
Perspectives of Therapeutic Drug Monitoring of Biological Agents in Non-Infectious Uveitis Treatment: A Review
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Biologics in Uveitis Treatment

{kind=link}
{kind=link}
| Drug | Target | Structure | Dosage | Uveitis Type | References |
|---|---|---|---|---|---|
| Adalimumab 1 | TNF-α | mAb, fully humanized | LD: 80 mg MD: 40 mg every other week | Non-infectious non-anterior uveitis † | [6,7] |
| Infliximab | TNF-α | mAb, mouse-human chimeric | LD: 5 mg/kg at weeks 0, 4, and 6 MD: 5 mg/kg every 4 to 8 weeks Max. dose: 10mg/kg for adults, 20 mg/kg for children every 4 weeks | JIA-related uveitis, Behçet, VKH, sarcoidosis, pars planitis, birdshot retinochoroidopathy, idiopatic uveitis | [1,4,33,34,37] |
| Etanercept 2 | TNF-α | Human fusion protein | 50 mg weekly | Behçet | [4] |
| Golimumab | TNF-α | mAb, fully humanized | MD: 50 mg monthly Max. dose: 100 mg monthly | Refractory uveitis | [40,41] |
| Certolizumab | TNF-α | mAb, fully humanized | 200 mg every 2 weeks | Refractory uveitis | [44] |
| Tocilizumab | IL-6 | mAb, fully humanized | 4–12 mg/kg every 2–4 weeks | Non-infectious non-anterior uveitis, Behçet, birdshot, JIA-related uveitis | [46,47,48,49] |
| Rituximab | CD-20 | mAb, mouse-human chimeric | LD: 500 or 1000 mg at 0, and 2 weeks. MD: Repeat at 6–12 months if needed | Refractory uveitis, JIA-related uveitis, Behçet, VKH, Wegener’s granulomatosis | [50,51,52,53,54,55] |
3. Therapeutic Drug Monitoring of Anti-TNFα in NIU
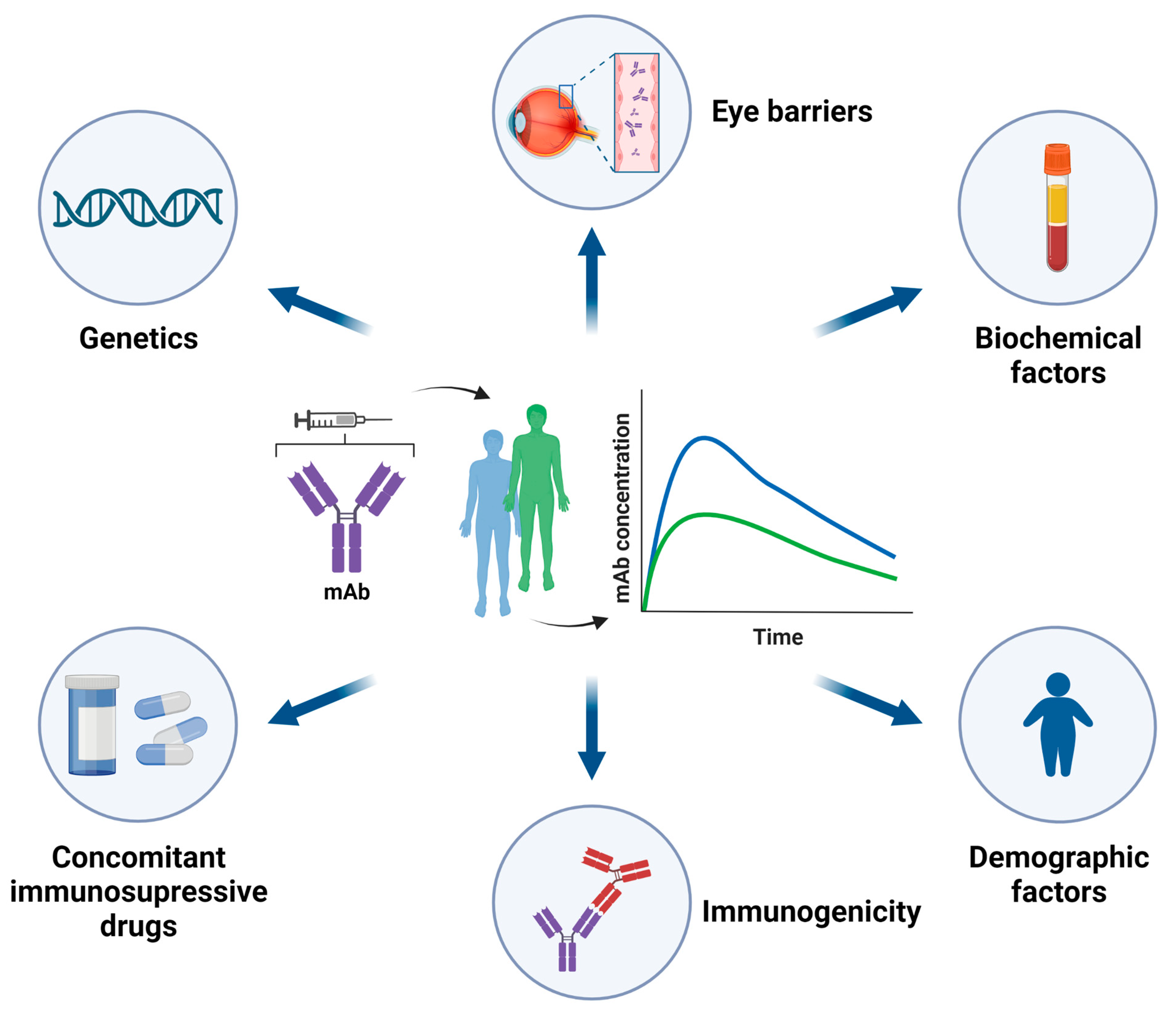
3.1. Pharmacokinetics (PK) of mAbs
3.1.1. Demographic Factors
3.1.2. Biochemical Factors
3.1.3. Immunogenicity of mAbs
3.1.4. Concomitant Immunosuppressive Therapy
3.2. Evidence Supporting TDM of Anti-TNFα in NIU
| Authors [Ref.] | Type of Study | Treatment | Type NIU | No. Patients | Results |
|---|---|---|---|---|---|
| Cordero-Coma et al. 2016 [18] | Observational, prospective | ADA | Refractory uveitis | 25 Naïve to biologics |
|
| Skrabl-Baumgartner et al. 2019 [17] | Observational, prospective | ADA | JIA related uveitis | 20 |
|
| Leinonen et al. 2017 [70] | Observational, retrospective | ADA | JIA related uveitis | 31 |
|
| Sejournet et al. 2021 [92] | Observational, retrospective | ADA | JIA related uveitis | 79 |
|
| EMA/501143/2016 [61] | Phase III studies (VISUAL I and VISUAL II) | ADA | NIU | 249 (118 VISUAL I/131 VISUAL II) |
|
| Sugita et al. 2011 [93] | Observational, prospective | IFX | RUBD | 20 |
|
3.3. TDM-Based Strategies and Therapeutic trough Levels of Anti-TNFα in NIU
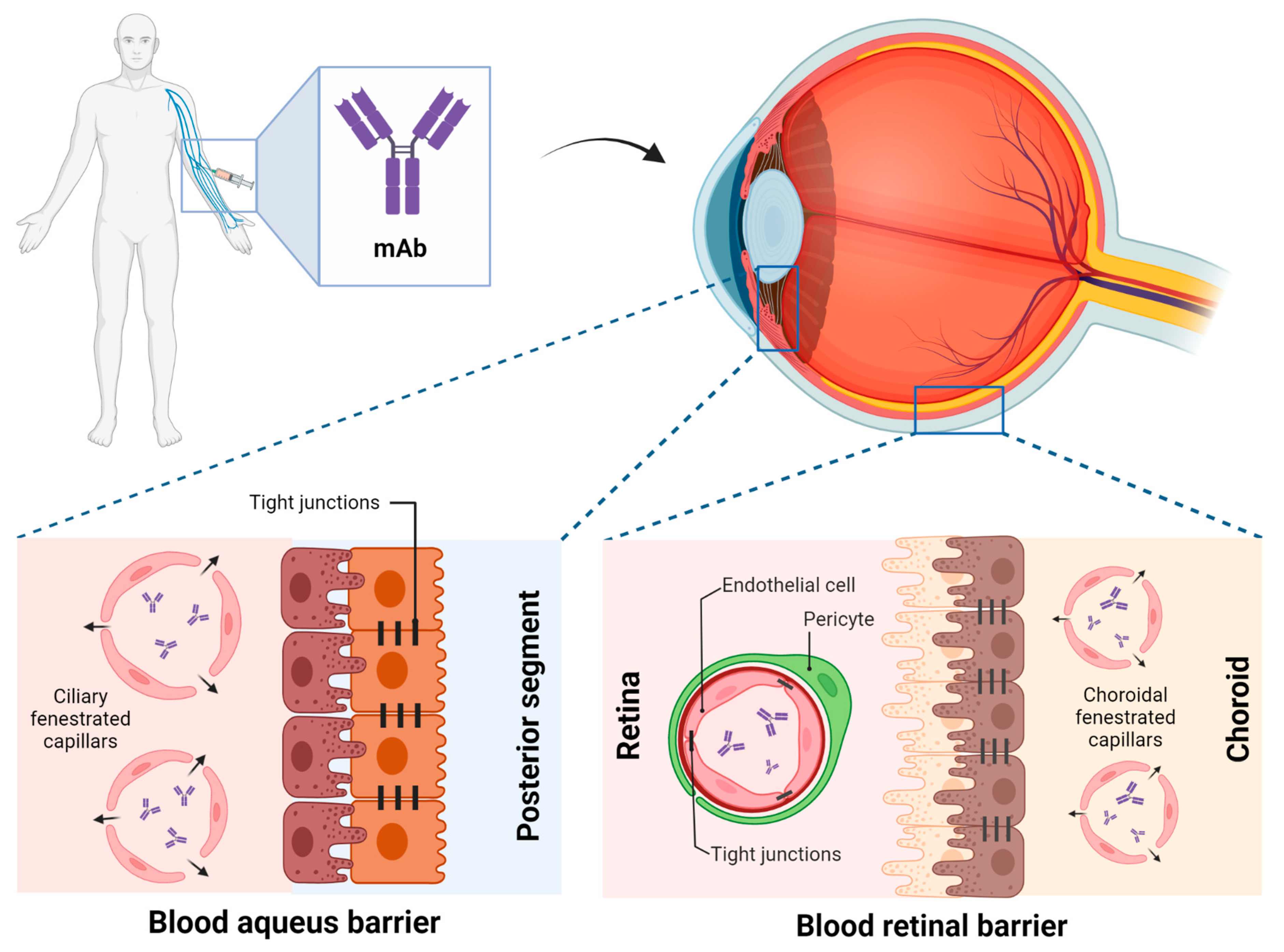
4. Implications of Ocular Drug PK
5. Pharmacogenetics (PG) of Anti-TNFα in NIU
5.1. Candidate Gene Association Studies
5.2. HLA Complex
| Authors [Ref.] | Gene | SNP (Allele) | Effect of the SNP | Disease | Proposed Gene/Protein Function |
|---|---|---|---|---|---|
| Bek et al. 2017 [130] | CHUK | rs11591741 (C) | non-response | RA | Component of a cytokine-activated protein complex that inhibits NFκB. |
| PTPRC | rs10919563 (A) | non-response | RA | Suppresses JAK kinases, functions as a regulator of cytokine receptor signalling. | |
| TRAF1/C5 | rs3761847 (G) | non-response | RA | Required for TNFα-mediated activation of MAPK8/JNK and NFκB. Mediates the anti-apoptotic signals from TNF receptors. | |
| NFΚBIB | rs9403 (C) | non-response | RA | Inhibits NFκB by complexing with and trapping it in the cytoplasm. | |
| FCGR2A | rs1801274 (G) | non-response | RA | Involved in the process of phagocytosis and clearing of immune complexes. | |
| IRAK3 | rs11541076 (T) | non-response | RA | Negative regulator of Toll-like receptor signalling. | |
| Bartelds et al. 2009 [134] | IL10 | rs6703630, rs1800896, rs1800871 (AGC haplotype) | non-response a | RA | Pleiotropic cytokine with a role in immunoregulation and inflammation, enhances B cell survival, proliferation, and antibody production, can block NFκB activity, and is involved in the regulation of the JAK-STAT signalling pathway |
| rs6703630, rs1800896, rs1800871 (GAT haplotype) | response a | ||||
| Bank et al. 2014 [131] | TLR2 | rs4696480 (T) | non-response | Only UC | Activates inflammation through the canonical NFκB pathway. |
| rs11938228 (A) b | non-response | IBD | |||
| rs1816702 (T) | response | Only CD | |||
| rs3804099 (C) | response | IBD | |||
| TLR4 | rs1554973 (C) b | non-response | IBD | Activates inflammation through the canonical or noncanonical NFκB pathway. | |
| rs5030728 (A) b | response | ||||
| TLR9 | rs352139 (A) | non-response | IBD | Activates inflammation through the canonical NFκB pathway. | |
| rs187084 (C) | response | ||||
| CD14 | rs2569190 (A) | non-response | Only UC | Binds LPS and transport it to TLR4 | |
| TNFA | rs361525 (A) | non-response | IBD | Pro-inflammatory cytokine activated by NFκB1. | |
| TNFAIP3 | rs6927172 (G) | non-response | IBD | Inhibits NFκB activation and TNFα-mediated apoptosis. | |
| IL1RN | rs4251961 (C) b | non-response | Only UC | Inhibits IL-1β signalling. | |
| IL17A | rs2275913 (A) | non-response | IBD | Pro-inflammatory cytokine activated by NFκB1, induces production of IL-1β, IL-6, and TNFα. | |
| LY96 | rs11465996 (G) | response | IBD | Binds to TLR2 or TLR4 and is required for their activation to LPS stimuli | |
| MAP3K14 | rs7222094 (C) | response | IBD | Central kinase in the noncanonical NFκB pathway | |
| TNFRSF1A | rs4149570 (T) b | response | IBD | Binds TNFα and initiates a kinase cascade. | |
| IL1B | rs4848306 (A) | response | IBD | Pro-inflammatory cytokine activated by NFκB1. | |
| IL6 | rs10499563 (C) | response | IBD | Pro- and anti-inflammatory cytokine activated by NFκB1. | |
| IFNG | rs2430561 (A) | response | IBD | Pro- and anti-inflammatory cytokine activated by NFκB1. | |
