
Prognostic and Predictive Value of LIV1 Expression in Early Breast Cancer and by Molecular Subtype
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Breast Cancer Samples and Gene Expression Profiling
2.2. Gene Expression Data Analysis
2.3. Statistical Analysis
3. Results
3.1. Patient Population and LIV1 Expression
3.2. Correlations of LIV1 Expression with Clinicopathological Features
3.3. Correlation with Disease-Free Survival
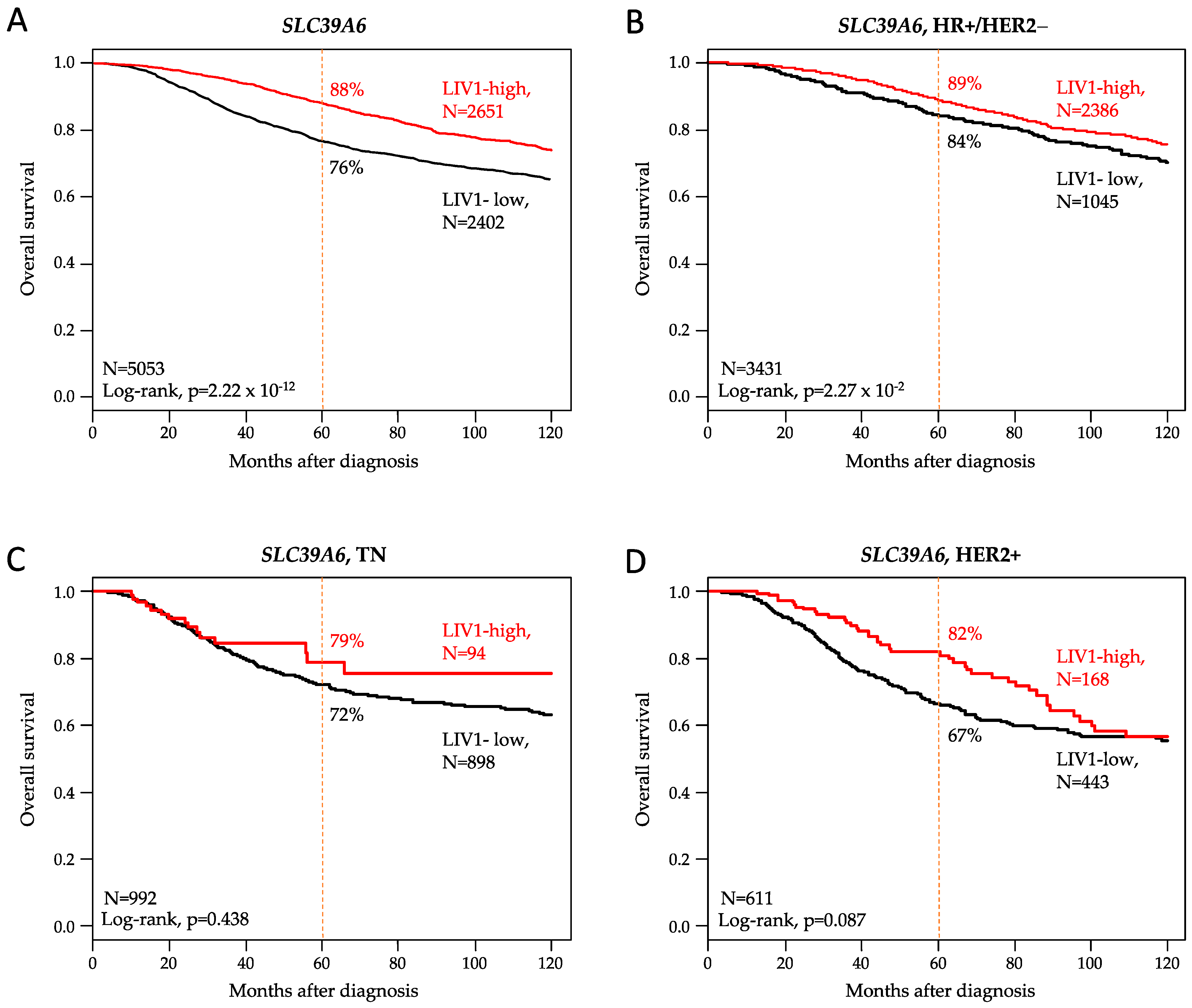
3.4. Correlation with Overall Survival
3.5. Correlation with Pathological Response to Chemotherapy
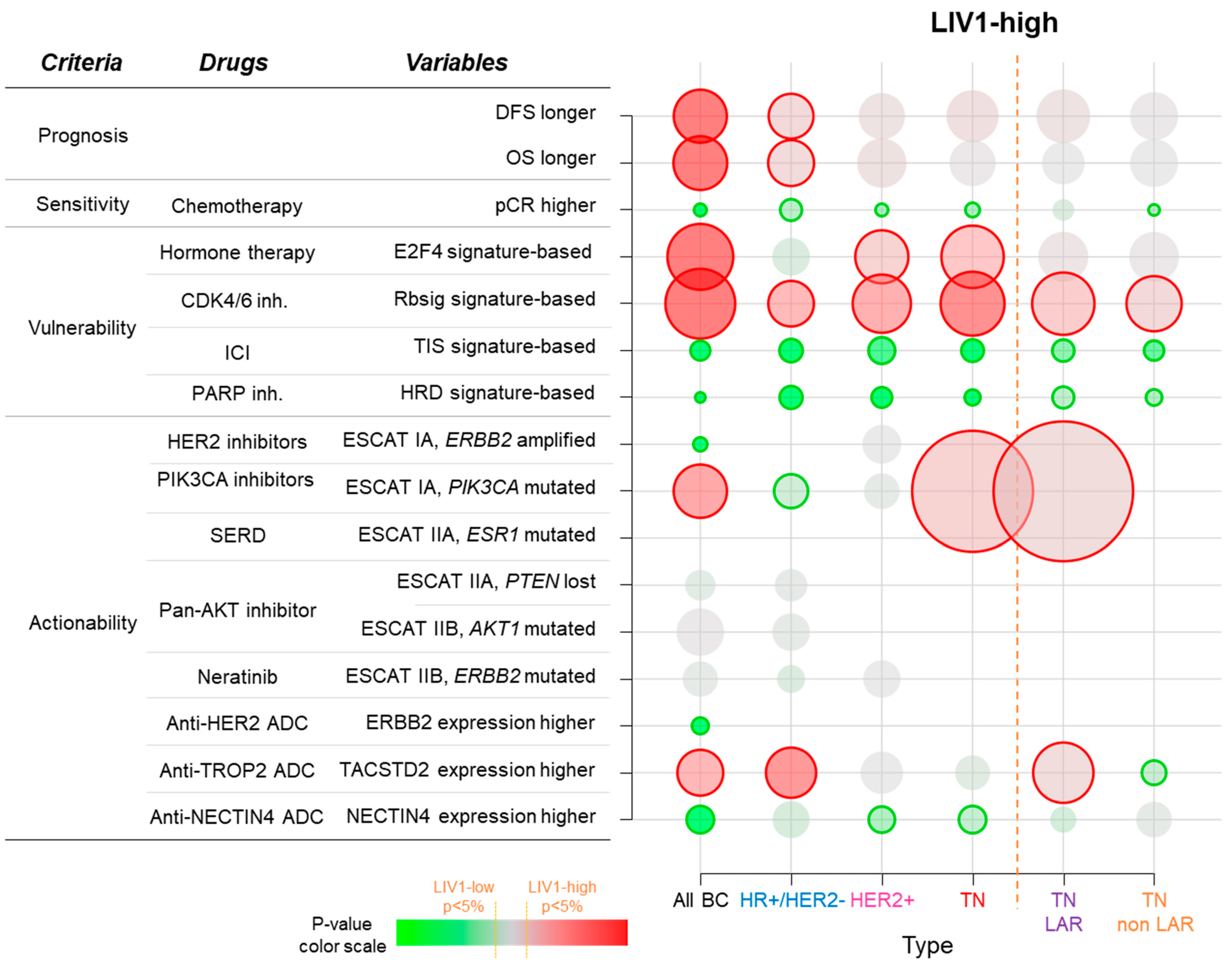
3.6. Correlations with Potential Therapeutic Vulnerability or Actionability
3.7. Analysis of LIV1 Expression in HR+/HER2- Breast Cancers
3.8. Analysis of LIV1 Expression in TN Breast Cancers
3.9. Analysis of LIV1 Expression in HER2+ Breast Cancers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 5). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef]
- Tarantino, P.; Carmagnani Pestana, R.; Corti, C.; Modi, S.; Bardia, A.; Tolaney, S.M.; Cortes, J.; Soria, J.-C.; Curigliano, G. Antibody-Drug Conjugates: Smart Chemotherapy Delivery across Tumor Histologies. CA Cancer J. Clin. 2022, 72, 165–182. [Google Scholar] [CrossRef]
- Corti, C.; Giugliano, F.; Nicolò, E.; Ascione, L.; Curigliano, G. Antibody–Drug Conjugates for the Treatment of Breast Cancer. Cancers 2021, 13, 2898. [Google Scholar] [CrossRef]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.-Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [Green Version]
- Hurvitz, S.A.; Hegg, R.; Chung, W.-P.; Im, S.-A.; Jacot, W.; Ganju, V.; Chiu, J.W.Y.; Xu, B.; Hamilton, E.; Madhusudan, S.; et al. Trastuzumab Deruxtecan versus Trastuzumab Emtansine in Patients with HER2-Positive Metastatic Breast Cancer: Updated Results from DESTINY-Breast03, a Randomised, Open-Label, Phase 3 Trial. Lancet Lond. Engl. 2023, 401, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef]
- de Nonneville, A.; Goncalves, A.; Mamessier, E.; Bertucci, F. Sacituzumab Govitecan in Triple-Negative Breast Cancer. Ann. Transl. Med. 2022, 10, 647. [Google Scholar] [CrossRef] [PubMed]
