3.1. Aerosol Particle Size and Geometry
The aerosol particle size of Technegas has had a wide range of reported values, using numerous techniques over the years, with size ranging from a few nanometres to hundreds of nanometres. This variation in reported size (and composition) has caused some controversy within the scientific community and many follow-up studies. Subsequently, there is an extensive understanding of the physicochemical aspects of this material as well as a detailed understanding of particle size methodology. Here, we report historical findings and discussion relating to particle size, characterisation, and methodology as well as highlight recent studies that overcome some of the earlier approaches and challenges relating to Technegas measurement.
In 1986, Burch et al. examined Technegas with electron microscopy and electron energy loss analysis. They described Technegas as radioactive ‘soot’ due to its appearance and reported it to be structured aggregates of carbon at a size ≤ 5.0 nm in diameter [
16]. Three years later, Strong and Agnew estimated the aerosol particle size to be above 100 nm. Strong and Agnew studied the particle size of Technegas using a multichannel diffusion battery, which sampled the aerosol through several parallel screens with collection filters. Filters were collected and analysed for radioactivity and a particle size distribution generated [
17]. Strong and Agnew reported a mean particle size of 140 nm with a GSD of 1.5, over a 4.5 min sampling period. Additionally, the team reported that there was little difference in the particle size distribution with respect to sampling time when measurements were taken at 1, 4.5, and 8.5 min. Using these data, Strong and Agnew described the fractional deposition in the tracheobronchial (TB) and parenchymal (P) regions for aerosols with aerodynamic median diameters of less than 500 nm. The study proposed that particles with a diameter of 140 nm were estimated to have a fractional deposition of 0.05 in the TB and 0.2 in the P region. Considering Technegas particle size, a higher fraction of Technegas aerosols would deposit in the P region for good-quality gamma-camera images [
17].
In the 1990s, Lemb et al. [
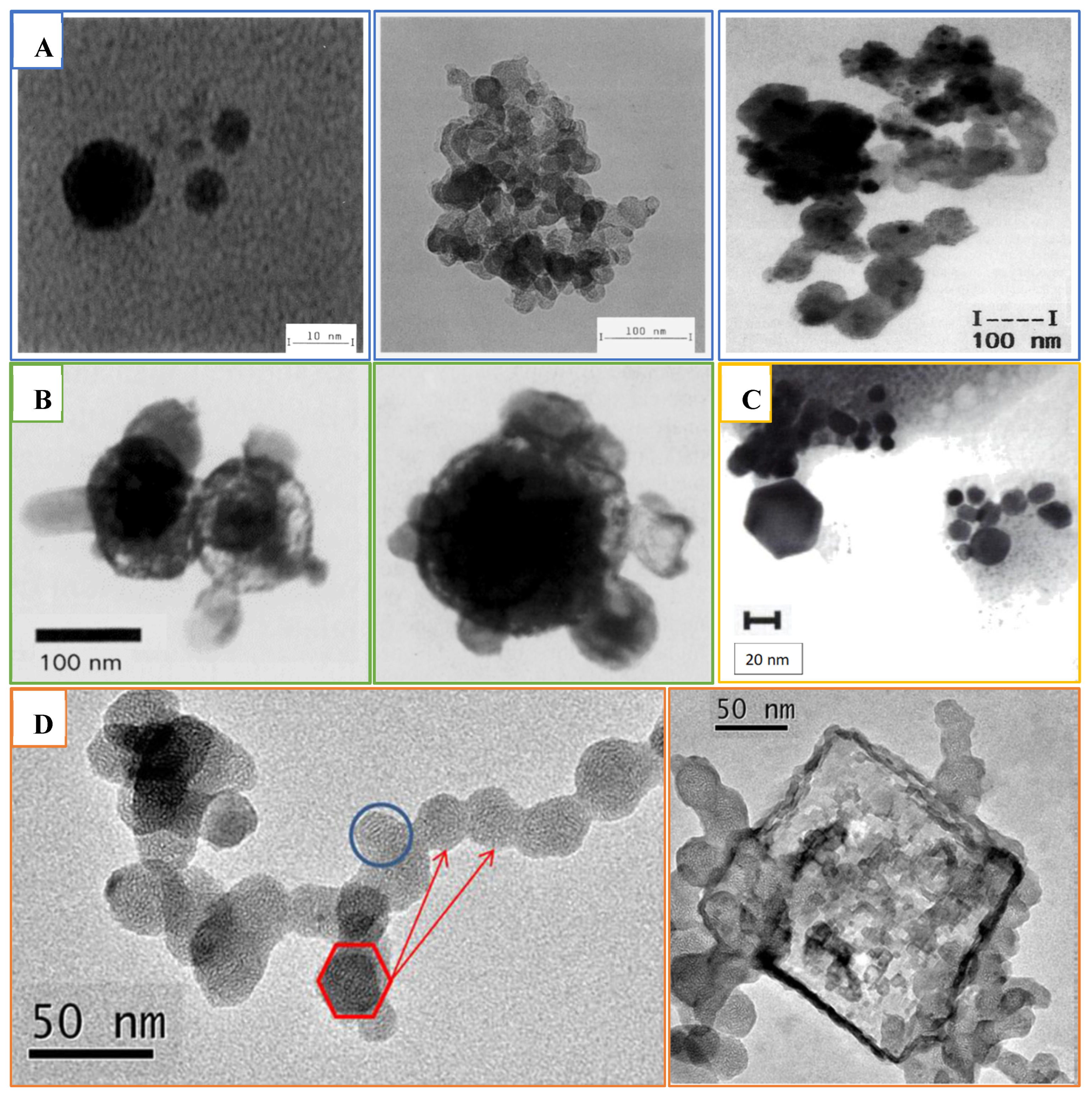
18] evaluated the Technegas particle’s structure and measured its size after passing the gas through two solvents: isopropanol and water. Collected samples were analysed using transmission electron microscopy (TEM), photon correlation spectroscopy (PCS), and time-of-flight mass spectroscopy (TOF-MS). The obtained data revealed Technegas consisting of carbon or graphite particle agglomerates (
Figure 6B) with a size range between 60 and 160 nm. These larger agglomerates were composed of primary particles in a size range between 7 and 23 nm (
Figure 6A). Compared to the original report by Burch et al., Lemb and his colleagues did not detect particles in the 1 nm range. Lemb et al. reported the particles to be hydrophobic and soluble only in organic solvents. Furthermore, in line with Strong and Agnew’s conclusions, Technegas was concluded to be superior to other conventional aerosols used for lung ventilation studies in nuclear medicine. This conclusion was supported by the fact that Technegas particles were of a size around 100 nm with a hydrophobic nature which enhanced size stability in a humid lung atmosphere [
18].
A year following the Lemb et al. publication, Burch et al. questioned the correctness of the Lemb et al. work in a letter to the editor of the
European Journal of Nuclear Medicine [
19]. He explained that Lemb et al.’s findings were suspicious due to inaccurate interpretation of the experiment as well as unsuitable sampling procedures. Burch et al. examined Technegas particles using electron microscopy from the gas stream, while Lemb et al. scanned the extracted particles of Technegas after collection from liquid using TEM. It was proposed that the complicated nature of Technegas particles created pitfalls when studying the physical behaviour of small particles in the nm size range. For instance, Technegas particles would aggregate into larger agglomerates or clusters whenever the particles were brought into close contact to each other.
Lemb et al. rebutted Burch et al.’s claims with support using unpublished results and their historical experience with using Technegas [
19]. They collected TcC particles from a Technegas stream on a TEM grid and examined them on TEM. An average of 20 particles were detected in the TEM images (
Figure 6C), and they were all of a size and structure matching those particles observed by TEM from liquid collection in their previous publication. The collected particles directly from Technegas stream were reported as more representative to what the patient inhales. In accordance with the observed morphology of these aggregates and from observations of other materials evaporated in gas atmospheres, it could be concluded that aggregation occurred in the hot gas zone of produced TcC and not as a result of particle assembly after collection in liquid as proposed by Burch et al.
In 1995, Lloyd et al. studied Technegas and Pertechnegas to investigate factors that may impact Technegas particle size distribution in standard clinical use [
20]. Technegas is produced in an inert argon environment, while Pertechnegas requires an oxygen/argon mixture to produce technetium oxides. As with the Strong and Agnew study, Llyod et al. used a diffusion battery for measurement of the aerosol particle size; however, they included a primary impactor stage to remove 500 nm particulates. The activity size distribution of both Technegas and Pertechnegas was similar and fitted a log-normal distribution. The activity median diameter and GSD were 158 nm and 1.5 for Technegas, while 167 nm and 1.6 was recorded for Pertechnegas. Consequently, the difference in their physiological behaviour could be related to differences in their chemical nature or composition and not attributed to their physical properties. Hence, it was likely that both gases would have similar distributions after lung deposition.
In contrast to Burch et al., Lloyd et al. reported that only 1% of the total radioactivity was within particles of the size ≤ 5 nm. Furthermore, in general, the particle size was similar to that reported by Lemb et al. and, for aggregates, the findings of Strong and Agnew. Interestingly, aerosol aging was reported at 8.5 min with an observed increase in activity median diameter from 158 to 225 nm. This difference was attributed to the method setup and the inclusion of an impactor stage in the Lloyd et al. study. Additionally, it was reported that particle size increased in response to the number of simmers used, with activity median diameters of 158, 167, and 194 nm being reported for 1, 2, and 3 simmers, respectively. This was explained to be due to an increase in salt content over multiple simmers and was confirmed by conducting a low salt vehicle study in which the activity median diameter was 102 nm. Furthermore, TEM analysis (
Figure 6D,E) of particles collected onto copper grids directly from a stream of Technegas showed the presence of agglomerations with total dimensions between 100 and 300 nm, correlating well with previous findings.
A geometrical description of Technegas particles was reported in 1997 by Senden et al. by sampling the Technegas particles using electrostatic precipitation [
22]. The TEM images showed metallic technetium encapsulated within a layered graphite or carbon matrix in near-perfect hexagonally shaped platelets (
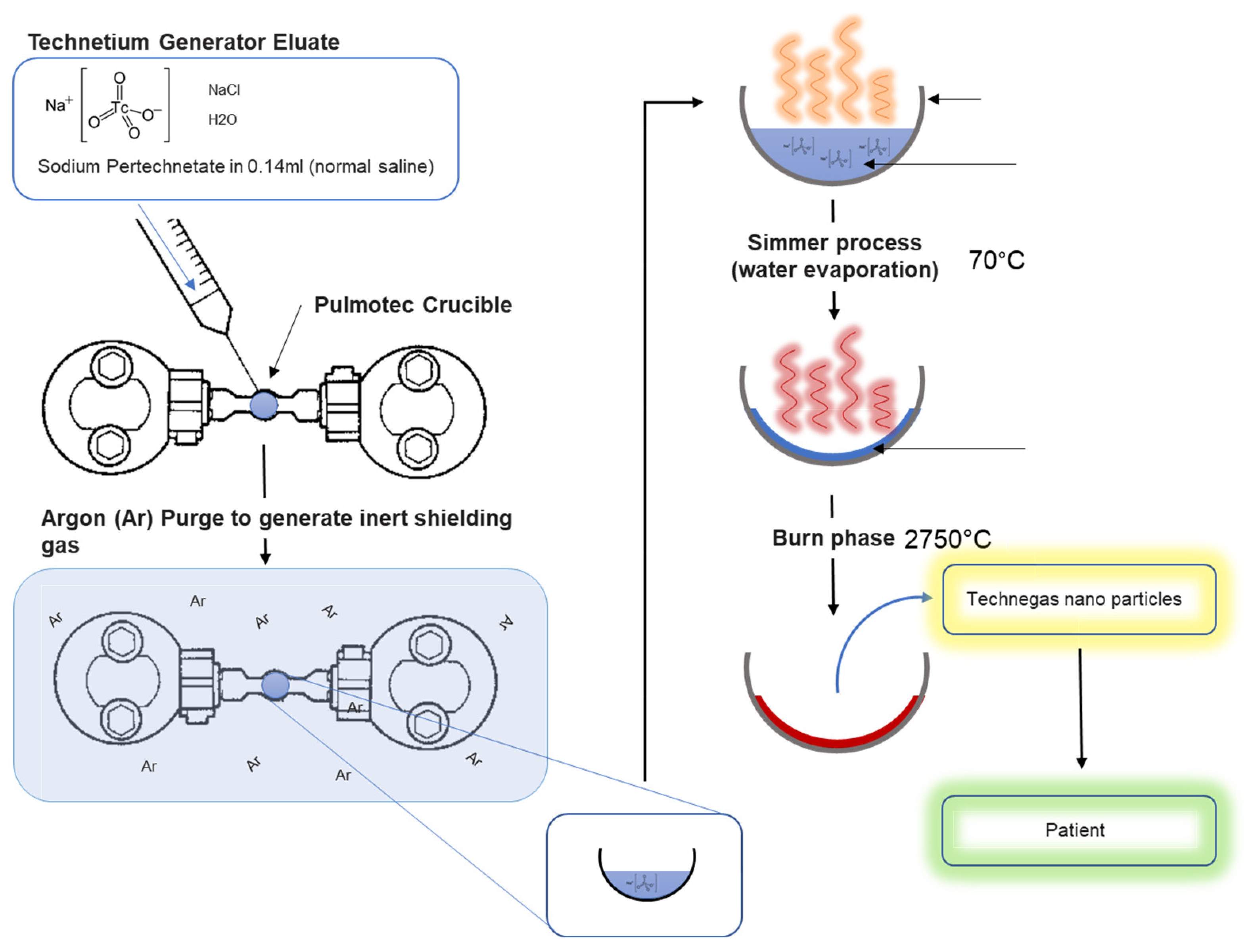
Figure 6F). The average particle size of 80% of the particles was below 100 nm, with a particle width of around 30–60 nm and thickness around 5 nm. Most of these platelets had a thickness to diameter ratio of about 1:10. A possible controlling factor for changes in particle size is the rate of cooling (
Figure 5). It was proposed that during the vapor condensation step a drop in temperature of only 300 °C would limit the collisions within the vapour phase, limiting particle growth [
7].
More recently, Blanc-Béguin et al. compared the physical properties of carbon nanoparticles labelled with either
68Ga or
99mTc prepared using a Technegas generator following the standard clinical procedure [
21]. Collection was achieved using an airborne aerosol sampler with collection on filters or TEM grids. TEM images revealed the presence of large secondary clusters or agglomerated hexagonally structured primary particles (
Figure 6G). Both showed a layered structure, implying that gallium or technetium were covered with a layer of graphite positioned in parallel to their surfaces. The primary particle size was close for both types of aerosols, with a primary mean diameter of 20.9 ± 7.2 nm and 19.8 ± 11.7 nm for
99mTc-labelled and
68Zn-labelled (decayed Ga) carbon nanoparticles, respectively. These data are comparable to the previously reported particle size of
99Tc-labelled carbon nanoparticles, which suggests ultrafine particles for both nanoparticles. In this study, NaCl crystals (
Figure 6H) were also observed in the TEM images of carbon nanoparticles in the shape of quadratic crystals [
21].
3.2. Limitations of Particle Size Distribution Analysis and Application of Cascade Impaction
As discussed previously, numerous methods have been used to assess the particle size and size distribution of Technegas, with each having advantages and disadvantages. The three common approaches are (1) collection in liquid by passing the air stream through a suitable chamber, (2) collection from the chamber via sedimentation, and (3) collection from the generator output by sampling the air stream directly. The latter method can be subclassified into (a) ‘whole’ air sampling (i.e., collection of a representative sample on a filter or sample grid) and (b) size classification apparatuses that separate out particle size distributions through filtration.
Examples of liquid extraction processes include the work by Lemb et al. in which Technegas particles were collected by passing the output stream through aqueous or nonaqueous solvents before subsampling [
18]. Examples of collection via sedimentation include the work by Jackson et al., who collected samples on a stainless-steel probe or copper SEM grid mounted inside the main chamber [
23]. Similarly, Isawa et al. placed holey carbon films (or colloidion films) directly into the chamber and collected after sedimentation for 1 day [
24,
25]. In terms of whole air sampling, Blanc-Béguin F. et al. collected aerosol directly from the exit inhalation tubing using an aerosol collector.
As all the above methods collect the whole aerosol on solid substrates (with the exemption of the liquid capture method), subsequent particle size distributions must then generally be evaluated using microscopy and image analysis techniques. This generates issues with ensuring that sampling is representative, since the number of particles evaluated will be only a tiny fraction of that produced. Furthermore, collection in liquids (or resuspension of filtered samples in liquids) can be subsampled for laser scattering methods; however, care needs to be taken to ensure that aggregation or segregation does not occur due to Van der Waals, DLVO, and surface tension forces that would give a sample bias different from the Technegas properties in air.
Size classification through filtration overcomes the aforementioned issues as it samples the whole aerosol and classifies it through filtration or impaction. Lloyd et al. is a good example of the filtration approach, where they reported the particle size of Technegas using a diffusion battery [
20]. The diffusion battery works on the principle of filtration (tortuosity) of the particles as they pass through filters with different particle size capture efficiency. In the case of Lemb et al., these covered a range of 5–500 nm with a final wool filter stage and primary impaction stage to remove everything greater than 500. Particle size in this system can be determined by measuring the radioactivity on each screen. Lloyd et al. used a serial diffusion setup; however, this can also be assembled in a parallel configuration as in the earlier work by Strong and Agnew [
17] (
Figure 7).
As with all methods, the diffusion battery also has limitations. First, the equipment will only produce radioactive particle size since the resulting particles are generally analysed using a gamma counter. Second, particles are measured in terms of filter porosity and not aerodynamic diameter (the latter being more useful when assessing respiratory deposition). Third, such techniques make it difficult to conduct subsequent image or chemical analysis since collection from the screens has analytical challenges.
One approach to overcome the sampling issues encountered in the above methods is to use cascade impaction. Cascade impaction is an industry standard for testing therapeutic aerosols, and the United States Pharmacopeia Chapter <601> establishes methods, validation requirements, and apparatuses that can be used for routine quality control. Cascade impactors work by inertial impaction and classify an aerosol onto a series of stacked plates by passing the air stream through a series of jets with decreasing size. Pharmaceutical impactors are not suitable for evaluating Technegas, since they are designed for conventional nebulisers, metered dose, and dry powder inhalers that have much higher particle sizes (ca. 1000–6000 nm). Low-pressure impactors work on the same principle, and there are commercial systems designed for evaluating submicron particulates, including environmental pollution and carbonous exhaust particulates for the automotive industry. The electrical low-pressure impactor (ELPI) is one such device.
3.2.1. Application of the Electrical Low-Pressure Impactor to Evaluate Technegas Particle Size
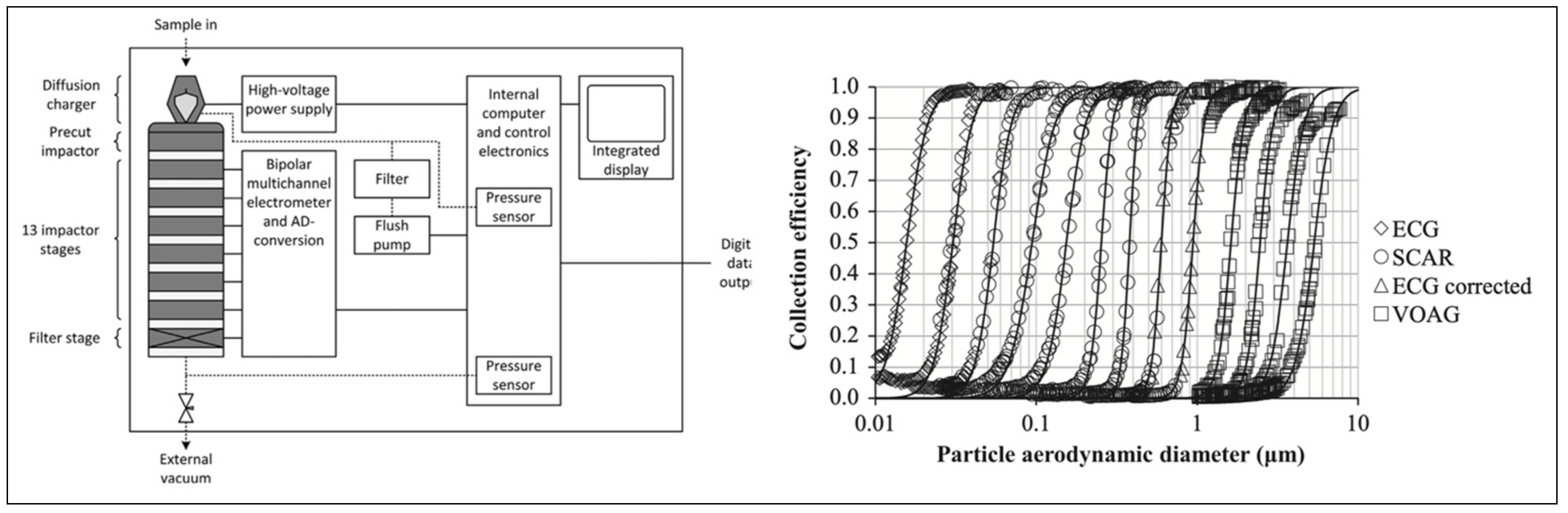
The electrical low-pressure impactor allows measurement of real-time particle size distribution and concentration across a wide size range suitable for evaluating Technegas. The current ELPI (ELPI+, DEKATI, Finland) has a working range of 6–10,000 nm and collects data at a rate of 10,000 measurements per second.
In simple terms, the equipment works by charging an incoming aerosol and then measures the electrostatic charge as particles deposit on each impaction stage. With a knowledge of the cut-off diameter of a given stage and the charge measured, it becomes possible to report the aerodynamic size distribution in real time. Furthermore, particles deposited on each stage may be collected for radioactive or chemical quantitation, allowing the measurement of aerodynamic radioactive or chemical distributions as well as being available for collection for microscopic analysis. A schematic of the operating principles of the ELPI and particle size distributions on each stage from calibration data is shown in
Figure 8 [
26].
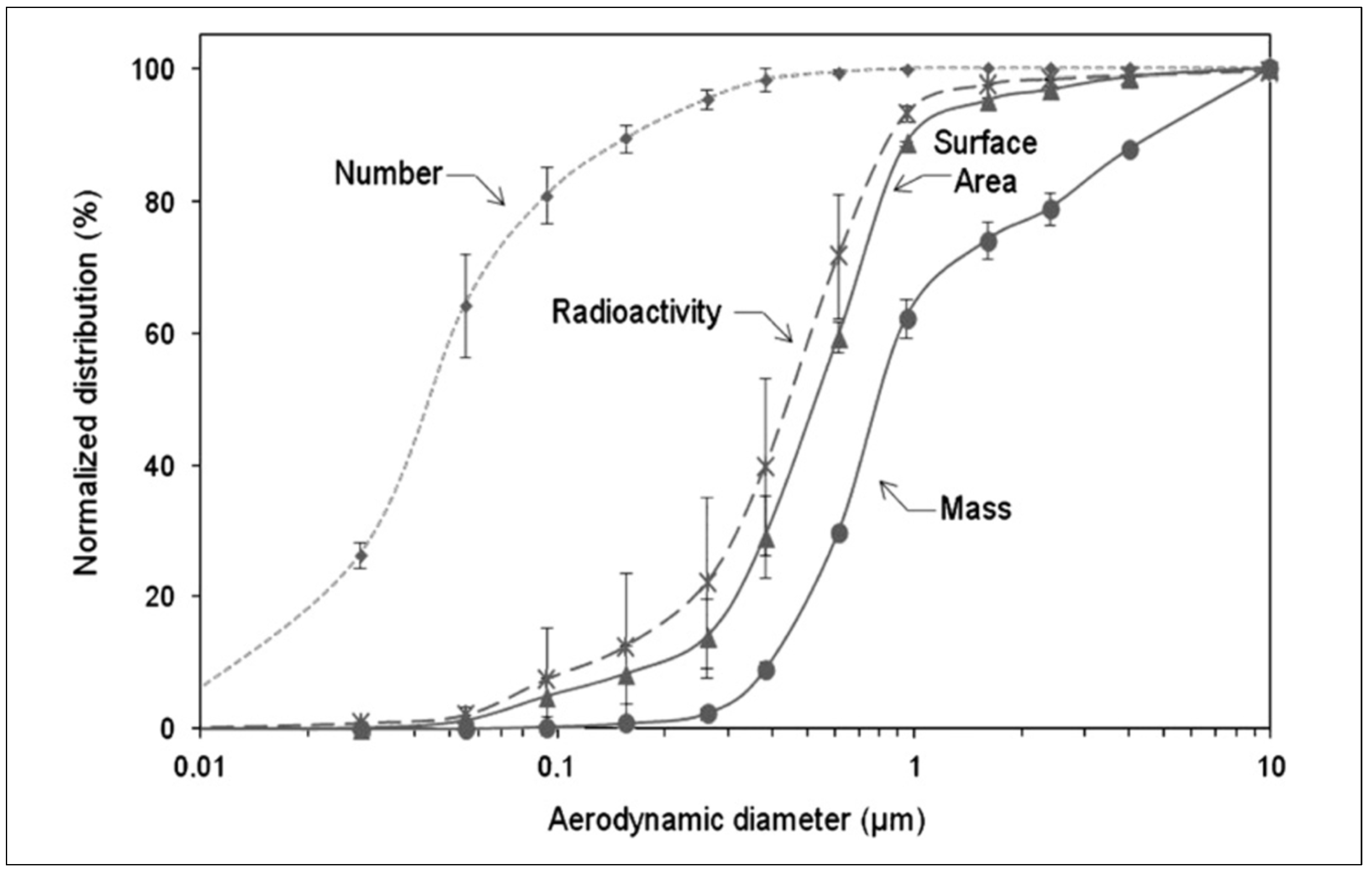
Pourchez et al. utilised the ELPI in combination with a gamma camera to determine the radioactivity aerodynamic diameter as well as the particle size distribution by weight, number, surface area, and radioactivity of Technegas [
27]. With the capability to measure both the aerodynamic mass and aerodynamic radioactivity, it becomes possible to deconvolute the contributions of different components of the formulation to the inhaled particle size of Technegas. For example, using the conventional clinical settings and sodium pertechnetate saline solution, a plot of mass, radioactivity surface area, and particle number as a function of aerodynamic diameter shows stark differences (
Figure 9).
In general, Pourchez et al. found that the mass median aerodynamic diameter (MMAD) (820 nm) of Technegas was significantly higher (20×) than the activity aerodynamic diameter (AMAD) (450 nm). This finding corresponded to half of the overall mass and could be attributed to the high number of nanoparticles with significant radioactivity. Furthermore, the higher MMAD when compared to AMAD could be attributed to larger sodium chloride particles generated from the saline component that had negligible radioactivity. In this landmark paper, Pourchez et al. additionally studied the impact of simmer time, burn time, burn temperature, and residency time using this technique [
27].
3.2.2. Chronology of Particle Size Studies, Methodology, and Findings
A summary of Technegas sampling approaches, particle size analysis methodology, and findings over the years is outlined in
Table 1.
It is interesting to note that while the diameter of Technegas has numerous reported values, historical measurements were collected using a multitude of different techniques that yield different size descriptors. These include geometric diameter, volume diameter, aerodynamic diameter, and aerodynamic activity diameter. Furthermore, some of the historical studies investigate the aerosolized Technegas in its agglomerated inhaled form, while others investigate the size of the primary particles. Importantly, throughout all these studies, the particle diameter of Technegas was reported as less than 1 µm, and the activity aerodynamic diameter <500 nm. Given that the analysis of the Technegas particle has repeatedly been demonstrated to be under 1 µm, the ultimate deposition of the radiopharmaceutical in the periphery of the lung at the alveoli level makes it a strong indicator for functional ventilation imaging [
28].
To date, the ELPI appears to be the most appropriate technique for sampling Technegas aerosols for particle size measurement. The device can measure particle count, surface area, and aerodynamic mass in real time as well as be used to quantify chemical or radioactive mass distributions on each stage. Furthermore, the ability to collect samples directly from individual impactor stages enables additional opportunities for microscopy and surface analysis.
3.3. Composition
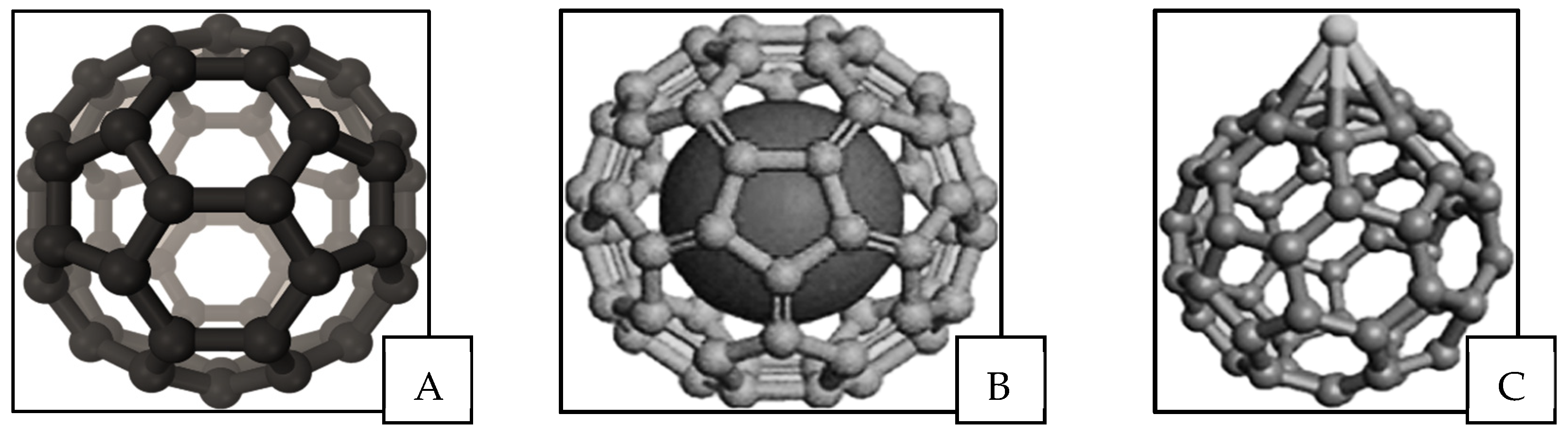
Technegas particle composition and structure have been described using different assumptions and techniques over the years. In the early 1990s, Mackey et al. used a gamma camera to capture momentary dynamic creation of Technegas at the evaporation stage from the graphite crucible [
29]. It was observed that Technegas was generated in a pulse-like nature at a temperature of around 2500 °C with a threshold for generation of around 2250 °C. The vaporisation of
99mTc atoms as well as the crystalline graphitic layers of the crucible occur simultaneously, and it was proposed that
99mTc could incorporate into fullerenes. The presence of buckminsterfullerene (
Figure 10A) and other fullerenes was confirmed by Mackey et al. after analysing the gas using negative-ion laser desorption Fourier transform mass spectrometry by collecting it as a film on a stainless-steel substrate. It was proposed that fullerene structures formed in the process of generating the Technegas can transform into metallofullerenes due to a technetium atom being attached to the fullerene either in endohedral (
Figure 10B) or exohedral form (
Figure 10C) [
29]. Interestingly, Mackay et al. discussed the previous work of Lemb et al., highlighting that they reported agglomerated particles at 97 nm and primary particles at 10 nm, noting that a C
60 fullerene has a diameter of 0.7 nm. This is interesting since it does not address whether the primary particles reported by Lemb et al. contain fullerenes or that fullerenes are present but undetectable using conventional size techniques. In addition, Mackey et al. reported that the purity of argon gas used had an observable impact on the nature of the produced gas. For instance, the use of argon gas with a 3% oxygen during the gas generation process led to the production of a chemically different ventilation agent, Pertechnegas. In the Pertechnegas, no fullerene ions were found with mass spectrometry showing a range of technetium metal oxides [
29].
Lloyd et al. suggested that the mechanism of formation could not be purely the aggregation of fullerenes since the final particle size was also dependent on salt concentration [
20]. They proposed the formation of a vapourised salt aerosol during the temperature ramp followed by condensation of carbon around these molecules to form nucleation centres for generation of Technegas. Therefore, a high salt content would produce a high number of primary particles, which leads to a higher coagulation rate and larger agglomerated particles. Lloyd et al. went on to use this theory to explain why Technegas differs clinically from Pertechnegas. When oxygen is present, the interaction with carbon vapor hinders coagulating of carbon around the salt nuclei. This allows the formation of a soluble
99mTc-labelled salt aerosol lacking a protective outer carbon layer. This protective outer carbon layer in Technegas gives it a hydrophobic property which leads to slower clearance when imaging [
20].
Isawa et al. reported the structures of Technegas by collecting sedimented particles from a generator [
24]. Importantly, they reported hexagonal structures for technetium metal with two distinct types of particles. On rare occasions, particles that resembled carbon nanocapsules were observed; however, more often, crystals with a boundary halo consisting of amorphous carbon was seen. Interestingly, Isawa et al. reported that carbon films present on Technegas were not present on Pertechnegas, indicating that while particle size remained similar, the presence of carbon films drove the difference in clinical properties as highlighted by Lloyd. Isawa et al. also evaluated particle size by SEM. In their analysis, the team reported two size distributions of ~5 nm and larger spherical particles of ~50 nm. The larger particles were reported as being NaCl; however, there was no indication how this was identified or why these had not crystalised into a standard cubic structure [
24].
Llyod et al. questioned both the size analysis and methodology underpinning this study [
25] since particle sizing was conducted on limited particles after sedimentation and measured in terms of physical diameter rather than activity diameter (which would consider volume). Interestingly, Isawa rebutted Lloyd et al.’s letter to the editor but also stated that samples were left overnight before sampling [
25], potentially impacting the properties of the resulting particles (particularly the hydroscopic salt).
During the same period, Jackson et al. used scintigraphic methods including X-ray photoelectron spectroscopy (XPS) and scanning transmission electron microscopy (STEM) coupled energy dispersion X-ray analysis (EDS) to study the chemisorption of pertechnetate on graphite [
23]. In general, they reported Technegas to be either (TcO
2)n or (TcO
2)n bound to carbon nanoparticles exohedrally in a fullerene structure. In addition, the chemical form of technetium in the crucible residue was found to differ from that detected in the aerosol particles. Jackson et al. reported the size of
99mTc-containing particles to be 10 and 80 nm, which agreed with the results of Lemb et al. and others; however, EDS from Technegas particle measurements varied from those obtained by other researchers in terms of carbon signal related to the carbon particles’ encapsulation of metals.
Senden et al. [
7] proposed the native metal was the main composition of the primary Technegas particles with no presence of oxides or hydroxides. This finding confirmed Fawdry and Gruenewald’s assumptions of the impossibility of Technegas aerosol to contain technetium oxides due to the high temperature used in the generation process. Therefore, volatile species (e.g., Tc
2O
7, TcO
2, and NaTcO
4) would be eliminated, and technetium halides are unlikely to form. They suggested elemental technetium and technetium carbide as the main forms of technetium under the furnace production conditions [
9].
During analysis, Senden et al. reported near-perfect hexagonal platelets, which would be consistent with the hexagonal closed lattice for technetium. Furthermore, the team found no evidence of a body-cantered cubic phase for TcC in the resulting aerosol and, instead, a layer of partially ordered graphite coating the surface of the technetium platelets, effectively encapsulating the metal crystal in carbon. Additional studies of crucible residues revealed the crucible interior had technetium-rich particles of 500 nm, composed only of technetium and carbon. The overall structure of these residues was technetium-rich spheres enveloped by equal quantities of carbon, technetium metal, and TcC. Senden et al. concluded that salt played no role in the growth of the primary Technegas particles due to no significant activity observed at the NaCl evaporation temperatures. Furthermore, they concluded that the lack of TcC in the resulting aerosol may potentially be due to decomposition. Lastly, the Senden et al. study discussed the fullerene model proposed by Mackey. They concluded that the vast majority of Technegas aerosol could be accounted for as hexagonal platelets, meaning that for a fullerene species to be the active species, it would have to exist in populations around a million times the number of observed platelets. Furthermore, the conditions for fullerene production were far from optimal in such a generator; in fact, it could be proposed that the carbon film is actually a mesoscopic fullerene structure present on the platelet surface [
7].
Jackson et al. in 1998 commented on Senden et al.’s work, drawing from several literature sources to suggest that the carbon-coated crystals were not the only species present within Technegas. For instance, Jackson highlighted the Isawa publication in which two species were reported. Additionally, Jackson et al. drew on other literature that studied mid-transition metals and the formation of small nanometre crystallites that acted as templates for carbon nucleation and growth while larger crystals were coated in the manner suggested by Senden et al. [
30]. In response to Jackson et al., Senden et al. reasserted their proposal that the main radiotracer species in Technegas is crystalline technetium metal in a nanometric-size range encapsulated by graphitic carbon layers. Senden et al. indicated that many of the cited works in the Jackson et al. letter to the editor studied carbon encapsulation through completely different methodologies and conditions to that in a Technegas generator (in some cases using temperatures surpassing 4000 °C, introducing ionization processes). Senden et al. also asserted that the suggested link between particle size and encapsulation was invalid since the encapsulation process would be independent of size and would be a simple matter of surface thermodynamics. In simple terms, they proposed that the high surface energy metal condensate would be lowered by the presence of carbon molecule attachment. Since the metal cannot react with the carbon, the two phases would stay separate, and the carbon would form a skin around the metal crystallite. [
30].
In a trial that estimated the radioactivity of the primary Technegas particles, Blanc-Beguin et al. reported that a percentage of more than 80.5% recovered radioactivity was attributed to particles with a size of < 80 nm. Therefore, it was concluded that the generated primary carbon nanoparticles were composed of radioactive metal with a diameter of less than 80 nm [
21].
3.4. Pertechnegas and Technegas
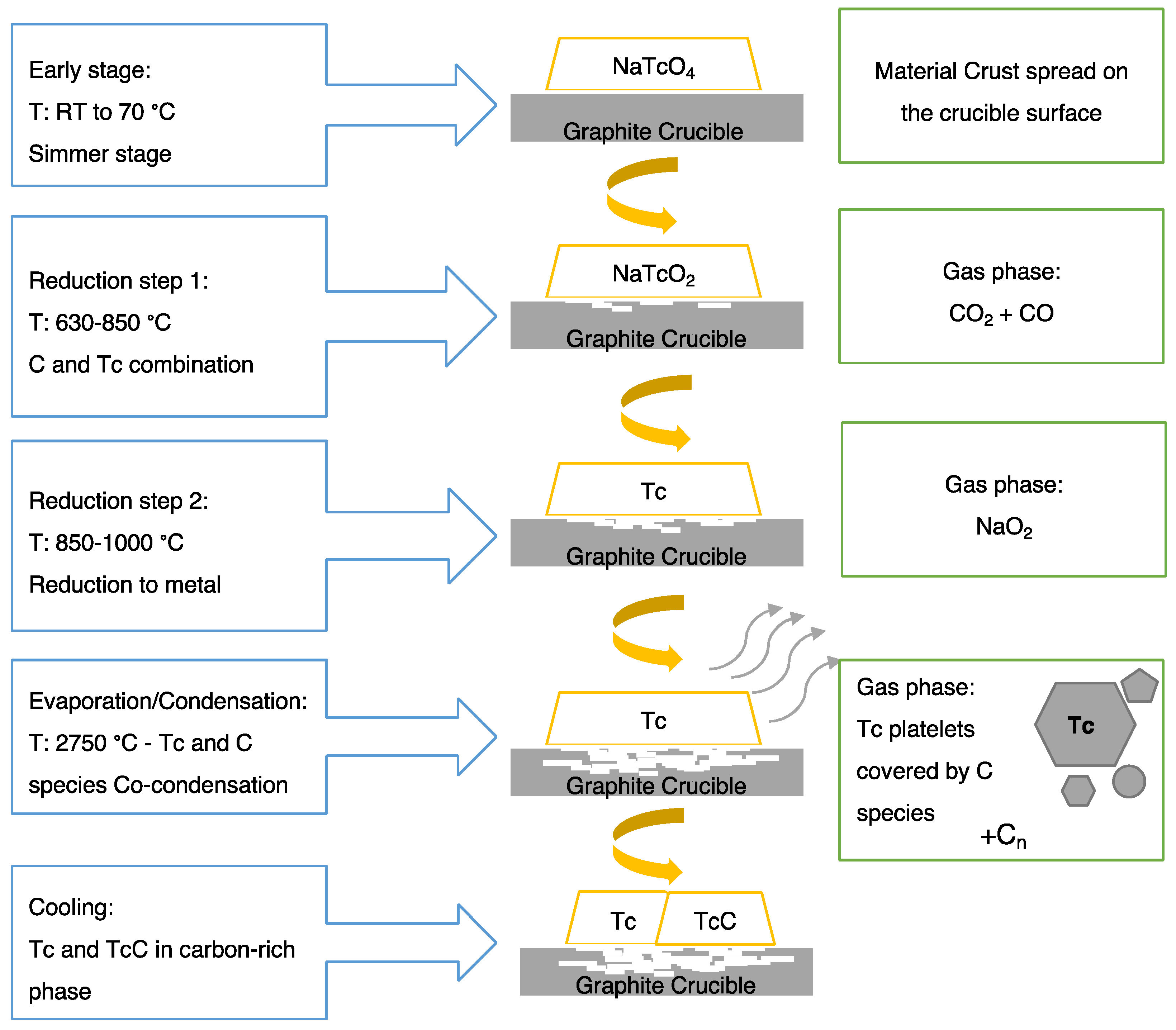
As previously discussed, Technegas forms in an inert argon environment, while Pertechnegas forms in the presence of oxygen (in an argon/oxygen mix). The differences between Technegas and Pertechnegas in terms of formation conditions and composition were studied by Scalzetti and Gagne in 1995 using thin-layer chromatography (TLC) [
31]. The study assessed the behaviour changes of the generated gas as a function of the level of oxygen in an argon–oxygen mixture and monitored the transition between Technegas, Pertechnegas, and other related radioaerosols at different oxygen concentrations. An abrupt transition from Technegas into Pertechnegas was observed between 0.1% and 0.2% levels of oxygen. In the presence of pure argon,
99mTc pertechnetate (
99mTcO
4-) heated inside the graphite crucible undergoes reduction. Therefore, the formed mixture contains insoluble metallic technetium and
99mTc carbides along with soluble
99mTcO
2 formed by incomplete reduction of
99mTcO
4− and reverts to that form in an aqueous media. In the presence of small amounts of oxygen in the argon mixture, the vaporized graphite at high temperatures will combine with the oxygen forming carbon monoxide (Co) and carbon dioxide (CO
2). The presence of extreme amounts of oxygen constrains the reduction of
99mTcO
4− into
99mTc carbides and metallic technetium and favours the production of
99mTcO
2 and
99mTcO
4−. Hence, the purity of argon that is suitable to generate Technegas preferably should be above 99.9% [
31].
Another factor affecting the Technegas/Pertechnegas ratio is the operating temperature of the Technegas generator. Burch and Browitt praised Scalzetti and Gagne’s publication that examined the gas phase reaction that accompanies the formation of Technegas and Pertechnegas but additionally highlighted the importance of operating temperature on Technegas that naturally forms by coating the technetium with graphite into micro-aerosol. They found in one set of measurements that the yield of Pertechnegas reduced between 65% and 3% if the operating temperatures were increased from 2475 °C to 2550 °C. Presumably, this is due to an increase in carbon species coating the technetium [
32].

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}