| Bank et al. 2019 [132] | NLRP3 | rs4612666 (T) | non-response | IBD | Member of the NLRP3 inflammasome complex, upstream activator of NFκB signalling. |
| IL18 | rs187238 (C) | response | Only CD | Proinflammatory cytokine of the IL-1 family, capable of stimulating IFNγ production. | |
| rs1946518 (T) | response | IBD | |||
| JAK2 | rs12343867 (C) | response | IBD | Plays a central role in cytokine and growth factor signalling, downstream target of IL6 | |
| NFΚBIA | rs696 (A) | response | IBD | Complexes with REL dimers inhibit NFκB/REL complexes. | |
| Hässler et al. 2020 [133] | CXCL12 | rs10508884 (T) | non-response a | Several diseases | Plays a role in embryogenesis, immune surveillance, antibody affinity maturation, inflammation response, tissue homeostasis, and tumour growth and metastasis. |
| HLA-DQ | HLA-DQA1*05 | non-response a | Plays a central role in the immune system by presenting peptides from extracellular proteins. | ||
| Sazonovs et al. 2020 [136] | HLA-DQ | HLA-DQA1*05 | non-response a | CD | Plays a central role in the immune system by presenting peptides from extracellular proteins. |
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shahab, M.A.; Mir, T.A.; Zafar, S. Optimising Drug Therapy for Non-Infectious Uveitis. Int. Ophthalmol. 2019, 39, 1633–1650. [Google Scholar] [CrossRef]
- Jabs, D.A. Immunosuppression for the Uveitides. Ophthalmology 2018, 125, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leclercq, M.; Desbois, A.-C.; Domont, F.; Maalouf, G.; Touhami, S.; Cacoub, P.; Bodaghi, B.; Saadoun, D. Biotherapies in Uveitis. J. Clin. Med. 2020, 9, 3599. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.S. Biologics for the Treatment of Noninfectious Uveitis: Current Concepts and Emerging Therapeutics. Curr. Opin. Ophthalmol. 2019, 30, 138–150. [Google Scholar] [CrossRef] [PubMed]
- Ozguler, Y.; Leccese, P.; Christensen, R.; Esatoglu, S.N.; Bang, D.; Bodaghi, B.; Çelik, A.F.; Fortune, F.; Gaudric, J.; Gul, A.; et al. Management of Major Organ Involvement of Behçet’s Syndrome: A Systematic Review for Update of the EULAR Recommendations. Rheumatology 2018, 57, 2200–2212. [Google Scholar] [CrossRef]
- Nguyen, Q.D.; Merrill, P.T.; Jaffe, G.J.; Dick, A.D.; Kurup, S.K.; Sheppard, J.; Schlaen, A.; Pavesio, C.; Cimino, L.; Van Calster, J.; et al. Adalimumab for Prevention of Uveitic Flare in Patients with Inactive Non-Infectious Uveitis Controlled by Corticosteroids (VISUAL II): A Multicentre, Double-Masked, Randomised, Placebo-Controlled Phase 3 Trial. Lancet 2016, 388, 1183–1192. [Google Scholar] [CrossRef] [Green Version]
- Jaffe, G.J.; Dick, A.D.; Brézin, A.P.; Nguyen, Q.D.; Thorne, J.E.; Kestelyn, P.; Barisani-Asenbauer, T.; Franco, P.; Heiligenhaus, A.; Scales, D.; et al. Adalimumab in Patients with Active Noninfectious Uveitis. N. Engl. J. Med. 2016, 375, 932–943. [Google Scholar] [CrossRef] [Green Version]
- Llorenç, V.; Cordero-Coma, M.; Blanco-Esteban, A.; Heras-Mulero, H.; Losada-Castillo, M.-J.; Jovani-Casano, V.; Valls-Pascual, E.; Jodar-Marquez, M.; García-Aparicio, Á.; Fonollosa, A.; et al. Drug Retention Rate and Causes of Discontinuation of Adalimumab in Uveitis: Real-World Data from the Biotherapies in Uveitis (BioÚvea) Study Group. Ophthalmology 2020, 127, 814–825. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, K.; Mangas-Sanjuán, V.; Merino-Sanjuán, M.; Martorell-Calatayud, A.; Mateu-Puchades, A.; Climente-Martí, M.; Gras-Colomer, E. Impact of Pharmacokinetic and Pharmacodynamic Properties of Monoclonal Antibodies in the Management of Psoriasis. Pharmaceutics 2022, 14, 654. [Google Scholar] [CrossRef]
- Barar, J.; Javadzadeh, A.R.; Omidi, Y. Ocular Novel Drug Delivery: Impacts of Membranes and Barriers. Expert Opin. Drug Deliv. 2008, 5, 567–581. [Google Scholar] [CrossRef]
- An, G. Concept of Pharmacologic Target-Mediated Drug Disposition in Large-Molecule and Small-Molecule Compounds. J. Clin. Pharmacol. 2020, 60, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Juncadella, A.; Wong, D.; Rakowsky, S.; Sattler, L.A.; Campbell, J.P.; Vaughn, B.P.; Cheifetz, A.S. Proactive Therapeutic Drug Monitoring of Adalimumab Is Associated with Better Long-Term Outcomes Compared with Standard of Care in Patients with Inflammatory Bowel Disease. J. Crohns Colitis 2019, 13, 976–981. [Google Scholar] [CrossRef]
- Jani, M.; Chinoy, H.; Warren, R.B.; Griffiths, C.E.M.; Plant, D.; Fu, B.; Morgan, A.W.; Wilson, A.G.; Isaacs, J.D.; Hyrich, K.; et al. Clinical Utility of Random Anti–Tumor Necrosis Factor Drug–Level Testing and Measurement of Antidrug Antibodies on the Long-Term Treatment Response in Rheumatoid Arthritis. Arthritis Rheumatol. 2015, 67, 2011–2019. [Google Scholar] [CrossRef] [Green Version]
- Papamichael, K.; Vogelzang, E.H.; Lambert, J.; Wolbink, G.; Cheifetz, A.S. Therapeutic Drug Monitoring with Biologic Agents in Immune Mediated Inflammatory Diseases. Expert Rev. Clin. Immunol. 2019, 15, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Meroni, P.L.; Valentini, G.; Ayala, F.; Cattaneo, A.; Valesini, G. New Strategies to Address the Pharmacodynamics and Pharmacokinetics of Tumor Necrosis Factor (TNF) Inhibitors: A Systematic Analysis. Autoimmun. Rev. 2015, 14, 812–829. [Google Scholar] [CrossRef] [PubMed]
- Gorovits, B.; Baltrukonis, D.J.; Bhattacharya, I.; Birchler, M.A.; Finco, D.; Sikkema, D.; Vincent, M.S.; Lula, S.; Marshall, L.; Hickling, T.P. Immunoassay Methods Used in Clinical Studies for the Detection of Anti-Drug Antibodies to Adalimumab and Infliximab. Clin. Exp. Immunol. 2018, 192, 348–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skrabl-Baumgartner, A.; Seidel, G.; Langner-Wegscheider, B.; Schlagenhauf, A.; Jahnel, J. Drug Monitoring in Long-Term Treatment with Adalimumab for Juvenile Idiopathic Arthritis-Associated Uveitis. Arch. Dis. Child. 2019, 104, 246–250. [Google Scholar] [CrossRef]