- Rugo, H.S.; Bardia, A.; Tolaney, S.M.; Arteaga, C.; Cortes, J.; Sohn, J.; Marmé, F.; Hong, Q.; Delaney, R.J.; Hafeez, A.; et al. TROPiCS-02: A Phase III Study Investigating Sacituzumab Govitecan in the Treatment of HR+/HER2- Metastatic Breast Cancer. Future Oncol. Lond. Engl. 2020, 16, 705–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- M-Rabet, M.; Cabaud, O.; Josselin, E.; Finetti, P.; Castellano, R.; Farina, A.; Agavnian-Couquiaud, E.; Saviane, G.; Collette, Y.; Viens, P.; et al. Nectin-4: A New Prognostic Biomarker for Efficient Therapeutic Targeting of Primary and Metastatic Triple-Negative Breast Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 769–776. [Google Scholar] [CrossRef]
- Cabaud, O.; Berger, L.; Crompot, E.; Adélaide, J.; Finetti, P.; Garnier, S.; Guille, A.; Carbuccia, N.; Farina, A.; Agavnian, E.; et al. Overcoming Resistance to Anti-Nectin-4 Antibody-Drug Conjugate. Mol. Cancer Ther. 2022, 21, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Sussman, D.; Smith, L.M.; Anderson, M.E.; Duniho, S.; Hunter, J.H.; Kostner, H.; Miyamoto, J.B.; Nesterova, A.; Westendorf, L.; Van Epps, H.A.; et al. SGN-LIV1A: A Novel Antibody-Drug Conjugate Targeting LIV-1 for the Treatment of Metastatic Breast Cancer. Mol. Cancer Ther. 2014, 13, 2991–3000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolò, E.; Repetto, M.; Boscolo Bielo, L.; Tarantino, P.; Curigliano, G. Antibody-Drug Conjugates in Breast Cancer: What Is Beyond HER2? Cancer J. 2022, 28, 436–445. [Google Scholar] [CrossRef]
- El-Tanani, M.K.K.; Green, C.D. Interaction between Estradiol and CAMP in the Regulation of Specific Gene Expression. Mol. Cell. Endocrinol. 1996, 124, 71–77. [Google Scholar] [CrossRef]
- Frasor, J.; Stossi, F.; Danes, J.M.; Komm, B.; Lyttle, C.R.; Katzenellenbogen, B.S. Selective Estrogen Receptor Modulators: Discrimination of Agonistic versus Antagonistic Activities by Gene Expression Profiling in Breast Cancer Cells. Cancer Res. 2004, 64, 1522–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaither, L.A.; Eide, D.J. Eukaryotic Zinc Transporters and Their Regulation. Biometals Int. J. Role Met. Ions Biol. Biochem. Med. 2001, 14, 251–270. [Google Scholar] [CrossRef]
- Taylor, K.M. The LIV-1 Subfamily of Zinc Transporters: From Origins to Present Day Discoveries. Int. J. Mol. Sci. 2023, 24, 1255. [Google Scholar] [CrossRef]
