
Predicting Hydroxychloroquine Clearance in Healthy and Diseased Populations Using a Physiologically Based Pharmacokinetic Approach
 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Observed Pharmacokinetic Data
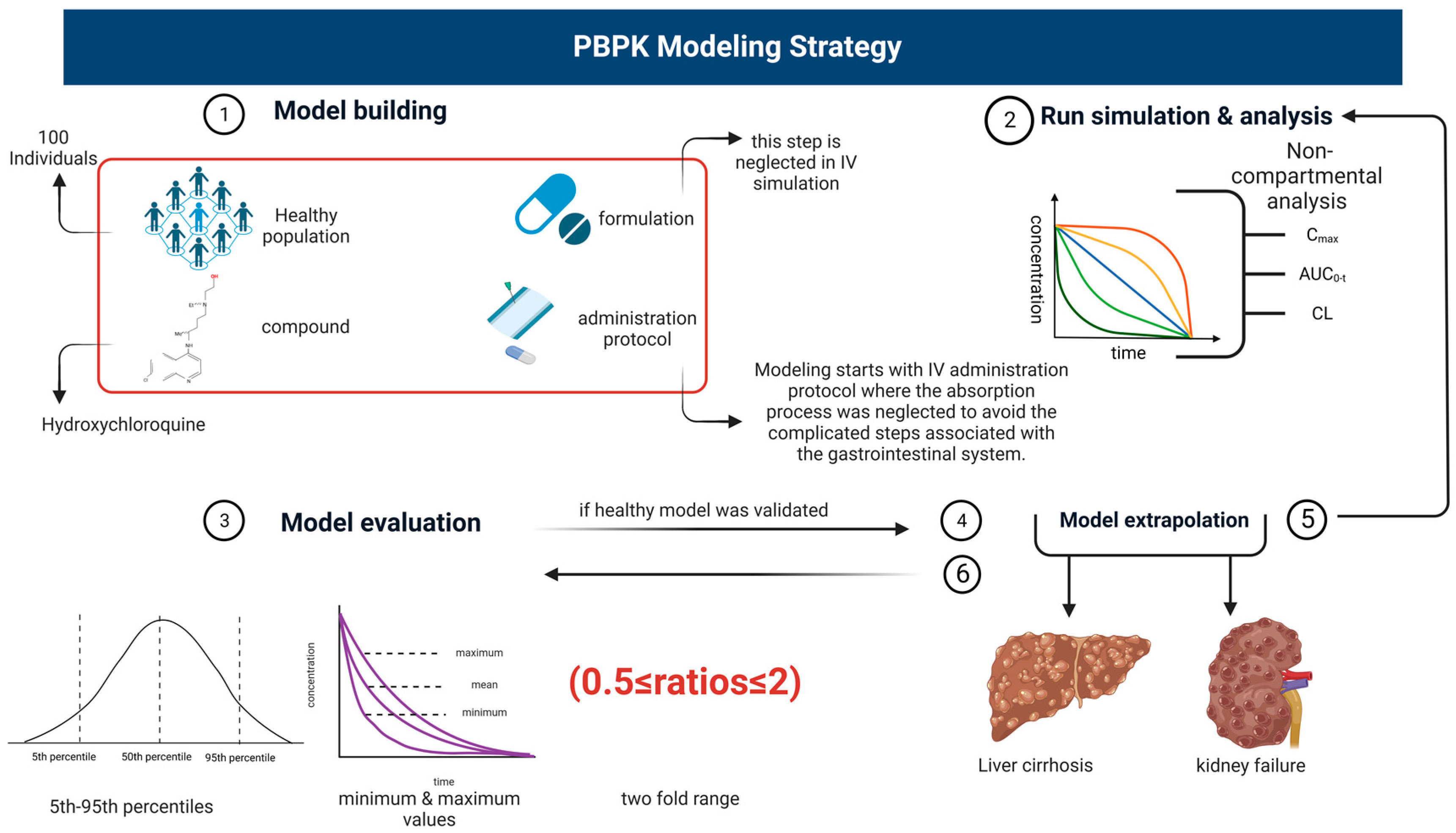
2.2. Modeling Software and Design
Model Designing
2.3. Model Parametrization
2.4. Software
2.4.1. Absorption
2.4.2. Distribution
2.4.3. Metabolism
2.5. Model Predictions in Liver Cirrhosis and CKD Populations
2.6. Evaluation of Developed PBPK Models
3. Results
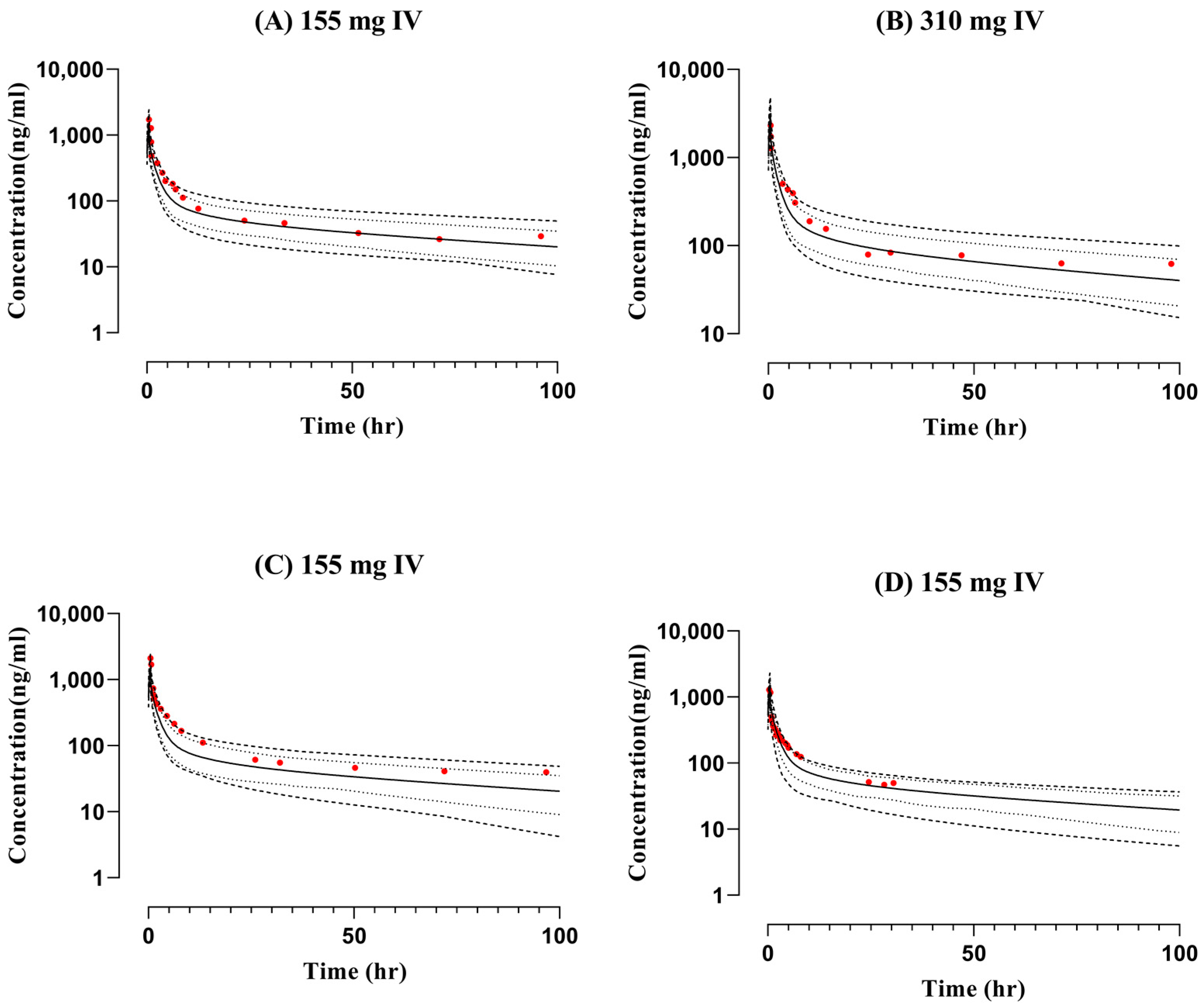
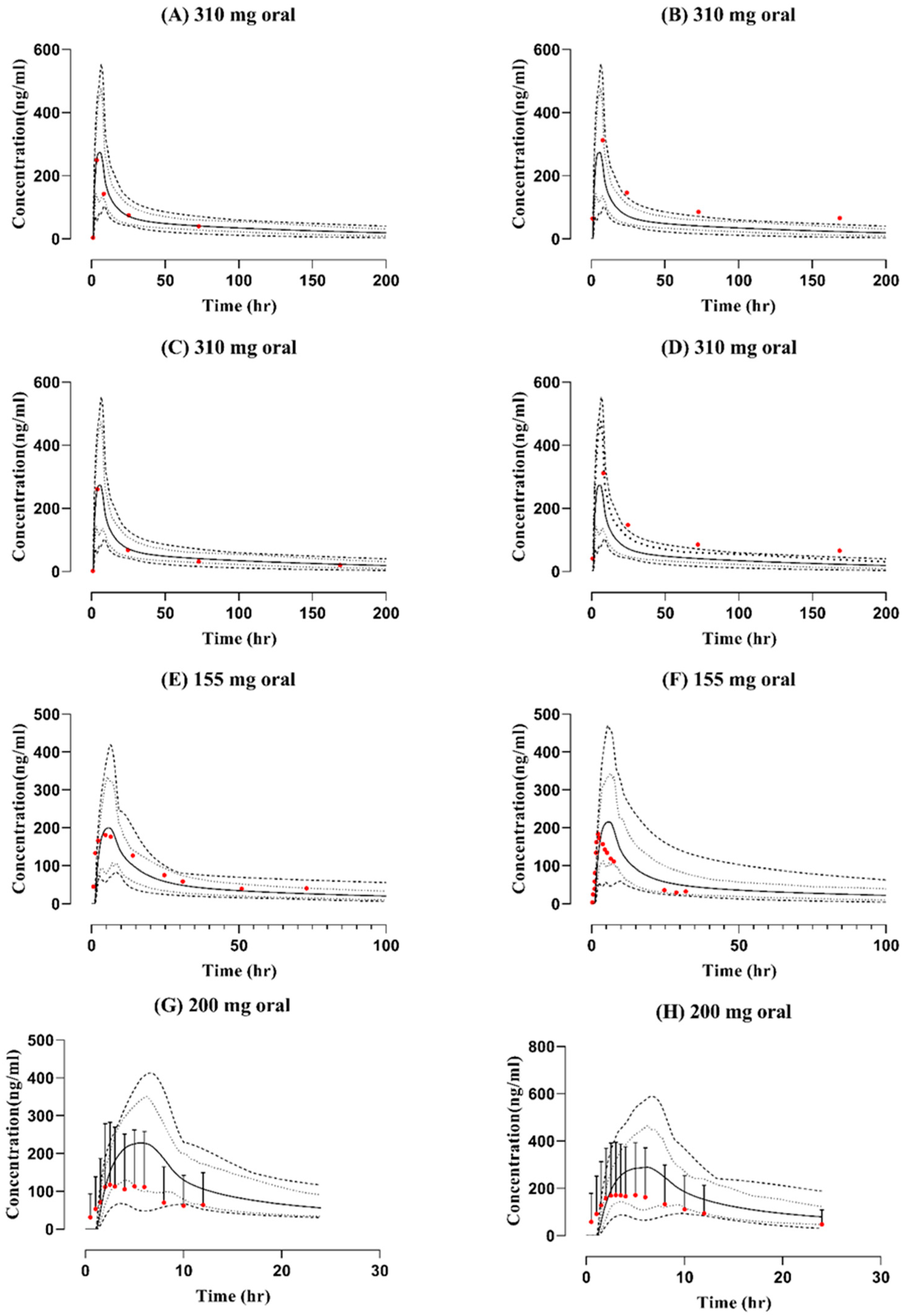
3.1. Intravenous and Oral Administration in the Healthy Population
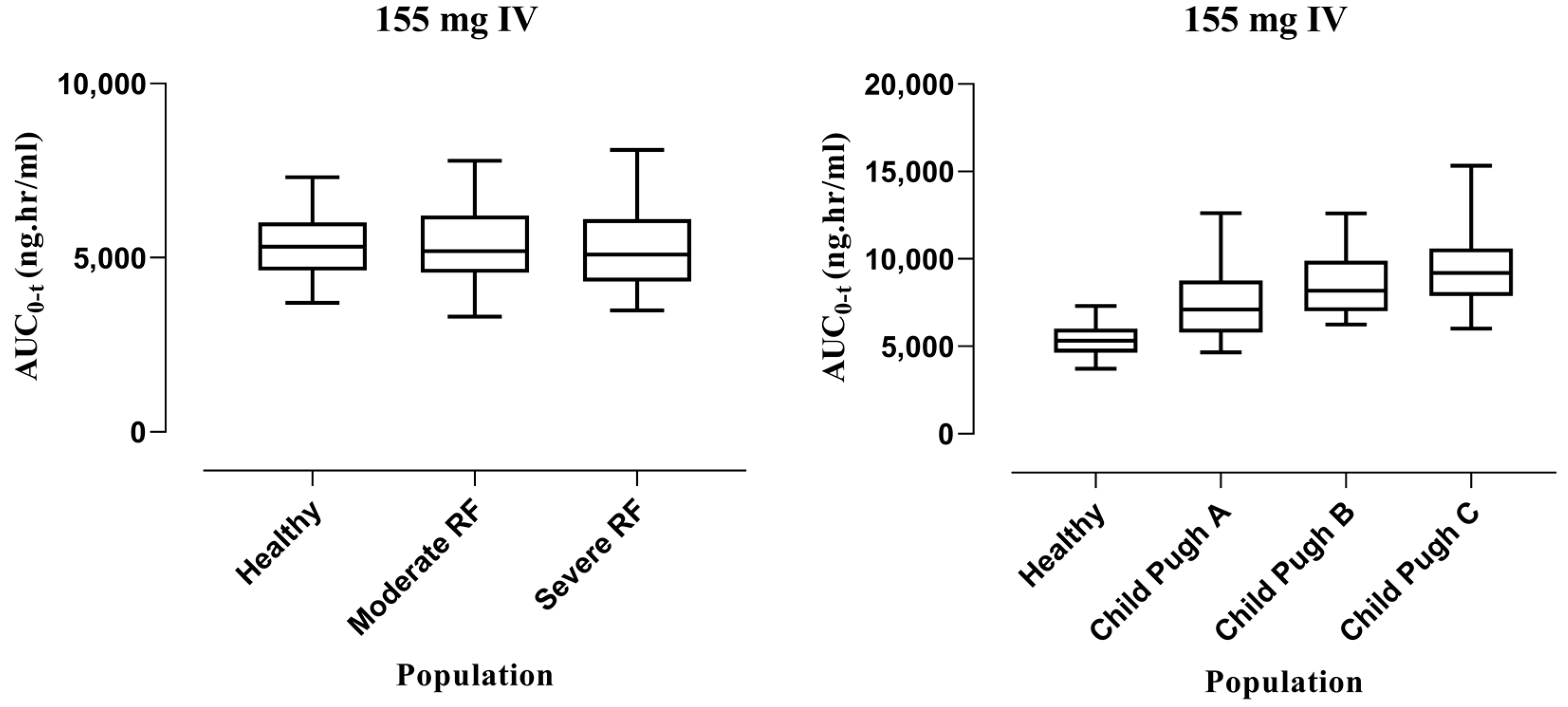
3.2. Extrapolation of the Model to Liver Cirrhosis and CKD
3.2.1. Intravenous Administration
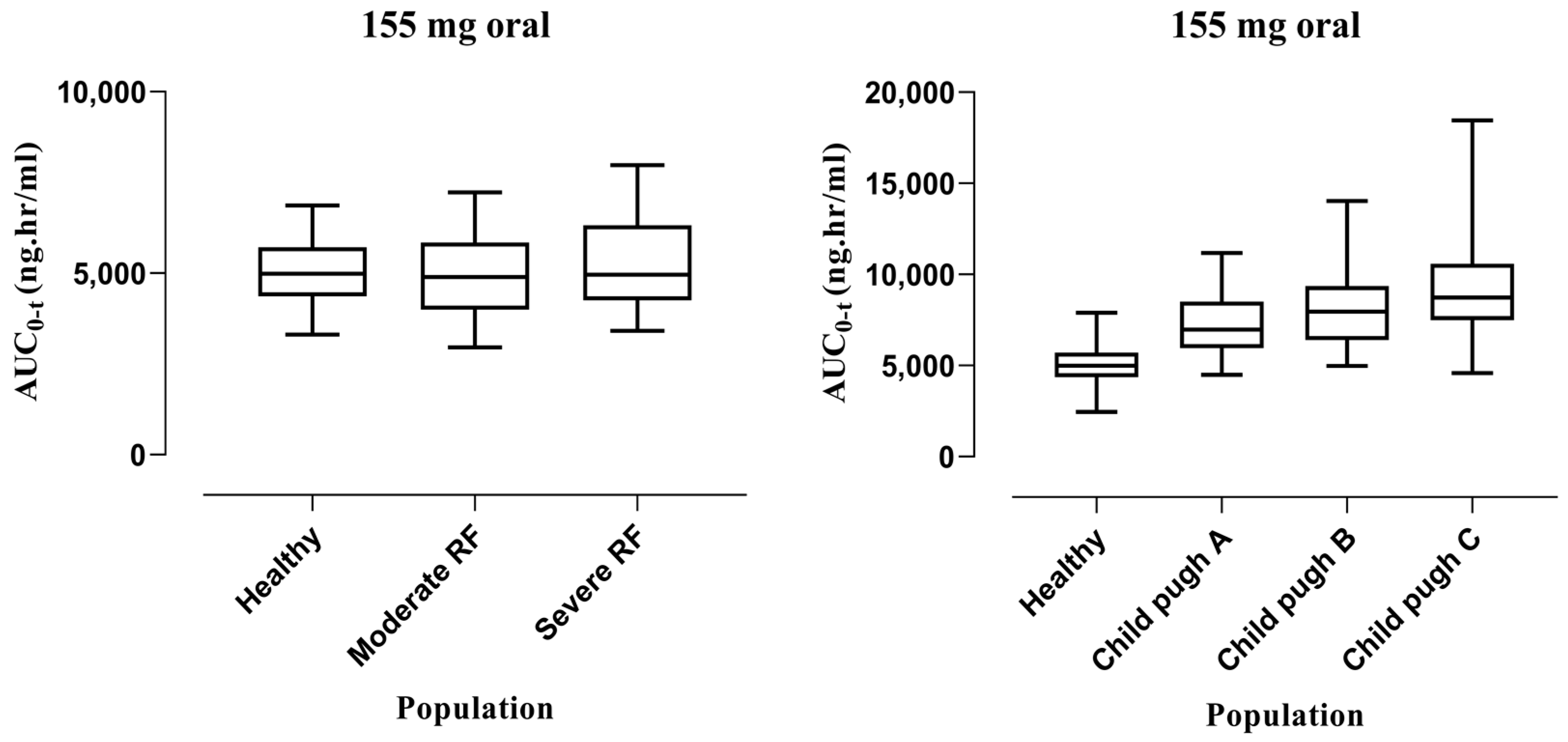
3.2.2. Oral Administration
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McChesney, E.W. Animal toxicity and pharmacokinetics of hydroxychloroquine sulfate. Am. J. Med. 1983, 75, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Tett, S.; Cutler, D.; Day, R. Antimalarials in rheumatic diseases. Bailliere’s Clin. Rheumatol. 1990, 4, 467–489. [Google Scholar] [CrossRef] [PubMed]
- Ben-Zvi, I.; Kivity, S.; Langevitz, P.; Shoenfeld, Y. Hydroxychloroquine: From malaria to autoimmunity. Clin. Rev. Allergy Immunol. 2012, 42, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wang, Y.; Agostinis, P.; Rabson, A.; Melino, G.; Carafoli, E.; Shi, Y.; Sun, E. Is hydroxychloroquine beneficial for COVID-19 patients? Cell Death Dis. 2020, 11, 512. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.I. Mechanism of action of hydroxychloroquine as an antirheumatic drug. Semin. Arthritis Rheum. 1993, 23, 82–91. [Google Scholar] [CrossRef]
- Tett, S.; Cutler, D.; Day, R.; Brown, K. Bioavailability of hydroxychloroquine tablets in healthy volunteers. Br. J. Clin. Pharmacol. 1989, 27, 771–779. [Google Scholar] [CrossRef]
- Benet, L.Z.; Broccatelli, F.; Oprea, T.I. BDDCS applied to over 900 drugs. AAPS J. 2011, 13, 519–547. [Google Scholar] [CrossRef]
- Warhurst, D.C.; Steele, J.C.; Adagu, I.S.; Craig, J.C.; Cullander, C. Hydroxychloroquine is much less active than chloroquine against chloroquine-resistant Plasmodium falciparum, in agreement with its physicochemical properties. J. Antimicrob. Chemother. 2003, 52, 188–193. [Google Scholar] [CrossRef]
- Tett, S.; Cutler, D.; Day, R.; Brown, K. A dose-ranging study of the pharmacokinetics of hydroxy-chloroquine following intravenous administration to healthy volunteers. Br. J. Clin. Pharmacol. 1988, 26, 303–313. [Google Scholar] [CrossRef]
- McLachlan, A.; Cutler, D.; Tett, S. Plasma protein binding of the enantiomers of hydroxychloroquine and metabolites. Eur. J. Clin. Pharmacol. 1993, 44, 481–484. [Google Scholar] [CrossRef]
- Wahie, S.; Daly, A.K.; Cordell, H.J.; Goodfield, M.J.; Jones, S.K.; Lovell, C.R.; Carmichael, A.J.; Carr, M.M.; Drummond, A.; Natarajan, S. Clinical and pharmacogenetic influences on response to hydroxychloroquine in discoid lupus erythematosus: A retrospective cohort study. J. Investig. Dermatol. 2011, 131, 1981–1986. [Google Scholar] [CrossRef]
- Furst, D.E. Pharmacokinetics of hydroxychloroquine and chloroquine during treatment of rheumatic diseases. Lupus 1996, 5, 11–15. [Google Scholar] [CrossRef]
- Liu, J.; Cao, R.; Xu, M.; Wang, X.; Zhang, H.; Hu, H.; Li, Y.; Hu, Z.; Zhong, W.; Wang, M. Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell Discov. 2020, 6, 16. [Google Scholar] [CrossRef]
- Chatre, C.; Roubille, F.; Vernhet, H.; Jorgensen, C.; Pers, Y.-M. Cardiac complications attributed to chloroquine and hydroxychloroquine: A systematic review of the literature. Drug Saf. 2018, 41, 919–931. [Google Scholar] [CrossRef]
- Marmor, M.F.; Kellner, U.; Lai, T.Y.; Melles, R.B.; Mieler, W.F. Recommendations on screening for chloroquine and hydroxychloroquine retinopathy (2016 revision). Ophthalmology 2016, 123, 1386–1394. [Google Scholar] [CrossRef]
- Jamei, M. Recent advances in development and application of physiologically-based pharmacokinetic (PBPK) models: A transition from academic curiosity to regulatory acceptance. Curr. Pharmacol. Rep. 2016, 2, 161–169. [Google Scholar] [CrossRef]
- Mumtaz, M.; Fisher, J.; Blount, B.; Ruiz, P. Application of physiologically based pharmacokinetic models in chemical risk assessment. J. Toxicol. 2012, 2012, 904603. [Google Scholar] [CrossRef]
- Shreekant, D.; Bhimanna, K. 4-Aminoquinolines: An overview of antimalarial chemotherapy. Med. Chem. 2016, 6, 001–011. [Google Scholar]
- Rasool, M.F.; Khalil, F.; Läer, S. Optimizing the clinical use of carvedilol in liver cirrhosis using a physiologically based pharmacokinetic modeling approach. Eur. J. Drug Metab. Pharmacokinet. 2017, 42, 383–396. [Google Scholar] [CrossRef]
- Kalam, M.N.; Rasool, M.F.; Alqahtani, F.; Imran, I.; Rehman, A.U.; Ahmed, N. Development and evaluation of a physiologically based pharmacokinetic drug-disease model of propranolol for suggesting model informed dosing in liver cirrhosis patients. Drug Des. Dev. Ther. 2021, 15, 1195. [Google Scholar] [CrossRef]
- Rasool, M.F.; Khalil, F.; Läer, S. A physiologically based pharmacokinetic drug–disease model to predict carvedilol exposure in adult and Paediatric heart failure patients by incorporating pathophysiological changes in hepatic and renal blood flows. Clin. Pharmacokinet. 2015, 54, 943–962. [Google Scholar] [CrossRef] [PubMed]
- Edginton, A.N.; Willmann, S. Physiology-based simulations of a pathological condition. Clin. Pharmacokinet. 2008, 47, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.N.; Boussery, K.; Rowland-Yeo, K.; Tucker, G.T.; Rostami-Hodjegan, A. A semi-mechanistic model to predict the effects of liver cirrhosis on drug clearance. Clin. Pharmacokinet. 2010, 49, 189–206. [Google Scholar] [CrossRef] [PubMed]
- Malik, P.R.; Yeung, C.H.; Ismaeil, S.; Advani, U.; Djie, S.; Edginton, A.N. A physiological approach to pharmacokinetics in chronic kidney disease. J. Clin. Pharmacol. 2020, 60, S52–S62. [Google Scholar] [CrossRef] [PubMed]
- Rowland Yeo, K.; Aarabi, M.; Jamei, M.; Rostami-Hodjegan, A. Modeling and predicting drug pharmacokinetics in patients with renal impairment. Expert Rev. Clin. Pharmacol. 2011, 4, 261–274. [Google Scholar] [CrossRef]
- Zhang, M.; Yao, X.; Hou, Z.; Guo, X.; Tu, S.; Lei, Z.; Yu, Z.; Liu, X.; Cui, C.; Chen, X. Development of a Physiologically Based Pharmacokinetic Model for Hydroxychloroquine and Its Application in Dose Optimization in Specific COVID-19 Patients. Front. Pharmacol. 2021, 11, 585021. [Google Scholar] [CrossRef]
- Yao, X.; Ye, F.; Zhang, M.; Cui, C.; Huang, B.; Niu, P.; Liu, X.; Zhao, L.; Dong, E.; Song, C. In vitro antiviral activity and projection of optimized dosing design of hydroxychloroquine for the treatment of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 71, 732–739. [Google Scholar] [CrossRef]
- Collins, K.P.; Jackson, K.M.; Gustafson, D.L. Hydroxychloroquine: A Physiologically-Based Pharmacokinetic Model in the Context of Cancer-Related Autophagy Modulation. J. Pharmacol. Exp. Ther. 2018, 365, 447–459. [Google Scholar] [CrossRef]
- Tett, S.E.; Cutler, D.J.; Day, R.O. Bioavailability of hydroxychloroquine tablets assessed with deconvolution techniques. J. Pharm. Sci. 1992, 81, 155–159. [Google Scholar] [CrossRef]
- Williams, S.B.; Patchen, L.C.; Churchill, F.C. Analysis of blood and urine samples for hydroxychloroquine and three major metabolites by high-performance liquid chromatography with fluorescence detection. J. Chromatogr. B Biomed. Sci. Appl. 1988, 433, 197–206. [Google Scholar] [CrossRef]
- Ducharme, J.; Fieger, H.; Ducharme, M.; Khalil, S.; Wainer, I. Enantioselective disposition of hydroxychloroquine after a single oral dose of the racemate to healthy subjects [see comments]. Br. J. Clin. Pharmacol. 1995, 40, 127–133. [Google Scholar] [CrossRef]
- Liu, Y.-M.; Chen, Q.; Zhang, M.-Q.; Liu, G.-Y.; Jia, J.-Y.; Pu, H.-H.; Liu, Y.; Hu, C.-Y.; Lu, C.; Wang, W. A parallel design study to assess the bioequivalence of generic and branded hydroxychloroquine sulfate tablets in healthy volunteers. Arzneimittelforschung 2012, 62, 644–649. [Google Scholar] [CrossRef]
- Rasool, M.; Khalid, R.; Imran, I.; Majeed, A.; Saeed, H.; Alasmari, F.; Alanazi, M.; Alqahtani, F. Investigating the Role of Altered Systemic Albumin Concentration on the Disposition of Theophylline in Adult and Pediatric Patients with Asthma by Using the Physiologically Based Pharmacokinetic Approach. Drug Metab. Dispos. 2020, 48, 570–579. [Google Scholar] [CrossRef]
- Khalid, S.; Rasool, M.F.; Imran, I.; Majeed, A.; Saeed, H.; Rehman, A.U.; Ashraf, W.; Ahmad, T.; Bin Jardan, Y.A.; Alqahtani, F. A Physiologically Based Pharmacokinetic Model for Predicting Diazepam Pharmacokinetics after Intravenous, Oral, Intranasal, and Rectal Applications. Pharmaceutics 2021, 13, 1480. [Google Scholar] [CrossRef]
- Rasool, M.F.; Khalid, S.; Majeed, A.; Saeed, H.; Imran, I.; Mohany, M.; Al-Rejaie, S.S.; Alqahtani, F. Development and Evaluation of Physiologically Based Pharmacokinetic Drug–Disease Models for Predicting Rifampicin Exposure in Tuberculosis and Cirrhosis Populations. Pharmaceutics 2019, 11, 578. [Google Scholar] [CrossRef]
- Zhang, Y.; Huo, M.; Zhou, J.; Xie, S. PKSolver: An add-in program for pharmacokinetic and pharmacodynamic data analysis in Microsoft Excel. Comput. Methods Programs Biomed. 2010, 99, 306–314. [Google Scholar] [CrossRef]
- Jallouli, M.; Galicier, L.; Zahr, N.; Aumaitre, O.; Frances, C.; Le Guern, V.; Lioté, F.; Smail, A.; Limal, N.; Perard, L. Determinants of hydroxychloroquine blood concentration variations in systemic lupus erythematosus. Arthritis Rheumatol. 2015, 67, 2176–2184. [Google Scholar] [CrossRef]
- Lee, J.; Luc, S.; Greenblatt, D.; Kalish, R.; McAlindon, T. Factors associated with blood hydroxychloroquine level in lupus patients: Renal function could be important. Lupus 2013, 22, 541. [Google Scholar] [CrossRef]
- Lu, J.; Huang, Y.; Ye, Q.; Shang, F.; Ming, M.; Xu, H.; Li, Z. Low-dose oral hydroxychloroquine led to impaired vision in a child with renal failure: Case report and literature review. Medicine 2021, 100, e24919. [Google Scholar] [CrossRef]
- Marra, F.; Smolders, E.J.; El-Sherif, O.; Boyle, A.; Davidson, K.; Sommerville, A.J.; Marzolini, C.; Siccardi, M.; Burger, D.; Gibbons, S. Recommendations for dosing of repurposed COVID-19 medications in patients with renal and hepatic impairment. Drugs RD 2021, 21, 9–27. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr. No. | Study ID | Dose (mg) | Infusion Time | N | Female (n) % | Mean Age (years) | Mean Weight (kg) | Population |
|---|---|---|---|---|---|---|---|---|
| Hydroxychloroquine administered by intravenous infusion | ||||||||
| 1- | Tett et al. (1988) [9] | 155 | 30 min | 5 | 60 | 22.6 (range: 19–27 | 63.5 (range: 55–68) | Healthy |
| 310 | ||||||||
| 2- | Tett et al. (1989) [6] | 155 | 30 min | 5 | 60 | 22.6 (range: 19–27 | 63.5 (range: 55–68) | Healthy |
| 3- | Tett et al. (1992) [29] | 155 | 30 min | 9 | 66 | 24.4 (range: 20–28) | 71.4 (range: 51–92.5) | Healthy |
| Hydroxychloroquine administered orally | ||||||||
| 1- | Sharyon B. Williams et al. (1988) [30] | 310 | NA | 2 | N/R | NA | 84 | Healthy |
| 88 | ||||||||
| 2- | Tett et al. (1989) [6] | 155 | NA | 5 | 60 | 22.6 (range: 19–27 | 63.5 (range: 55–68) | Healthy |
| 3- | Tett et al. (1992) [29] | 155 | NA | 9 | 66 | 24.4 (range: 20–28) | 71.4 (range: 51–92.5) | Healthy |
| 4- | J. Ducharme et al. (1995) [31] | 200 | NA | 24 | 0 | 20–36 | 72–88 | Healthy |
| 5- | Liu. Y.-M et al. (2012) [32] | 200 | NA | Test: 27 | 0 | 20.1–30.0 | 51.0–74.8 | Healthy |
| Reference: [27] | 20.1–27.9 | 51.9–71.5 | ||||||
| Parameter | Input Value | Reference |
|---|---|---|
| Physicochemical properties | ||
| Molecular weight (g/mol) | 335.87 | [6] |
| Lipophilicity (Log P) | 2.4 | Optimized value |
| Dissociation constant (pKa) | 8.27, 9.67 | [8] |
| ADME properties | ||
| Blood to plasma ratio (B/P) | 7.2 | [26] |
| Fraction unbound plasma (fu) | 0.48 | [12] |
| Plasma protein binding partner | alpha-1 acid glycoprotein | [12] |
| Solubility of hydroxychloroquine sulfate (phosphate-buffered saline) | 5 mg/mL (at pH 7.2) | [30] |
| Intestinal permeability | 1.06 × 10−5 cm/min | Optimized value |
| In vitro clearance (CYP2C8) (ul/min/pmol) | 0.0078 | Back calculated by using a well-stirred liver model |
| In vitro clearance (CYP2D6) (ul/min/pmol) | 0.025 | |
| Intrinsic clearance (CYP3A4) (ul/min/pmol) | 0.002 | |
| Partition coefficients | PK-Sim standard | |
| Cellular permeability | PK-Sim standard | |
| Renal plasma clearance (CLR) | 12.7 L/h | [26] |
| Cmax (ng/mL) | AUC0-t (ng/mL·hr) | CL(L/h) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Observed | Predicted | R Ratio | Observed | Predicted | R Ratio | Observed | Predicted | R Ratio |
| IV | |||||||||
| 1988 | 1716.74 | 1457.96 | 1.17 | 6587.57 | 5405.63 | 1.21 | 16.9 | 20.6 | 0.82 |
| 1988 310 | 2321.71 | 2017.4 | 1.15 | 12,607.25 | 11,122.39 | 1.13 | 12 | 20.36 | 0.6 |
| 1989 | 2105.9 | 1517.82 | 1.38 | 8649.54 | 5553.82 | 1.55 | 10.2 | 20.27 | 0.51 |
| 1992 | 1287.03 | 1280.82 | 1 | 3984.54 | 3364.52 | 1.18 | 31.05 | 26.85 | 1.15 |
| Oral | |||||||||
| 1988 vol * 1 wk * 1 | 249.18 | 251.96 | 0.98 | 5812.48 | 6566.34 | 0.88 | 38.94 | 37.98 | 1.02 |
| 1988 vol 1 wk 4 | 311.932 | 236.80 | 1.31 | 17,952.57 | 9209.71 | 1.94 | 10.06 | 25.59 | 0.5 |
| 1988 vol 2 wk 1 | 261.05 | 264.16 | 0.98 | 8237.36 | 9667.94 | 0.85 | 28.78 | 24.59 | 1.17 |
| 1988 vol 2 wk 4 | 311.932 | 236.80 | 1.31 | 17,938.45 | 9210.98 | 1.94 | 10.12 | 25.51 | 0.5 |
| 1989 | 180.77 | 197.96 | 0.91 | 5470.81 | 4596.05 | 1.19 | 21.56 | 24.05 | 0.89 |
| 1992 | 183.5 | 214.80 | 0.85 | 2432.33 | 3680.55 | 0.66 | 52.32 | 28.29 | 1.84 |
| 1995 | 117.427 | 226.99 | 0.51 | 988.14 | 1799.07 | 0.54 | 110.03 | 76.76 | 1.43 |
| 2012 | 171.833 | 288.66 | 0.59 | 2446.55 | 3771.88 | 0.64 | 61.33 | 38.94 | 1.57 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, F.; Asiri, A.M.; Zamir, A.; Rasool, M.F.; Alali, A.S.; Alsanea, S.; Walbi, I.A. Predicting Hydroxychloroquine Clearance in Healthy and Diseased Populations Using a Physiologically Based Pharmacokinetic Approach. Pharmaceutics 2023, 15, 1250. https://doi.org/10.3390/pharmaceutics15041250
Alqahtani F, Asiri AM, Zamir A, Rasool MF, Alali AS, Alsanea S, Walbi IA. Predicting Hydroxychloroquine Clearance in Healthy and Diseased Populations Using a Physiologically Based Pharmacokinetic Approach. Pharmaceutics. 2023; 15(4):1250. https://doi.org/10.3390/pharmaceutics15041250
Chicago/Turabian StyleAlqahtani, Faleh, Ali Mohammed Asiri, Ammara Zamir, Muhammad Fawad Rasool, Amer S. Alali, Sary Alsanea, and Ismail A. Walbi. 2023. "Predicting Hydroxychloroquine Clearance in Healthy and Diseased Populations Using a Physiologically Based Pharmacokinetic Approach" Pharmaceutics 15, no. 4: 1250. https://doi.org/10.3390/pharmaceutics15041250