- Cordero-Coma, M.; Calleja-Antolín, S.; Garzo-García, I.; Nuñez-Garnés, A.M.; Álvarez-Castro, C.; Franco-Benito, M.; Ruiz de Morales, J.G. Adalimumab for Treatment of Noninfectious Uveitis. Ophthalmology 2016, 123, 2618–2625. [Google Scholar] [CrossRef]
- Hanauer, S.B.; Sandborn, W.J.; Rutgeerts, P.; Fedorak, R.N.; Lukas, M.; MacIntosh, D.; Panaccione, R.; Wolf, D.; Pollack, P. Human Anti-Tumor Necrosis Factor Monoclonal Antibody (Adalimumab) in Crohn’s Disease: The CLASSIC-I Trial. Gastroenterology 2006, 130, 323–333, quiz 591. [Google Scholar] [CrossRef] [Green Version]
- Bartelds, G.M.; Wijbrandts, C.A.; Nurmohamed, M.T.; Stapel, S.; Lems, W.F.; Aarden, L.; Dijkmans, B.A.C.; Tak, P.P.; Wolbink, G.J. Clinical Response to Adalimumab: Relationship to Anti-Adalimumab Antibodies and Serum Adalimumab Concentrations in Rheumatoid Arthritis. Ann. Rheum. Dis. 2007, 66, 921–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, V.A.; Balthasar, J.P. Understanding Inter-Individual Variability in Monoclonal Antibody Disposition. Antibodies Basel Switz. 2019, 8, 56. [Google Scholar] [CrossRef] [Green Version]
- Escudero-Ortiz, V.; Domínguez-Leñero, V.; Catalán-Latorre, A.; Rebollo-Liceaga, J.; Sureda, M. Relevance of Therapeutic Drug Monitoring of Tyrosine Kinase Inhibitors in Routine Clinical Practice: A Pilot Study. Pharmaceutics 2022, 14, 1216. [Google Scholar] [CrossRef]
- Egwuagu, C.E.; Alhakeem, S.A.; Mbanefo, E.C. Uveitis: Molecular Pathogenesis and Emerging Therapies. Front. Immunol. 2021, 12, 623725. [Google Scholar] [CrossRef]
- Gangaputra, S.S.; Newcomb, C.W.; Joffe, M.M.; Dreger, K.; Begum, H.; Artornsombudh, P.; Pujari, S.S.; Daniel, E.; Sen, H.N.; Suhler, E.B.; et al. Comparison Between Methotrexate and Mycophenolate Mofetil Monotherapy for the Control of Noninfectious Ocular Inflammatory Diseases. Am. J. Ophthalmol. 2019, 208, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Errera, M.-H.; Pratas, A.; Fisson, S.; Manicom, T.; Boubaya, M.; Sedira, N.; Héron, E.; Merabet, L.; Kobal, A.; Levy, V.; et al. Cytokines, Chemokines and Growth Factors Profile in Human Aqueous Humor in Idiopathic Uveitis. PLoS ONE 2022, 17, e0254972. [Google Scholar] [CrossRef] [PubMed]
- Ramanan, A.V.; Dick, A.D.; Jones, A.P.; Hughes, D.A.; McKay, A.; Rosala-Hallas, A.; Williamson, P.R.; Hardwick, B.; Hickey, H.; Rainford, N.; et al. Adalimumab in Combination with Methotrexate for Refractory Uveitis Associated with Juvenile Idiopathic Arthritis: A RCT. Health Technol. Assess. 2019, 23, 1–140. [Google Scholar] [CrossRef] [PubMed]
- Cordero-Coma, M.; Sobrin, L. Anti–Tumor Necrosis Factor-α Therapy in Uveitis. Surv. Ophthalmol. 2015, 60, 575–589. [Google Scholar] [CrossRef]
- Diaz-Llopis, M.; García-Delpech, S.; Salom, D.; Udaondo, P.; Hernández-Garfella, M.; Bosch-Morell, F.; Quijada, A.; Romero, F.J. Adalimumab Therapy for Refractory Uveitis: A Pilot Study. J. Ocul. Pharmacol. Ther. 2008, 24, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Suhler, E.B.; Jaffe, G.J.; Fortin, E.; Lim, L.L.; Merrill, P.T.; Dick, A.D.; Brezin, A.P.; Nguyen, Q.D.; Thorne, J.E.; Van Calster, J.; et al. Long-Term Safety and Efficacy of Adalimumab in Patients with Noninfectious Intermediate Uveitis, Posterior Uveitis, or Panuveitis. Ophthalmology 2021, 128, 899–909. [Google Scholar] [CrossRef]
- Li, B.; Li, H.; Zhang, L.; Zheng, Y. Efficacy and Safety of Adalimumab in Noninfectious Uveitis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Pharmacol. 2021, 12, 673984. [Google Scholar] [CrossRef]
- Rivas, A.B.; Lopez-Picado, A.; Calamia, V.; Carreño, E.; Cocho, L.; Cordero-Coma, M.; Fonollosa, A.; Francisco Hernandez, F.M.; Garcia-Aparicio, A.; Garcia-Gonzalez, J.; et al. Efficacy, Safety and Cost-Effectiveness of Methotrexate, Adalimumab or Their Combination in Non-Infectious Non-Anterior Uveitis: A Protocol for a Multicentre, Randomised, Parallel Three Arms, Active-Controlled, Phase III Open Label with Blinded Outcome Assessment Study. BMJ Open 2022, 12, e051378. [Google Scholar] [CrossRef]
- Sfikakis, P.P.; Theodossiadis, P.G.; Katsiari, C.G.; Kaklamanis, P.; Markomichelakis, N.N. Effect of Infliximab on Sight-Threatening Panuveitis in Behçet’s Disease. Lancet Lond. Engl. 2001, 358, 295–296. [Google Scholar] [CrossRef]
- Ardoin, S.P.; Kredich, D.; Rabinovich, E.; Schanberg, L.E.; Jaffe, G.J. Infliximab to Treat Chronic Noninfectious Uveitis in Children: Retrospective Case Series with Long-Term Follow-Up. Am. J. Ophthalmol. 2007, 144, 844–849.e1. [Google Scholar] [CrossRef] [Green Version]
- Markomichelakis, N.; Delicha, E.; Masselos, S.; Fragiadaki, K.; Kaklamanis, P.; Sfikakis, P.P. A Single Infliximab Infusion vs Corticosteroids for Acute Panuveitis Attacks in Behcet’s Disease: A Comparative 4-Week Study. Rheumatology 2011, 50, 593–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohno, S.; Umebayashi, I.; Matsukawa, M.; Goto, T.; Yano, T. Safety and Efficacy of Infliximab in the Treatment of Refractory Uveoretinitis in Behçet’s Disease: A Large-Scale, Long-Term Postmarketing Surveillance in Japan. Arthritis Res. Ther. 2019, 21, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy-Clarke, G.; Jabs, D.A.; Read, R.W.; Rosenbaum, J.T.; Vitale, A.; Van Gelder, R.N. Expert Panel Recommendations for the Use of Anti–Tumor Necrosis Factor Biologic Agents in Patients with Ocular Inflammatory Disorders. Ophthalmology 2014, 121, 785–796.e3. [Google Scholar] [CrossRef]