- Rozenberg, J.M.; Kamynina, M.; Sorokin, M.; Zolotovskaia, M.; Koroleva, E.; Kremenchutckaya, K.; Gudkov, A.; Buzdin, A.; Borisov, N. The Role of the Metabolism of Zinc and Manganese Ions in Human Cancerogenesis. Biomedicines 2022, 10, 1072. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, H.; Xu, Z.; Cheng, X. Zinc Dysregulation in Cancers and Its Potential as a Therapeutic Target. Cancer Biol. Med. 2020, 17, 612–625. [Google Scholar] [CrossRef] [PubMed]
- Hogstrand, C.; Kille, P.; Ackland, M.L.; Hiscox, S.; Taylor, K.M. A Mechanism for Epithelial-Mesenchymal Transition and Anoikis Resistance in Breast Cancer Triggered by Zinc Channel ZIP6 and STAT3 (Signal Transducer and Activator of Transcription 3). Biochem. J. 2013, 455, 229–237. [Google Scholar] [CrossRef]
- Kasper, G.; Weiser, A.A.; Rump, A.; Sparbier, K.; Dahl, E.; Hartmann, A.; Wild, P.; Schwidetzky, U.; Castaños-Vélez, E.; Lehmann, K. Expression Levels of the Putative Zinc Transporter LIV-1 Are Associated with a Better Outcome of Breast Cancer Patients. Int. J. Cancer 2005, 117, 961–973. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Yang, J.; Wang, C. Analysis of the Prognostic Significance of Solute Carrier (SLC) Family 39 Genes in Breast Cancer. Biosci. Rep. 2020, 40, BSR20200764. [Google Scholar] [CrossRef]
- Althobiti, M.; El-sharawy, K.A.; Joseph, C.; Aleskandarany, M.; Toss, M.S.; Green, A.R.; Rakha, E.A. Oestrogen-Regulated Protein SLC39A6: A Biomarker of Good Prognosis in Luminal Breast Cancer. Breast Cancer Res. Treat. 2021, 189, 621–630. [Google Scholar] [CrossRef]
- Jones, S.; Farr, G.; Nimmanon, T.; Ziliotto, S.; Gee, J.M.W.; Taylor, K.M. The Importance of Targeting Signalling Mechanisms of the SLC39A Family of Zinc Transporters to Inhibit Endocrine Resistant Breast Cancer. Explor. Target. Anti-Tumor Ther. 2022, 3, 224–239. [Google Scholar] [CrossRef]
- Bertucci, F.; Finetti, P.; Simeone, I.; Hendrickx, W.; Wang, E.; Marincola, F.M.; Viens, P.; Mamessier, E.; Ceccarelli, M.; Birnbaum, D.; et al. The Immunologic Constant of Rejection Classification Refines the Prognostic Value of Conventional Prognostic Signatures in Breast Cancer. Br. J. Cancer 2018, 119, 1383–1391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabatier, R.; Finetti, P.; Adelaide, J.; Guille, A.; Borg, J.-P.; Chaffanet, M.; Lane, L.; Birnbaum, D.; Bertucci, F. Down-Regulation of ECRG4, a Candidate Tumor Suppressor Gene, in Human Breast Cancer. PLoS ONE 2011, 6, e27656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birnbaum, D.J.; Finetti, P.; Lopresti, A.; Gilabert, M.; Poizat, F.; Turrini, O.; Raoul, J.-L.; Delpero, J.-R.; Moutardier, V.; Birnbaum, D.; et al. Prognostic Value of PDL1 Expression in Pancreatic Cancer. Oncotarget 2016, 7, 71198–71210. [Google Scholar] [CrossRef] [Green Version]
- Ghandi, M.; Huang, F.W.; Jané-Valbuena, J.; Kryukov, G.V.; Lo, C.C.; McDonald, E.R.; Barretina, J.; Gelfand, E.T.; Bielski, C.M.; Li, H.; et al. Next-Generation Characterization of the Cancer Cell Line Encyclopedia. Nature 2019, 569, 503–508. [Google Scholar] [CrossRef]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of Human Triple-Negative Breast Cancer Subtypes and Preclinical Models for Selection of Targeted Therapies. J. Clin. Investig. 2011, 121, 2750–2767. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, B.D.; Jovanović, B.; Chen, X.; Estrada, M.V.; Johnson, K.N.; Shyr, Y.; Moses, H.L.; Sanders, M.E.; Pietenpol, J.A. Refinement of Triple-Negative Breast Cancer Molecular Subtypes: Implications for Neoadjuvant Chemotherapy Selection. PLoS ONE 2016, 11, e0157368. [Google Scholar] [CrossRef]
- Guerrero-Zotano, A.L.; Stricker, T.P.; Formisano, L.; Hutchinson, K.E.; Stover, D.G.; Lee, K.; Schwarz, L.J.; Giltnane, J.M.; Estrada, V.M.; Jansen, V.M.; et al. ER+ Breast Cancers Resistant to Prolonged Neoadjuvant Letrozole Exhibit an E2F4 Transcriptional Program Sensitive to CDK4/6 Inhibitors. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2018, 24, 2517–2529. [Google Scholar] [CrossRef] [Green Version]
- Malorni, L.; Piazza, S.; Ciani, Y.; Guarducci, C.; Bonechi, M.; Biagioni, C.; Hart, C.D.; Verardo, R.; Leo, A.D.; Migliaccio, I. A Gene Expression Signature of Retinoblastoma Loss-of-Function Is a Predictive Biomarker of Resistance to Palbociclib in Breast Cancer Cell Lines and Is Prognostic in Patients with ER Positive Early Breast Cancer. Oncotarget 2016, 7, 68012–68022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-γ–Related MRNA Profile Predicts Clinical Response to PD-1 Blockade. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef]
- Walens, A.; Van Alsten, S.C.; Olsson, L.T.; Smith, M.A.; Lockhart, A.; Gao, X.; Hamilton, A.M.; Kirk, E.L.; Love, M.I.; Gupta, G.P.; et al. RNA-Based Classification of Homologous Recombination Deficiency in Racially-Diverse Patients with Breast Cancer. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2022, 31, 2136–2147. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Network Comprehensive Molecular Portraits of Human Breast Tumours. Nature 2012, 490, 61–70. [CrossRef] [PubMed] [Green Version]
- Curtis, C.; Shah, S.P.; Chin, S.-F.; Turashvili, G.; Rueda, O.M.; Dunning, M.J.; Speed, D.; Lynch, A.G.; Samarajiwa, S.; Yuan, Y.; et al. The Genomic and Transcriptomic Architecture of 2,000 Breast Tumours Reveals Novel Subgroups. Nature 2012, 486, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Condorelli, R.; Mosele, F.; Verret, B.; Bachelot, T.; Bedard, P.L.; Cortes, J.; Hyman, D.M.; Juric, D.; Krop, I.; Bieche, I.; et al. Genomic Alterations in Breast Cancer: Level of Evidence for Actionability According to ESMO Scale for Clinical Actionability of Molecular Targets (ESCAT). Ann. Oncol. 2019, 30, 365–373. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W. Identification of Clinically Useful Cancer Prognostic Factors: What Are We Missing? JNCI J. Natl. Cancer Inst. 2005, 97, 1023–1025. [Google Scholar] [CrossRef]
- Abd El-Rehim, D.M.; Ball, G.; Pinder, S.E.; Rakha, E.; Paish, C.; Robertson, J.F.R.; Macmillan, D.; Blamey, R.W.; Ellis, I.O. High-Throughput Protein Expression Analysis Using Tissue Microarray Technology of a Large Well-Characterised Series Identifies Biologically Distinct Classes of Breast Cancer Confirming Recent CDNA Expression Analyses. Int. J. Cancer 2005, 116, 340–350. [Google Scholar] [CrossRef]
- Tozlu, S.; Girault, I.; Vacher, S.; Vendrell, J.; Andrieu, C.; Spyratos, F.; Cohen, P.; Lidereau, R.; Bieche, I. Identification of Novel Genes That Co-Cluster with Estrogen Receptor Alpha in Breast Tumor Biopsy Specimens, Using a Large-Scale Real-Time Reverse Transcription-PCR Approach. Endocr. Relat. Cancer 2006, 13, 1109–1120. [Google Scholar] [CrossRef]
- Modi, S.; Pusztai, L.; Forero, A.; Mita, M.; Miller, K.; Weise, A.; Krop, I.; Burris, H., III.; Kalinsky, K.; Tsai, M.; et al. Abstract PD3-14: Phase 1 Study of the Antibody-Drug Conjugate SGN-LIV1A in Patients with Heavily Pretreated Triple-Negative Metastatic Breast Cancer. Cancer Res. 2018, 78, PD3–PD14. [Google Scholar] [CrossRef]
- Tsai, M.; Han, H.S.; Montero, A.J.; Tkaczuk, K.H.; Assad, H.; Pusztai, L.; Hurvitz, S.A.; Wilks, S.T.; Specht, J.M.; Nanda, R.; et al. 259P Weekly Ladiratuzumab Vedotin Monotherapy for Metastatic Triple-Negative Breast Cancer. Ann. Oncol. 2021, 32, S474–S475. [Google Scholar] [CrossRef]
- Beckwith, H.; Schwab, R.; Yau, C.; Stringer-Reasor, E.; Wei, S.; Chien, A.J.; Albain, K.S.; Kalinsky, K.; Wallace, A.; Elias, A.; et al. Abstract PD1-10: Evaluation of SGN-LIV1a Followed by AC in High-Risk HER2 Negative Stage II/III Breast Cancer: Results from the I-SPY 2 TRIAL. Cancer Res. 2021, 81, PD1–PD10. [Google Scholar] [CrossRef]
- Cao, A.T.; Higgins, S.; Stevens, N.; Gardai, S.J.; Sussman, D. Abstract 2742: Additional Mechanisms of Action of Ladiratuzumab Vedotin Contribute to Increased Immune Cell Activation within the Tumor. Cancer Res. 2018, 78, 2742. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| N | All | LIV1 Class | ||||
|---|---|---|---|---|---|---|
| Low | High | p-Value | ||||
| Age at diagnosis (years) | 4.28 × 10−9 | |||||
| ≤50 | 2540 | 2540 (36%) | 1379 (40%) | 1161 (33%) | ||
| >50 | 4488 | 4488 (64%) | 2108 (60%) | 2380 (67%) | ||
| Pathological lymph node (pN) | 0.469 | |||||
| negative | 3446 | 3446 (56%) | 1668 (55%) | 1778 (56%) | ||
| positive | 2743 | 2743 (44%) | 1354 (45%) | 1389 (44%) | ||
| Pathological tumor size (pT) | 4.42 × 10−4 | |||||
| pT1 | 2113 | 2113 (38%) | 956 (35%) | 1157 (40%) | ||
| pT2–3 | 3518 | 3518 (62%) | 1763 (65%) | 1755 (60%) | ||
| Pathological tumor grade | 2.12 × 10−21 | |||||
| 1 | 721 | 721 (11%) | 246 (8%) | 475 (15%) | ||
| 2–3 | 5559 | 5559 (89%) | 2946 (92%) | 2613 (85%) | ||
| ER status | <2.0 × 10−255 | |||||
| negative | 2764 | 2764 (31%) | 2502 (56%) | 262 (6%) | ||
| positive | 6218 | 6218 (69%) | 1989 (44%) | 4229 (94%) | ||
| PR status | <2.0 × 10−255 | |||||
| negative | 4670 | 4670 (52%) | 3151 (71%) | 1519 (34%) | ||
| positive | 4255 | 4255 (48%) | 1304 (29%) | 2951 (66%) | ||
| HER2 status | 1.49 × 10−58 | |||||
| negative | 7884 | 7884 (88%) | 3695 (82%) | 4189 (93%) | ||
| positive | 1098 | 1098 (12%) | 796 (18%) | 302 (7%) | ||
| Molecular subtype | <2.0 × 10−255 | |||||
| HR+/HER2- | 5929 | 5929 (66%) | 1878 (42%) | 4051 (90%) | ||
| HER2+ | 1098 | 1098 (12%) | 796 (18%) | 302 (7%) | ||
| TN | 1936 | 1936 (22%) | 1801 (40%) | 135 (3%) | ||
| Pathological complete response (pCR) | 6.84 × 10−20 | |||||
| no pCR | 922 | 922 (77%) | 448 (67%) | 474 (89%) | ||
| pCR | 281 | 281 (23%) | 224 (33%) | 57 (11%) | ||
| Follow-up median, months (min–max) | 6645 | 68 (1–382) | 62 (1–302) | 68 (1–382) | 6.42 × 10−3 | |
| DFS event, N (%) | 6645 | 1891 (28%) | 1072 (33%) | 819 (24%) | 1.17 × 10−16 | |
| 5-year DFS (95% CI) | 6645 | 75% (74–76) | 68% (67–70) | 81% (79–82) | <2.0 × 10−16 | |
| OS event, N (%) | 5053 | 1127 (22%) | 645 (27%) | 482 (18%) | 1.46 × 10−13 | |
| 5-year OS (95% CI) | 5053 | 82% (81–84) | 76% (75–78) | 88% (87–89) | 2.22 × 10−12 | |
| DFS | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| N | HR (95% CI) | p-Value | N | HR (95% CI) | p-Value | |
| Age at diagnosis (years), ≤50 vs. >50 years | 5317 | 1.22 (1.10–1.37) | 2.91 × 10−4 | 3229 | 1.25 (1.10–1.43) | 7.37 × 10−4 |
| Pathological lymph node (pN), pos vs. neg | 5165 | 1.63 (1.47–1.82) | 3.16 × 10−19 | 3229 | 1.46 (1.28–1.66) | 9.64 × 10−9 |
| Pathological tumour size (pT), pT2-pT3 vs. pT1 | 4719 | 1.68 (1.50–1.90) | 1.12 × 10−17 | 3229 | 1.57 (1.37–1.80) | 7.01 × 10−11 |
| Pathological tumour grade, 2–3 vs. 1 | 4588 | 2.21 (1.80–2.72) | 5.24 × 10−14 | 3229 | 1.58 (1.25–2.00) | 1.30 × 10−4 |
| Molecular subtype, HER2+ vs. HR+/HER2- | 6626 | 1.86 (1.64–2.11) | 4.86 × 10−35 | 3229 | 1.64 (1.37–1.98) | 1.49 × 10−7 |
| TN vs. HR+/HER2- | 1.77 (1.59–1.97) | 3229 | 1.25 (1.03–1.51) | 2.21 × 10−2 | ||
| LIV1 expression status, high vs. low | 6645 | 0.67 (0.61–0.73) | 4.87 × 10−18 | 3229 | 0.85 (0.73–0.99) | 3.88 × 10−2 |
| DFS | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| N | HR (95% CI) | p-Value | N | HR (95% CI) | p-Value | |
| Age at diagnosis (years), ≤50 vs. >50 years | 4542 | 1.05 (0.92–1.20} | 0.440 | |||
| Pathological lymph node (pN), pos vs. neg | 4274 | 2.22 (1.94–2.54} | 4.14 × 10−31 | 3070 | 1.92 (1.66–2.22} | 3.6 × 10−18 |
| Pathological tumour size (pT), pT2-pT3 vs. pT1 | 4250 | 1.96 (1.70–2.26} | 9.81 × 10−21 | 3070 | 1.68 (1.44–1.97} | 3.68 × 10−11 |
| Pathological tumour grade, 2–3 vs. 1 | 3745 | 2.98 (2.26–3.93} | 1.18 × 10−14 | 3070 | 2.04 (1.51–2.76} | 3.99 × 10−6 |
| Molecular subtype, HER2+ vs. HR+/HER2- | 5034 | 2.03 (1.73–2.38} | 3.51 × 10−23 | 3070 | 1.66 (1.35–2.04} | 1.13 × 10−6 |
| TN vs. HR+/HER2- | 1.70 (1.47–1.96} | 3070 | 1.29 (1.05–1.58} | 1.46 × 10−2 | ||
| LIV1 expression status, high vs. low | 5053 | 0.66 (0.58–0.74} | 3.20 × 10−12 | 3070 | 0.76 (0.64–0.90} | 1.74 × 10−3 |
| pCR | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| N | OR (95% CI) | p-Value | N | HR (95% CI) | p-Value | |
| Age at diagnosis (years), ≤50 vs. >50 years | 1202 | 1.16 (0.08–1.52) | 0.262 | |||
| Pathological grade, 2–3 vs. 1 | 1097 | 8.07 (1.95–33.4) | 3.93 × 10−3 | 1097 | 4.13 (0.98–17.5) | 0.054 |
| Molecular subtype, HER2+ vs. HR+/HER2- | 1203 | 3.85 (2.55–5.79) | 1.12 × 10−10 | 1097 | 2.77 (1.76–4.37) | 1.21 × 10−5 |
| TN vs. HR+/HER2- | 1203 | 3.58 (2.61–4.91) | 2.22 × 10−15 | 1097 | 2.31 (1.58–3.37) | 1.37 × 10−5 |
| LIV1 expression status, high vs. low | 1203 | 0.24 (0.17–0.33) | 1.65 × 10−18 | 1097 | 0.37 (0.25–0.54) | 1.57 × 10−5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Nonneville, A.; Finetti, P.; Boudin, L.; Denicolaï, E.; Birnbaum, D.; Mamessier, E.; Bertucci, F. Prognostic and Predictive Value of LIV1 Expression in Early Breast Cancer and by Molecular Subtype. Pharmaceutics 2023, 15, 938. https://doi.org/10.3390/pharmaceutics15030938
de Nonneville A, Finetti P, Boudin L, Denicolaï E, Birnbaum D, Mamessier E, Bertucci F. Prognostic and Predictive Value of LIV1 Expression in Early Breast Cancer and by Molecular Subtype. Pharmaceutics. 2023; 15(3):938. https://doi.org/10.3390/pharmaceutics15030938
Chicago/Turabian Stylede Nonneville, Alexandre, Pascal Finetti, Laurys Boudin, Emilie Denicolaï, Daniel Birnbaum, Emilie Mamessier, and François Bertucci. 2023. "Prognostic and Predictive Value of LIV1 Expression in Early Breast Cancer and by Molecular Subtype" Pharmaceutics 15, no. 3: 938. https://doi.org/10.3390/pharmaceutics15030938