
Therapeutic Drug Monitoring of Vedolizumab in Inflammatory Bowel Disease Patients during Maintenance Treatment—TUMMY Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population and Study Design
2.2. Statistics
2.3. Ethics
3. Results
3.1. Patient Population
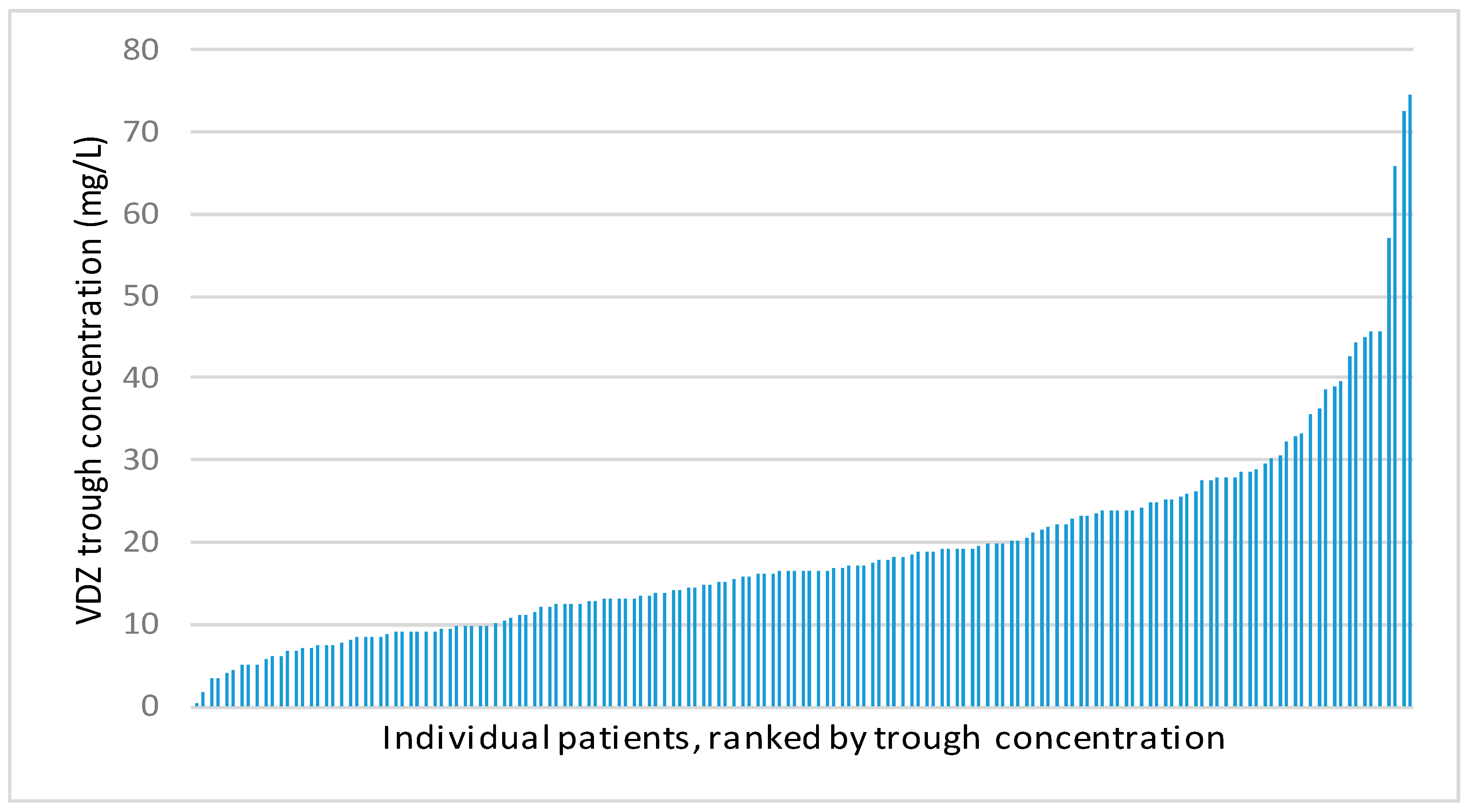
3.2. Vedolizumab Trough Concentrations
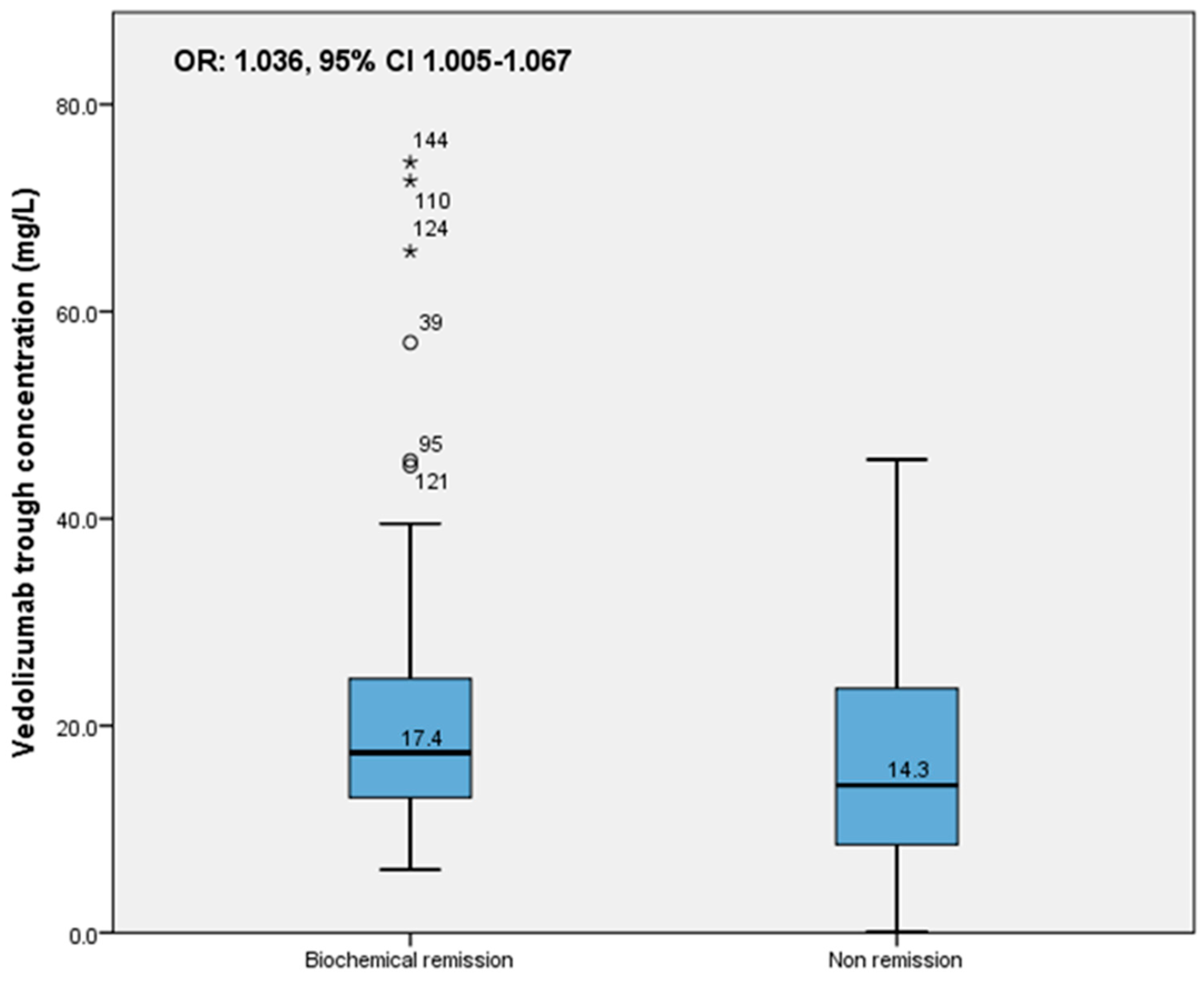
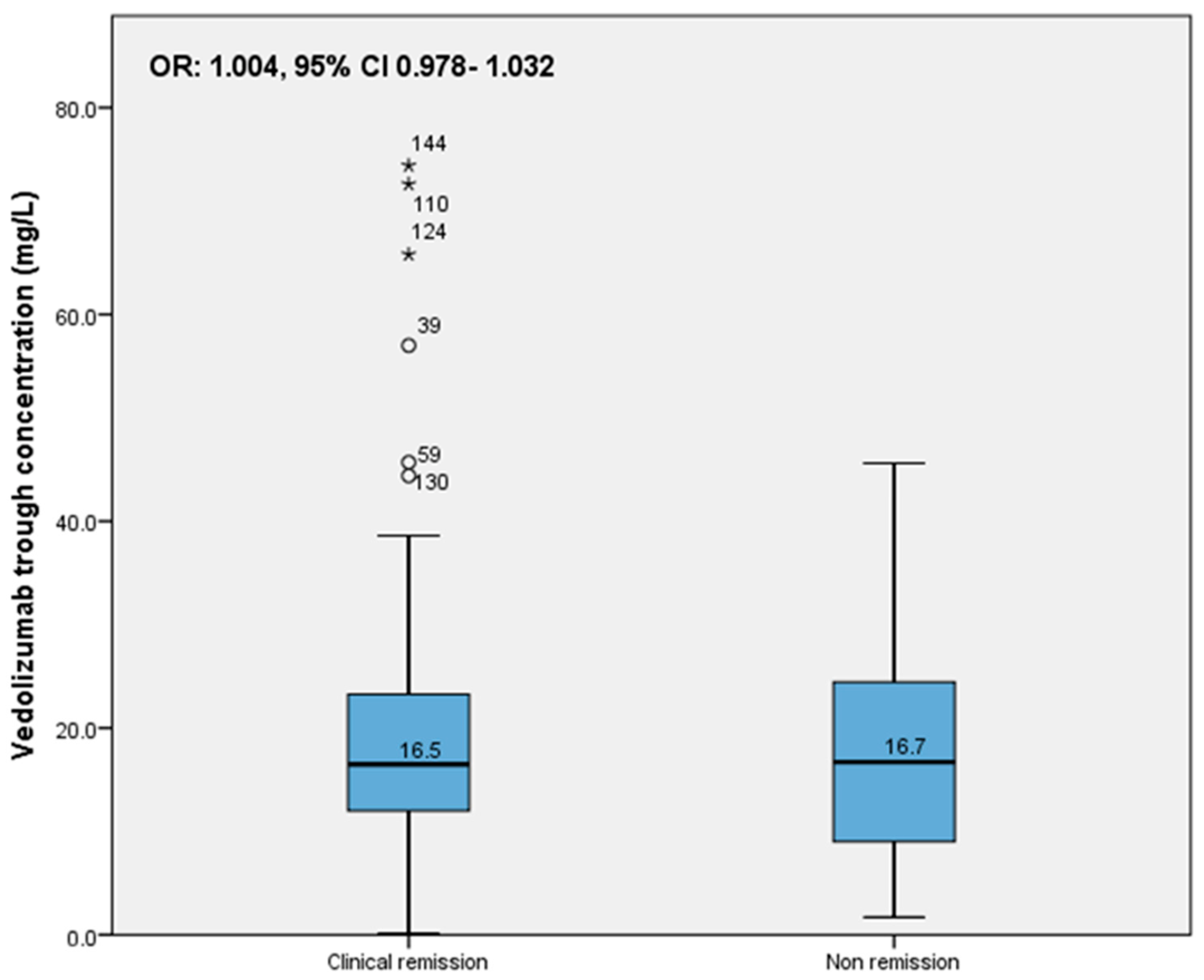
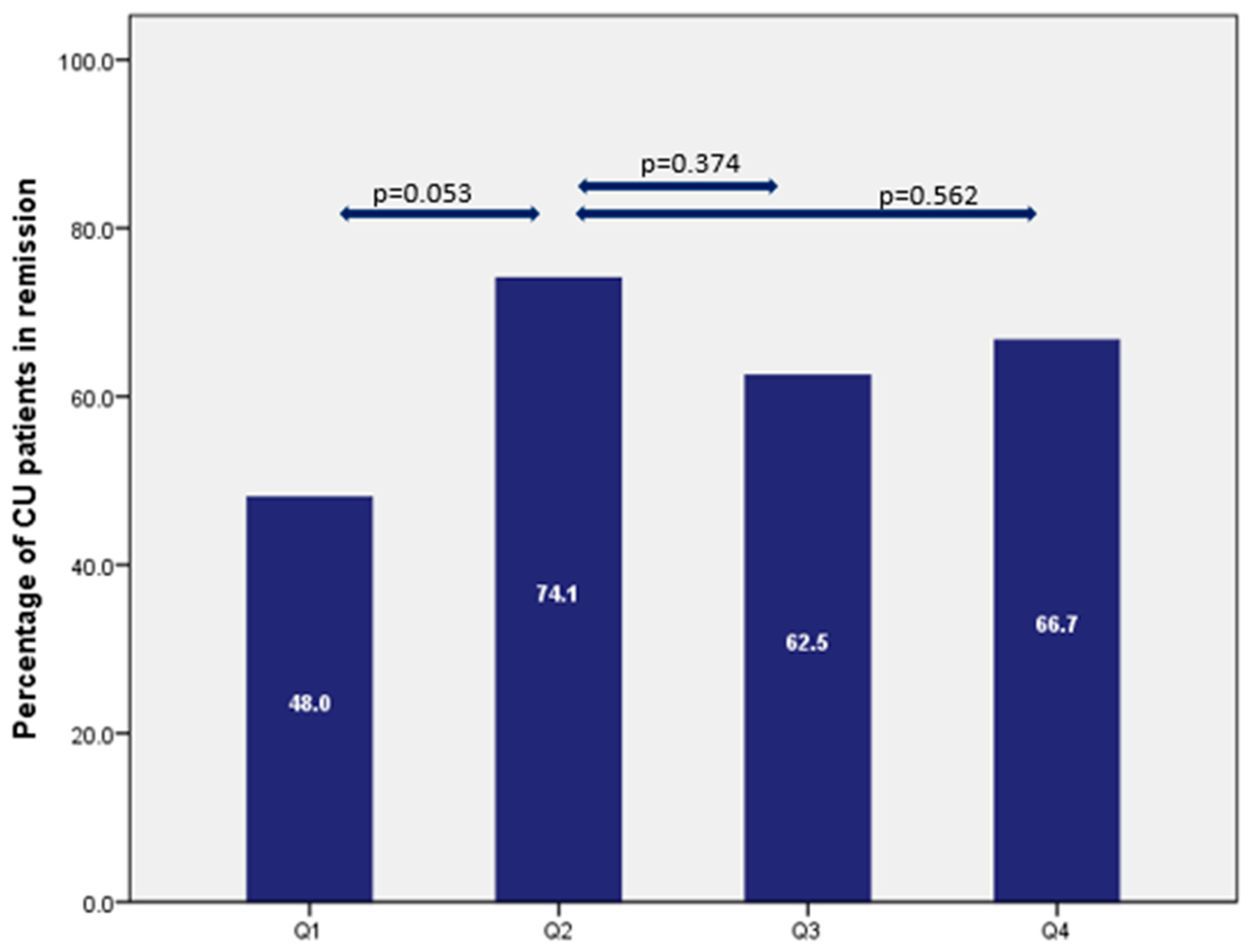
3.3. Clinical and Biochemical Remission and Relationship with Vedolizumab Trough Concentrations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feagan, B.G.; Rutgeerts, P.; Sands, B.E.; Hanauer, S.; Colombel, J.; Sandborn, W.J.; Van Assche, G.; Axler, J.; Kim, H.; Danese, S.; et al. Vedolizumab as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2013, 369, 699–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandborn, W.J.; Feagan, B.G.; Rutgeerts, P.; Hanauer, S.; Colombel, J.; Sands, B.E.; Lukas, M.; Fedorak, R.N.; Lee, S.; Bressler, B.; et al. Vedolizumab as Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2013, 369, 711–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raine, T.; Bonovas, S.; Burisch, J.; Kucharzik, T.; Adamina, M.; Annese, V.; Bachmann, O.; Bettenworth, D.; Chaparro, M.; Czuber-Dochan, W.; et al. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Medical Treatment. J. Crohn’s Colitis 2021, 16, 2–17. [Google Scholar] [CrossRef] [PubMed]
- Derijks, L.J.J.; Wong, D.R.; Hommes, D.W.; van Bodegraven, A.A. Clinical Pharmacokinetic and Pharmacodynamic Considerations in the Treatment of Inflammatory Bowel Disease. Clin. Pharmacokinet. 2018, 57, 1075–1106. [Google Scholar] [CrossRef]
- Rosario, M.; Dirks, N.L.; Gastonguay, M.R.; Fasanmade, A.A.; Wyant, T.; Parikh, A.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Fox, I. Population Pharmacokinetics-Pharmacodynamics of Vedolizumab in Patients with Ulcerative Colitis and Crohn’s Disease. Aliment. Pharm. 2015, 42, 188–202. [Google Scholar] [CrossRef]
- Maser, E.A.; Villela, R.; Silverberg, M.S.; Greenb, G.R. Association of Trough Serum Infliximab to Clinical Outcome After Scheduled Maintenance Treatment for Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2006, 4, 1248–1254. [Google Scholar] [CrossRef]
- Rosario, M.; French, J.L.; Dirks, N.L.; Sankoh, S.; Parikh, A.; Yang, H.; Danese, S.; Colombel, J.; Smyth, M.; Sandborn, W.J.; et al. Exposure-Efficacy Relationships for Vedolizumab Induction Therapy in Patients with Ulcerative Colitis Or Crohn’s Disease. J. Crohn’s Colitis 2017, 11, 921–929. [Google Scholar] [CrossRef] [Green Version]
- Osterman, M.T.; Rosario, M.; Lasch, K.; Barocas, M.; Wilbur, J.D.; Dirks, N.L.; Gastonguay, M.R. Vedolizumab Exposure Levels and Clinical Outcomes in Ulcerative Colitis: Determining the Potential for Dose Optimisation. Aliment. Pharmacol. Ther. 2019, 49, 408–418. [Google Scholar] [CrossRef] [Green Version]
- Dreesen, E.; Verstockt, B.; Bian, S.; de Bruyn, M.; Compernolle, G.; Tops, S.; Noman, M.; Van Assche, G.; Ferrante, M.; Gils, A.; et al. Evidence to Support Monitoring of Vedolizumab Trough Concentrations in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2018, 16, 1937–1946.e8. [Google Scholar] [CrossRef]
- Pouillon, L.; Vermeire, S.; Bossuyt, P. Vedolizumab Trough Level Monitoring in Inflammatory Bowel Disease: A State-of-the-Art Overview. BMC Med. 2019, 17, 89. [Google Scholar] [CrossRef] [Green Version]
- Yacoub, W.; Williet, N.; Pouillon, L.; Di-Bernado, T.; De Carvalho Bittencourt, M.; Nancey, S.; Lopez, A.; Paul, S.; Zallot, C.; Roblin, X.; et al. Early Vedolizumab Trough Levels Predict Mucosal Healing in Inflammatory Bowel Disease: A Multicentre Prospective Observational Study. Aliment. Pharmacol. Ther. 2018, 47, 906–912. [Google Scholar] [CrossRef] [Green Version]
- Schulze, H.; Esters, P.; Hartmann, F.; Stein, J.; Christ, C.; Zorn, M.; Dignass, A. A Prospective Cohort Study to Assess the Relevance of Vedolizumab Drug Level Monitoring in IBD Patients. Scand. J. Gastroenterol. 2018, 53, 670–676. [Google Scholar] [CrossRef]
- Löwenberg, M.; Vermeire, S.; Mostafavi, N.; Hoentjen, F.; Franchimont, D.; Bossuyt, P.; Hindryckx, P.; Rispens, T.; de Vries, A.; van der Woude, C.J.; et al. Vedolizumab Induces Endoscopic and Histologic Remission in Patients with Crohn’s Disease. Gastroenterology 2019, 157, 997–1006.e6. [Google Scholar] [CrossRef] [Green Version]
- Ungaro, R.C.; Yarur, A.; Jossen, J.; Phan, B.L.; Chefitz, E.; Sehgal, P.; Kamal, K.; Bruss, A.; Beniwal-Patel, P.; Fox, C.; et al. Higher Trough Vedolizumab Concentrations during Maintenance Therapy are Associated with Corticosteroid-Free Remission in Inflammatory Bowel Disease. J. Crohn’s Colitis 2019, 13, 963–969. [Google Scholar] [CrossRef]
- Gubatan, J.; Mitsuhashi, S.; Zenlea, T.; Rosenberg, L.; Robson, S.; Moss, A.C. Low Serum Vitamin D during Remission Increases Risk of Clinical Relapse in Patients with Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2017, 15, 240–246.e1. [Google Scholar] [CrossRef] [Green Version]
- Buisson, A.; Mak, W.Y.; Andersen, M.J.; Lei, D.; Kahn, S.A.; Pekow, J.; Cohen, R.D.; Zmeter, N.; Pereira, B.; Rubin, D.T. Faecal Calprotectin is a very Reliable Tool to Predict and Monitor the Risk of Relapse After Therapeutic De-Escalation in Patients with Inflammatory Bowel Diseases. J. Crohn’s Colitis 2019, 13, 1012–1024. [Google Scholar] [CrossRef]
- Vermeire, S.; Schreiber, S.; Sandborn, W.J.; Dubois, C.; Rutgeerts, P. Correlation between the Crohn’s Disease Activity and Harvey-Bradshaw Indices in Assessing Crohn’s Disease Severity. Clin. Gastroenterol. Hepatol. 2010, 8, 357–363. [Google Scholar] [CrossRef]
- Bloem, K.; Schaap, T.; Boshuizen, R.; Kneepkens, E.L.; Wolbink, G.J.; Vries, A.d.; Rispens, T. Capillary Blood Microsampling to Determine Serum Biopharmaceutical Concentration: Mitra(®) Microsampler Vs Dried Blood Spot. Bioanalysis 2018, 10, 815–823. [Google Scholar] [CrossRef]
- Yarur, A.J.; Bruss, A.; Naik, S.; Beniwal-Patel, P.; Fox, C.; Jain, A.; Berens, B.; Patel, A.; Ungaro, R.; Bahur, B.; et al. Vedolizumab Concentrations are Associated with Long-Term Endoscopic Remission in Patients with Inflammatory Bowel Diseases. Dig. Dis. Sci. 2019, 64, 1651–1659. [Google Scholar] [CrossRef]
- Al-Bawardy, B.; Ramos, G.P.; Willrich, M.A.V.; Jenkins, S.M.; Park, S.H.; Aniwan, S.; Schoenoff, S.A.; Bruining, D.H.; Papadakis, K.A.; Raffals, L.; et al. Vedolizumab Drug Level Correlation with Clinical Remission, Biomarker Normalization, and Mucosal Healing in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 580–586. [Google Scholar] [CrossRef]
- Guidi, L.; Pugliese, D.; Tonucci, T.P.; Bertani, L.; Costa, F.; Privitera, G.; Tolusso, B.; Di Mario, C.; Albano, E.; Tapete, G.; et al. Early Vedolizumab Trough Levels Predict Treatment Persistence Over the First Year in Inflammatory Bowel Disease. United Eur. Gastroenterol. J. 2019, 7, 1189–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanžel, J.; Sever, N.; Ferkolj, I.; Štabuc, B.; Smrekar, N.; Kurent, T.; Koželj, M.; Novak, G.; Compernolle, G.; Tops, S.; et al. Early Vedolizumab Trough Levels Predict Combined Endoscopic and Clinical Remission in Inflammatory Bowel Disease. United Eur. Gastroenterol. J. 2019, 7, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Vande Casteele, N.; Sandborn, W.J.; Feagan, B.G.; Vermeire, S.; Dulai, P.S.; Yarur, A.; Roblin, X.; Ben-Horin, S.; Dotan, I.; Osterman, M.T.; et al. Real-World Multicentre Observational Study Including Population Pharmacokinetic Modelling to Evaluate the Exposure-Response Relationship of Vedolizumab in Inflammatory Bowel Disease: ERELATE Study. Aliment. Pharmacol. Ther. 2022, 56, 463–476. [Google Scholar] [CrossRef] [PubMed]
- Williet, N.; Boschetti, G.; Fovet, M.; Di Bernado, T.; Claudez, P.; Del Tedesco, E.; Jarlot, C.; Rinaldi, L.; Berger, A.; Phelip, J.; et al. Association between Low Trough Levels of Vedolizumab during Induction Therapy for Inflammatory Bowel Diseases and Need for Additional Doses within 6 Months. Clin. Gastroenterol. Hepatol. 2017, 15, 1750–1757.e3. [Google Scholar] [CrossRef] [Green Version]
- Dreesen, E.; Gils, A. Blocking α4β7 Integrin through Vedolizumab: Necessary but Not Sufficient? J. Crohn’s Colitis 2017, 11, 903–904. [Google Scholar] [CrossRef] [Green Version]
- Plevris, N.; Jenkinson, P.W.; Chuah, C.S.; Lyons, M.; Merchant, L.M.; Pattenden, R.J.; Arnott, I.D.; Jones, G.R.; Lees, C.W. Association of Trough Vedolizumab Levels with Clinical, Biological and Endoscopic Outcomes during Maintenance Therapy in Inflammatory Bowel Disease. Frontline Gastroenterol. 2020, 11, 117–123. [Google Scholar] [CrossRef]
- Gracie, D.J.; Williams, C.J.M.; Sood, R.; Mumtaz, S.; Bholah, M.H.; Hamlin, P.J.; Ford, A.C. Poor Correlation between Clinical Disease Activity and Mucosal Inflammation, and the Role of Psychological Comorbidity, in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2016, 111, 541–551. [Google Scholar] [CrossRef]
- Sturm, A.; Maaser, C.; Calabrese, E.; Annese, V.; Fiorino, G.; Kucharzik, T.; Vavricka, S.R.; Verstockt, B.; van Rheenen, P.; Tolan, D.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 2: IBD Scores and General Principles and Technical Aspects. J. Crohn’s Colitis 2019, 13, 273–284. [Google Scholar] [CrossRef]
- Sakurai, T.; Saruta, M. Positioning and Usefulness of Biomarkers in Inflammatory Bowel Disease. Digestion 2023, 104, 30–41. [Google Scholar] [CrossRef]
- Pauwels, R.W.M.; Proietti, E.; Van Der Woude, C.J.; Oudijk, L.; Crombag, M.-B.S.; Peppelenbosch, M.P.; Grohmann, U.; Fuhler, G.M.; De Vries, A.C. Vedolizumab Tissue Concentration Correlates to Mucosal Inflammation and Objective Treatment Response in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2021, 27, 1813–1820. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CD | UC | Total | |
|---|---|---|---|
| Number of patients, (n (%)) | 59 (37.1) | 100 (62.9) | 159 |
| Age, mean (SD) | 48 (15.2) | 53 (16.2) | 51 (16.0) |
| Sex (male, n (%)) | 15 (25.4) | 54 (54.0) | 69 (43.4) |
| BMI (kg/m2, median, [IQR]) | 24.7 [21.4–29.4] | 25.6 [23.5–28.3] | 25.3 [23.1–28.6] |
| Disease duration (year, median [IQR]) | 14.0 [10.0–29.0] | 11.8 [5.0–18.0] | 13 [7.0–21.0] |
| Vedolizumab treatment duration (year, median [IQR]) | 2.6 [1.1–5.1] | 2.3 [0.7–4.5] | 2.4 [0.9–4.8] |
| Interval vedolizumab (weeks, median, [range]) | 8 [4–8] | 8 [4–12] | 8 [4–12] |
| Active smoker (n (%)) | 5 (8.5) | 9 (9.0) | 14 (8.8) |
| Prior biological exposure (n (%)) | |||
| 48 (81.4) | 83 (83.0) | 131 (82.4) |
| 10 (16.9) | 1 (1.0) | 11 (6.9) |
| Co-medication (n (%)) | |||
| 4 (6.8) | 16 (16.0) | 20 (12.6) |
| 4 (6.8) | 18 (18.0) | 22 (13.8) |
| 7 (11.9) | 36 (36.0) | 43 (27.0) |
| Clinical remission (n (%)) | 40 (67.8) | 63 (63.0) | 103 (64.8) |
| Nonremission (n (%)) | 19 (32.2) | 37 (37.0) | 56 (35.2) |
| Biochemical remission (n (%)) | 19 (33.9) | 48 (51.6) | 67 (45.0) |
| Nonremission (n (%)) | 37 (66.1) | 45 (48.4) | 82 (55.0) |
| CRP (mg/L, median [IQR]) | 6 [2.0–6.3] | 2.9 [0.98–6.0] | 4 [1.0–6.0] |
| Hemoglobin (mmol/L, median [IQR]) | 8 [8.0–9.0] | 9 [8.0–9.0] | 9 [8.0–9.0] |
| Albumin (g/L, median [IQR]) | 43 [40.0–44.0] | 44 [42.0–46.0] | 44 [41.0–45.0] |
| Fecal calprotectin (mg/kg, median [IQR]) | 58 [24.5–182.5] | 63 [14.0–230.0] | 59 [17.5–215.0] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sivridaş, M.; Creemers, R.H.; Wong, D.R.; Boekema, P.J.; Römkens, T.E.H.; Gilissen, L.P.L.; van Bodegraven, A.A.; Loeff, F.C.; Rispens, T.; Derijks, L.J.J. Therapeutic Drug Monitoring of Vedolizumab in Inflammatory Bowel Disease Patients during Maintenance Treatment—TUMMY Study. Pharmaceutics 2023, 15, 972. https://doi.org/10.3390/pharmaceutics15030972
Sivridaş M, Creemers RH, Wong DR, Boekema PJ, Römkens TEH, Gilissen LPL, van Bodegraven AA, Loeff FC, Rispens T, Derijks LJJ. Therapeutic Drug Monitoring of Vedolizumab in Inflammatory Bowel Disease Patients during Maintenance Treatment—TUMMY Study. Pharmaceutics. 2023; 15(3):972. https://doi.org/10.3390/pharmaceutics15030972
Chicago/Turabian StyleSivridaş, Merve, Rob H. Creemers, Dennis R. Wong, Paul J. Boekema, Tessa E. H. Römkens, Lennard P. L. Gilissen, Adriaan A. van Bodegraven, Floris C. Loeff, Theo Rispens, and Luc J. J. Derijks. 2023. "Therapeutic Drug Monitoring of Vedolizumab in Inflammatory Bowel Disease Patients during Maintenance Treatment—TUMMY Study" Pharmaceutics 15, no. 3: 972. https://doi.org/10.3390/pharmaceutics15030972