- Tambralli, A.; Beukelman, T.; Weiser, P.; Atkinson, T.P.; Cron, R.Q.; Stoll, M.L. High Doses of Infliximab in the Management of Juvenile Idiopathic Arthritis. J. Rheumatol. 2013, 40, 1749–1755. [Google Scholar] [CrossRef]
- Hasegawa, E.; Takeda, A.; Yawata, N.; Sonoda, K.-H. The Effectiveness of Adalimumab Treatment for Non-Infectious Uveitis. Immunol. Med. 2019, 42, 79–83. [Google Scholar] [CrossRef]
- Lim, L.L.; Fraunfelder, F.W.; Rosenbaum, J.T. Do Tumor Necrosis Factor Inhibitors Cause Uveitis? A Registry-Based Study. Arthritis Rheum. 2007, 56, 3248–3252. [Google Scholar] [CrossRef] [PubMed]
- Miserocchi, E.; Modorati, G.; Pontikaki, I.; Meroni, P.L.; Gerloni, V. Long-Term Treatment with Golimumab for Severe Uveitis. Ocul. Immunol. Inflamm. 2014, 22, 90–95. [Google Scholar] [CrossRef]
- Calvo-Río, V.; Blanco, R.; Santos-Gómez, M.; Rubio-Romero, E.; Cordero-Coma, M.; Gallego-Flores, A.; Veroz, R.; Torre, I.; Hernández, F.F.; Atanes, A.; et al. Golimumab in Refractory Uveitis Related to Spondyloarthritis. Multicenter Study of 15 Patients. Semin. Arthritis Rheum. 2016, 46, 95–101. [Google Scholar] [CrossRef]
- Atiqi, S.; Hooijberg, F.; Loeff, F.C.; Rispens, T.; Wolbink, G.J. Immunogenicity of TNF-Inhibitors. Front. Immunol. 2020, 11, 312. [Google Scholar] [CrossRef] [PubMed]
- Ternant, D.; Bejan-Angoulvant, T.; Passot, C.; Mulleman, D.; Paintaud, G. Clinical Pharmacokinetics and Pharmacodynamics of Monoclonal Antibodies Approved to Treat Rheumatoid Arthritis. Clin. Pharmacokinet. 2015, 54, 1107–1123. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Peña, D.; Calderón-Goercke, M.; Adán, A.; Chamorro-López, L.; Maíz-Alonso, O.; De Dios-Jiménez Aberásturi, J.R.; Veroz, R.; Blanco, S.; Martín-Santos, J.M.; Navarro, F.; et al. Efficacy and Safety of Certolizumab Pegol in Pregnant Women with Uveitis. Recommendations on the Management with Immunosuppressive and Biologic Therapies in Uveitis during Pregnancy. Clin. Exp. Rheumatol. 2021, 39, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Sepah, Y.J.; Sadiq, M.A.; Chu, D.S.; Dacey, M.; Gallemore, R.; Dayani, P.; Hanout, M.; Hassan, M.; Afridi, R.; Agarwal, A.; et al. Primary (Month-6) Outcomes of the STOP-Uveitis Study: Evaluating the Safety, Tolerability, and Efficacy of Tocilizumab in Patients with Noninfectious Uveitis. Am. J. Ophthalmol. 2017, 183, 71–80. [Google Scholar] [CrossRef]
- Calvo-Río, V.; Santos-Gómez, M.; Calvo, I.; González-Fernández, M.I.; López-Montesinos, B.; Mesquida, M.; Adán, A.; Hernández, M.V.; Maíz, O.; Atanes, A.; et al. Anti-Interleukin-6 Receptor Tocilizumab for Severe Juvenile Idiopathic Arthritis-Associated Uveitis Refractory to Anti-Tumor Necrosis Factor Therapy: A Multicenter Study of Twenty-Five Patients. Arthritis Rheumatol. 2017, 69, 668–675. [Google Scholar] [CrossRef]
- Atienza-Mateo, B.; Calvo-Río, V.; Beltrán, E.; Martínez-Costa, L.; Valls-Pascual, E.; Hernández-Garfella, M.; Atanes, A.; Cordero-Coma, M.; Miquel Nolla, J.; Carrasco-Cubero, C.; et al. Anti-Interleukin 6 Receptor Tocilizumab in Refractory Uveitis Associated with Behçet’s Disease: Multicentre Retrospective Study. Rheumatology 2018, 57, 856–864. [Google Scholar] [CrossRef] [Green Version]
- Leclercq, M.; Le Besnerais, M.; Langlois, V.; Girszyn, N.; Benhamou, Y.; Ngo, C.; Levesque, H.; Muraine, M.; Gueudry, J. Tocilizumab for the Treatment of Birdshot Uveitis That Failed Interferon Alpha and Anti-Tumor Necrosis Factor-Alpha Therapy: Two Cases Report and Literature Review. Clin. Rheumatol. 2018, 37, 849–853. [Google Scholar] [CrossRef]
- Leclercq, M.; Andrillon, A.; Maalouf, G.; Sève, P.; Bielefeld, P.; Gueudry, J.; Sené, T.; Moulinet, T.; Rouvière, B.; Sène, D.; et al. Anti–Tumor Necrosis Factor α versus Tocilizumab in the Treatment of Refractory Uveitic Macular Edema. Ophthalmology 2022, 129, 520–529. [Google Scholar] [CrossRef]
- Miserocchi, E.; Modorati, G.; Berchicci, L.; Pontikaki, I.; Meroni, P.; Gerloni, V. Long-Term Treatment with Rituximab in Severe Juvenile Idiopathic Arthritis-Associated Uveitis. Br. J. Ophthalmol. 2016, 100, 782–786. [Google Scholar] [CrossRef]
- Abu El-Asrar, A.M.; Dheyab, A.; Khatib, D.; Struyf, S.; Van Damme, J.; Opdenakker, G. Efficacy of B Cell Depletion Therapy with Rituximab in Refractory Chronic Recurrent Uveitis Associated with Vogt-Koyanagi-Harada Disease. Ocul. Immunol. Inflamm. 2022, 30, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Bolletta, E.; Gozzi, F.; Mastrofilippo, V.; Pipitone, N.; De Simone, L.; Croci, S.; Invernizzi, A.; Adani, C.; Iannetta, D.; Coassin, M.; et al. Efficacy of Rituximab Treatment in Vogt-Koyanagi-Harada Disease Poorly Controlled by Traditional Immunosuppressive Treatment. Ocul. Immunol. Inflamm. 2022, 30, 1303–1308. [Google Scholar] [CrossRef] [PubMed]
- Davatchi, F.; Shams, H.; Rezaipoor, M.; Sadeghi-Abdollahi, B.; Shahram, F.; Nadji, A.; Chams-Davatchi, C.; Akhlaghi, M.; Faezi, T.; Naderi, N. Rituximab in Intractable Ocular Lesions of Behcet’s Disease; Randomized Single-Blind Control Study (Pilot Study). Int. J. Rheum. Dis. 2010, 13, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Joshi, L.; Lightman, S.L.; Salama, A.D.; Shirodkar, A.L.; Pusey, C.D.; Taylor, S.R.J. Rituximab in Refractory Ophthalmic Wegener’s Granulomatosis: PR3 Titers May Predict Relapse, but Repeat Treatment Can Be Effective. Ophthalmology 2011, 118, 2498–2503. [Google Scholar] [CrossRef]
- Ng, C.C.; Sy, A.; Cunningham, E.T. Rituximab for Non-Infectious Uveitis and Scleritis. J. Ophthalmic Inflamm. Infect. 2021, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Datta-Mannan, A. Mechanisms Influencing the Pharmacokinetics and Disposition of Monoclonal Antibodies and Peptides. Drug Metab. Dispos. 2019, 47, 1100–1110. [Google Scholar] [CrossRef] [Green Version]
- Pyzik, M.; Sand, K.M.K.; Hubbard, J.J.; Andersen, J.T.; Sandlie, I.; Blumberg, R.S. The Neonatal Fc Receptor (FcRn): A Misnomer? Front. Immunol. 2019, 10, 1540. [Google Scholar] [CrossRef] [Green Version]
- Ternant, D.; Azzopardi, N.; Raoul, W.; Bejan-Angoulvant, T.; Paintaud, G. Influence of Antigen Mass on the Pharmacokinetics of Therapeutic Antibodies in Humans. Clin. Pharmacokinet. 2019, 58, 169–187. [Google Scholar] [CrossRef]
- Ternant, D.; Ducourau, E.; Fuzibet, P.; Vignault, C.; Watier, H.; Lequerré, T.; Le Loët, X.; Vittecoq, O.; Goupille, P.; Mulleman, D.; et al. Pharmacokinetics and Concentration-Effect Relationship of Adalimumab in Rheumatoid Arthritis. Br. J. Clin. Pharmacol. 2015, 79, 286–297. [Google Scholar] [CrossRef] [Green Version]
- Weisman, M.H.; Moreland, L.W.; Furst, D.E.; Weinblatt, M.E.; Keystone, E.C.; Paulus, H.E.; Teoh, L.S.; Velagapudi, R.B.; Noertersheuser, P.A.; Granneman, G.R.; et al. Efficacy, Pharmacokinetic, and Safety Assessment of Adalimumab, a Fully Human Anti-Tumor Necrosis Factor-Alpha Monoclonal Antibody, in Adults with Rheumatoid Arthritis Receiving Concomitant Methotrexate: A Pilot Study. Clin. Ther. 2003, 25, 1700–1721. [Google Scholar] [CrossRef]
- AbbVie Ltd Humira (Adalimumab). Extension of Indication Variation Assessment Report; European Medicines Agency: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Matsuoka, K.; Hamada, S.; Shimizu, M.; Nanki, K.; Mizuno, S.; Kiyohara, H.; Arai, M.; Sugimoto, S.; Iwao, Y.; Ogata, H.; et al. Factors Contributing to the Systemic Clearance of Infliximab with Long-Term Administration in Japanese Patients with Crohn’s Disease: Analysis Using Population Pharmacokinetics. Int. J. Clin. Pharmacol. Ther. 2020, 58, 89–102. [Google Scholar] [CrossRef]
- Ng, C.M.; Bruno, R.; Combs, D.; Davies, B. Population Pharmacokinetics of Rituximab (Anti-CD20 Monoclonal Antibody) in Rheumatoid Arthritis Patients during a Phase II Clinical Trial. J. Clin. Pharmacol. 2005, 45, 792–801. [Google Scholar] [CrossRef]
- Lee, H.; Kimko, H.C.; Rogge, M.; Wang, D.; Nestorov, I.; Peck, C.C. Population Pharmacokinetic and Pharmacodynamic Modeling of Etanercept Using Logistic Regression Analysis. Clin. Pharmacol. Ther. 2003, 73, 348–365. [Google Scholar] [CrossRef] [PubMed]
- Adedokun, O.J.; Xu, Z.; Liao, S.; Strauss, R.; Reinisch, W.; Feagan, B.G.; Sandborn, W.J. Population Pharmacokinetics and Exposure-Response Modeling of Golimumab in Adults with Moderately to Severely Active Ulcerative Colitis. Clin. Ther. 2020, 42, 157–174. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S.; Eckert, D.; Hyams, J.S.; Mensing, S.; Thakkar, R.B.; Robinson, A.M.; Rosh, J.R.; Ruemmele, F.M.; Awni, W.M. Pharmacokinetics and Exposure-Efficacy Relationship of Adalimumab in Pediatric Patients with Moderate to Severe Crohn’s Disease: Results from a Randomized, Multicenter, Phase-3 Study. Inflamm. Bowel Dis. 2015, 21, 783–792. [Google Scholar] [CrossRef]
- Fasanmade, A.A.; Adedokun, O.J.; Blank, M.; Zhou, H.; Davis, H.M. Pharmacokinetic Properties of Infliximab in Children and Adults with Crohn’s Disease: A Retrospective Analysis of Data from 2 Phase III Clinical Trials. Clin. Ther. 2011, 33, 946–964. [Google Scholar] [CrossRef] [PubMed]
- Wolbink, G.J.; Voskuyl, A.E.; Lems, W.F.; de Groot, E.; Nurmohamed, M.T.; Tak, P.P.; Dijkmans, B.A.C.; Aarden, L. Relationship between Serum Trough Infliximab Levels, Pretreatment C Reactive Protein Levels, and Clinical Response to Infliximab Treatment in Patients with Rheumatoid Arthritis. Ann. Rheum. Dis. 2005, 64, 704–707. [Google Scholar] [CrossRef]
- Curtis, J.R.; Chakravarty, S.D.; Black, S.; Kafka, S.; Xu, S.; Langholff, W.; Parenti, D.; Greenspan, A.; Schwartzman, S. Incidence of Infusion Reactions and Clinical Effectiveness of Intravenous Golimumab Versus Infliximab in Patients with Rheumatoid Arthritis: The Real-World AWARE Study. Rheumatol. Ther. 2021, 8, 1551–1563. [Google Scholar] [CrossRef] [PubMed]
- Leinonen, S.T.; Aalto, K.; Kotaniemi, K.M.; Kivelä, T.T. Anti-Adalimumab Antibodies in Juvenile Idiopathic Arthritis-Related Uveitis. Clin. Exp. Rheumatol. 2017, 35, 1043–1046. [Google Scholar]
- Imaeda, H.; Takahashi, K.; Fujimoto, T.; Bamba, S.; Tsujikawa, T.; Sasaki, M.; Fujiyama, Y.; Andoh, A. Clinical Utility of Newly Developed Immunoassays for Serum Concentrations of Adalimumab and Anti-Adalimumab Antibodies in Patients with Crohn’s Disease. J. Gastroenterol. 2014, 49, 100–109. [Google Scholar] [CrossRef]
- Ding, X.; Zhu, R.; Wu, J.; Xue, L.; Gu, M.; Miao, L. Early Adalimumab and Anti-Adalimumab Antibody Levels for Prediction of Primary Nonresponse in Ankylosing Spondylitis Patients. Clin. Transl. Sci. 2020, 13, 547–554. [Google Scholar] [CrossRef]
- Brunelli, J.B.; Silva, C.A.; Pasoto, S.G.; Saa, C.G.S.; Kozu, K.T.; Goldenstein-Schainberg, C.; Leon, E.P.; Vendramini, M.B.G.; Fontoura, N.; Bonfa, E.; et al. Anti-Adalimumab Antibodies Kinetics: An Early Guide for Juvenile Idiopathic Arthritis (JIA) Switching. Clin. Rheumatol. 2020, 39, 515–521. [Google Scholar] [CrossRef]
- Skrabl-Baumgartner, A.; Erwa, W.; Muntean, W.; Jahnel, J. Anti-Adalimumab Antibodies in Juvenile Idiopathic Arthritis: Frequent Association with Loss of Response. Scand. J. Rheumatol. 2015, 44, 359–362. [Google Scholar] [CrossRef]
- Breedveld, F.C.; Weisman, M.H.; Kavanaugh, A.F.; Cohen, S.B.; Pavelka, K.; van Vollenhoven, R.; Sharp, J.; Perez, J.L.; Spencer-Green, G.T. The PREMIER Study: A Multicenter, Randomized, Double-Blind Clinical Trial of Combination Therapy with Adalimumab plus Methotrexate versus Methotrexate Alone or Adalimumab Alone in Patients with Early, Aggressive Rheumatoid Arthritis Who Had Not Had Previous Methotrexate Treatment. Arthritis Rheum. 2006, 54, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Lindström, U.; Di Giuseppe, D.; Delcoigne, B.; Glintborg, B.; Möller, B.; Ciurea, A.; Pombo-Suarez, M.; Sanchez-Piedra, C.; Eklund, K.; Relas, H.; et al. Effectiveness and Treatment Retention of TNF Inhibitors When Used as Monotherapy versus Comedication with CsDMARDs in 15 332 Patients with Psoriatic Arthritis. Data from the EuroSpA Collaboration. Ann. Rheum. Dis. 2021, 80, 1410–1418. [Google Scholar] [CrossRef] [PubMed]
- Ducourau, E.; Rispens, T.; Samain, M.; Dernis, E.; Le Guilchard, F.; Andras, L.; Perdriger, A.; Lespessailles, E.; Martin, A.; Cormier, G.; et al. Methotrexate Effect on Immunogenicity and Long-Term Maintenance of Adalimumab in Axial Spondyloarthritis: A Multicentric Randomised Trial. RMD Open 2020, 6, e001047. [Google Scholar] [CrossRef]
- van der Heijde, D.; Klareskog, L.; Rodriguez-Valverde, V.; Codreanu, C.; Bolosiu, H.; Melo-Gomes, J.; Tornero-Molina, J.; Wajdula, J.; Pedersen, R.; Fatenejad, S.; et al. Comparison of Etanercept and Methotrexate, Alone and Combined, in the Treatment of Rheumatoid Arthritis: Two-Year Clinical and Radiographic Results from the TEMPO Study, a Double-Blind, Randomized Trial. Arthritis Rheum. 2006, 54, 1063–1074. [Google Scholar] [CrossRef] [PubMed]
- Chatzidionysiou, K.; Lie, E.; Nasonov, E.; Lukina, G.; Hetland, M.L.; Tarp, U.; van Riel, P.L.C.M.; Nordström, D.C.; Gomez-Reino, J.; Pavelka, K.; et al. Effectiveness of Disease-Modifying Antirheumatic Drug Co-Therapy with Methotrexate and Leflunomide in Rituximab-Treated Rheumatoid Arthritis Patients: Results of a 1-Year Follow-up Study from the CERERRA Collaboration. Ann. Rheum. Dis. 2012, 71, 374–377. [Google Scholar] [CrossRef]
- Colombel, J.F.; Sandborn, W.J.; Reinisch, W.; Mantzaris, G.J.; Kornbluth, A.; Rachmilewitz, D.; Lichtiger, S.; D’Haens, G.; Diamond, R.H.; Broussard, D.L.; et al. Infliximab, Azathioprine, or Combination Therapy for Crohn’s Disease. N. Engl. J. Med. 2010, 362, 1383–1395. [Google Scholar] [CrossRef] [Green Version]
- Dulai, P.S.; Siegel, C.A.; Peyrin-Biroulet, L. Anti-Tumor Necrosis Factor-α Monotherapy versus Combination Therapy with an Immunomodulator in IBD. Gastroenterol. Clin. N. Am. 2014, 43, 441–456. [Google Scholar] [CrossRef]
- Klein, A.; Becker, I.; Minden, K.; Foeldvari, I.; Haas, J.P.; Horneff, G. Adalimumab versus Adalimumab and Methotrexate for the Treatment of Juvenile Idiopathic Arthritis: Long-Term Data from the German BIKER Registry. Scand. J. Rheumatol. 2019, 48, 95–104. [Google Scholar] [CrossRef]
- Feuerstein, J.D.; Isaacs, K.L.; Schneider, Y.; Siddique, S.M.; Falck-Ytter, Y.; Singh, S.; Chachu, K.; Day, L.; Lebwohl, B.; Muniraj, T.; et al. AGA Clinical Practice Guidelines on the Management of Moderate to Severe Ulcerative Colitis. Gastroenterology 2020, 158, 1450–1461. [Google Scholar] [CrossRef] [Green Version]
- Pouw, M.F.; Krieckaert, C.L.; Nurmohamed, M.T.; van der Kleij, D.; Aarden, L.; Rispens, T.; Wolbink, G. Key Findings towards Optimising Adalimumab Treatment: The Concentration–Effect Curve. Ann. Rheum. Dis. 2015, 74, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Mao, R.; Chen, B.; Zhang, S.; Guo, J.; He, Y.; Zeng, Z.; Ben-Horin, S.; Chen, M. Effects of Combination Therapy with Immunomodulators on Trough Levels and Antibodies Against Tumor Necrosis Factor Antagonists in Patients with Inflammatory Bowel Disease: A Meta-Analysis. Clin. Gastroenterol. Hepatol. 2017, 15, 1359–1372.e6. [Google Scholar] [CrossRef] [Green Version]
- Yao, J.; Jiang, X.; You, J.H.S. Proactive Therapeutic Drug Monitoring of Adalimumab for Pediatric Crohn’s Disease Patients: A Cost-effectiveness Analysis. J. Gastroenterol. Hepatol. 2021, 36, 2397–2407. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Arango, C.; Gorostiza, I.; Úcar, E.; García-Vivar, M.L.; Pérez, C.E.; De Dios, J.R.; Alvarez, B.; Ruibal-Escribano, A.; Stoye, C.; Vasques, M.; et al. Cost-Effectiveness of Therapeutic Drug Monitoring-Guided Adalimumab Therapy in Rheumatic Diseases: A Prospective, Pragmatic Trial. Rheumatol. Ther. 2021, 8, 1323–1339. [Google Scholar] [CrossRef]
- Fernandes, S.R.; Bernardo, S.; Simões, C.; Gonçalves, A.R.; Valente, A.; Baldaia, C.; Moura Santos, P.; Correia, L.A.; Tato Marinho, R. Proactive Infliximab Drug Monitoring Is Superior to Conventional Management in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2020, 26, 263–270. [Google Scholar] [CrossRef]
- Syversen, S.W.; Goll, G.L.; Jørgensen, K.K.; Sandanger, Ø.; Sexton, J.; Olsen, I.C.; Gehin, J.E.; Warren, D.J.; Brun, M.K.; Klaasen, R.A.; et al. Effect of Therapeutic Drug Monitoring vs Standard Therapy During Infliximab Induction on Disease Remission in Patients with Chronic Immune-Mediated Inflammatory Diseases: A Randomized Clinical Trial. JAMA 2021, 325, 1744–1754. [Google Scholar] [CrossRef]
- Ricciuto, A.; Dhaliwal, J.; Walters, T.D.; Griffiths, A.M.; Church, P.C. Clinical Outcomes with Therapeutic Drug Monitoring in Inflammatory Bowel Disease: A Systematic Review with Meta-Analysis. J. Crohns Colitis 2018, 12, 1302–1315. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.; Vermeire, S.; Lambrecht, G.; Baert, F.; Bossuyt, P.; Pariente, B.; Buisson, A.; Bouhnik, Y.; Filippi, J.; Vander Woude, J.; et al. Increasing Infliximab Dose Based on Symptoms, Biomarkers, and Serum Drug Concentrations Does Not Increase Clinical, Endoscopic, and Corticosteroid-Free Remission in Patients with Active Luminal Crohn’s Disease. Gastroenterology 2018, 154, 1343–1351.e1. [Google Scholar] [CrossRef]
- Sejournet, L.; Kerever, S.; Mathis, T.; Kodjikian, L.; Jamilloux, Y.; Seve, P. Therapeutic Drug Monitoring Guides the Management of Patients with Chronic Non-Infectious Uveitis Treated with Adalimumab: A Retrospective Study. Br. J. Ophthalmol. 2021, 106, 1380–1386. [Google Scholar] [CrossRef] [PubMed]
- Sugita, S.; Yamada, Y.; Mochizuki, M. Relationship between Serum Infliximab Levels and Acute Uveitis Attacks in Patients with Behcet Disease. Br. J. Ophthalmol. 2011, 95, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Assa, A.; Matar, M.; Turner, D.; Broide, E.; Weiss, B.; Ledder, O.; Guz-Mark, A.; Rinawi, F.; Cohen, S.; Topf-Olivestone, C.; et al. Proactive Monitoring of Adalimumab Trough Concentration Associated with Increased Clinical Remission in Children with Crohn’s Disease Compared with Reactive Monitoring. Gastroenterology 2019, 157, 985–996.e2. [Google Scholar] [CrossRef] [PubMed]
- Syed, N.; Tolaymat, M.; Brown, S.A.; Sivasailam, B.; Cross, R.K. Proactive Drug Monitoring Is Associated with Higher Persistence to Infliximab and Adalimumab Treatment and Lower Healthcare Utilization Compared with Reactive and Clinical Monitoring. Crohns Colitis 360 2020, 2, otaa050. [Google Scholar] [CrossRef]
- Papamichael, K.; Cheifetz, A.S. Is It Prime Time for Proactive Therapeutic Drug Monitoring of Anti-Tumor Necrosis Factor Therapy in Inflammatory Bowel Disease? Gastroenterology 2019, 157, 922–924. [Google Scholar] [CrossRef] [Green Version]
- Constantin, T.; Foeldvari, I.; Anton, J.; de Boer, J.; Czitrom -Guillaume, S.; Edelsten, C.; Gepstein, R.; Heiligenhaus, A.; Pilkington, C.A.; Simonini, G.; et al. Consensus-Based Recommendations for the Management of Uveitis Associated with Juvenile Idiopathic Arthritis: The SHARE Initiative. Ann. Rheum. Dis. 2018, 77, 1107–1117. [Google Scholar] [CrossRef]
- Bou, R.; Adán, A.; Borrás, F.; Bravo, B.; Calvo, I.; De Inocencio, J.; Díaz, J.; Escudero, J.; Fonollosa, A.; de Vicuña, C.G.; et al. Clinical Management Algorithm of Uveitis Associated with Juvenile Idiopathic Arthritis: Interdisciplinary Panel Consensus. Rheumatol. Int. 2015, 35, 777–785. [Google Scholar] [CrossRef]
- Kiely, P.D.W. Biologic Efficacy Optimization—A Step towards Personalized Medicine. Rheumatology 2016, 55, 780–788. [Google Scholar] [CrossRef] [Green Version]
- Papamichael, K.; Cheifetz, A.S. Use of Anti-TNF Drug Levels to Optimise Patient Management. Frontline Gastroenterol. 2016, 7, 289–300. [Google Scholar] [CrossRef] [Green Version]
- Hahn, A.; Burrell, A.; Chaney, H.; Sami, I.; Koumbourlis, A.C.; Freishtat, R.J.; Zemanick, E.T.; Louie, S.; Crandall, K.A. Importance of Beta-Lactam Pharmacokinetics and Pharmacodynamics on the Recovery of Microbial Diversity in the Airway of Persons with Cystic Fibrosis. J. Investig. Med. 2021, 69, 1350–1359. [Google Scholar] [CrossRef]
- Veiga, R.P.; Paiva, J.-A. Pharmacokinetics–Pharmacodynamics Issues Relevant for the Clinical Use of Beta-Lactam Antibiotics in Critically Ill Patients. Crit. Care 2018, 22, 233. [Google Scholar] [CrossRef] [Green Version]
- Bland, C.M.; Pai, M.P.; Lodise, T.P. Reappraisal of Contemporary Pharmacokinetic and Pharmacodynamic Principles for Informing Aminoglycoside Dosing. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2018, 38, 1229–1238. [Google Scholar] [CrossRef]
- Bastida, G.; Marín-Jiménez, I.; Forés, A.; García-Planella, E.; Argüelles-Arias, F.; Tagarro, I.; Fernandez-Nistal, A.; Montoto, C.; Aparicio, J.; Aguas, M.; et al. Treatment Patterns and Intensification within 5 Year of Follow-up of the First-Line Anti-TNFα Used for the Treatment of IBD: Results from the VERNE Study. Dig. Liver Dis. 2022, 54, 76–83. [Google Scholar] [CrossRef]
- Krieckaert, C.; Hernández-Breijo, B.; Gehin, J.E.; le Mélédo, G.; Balsa, A.; Jani, M.; Mulleman, D.; Navarro-Compan, V.; Wolbink, G.; Isaac, J.; et al. Therapeutic Drug Monitoring of Biopharmaceuticals in Inflammatory Rheumatic and Musculoskeletal Disease: A Systematic Literature Review Informing EULAR Points to Consider. RMD Open 2022, 8, e002216. [Google Scholar] [CrossRef] [PubMed]
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular Drug Delivery. AAPS J. 2010, 12, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Varela-Fernández, R.; Díaz-Tomé, V.; Luaces-Rodríguez, A.; Conde-Penedo, A.; García-Otero, X.; Luzardo-Álvarez, A.; Fernández-Ferreiro, A.; Otero-Espinar, F. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barar, J.; Aghanejad, A.; Fathi, M.; Omidi, Y. Advanced Drug Delivery and Targeting Technologies for the Ocular Diseases. BioImpacts 2016, 6, 49–67. [Google Scholar] [CrossRef] [Green Version]
- Caruso, A.; Füth, M.; Alvarez-Sánchez, R.; Belli, S.; Diack, C.; Maass, K.F.; Schwab, D.; Kettenberger, H.; Mazer, N.A. Ocular Half-Life of Intravitreal Biologics in Humans and Other Species: Meta-Analysis and Model-Based Prediction. Mol. Pharm. 2020, 17, 695–709. [Google Scholar] [CrossRef] [PubMed]
- Shivva, V.; Boswell, C.A.; Rafidi, H.; Kelley, R.F.; Kamath, A.V.; Crowell, S.R. Antibody Format and Serum Disposition Govern Ocular Pharmacokinetics of Intravenously Administered Protein Therapeutics. Front. Pharmacol. 2021, 12, 601569. [Google Scholar] [CrossRef] [PubMed]
- Simsek, M.; Cakar Ozdal, P.; Akbiyik, F.; Citirik, M.; Berker, N.; Ozdamar Erol, Y.; Yilmazbas, P. Aqueous Humor IL-8, IL-10, and VEGF Levels in Fuchs’ Uveitis Syndrome and Behçet’s Uveitis. Int. Ophthalmol. 2019, 39, 2629–2636. [Google Scholar] [CrossRef]
- Fukunaga, H.; Kaburaki, T.; Shirahama, S.; Tanaka, R.; Murata, H.; Sato, T.; Takeuchi, M.; Tozawa, H.; Urade, Y.; Katsura, M.; et al. Analysis of Inflammatory Mediators in the Vitreous Humor of Eyes with Pan-Uveitis According to Aetiological Classification. Sci. Rep. 2020, 10, 2783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Liu, C.-H.; Ji, T.; Mehta, M.; Wang, W.; Marino, E.; Chen, J.; Kohane, D.S. Intravenous Treatment of Choroidal Neovascularization by Photo-Targeted Nanoparticles. Nat. Commun. 2019, 10, 804. [Google Scholar] [CrossRef] [Green Version]
- Lamminsalo, M.; Karvinen, T.; Subrizi, A.; Urtti, A.; Ranta, V.-P. Extended Pharmacokinetic Model of the Intravitreal Injections of Macromolecules in Rabbits. Part 2: Parameter Estimation Based on Concentration Dynamics in the Vitreous, Retina, and Aqueous Humor. Pharm. Res. 2020, 37, 226. [Google Scholar] [CrossRef]
- García-Quintanilla, L.; Luaces-Rodríguez, A.; Gil-Martínez, M.; Mondelo-García, C.; Maroñas, O.; Mangas-Sanjuan, V.; González-Barcia, M.; Zarra-Ferro, I.; Aguiar, P.; Otero-Espinar, F.J.; et al. Pharmacokinetics of Intravitreal Anti-VEGF Drugs in Age-Related Macular Degeneration. Pharmaceutics 2019, 11, 365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamza, M.M.E.; Macky, T.A.; Sidky, M.K.; Ragab, G.; Soliman, M.M. Intravitreal Infliximab in Refractory Uveitis in Behcet’s Disease: A Safety and Efficacy Clinical Study. Retina 2016, 36, 2399–2408. [Google Scholar] [CrossRef] [PubMed]
- Farvardin, M.; Afarid, M.; Mehryar, M.; Hosseini, H. Intravitreal Infliximab for the Treatment of Sight-Threatening Chronic Noninfectious Uveitis. Retina 2010, 30, 1530–1535. [Google Scholar] [CrossRef]
- Refaat, M.; Abdullatif, A.M.; Hamza, M.M.; Macky, T.A.; El-Agha, M.-S.H.; Ragab, G.; Soliman, M.M. Monthly Intravitreal Infliximab in Behçet’s Disease Active Posterior Uveitis: A Long-Term Safety Study. Retina 2021, 41, 1739–1747. [Google Scholar] [CrossRef]
- Giganti, M.; Beer, P.M.; Lemanski, N.; Hartman, C.; Schartman, J.; Falk, N. Adverse Events after Intravitreal Infliximab (Remicade). Retina 2010, 30, 71–80. [Google Scholar] [CrossRef]
- Hamam, R.N.; Barikian, A.W.; Antonios, R.S.; Abdulaal, M.R.; Alameddine, R.M.; El Mollayess, G.; Mansour, A.M. Intravitreal Adalimumab in Active Noninfectious Uveitis: A Pilot Study. Ocul. Immunol. Inflamm. 2014, 24, 319–326. [Google Scholar] [CrossRef]
- Kheir, W.J.; Mehanna, C.-J.; Abdul Fattah, M.; Al Ghadban, S.; El Sabban, M.; Mansour, A.M.; Hamam, R.N. Intravitreal Adalimumab for the Control of Breakthrough Intraocular Inflammation. Ocul. Immunol. Inflamm. 2018, 26, 1206–1211. [Google Scholar] [CrossRef]
- Androudi, S.; Tsironi, E.; Kalogeropoulos, C.; Theodoridou, A.; Brazitikos, P. Intravitreal Adalimumab for Refractory Uveitis-Related Macular Edema. Ophthalmology 2010, 117, 1612–1616. [Google Scholar] [CrossRef]
- Tsilimbaris, M.; Diakonis, V.F.; Naoumidi, I.; Charisis, S.; Kritikos, I.; Chatzithanasis, G.; Papadaki, T.; Plainis, S. Evaluation of Potential Retinal Toxicity of Adalimumab (Humira). Graefes Arch. Clin. Exp. Ophthalmol. 2009, 247, 1119–1125. [Google Scholar] [CrossRef]
- Manzano, R.P.A.; Peyman, G.A.; Carvounis, P.E.; Damico, F.M.; Aguiar, R.G.; Ioshimoto, G.L.; Ventura, D.F.; Cursino, S.T.; Takahashi, W. Toxicity of High-Dose Intravitreal Adalimumab (Humira) in the Rabbit. J. Ocul. Pharmacol. Ther. 2011, 27, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Manzano, R.P.A.; Peyman, G.A.; Carvounis, P.E.; Kivilcim, M.; Khan, P.; Chevez-Barrios, P.; Takahashi, W. Ocular Toxicity of Intravitreous Adalimumab (Humira) in the Rabbit. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 907–911. [Google Scholar] [CrossRef]
- García-Otero, X.; Mondelo-García, C.; Bandín-Vilar, E.; Gómez-Lado, N.; Silva-Rodríguez, J.; Rey-Bretal, D.; Victoria Otero-Espinar, M.; Adan, A.; González-Barcia, M.; Aguiar, P.; et al. PET Study of Intravitreal Adalimumab Pharmacokinetics in a Uveitis Rat Model. Int. J. Pharm. 2022, 627, 122261. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.S.; Packer, M.; Lo, K.H.; Fasanmade, A.A.; Willerson, J.T. Anti-TNF Therapy Against Congestive Heart Failure Investigators Randomized, Double-Blind, Placebo-Controlled, Pilot Trial of Infliximab, a Chimeric Monoclonal Antibody to Tumor Necrosis Factor-Alpha, in Patients with Moderate-to-Severe Heart Failure: Results of the Anti-TNF Therapy Against Congestive Heart Failure (ATTACH) Trial. Circulation 2003, 107, 3133–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, B.R.; Nussenblatt, R.B.; Sen, H.N. Pharmacogenetics of Drugs Used in the Treatment of Ocular Inflammatory Diseases. Expert Opin. Drug Metab. Toxicol. 2013, 9, 875–882. [Google Scholar] [CrossRef]
- Liu, B.; Sen, H.N.; Nussenblatt, R. Susceptibility Genes and Pharmacogenetics in Ocular Inflammatory Disorders. Ocul. Immunol. Inflamm. 2012, 20, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Bek, S.; Bojesen, A.B.; Nielsen, J.V.; Sode, J.; Bank, S.; Vogel, U.; Andersen, V. Systematic Review and Meta-Analysis: Pharmacogenetics of Anti-TNF Treatment Response in Rheumatoid Arthritis. Pharmacogenomics J. 2017, 17, 403–411. [Google Scholar] [CrossRef] [Green Version]
- Bank, S.; Andersen, P.S.; Burisch, J.; Pedersen, N.; Roug, S.; Galsgaard, J.; Turino, S.Y.; Brodersen, J.B.; Rashid, S.; Rasmussen, B.K.; et al. Associations between Functional Polymorphisms in the NFκB Signaling Pathway and Response to Anti-TNF Treatment in Danish Patients with Inflammatory Bowel Disease. Pharmacogenomics J. 2014, 14, 526–534. [Google Scholar] [CrossRef] [Green Version]
- Bank, S.; Julsgaard, M.; Abed, O.K.; Burisch, J.; Broder Brodersen, J.; Pedersen, N.K.; Gouliaev, A.; Ajan, R.; Nytoft Rasmussen, D.; Honore Grauslund, C.; et al. Polymorphisms in the NFkB, TNF-Alpha, IL-1beta, and IL-18 Pathways Are Associated with Response to Anti-TNF Therapy in Danish Patients with Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2019, 49, 890–903. [Google Scholar] [CrossRef] [PubMed]
- Hässler, S.; Bachelet, D.; Duhaze, J.; Szely, N.; Gleizes, A.; Hacein-Bey Abina, S.; Aktas, O.; Auer, M.; