease. Int. J. Mol. Sci. 2022, 23, 13419. [Google Scholar] [CrossRef]
- Baba, S.; Yamada, Y.; Komuro, A.; Yotsui, Y.; Umeda, M.; Shimuzutani, K.; Nakamura, S. Phase I/II Trial of Autologous Bone Marrow Stem Cell Transplantation with a Three-Dimensional Woven-Fabric Scaffold for Periodontitis. Stem Cells Int. 2016, 2016, 6205910. [Google Scholar] [CrossRef]
- Takewaki, M.; Kajiya, M.; Takeda, K.; Sasaki, S.; Motoike, S.; Komatsu, N.; Matsuda, S.; Ouhara, K.; Mizuno, N.; Fujita, T.; et al. MSC/ECM Cellular Complexes Induce Periodontal Tissue Regeneration. J. Dent. Res. 2017, 96, 984–991. [Google Scholar] [CrossRef]
- Singh Malik, D.; Mital, N.; Kaur, G. Topical drug delivery systems: A patent review. Expert Opin. Ther. Pat. 2016, 26, 213–228. [Google Scholar] [CrossRef]
- Higashi, K.; Matsushita, M.; Morisaki, K.; Hayashi, S.; Mayumi, T. Local drug delivery systems for the treatment of periodontal disease. J. Pharmacobiodyn. 1991, 14, 72–81. [Google Scholar] [CrossRef]
- Finkelstein, A.; McClean, D.; Kar, S.; Takizawa, K.; Varghese, K.; Baek, N.; Park, K.; Fishbein, M.C.; Makkar, R.; Litvack, F.; et al. Local drug delivery via a coronary stent with programmable release pharmacokinetics. Circulation 2003, 107, 777–784. [Google Scholar] [CrossRef]
- Böhme, D.; Beck-Sickinger, A.G. Drug delivery and release systems for targeted tumor therapy. J. Pept. Sci. 2015, 21, 186–200. [Google Scholar] [CrossRef]
- Zhu, Y.S.; Tang, K.; Lv, J. Peptide-drug conjugate-based novel molecular drug delivery system in cancer. Trends Pharmacol. Sci. 2021, 42, 857–869. [Google Scholar] [CrossRef]
- Qamar, Z.; Qizilbash, F.F.; Iqubal, M.K.; Ali, A.; Narang, J.K.; Ali, J.; Baboota, S. Nano-Based Drug Delivery System: Recent Strategies for the Treatment of Ocular Disease and Future Perspective. Recent Pat. Drug Deliv. Formul. 2019, 13, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Sohail, M.; Guo, W.; Li, Z.; Xu, H.; Zhao, F.; Chen, D.; Fu, F. Nanocarrier-based Drug Delivery System for Cancer Therapeutics: A Review of the Last Decade. Curr. Med. Chem. 2021, 28, 3753–3772. [Google Scholar] [CrossRef] [PubMed]
- Adepu, S.; Ramakrishna, S. Controlled Drug Delivery Systems: Current Status and Future Directions. Molecules 2021, 26, 5905. [Google Scholar] [CrossRef] [PubMed]
- Kornman, K.S. Controlled-release local delivery antimicrobials in periodontics: Prospects for the future. J. Periodontol. 1993, 64, 782–791. [Google Scholar] [CrossRef]
- Goodson, J.M.; Haffajee, A.; Socransky, S.S. Periodontal therapy by local delivery of tetracycline. J. Clin. Periodontol. 1979, 6, 83–92. [Google Scholar] [CrossRef]
- Allen, T.M.; Cullis, P.R. Drug delivery systems: Entering the mainstream. Science 2004, 303, 1818–1822. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.K. Current status and future prospects of drug delivery systems. In Methods in Molecular Biology; Humana Press: New York, NY, USA, 2014; Volume 1141, pp. 1–56. [Google Scholar] [CrossRef]
- Fenton, O.S.; Olafson, K.N.; Pillai, P.S.; Mitchell, M.J.; Langer, R. Advances in Biomaterials for Drug Delivery. Adv. Mater. 2018, 30, e1705328. [Google Scholar] [CrossRef] [PubMed]
- Holborow, D.; Niederman, R.; Tonetti, M.; Cugini, M.; Goodson, J. Synergistic effects between chlorhexidine mouthwash and tetracycline fibers. J. Dent. Res. 1990, 69, 277. [Google Scholar]
- Goodson, J.M. Gingival crevice fluid flow. Periodontol. 2000 2003, 31, 43–54. [Google Scholar] [CrossRef]
- Addy, M.; Martin, M.V. Systemic antimicrobials in the treatment of chronic periodontal diseases: A dilemma. Oral Dis. 2003, 9 (Suppl. 1), 38–44. [Google Scholar] [CrossRef] [PubMed]
- el Kenawy, R.; Bowlin, G.L.; Mansfield, K.; Layman, J.; Simpson, D.G.; Sanders, E.H.; Wnek, G.E. Release of tetracycline hydrochloride from electrospun poly(ethylene-co-vinylacetate), poly(lactic acid), and a blend. J. Control. Release 2002, 81, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.F.; Carson, D.; Woodrow, K.A. Current strategies for sustaining drug release from electrospun nanofibers. J. Control. Release 2015, 220, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.; Cugini, M.A.; Goodson, J.M. Zero-order delivery with periodontal placement of tetracycline-loaded ethylene vinyl acetate fibers. J. Periodontal. Res. 1990, 25, 243–249. [Google Scholar] [CrossRef]
- Zhang, Y.; Sun, T.; Jiang, C. Biomacromolecules as carriers in drug delivery and tissue engineering. Acta Pharm. Sin. B 2018, 8, 34–50. [Google Scholar] [CrossRef]
- Kapoor, D.N.; Bhatia, A.; Kaur, R.; Sharma, R.; Kaur, G.; Dhawan, S. PLGA: A unique polymer for drug delivery. Ther. Deliv. 2015, 6, 41–58. [Google Scholar] [CrossRef]
- Chhina, S.; Rathore, A.S.; Juneja, S. Alpha-2-Macroglobulin Levels in Gingival Crevicular Fluid Pre- and Post-scaling and Root Planing with Adjunctive Tetracycline Fibers in Chronic Periodontitis: A Randomized Controlled Trial. J. Contemp. Dent. Pract. 2015, 16, 474–478. [Google Scholar] [CrossRef]
- Reise, M.; Wyrwa, R.; Müller, U.; Zylinski, M.; Völpel, A.; Schnabelrauch, M.; Berg, A.; Jandt, K.D.; Watts, D.C.; Sigusch, B.W. Release of metronidazole from electrospun poly(L-lactide-co-D/L-lactide) fibers for local periodontitis treatment. Dent. Mater. 2012, 28, 179–188. [Google Scholar] [CrossRef]
- Zhang, Z.; Zheng, Y.; Bian, X. Clinical effect of azithromycin as an adjunct to non-surgical treatment of chronic periodontitis: A meta-analysis of randomized controlled clinical trials. J. Periodontal. Res. 2016, 51, 275–283. [Google Scholar] [CrossRef]
- Maruyama, T.; Tomofuji, T.; Endo, Y.; Irie, K.; Azuma, T.; Ekuni, D.; Tamaki, N.; Yamamoto, T.; Morita, M. Supplementation of green tea catechins in dentifrices suppresses gingival oxidative stress and periodontal inflammation. Arch. Oral. Biol. 2011, 56, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Chava, V.K.; Vedula, B.D. Thermo-reversible green tea catechin gel for local application in chronic periodontitis: A 4-week clinical trial. J. Periodontol. 2013, 84, 1290–1296. [Google Scholar] [CrossRef] [PubMed]
- Assuma, R.; Oates, T.; Cochran, D.; Amar, S.; Graves, D.T. IL-1 and TNF antagonists inhibit the inflammatory response and bone loss in experimental periodontitis. J. Immunol. 1998, 160, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.A.; Song, Y.R.; Park, M.H.; Chung, H.Y.; Na, H.S.; Chung, J. Catechin ameliorates Porphyromonas gingivalis-induced inflammation via the regulation of TLR2/4 and inflammasome signaling. J. Periodontol. 2020, 91, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Qiu, W.; Hu, Z.; Lian, J.; Liu, Y.; Zhu, X.; Tu, M.; Fang, F.; Yu, Y.; Valverde, P.; et al. An Adiponectin Receptor Agonist Reduces Type 2 Diabetic Periodontitis. J. Dent. Res. 2019, 98, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Larsen, T. In vitro release of doxycycline from bioabsorbable materials and acrylic strips. J. Periodontol. 1990, 61, 30–34. [Google Scholar] [CrossRef]
- Pillai, O.; Panchagnula, R. Polymers in drug delivery. Curr. Opin. Chem. Biol. 2001, 5, 447–451. [Google Scholar] [CrossRef]
- Friesen, L.R.; Williams, K.B.; Krause, L.S.; Killoy, W.J. Controlled local delivery of tetracycline with polymer strips in the treatment of periodontitis. J. Periodontol. 2002, 73, 13–19. [Google Scholar] [CrossRef]
- Dixit, R.P.; Puthli, S.P. Oral strip technology: Overview and future potential. J. Control. Release 2009, 139, 94–107. [Google Scholar] [CrossRef]
- Vyas, S.P.; Sihorkar, V.; Mishra, V. Controlled and targeted drug delivery strategies towards intraperiodontal pocket diseases. J. Clin. Pharm. Ther. 2000, 25, 21–42. [Google Scholar] [CrossRef]
- Maze, G.I.; Reinhardt, R.A.; Agarwal, R.K.; Dyer, J.K.; Robinson, D.H.; DuBois, L.M.; Tussing, G.J.; Maze, C.R. Response to intracrevicular controlled delivery of 25% tetracycline from poly(lactide/glycolide) film strips in SPT patients. J. Clin. Periodontol. 1995, 22, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Moran, J.; Addy, M.; Wade, W.; Newcombe, R. The use of antimicrobial acrylic strips in the nonsurgical management of chronic periodontitis. Clin. Mater. 1990, 6, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Paolantonio, M.; D’Angelo, M.; Grassi, R.F.; Perinetti, G.; Piccolomini, R.; Pizzo, G.; Annunziata, M.; D’Archivio, D.; D’Ercole, S.; Nardi, G.; et al. Clinical and microbiologic effects of subgingival controlled-release delivery of chlorhexidine chip in the treatment of periodontitis: A multicenter study. J. Periodontol. 2008, 79, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Kudva, P.; Tabasum, S.T.; Shekhawat, N.K. Effect of green tea catechin, a local drug delivery system as an adjunct to scaling and root planing in chronic periodontitis patients: A clinicomicrobiological study. J. Indian Soc. Periodontol. 2011, 15, 39–45. [Google Scholar] [CrossRef]
- Kashi, T.S.; Eskandarion, S.; Esfandyari-Manesh, M.; Marashi, S.M.; Samadi, N.; Fatemi, S.M.; Atyabi, F.; Eshraghi, S.; Dinarvand, R. Improved drug loading and antibacterial activity of minocycline-loaded PLGA nanoparticles prepared by solid/oil/water ion pairing method. Int. J. Nanomed. 2012, 7, 221–234. [Google Scholar] [CrossRef]
- Jain, R.A. The manufacturing techniques of various drug loaded biodegradable poly(lactide-co-glycolide) (PLGA) devices. Biomaterials 2000, 21, 2475–2490. [Google Scholar] [CrossRef]
- Sitarek, K.; Stetkiewicz, J.; Wąsowicz, W. Evaluation of reproductive disorders in female rats exposed to N-methyl-2-pyrrolidone. Birth Defects Res. B Dev. Reprod. Toxicol. 2012, 95, 195–201. [Google Scholar] [CrossRef]
- Ruan, H.; Yu, Y.; Liu, Y.; Ding, X.; Guo, X.; Jiang, Q. Preparation and characteristics of thermoresponsive gel of minocycline hydrochloride and evaluation of its effect on experimental periodontitis models. Drug Deliv. 2016, 23, 525–531. [Google Scholar] [CrossRef]
- Oliveira, M.S.; Goulart, G.C.A.; Ferreira, L.A.M.; Carneiro, G. Hydrophobic ion pairing as a strategy to improve drug encapsulation into lipid nanocarriers for the cancer treatment. Expert Opin. Drug Deliv. 2017, 14, 983–995. [Google Scholar] [CrossRef]
- Lu, H.D.; Rummaneethorn, P.; Ristroph, K.D.; Prud’homme, R.K. Hydrophobic Ion Pairing of Peptide Antibiotics for Processing into Controlled Release Nanocarrier Formulations. Mol. Pharm. 2018, 15, 216–225. [Google Scholar] [CrossRef]
- Holmkvist, A.D.; Friberg, A.; Nilsson, U.J.; Schouenborg, J. Hydrophobic ion pairing of a minocycline/Ca(2+)/AOT complex for preparation of drug-loaded PLGA nanoparticles with improved sustained release. Int. J. Pharm. 2016, 499, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Bhattarai, N.; Gunn, J.; Zhang, M. Chitosan-based hydrogels for controlled, localized drug delivery. Adv. Drug Deliv. Rev. 2010, 62, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Gad, H.A.; Kamel, A.O.; Ezzat, O.M.; El Dessouky, H.F.; Sammour, O.A. Doxycycline hydrochloride-metronidazole solid lipid microparticles gels for treatment of periodontitis: Development, in-vitro and in-vivo clinical evaluation. Expert Opin. Drug Deliv. 2017, 14, 1241–1251. [Google Scholar] [CrossRef] [PubMed]
- Mehnert, W.; Mäder, K. Solid lipid nanoparticles: Production, characterization and applications. Adv. Drug Deliv. Rev. 2001, 47, 165–196. [Google Scholar] [CrossRef]
- Jadhav, K.; Dhamecha, D.; Bhattacharya, D.; Patil, M. Green and ecofriendly synthesis of silver nanoparticles: Characterization, biocompatibility studies and gel formulation for treatment of infections in burns. J. Photochem. Photobiol. B 2016, 155, 109–115. [Google Scholar] [CrossRef]
- Park, E.J.; Yi, J.; Kim, Y.; Choi, K.; Park, K. Silver nanoparticles induce cytotoxicity by a Trojan-horse type mechanism. Toxicol. In Vitro 2010, 24, 872–878. [Google Scholar] [CrossRef]
- Inkielewicz-Stepniak, I.; Santos-Martinez, M.J.; Medina, C.; Radomski, M.W. Pharmacological and toxicological effects of co-exposure of human gingival fibroblasts to silver nanoparticles and sodium fluoride. Int. J. Nanomed. 2014, 9, 1677–1687. [Google Scholar] [CrossRef]
- Yao, W.; Xu, P.; Pang, Z.; Zhao, J.; Chai, Z.; Li, X.; Li, H.; Jiang, M.; Cheng, H.; Zhang, B.; et al. Local delivery of minocycline-loaded PEG-PLA nanoparticles for the enhanced treatment of periodontitis in dogs. Int. J. Nanomed. 2014, 9, 3963–3970. [Google Scholar] [CrossRef]
- Kaya, M.; Baran, T.; Erdoğan, S.; Menteş, A.; Özüsağlam, M.A.; Çakmak, Y.S. Physicochemical comparison of chitin and chitosan obtained from larvae and adult Colorado potato beetle (Leptinotarsa decemlineata). Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 45, 72–81. [Google Scholar] [CrossRef]
- Moura, L.A.; Ribeiro, F.V.; Aiello, T.B.; Duek, E.A.; Sallum, E.A.; Nociti Junior, F.H.; Casati, M.Z.; Sallum, A.W. Characterization of the release profile of doxycycline by PLGA microspheres adjunct to non-surgical periodontal therapy. J. Biomater. Sci. Polym. Ed. 2015, 26, 573–584. [Google Scholar] [CrossRef]
- Sgolastra, F.; Petrucci, A.; Severino, M.; Graziani, F.; Gatto, R.; Monaco, A. Adjunctive photodynamic therapy to non-surgical treatment of chronic periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2013, 40, 514–526. [Google Scholar] [CrossRef] [PubMed]
- Alwaeli, H.A.; Al-Khateeb, S.N.; Al-Sadi, A. Long-term clinical effect of adjunctive antimicrobial photodynamic therapy in periodontal treatment: A randomized clinical trial. Lasers Med. Sci. 2015, 30, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Sreedhar, A.; Sarkar, I.; Rajan, P.; Pai, J.; Malagi, S.; Kamath, V.; Barmappa, R. Comparative evaluation of the efficacy of curcumin gel with and without photo activation as an adjunct to scaling and root planing in the treatment of chronic periodontitis: A split mouth clinical and microbiological study. J. Nat. Sci. Biol. Med. 2015, 6, S102–S109. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, L.M.; Calixto, G.M.; Chorilli, M.; Giusti, J.S.; Bagnato, V.S.; Soukos, N.S.; Amiji, M.M.; Fontana, C.R. Polymeric Nanoparticle-Based Photodynamic Therapy for Chronic Periodontitis in Vivo. Int. J. Mol. Sci. 2016, 17, 769. [Google Scholar] [CrossRef] [PubMed]
- Baelo, A.; Levato, R.; Julián, E.; Crespo, A.; Astola, J.; Gavaldà, J.; Engel, E.; Mateos-Timoneda, M.A.; Torrents, E. Disassembling bacterial extracellular matrix with DNase-coated nanoparticles to enhance antibiotic delivery in biofilm infections. J. Control. Release 2015, 209, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Forier, K.; Raemdonck, K.; De Smedt, S.C.; Demeester, J.; Coenye, T.; Braeckmans, K. Lipid and polymer nanoparticles for drug delivery to bacterial biofilms. J. Control. Release 2014, 190, 607–623. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Pacheco, C.G.; Fernandes, N.A.R.; Primo, F.L.; Tedesco, A.C.; Bellile, E.; Retamal-Valdes, B.; Feres, M.; Guimarães-Stabili, M.R.; Rossa, C., Jr. Local application of curcumin-loaded nanoparticles as an adjunct to scaling and root planing in periodontitis: Randomized, placebo-controlled, double-blind split-mouth clinical trial. Clin. Oral. Investig. 2021, 25, 3217–3227. [Google Scholar] [CrossRef]
- Izui, S.; Sekine, S.; Maeda, K.; Kuboniwa, M.; Takada, A.; Amano, A.; Nagata, H. Antibacterial Activity of Curcumin Against Periodontopathic Bacteria. J. Periodontol. 2016, 87, 83–90. [Google Scholar] [CrossRef]
- Zambrano, L.M.G.; Brandao, D.A.; Rocha, F.R.G.; Marsiglio, R.P.; Longo, I.B.; Primo, F.L.; Tedesco, A.C.; Guimaraes-Stabili, M.R.; Rossa Junior, C. Local administration of curcumin-loaded nanoparticles effectively inhibits inflammation and bone resorption associated with experimental periodontal disease. Sci. Rep. 2018, 8, 6652. [Google Scholar] [CrossRef]
- Zhou, T.; Chen, D.; Li, Q.; Sun, X.; Song, Y.; Wang, C. Curcumin inhibits inflammatory response and bone loss during experimental periodontitis in rats. Acta Odontol. Scand. 2013, 71, 349–356. [Google Scholar] [CrossRef]
- Perez-Pacheco, C.G.; Fernandes, N.A.R.; Camilli, A.C.; Ferrarezi, D.P.; Silva, A.F.; Zunareli, M.C.; Amantino, C.F.; Primo, F.L.; Guimarães-Stabilli, M.R.; Junior, C.R. Local administration of curcumin-loaded nanoparticles enhances periodontal repair in vivo. Naunyn Schmiedebergs Arch. Pharmacol. 2022, 396, 311–321. [Google Scholar] [CrossRef]
- Allen, T.M.; Cullis, P.R. Liposomal drug delivery systems: From concept to clinical applications. Adv. Drug Deliv. Rev. 2013, 65, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Thangavelu, A.; Stelin, K.S.; Vannala, V.; Mahabob, N.; Hayyan, F.M.B.; Sundaram, R. An Overview of Chitosan and Its Role in Periodontics. J. Pharm. Bioallied. Sci. 2021, 13, S15–S18. [Google Scholar] [CrossRef]
- Akncbay, H.; Senel, S.; Ay, Z.Y. Application of chitosan gel in the treatment of chronic periodontitis. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 80, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Ikinci, G.; Senel, S.; Akincibay, H.; Kaş, S.; Erciş, S.; Wilson, C.G.; Hincal, A.A. Effect of chitosan on a periodontal pathogen Porphyromonas gingivalis. Int. J. Pharm. 2002, 235, 121–127. [Google Scholar] [CrossRef]
- Dong, W.Y.; Körber, M.; López Esguerra, V.; Bodmeier, R. Stability of poly(D,L-lactide-co-glycolide) and leuprolide acetate in in-situ forming drug delivery systems. J. Control. Release 2006, 115, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, H.M.; Ahmed, T.A.; Hussain, M.D.; Rahman, Z.; Samy, A.M.; Kaseem, A.A.; Nutan, M.T. Development of meloxicam in situ implant formulation by quality by design principle. Drug Dev. Ind. Pharm. 2014, 40, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Wang, J.; Shao, J.; Kouwer, P.H.J.; Bronkhorst, E.M.; Jansen, J.A.; Walboomers, X.F.; Yang, F. A tunable and injectable local drug delivery system for personalized periodontal application. J. Control. Release 2020, 324, 134–145. [Google Scholar] [CrossRef]
- Lu, S.; Ren, X.; Guo, T.; Cao, Z.; Sun, H.; Wang, C.; Wang, F.; Shu, Z.; Hao, J.; Gui, S.; et al. Controlled release of iodine from cross-linked cyclodextrin metal-organic frameworks for prolonged periodontal pocket therapy. Carbohydr. Polym. 2021, 267, 118187. [Google Scholar] [CrossRef]
- Messora, M.R.; Apolinário Vieira, G.H.; Vanderlei, J.; Mariguela, V.C.; Fernandes, P.G.; Palioto, D.B.; Scombatti de Souza, S.L.; Novaes, A.B., Jr.; Furlaneto, F.; Taba, M., Jr. Rosuvastatin promotes benefits on induced periodontitis in hypertensive rats. J. Periodontal. Res. 2017, 52, 734–744. [Google Scholar] [CrossRef]
- Lim, S.Y.; Dafydd, M.; Ong, J.; Ord-McDermott, L.A.; Board-Davies, E.; Sands, K.; Williams, D.; Sloan, A.J.; Heard, C.M. Mucoadhesive thin films for the simultaneous delivery of microbicide and anti-inflammatory drugs in the treatment of periodontal diseases. Int. J. Pharm. 2020, 573, 118860. [Google Scholar] [CrossRef] [PubMed]
- Lizambard, M.; Menu, T.; Fossart, M.; Bassand, C.; Agossa, K.; Huck, O.; Neut, C.; Siepmann, F. In-situ forming implants for the treatment of periodontal diseases: Simultaneous controlled release of an antiseptic and an anti-inflammatory drug. Int. J. Pharm. 2019, 572, 118833. [Google Scholar] [CrossRef] [PubMed]
- de Santana, R.B.; de Santana, C.M. Human intrabony defect regeneration with rhFGF-2 and hyaluronic acid—A randomized controlled clinical trial. J. Clin. Periodontol. 2015, 42, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Yang, J.; Chi, Y.; Wen, P.; Wang, Z.; Yu, S.; Xue, R.; Fan, J.; Li, H.; Chen, W.; et al. Natural polyphenol self-assembled pH-responsive nanoparticles loaded into reversible hydrogel to inhibit oral bacterial activity. Mol. Biomed. 2022, 3, 28. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Peng, X.; Zhou, X.; Zou, J.; Cheng, L. Emerging Applications of Drug Delivery Systems in Oral Infectious Diseases Prevention and Treatment. Molecules 2020, 25, 516. [Google Scholar] [CrossRef] [PubMed]
- Gottlow, J. Guided Tissue Regeneration Using Bioresorbable and Non-Resorbable Devices: Initial Healing and Long-Term Results. J. Periodontol. 1993, 64 (Suppl. 11S), 1157–1165. [Google Scholar] [CrossRef]
- Bunyaratavej, P.; Wang, H.L. Collagen membranes: A review. J. Periodontol. 2001, 72, 215–229. [Google Scholar] [CrossRef]
- Behring, J.; Junker, R.; Walboomers, X.F.; Chessnut, B.; Jansen, J.A. Toward guided tissue and bone regeneration: Morphology, attachment, proliferation, and migration of cells cultured on collagen barrier membranes. A systematic review. Odontology 2008, 96, 1–11. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, W.; Wang, Y.; Chen, Y.; Xie, J.; Su, J.; Huang, C. One-step treatment of periodontitis based on a core-shell micelle-in-nanofiber membrane with time-programmed drug release. J. Control. Release 2020, 320, 201–213. [Google Scholar] [CrossRef]
- Ho, M.H.; Claudia, J.C.; Tai, W.C.; Huang, K.Y.; Lai, C.H.; Chang, C.H.; Chang, Y.C.; Wu, Y.C.; Kuo, M.Y.; Chang, P.C. The treatment response of barrier membrane with amoxicillin-loaded nanofibers in experimental periodontitis. J. Periodontol. 2021, 92, 886–895. [Google Scholar] [CrossRef]
- Carlson-Mann, L.D.; Ibbott, C.G.; Grieman, R.B. Ridge augmentation with guided bone regeneration and GTAM case illustrations. Probe 1996, 30, 232–233. [Google Scholar]
- Ma, W.; Lyu, H.; Pandya, M.; Gopinathan, G.; Luan, X.; Diekwisch, T.G.H. Successful Application of a Galanin-Coated Scaffold for Periodontal Regeneration. J. Dent. Res. 2021, 100, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Ouchi, T.; Nakagawa, T. Mesenchymal stem cell-based tissue regeneration therapies for periodontitis. Regen. Ther. 2020, 14, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Sanz, M. Clinical and public health implications of periodontal and systemic diseases: An overview. Periodontol. 2000 2020, 83, 7–13. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, P.A.; Taba, M.; Nomizo, A.; Foss Freitas, M.C.; Suaid, F.A.; Uyemura, S.A.; Trevisan, G.L.; Novaes, A.B.; Souza, S.L.; Palioto, D.B.; et al. Effects of periodontal therapy on glycemic control and inflammatory markers. J. Periodontol. 2008, 79, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Faria-Almeida, R.; Navarro, A.; Bascones, A. Clinical and metabolic changes after conventional treatment of type 2 diabetic patients with chronic periodontitis. J. Periodontol. 2006, 77, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Matesanz-Pérez, P.; García-Gargallo, M.; Figuero, E.; Bascones-Martínez, A.; Sanz, M.; Herrera, D. A systematic review on the effects of local antimicrobials as adjuncts to subgingival debridement, compared with subgingival debridement alone, in the treatment of chronic periodontitis. J. Clin. Periodontol. 2013, 40, 227–241. [Google Scholar] [CrossRef]
- Lecio, G.; Ribeiro, F.V.; Pimentel, S.P.; Reis, A.A.; da Silva, R.V.C.; Nociti, F., Jr.; Moura, L.; Duek, E.; Casati, M.; Casarin, R.C.V. Novel 20% doxycycline-loaded PLGA nanospheres as adjunctive therapy in chronic periodontitis in type-2 diabetics: Randomized clinical, immune and microbiological trial. Clin. Oral. Investig. 2020, 24, 1269–1279. [Google Scholar] [CrossRef]
- Pereira, A.; Brito, G.A.C.; Lima, M.L.S.; Silva Júnior, A.A.D.; Silva, E.D.S.; de Rezende, A.A.; Bortolin, R.H.; Galvan, M.; Pirih, F.Q.; Araújo Júnior, R.F.; et al. Metformin Hydrochloride-Loaded PLGA Nanoparticle in Periodontal Disease Experimental Model Using Diabetic Rats. Int. J. Mol. Sci. 2018, 19, 3488. [Google Scholar] [CrossRef]
- Giménez-Siurana, A.; Gómez García, F.; Pagan Bernabeu, A.; Lozano-Pérez, A.A.; Aznar-Cervantes, S.D.; Cenis, J.L.; López-Jornet, P. Chemoprevention of Experimental Periodontitis in Diabetic Rats with Silk Fibroin Nanoparticles Loaded with Resveratrol. Antioxidants 2020, 9, 85. [Google Scholar] [CrossRef]
- de Souza Malta, F.; Napimoga, M.H.; Marins, L.M.; Miranda, T.S.; de Oliveira, F.B.; Posch, A.T.; Feres, M.; Duarte, P.M. Lithium chloride assuages bone loss in experimental periodontitis in estrogen-deficient rats. Clin. Oral. Investig. 2020, 24, 2025–2036. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, R.S.; Messora, M.R.; Silva, P.H.F.; Oliveira, L.F.; Leite-Panissi, C.; Salvador, S.; Casarin, R.; Novaes, A.B., Jr.; Palioto, D.B.; Furlaneto, F.A.C. Effects of Bifidobacterium animalis subsp. lactis HN019 on ligature-induced periodontitis in rats with experimental rheumatoid arthritis. Benef. Microbes 2020, 11, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Boese, S.; Gill, H.S. Coated floss for drug delivery into the gum pocket. Int. J. Pharm. 2021, 606, 120855. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Periodontitis | Therapy | Studied Adjunctive Therapeutical Agents | LDDS for Adjunctive Therapeutic Agents |
|---|---|---|---|
| Stage I, II, III | SRP, motivation and education for domiciliary oral hygiene, correction of bad habits (ex. Smoking), control of systemic diseases (ex. Diabetes). [1] | Anti-bacterial and anti-septic drugs (tetracyclines, metronidazole, azithromycin, metronidazole, chlorhexidine), inflammation modulators (statins, lipoxin, aspirin, erythropoietin), natural agents (TP, curcumin, TGEC, mangosteen) [3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30] | Fibers, Strips and Films, Microparticles, Nanosystems, Gels. [31,32] |
| Stage IV | SRP, motivation and education for domiciliary oral hygiene, correction of bad habits (ex. Smoking), control of systemic diseases (ex. Diabetes), surgical correction of bone defects. [2] | Antibiotic (amoxicillin), alveolar bone and tissue repairing agents (inhibitor SP600125, BMP-2, rhAm, GAL, MSCs) [33,34,35,36,37] | Membranes, Scaffolds. [31] |
| Type of Administration | Advantages | Disadvantages | References |
|---|---|---|---|
| Systemic | Some patients may prefer conventional drug- administration; well-known associated risk; no need of second intervention; cheap. | Low bioavailability of the drug; need for frequent doses; gastrointestinal issues; dysbacteriosis; drug resistance; interaction with other systemic administrated drugs. | [31,45] |
| LDDS | High bioavailability of the drug; controlled drug release; bypass of the hepatic metabolism; no gastrointestinal issues; reduction in frequent doses; mini-invasiveness of some LDDSs; high compliance of the patient; use of drugs that are not compatible with systemic administration (ex. Chlorhexidine); no interaction with other drugs. | Difficulty of management of some types of LDDS, some of them have difficulty to provide sufficient drug-concentration; the need of reintervention for the oldest LDDS; the need of further investigations to assess which kind of LDDS is the best one; high costs. | [31,32,46,47] |
| Type of LDDS | Indications | Contraindications |
|---|---|---|
| Fibers | Adjunct to SRP, suitable for inaccessible areas | Larger pockets areas, surgical correction of periodontal site |
| Strips and Films | Adjunct to SRP, suitable for larger pocket areas | Inaccessible posterior sites, surgical correction of periodontal site |
| Microparticles | Adjunct to SRP | surgical correction of periodontal site |
| Nanosystems | Adjunct to SRP | surgical correction of periodontal site |
| Gels | Adjunct to SRP | surgical correction of periodontal site |
| Membranes | Adjunct to surgical correction of periodontal site | Not indicated as adjunct to periodontal therapy if it does not require surgical correction of the bone defect |
| Scaffolds | Adjunct to surgical correction of periodontal site | Not indicated as adjunct to periodontal therapy if it does not require surgical correction of the bone defect |
| System | Material | Drug | Study Design | Time of Constant Drug Release | % Drug Loaded | % EE | References |
|---|---|---|---|---|---|---|---|
| Fibers | Ethyl vinyl acetate | Tetracyclines | Clinical trial | 10 days | 25% | Not mentioned | [56] |
| Fibers | Collagen | Tetracyclines | Case control | Not mentioned | Not mentioned | Not mentioned | [3] |
| Fibers | Fibrillar collagen | Tetracyclines | In vitro | 10 days | Not mentioned | Not mentioned | [4] |
| Nanofibers | PLGA | TP | In vitro/in vivo | 14 days | Not mentioned | Not mentioned | [5] |
| Strip | Polyhydroxybutyric acid | Tetracycline hydrochloride or metronidazole | In vitro/in vivo | 4/5 days | 25% metronidazole, 25% tetracycline HCI, 10% tetracycline HCI | Not mentioned | [6] |
| Film | Hydroxypropylcellulose | Chlorhexidine diacetate | In vitro | 3 days | 20% chlorhexidine | Not mentioned | [7] |
| Microparticles | Sulfate/sulfonate-bearing biopolymers | Minocycline | In vitro | 9 days at pH 7.4 and 18 days at pH 6.4 | 44.69% ± 0.03% | 96.98% ± 0.12% | [8] |
| Microparticles | Cross-linked chitosan | Metronidazole | In vitro | Prolonged release (not specified how many days) | Not mentioned | 59.40% | [9] |
| Nanoparticles | Chitosan | Doxycycline | In vitro | Not specified | 28% | 75% | [10] |
| Microspheres in combination with Hydrogel | serum albumin microspheres containing minocycline and zinc oxide nanoparticles (ZnO NPs) in a Carbopol 940® hydrogel. | Minocycline | In vitro | slow-release time was more than 72 h with pH-sensitive property | Not mentioned | 99.99% | [11] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amato, M.; Santonocito, S.; Polizzi, A.; Tartaglia, G.M.; Ronsivalle, V.; Viglianisi, G.; Grippaudo, C.; Isola, G. Local Delivery and Controlled Release Drugs Systems: A New Approach for the Clinical Treatment of Periodontitis Therapy. Pharmaceutics 2023, 15, 1312. https://doi.org/10.3390/pharmaceutics15041312
Amato M, Santonocito S, Polizzi A, Tartaglia GM, Ronsivalle V, Viglianisi G, Grippaudo C, Isola G. Local Delivery and Controlled Release Drugs Systems: A New Approach for the Clinical Treatment of Periodontitis Therapy. Pharmaceutics. 2023; 15(4):1312. https://doi.org/10.3390/pharmaceutics15041312
Chicago/Turabian StyleAmato, Mariacristina, Simona Santonocito, Alessandro Polizzi, Gianluca Martino Tartaglia, Vincenzo Ronsivalle, Gaia Viglianisi, Cristina Grippaudo, and Gaetano Isola. 2023. "Local Delivery and Controlled Release Drugs Systems: A New Approach for the Clinical Treatment of Periodontitis Therapy" Pharmaceutics 15, no. 4: 1312. https://doi.org/10.3390/pharmaceutics15041312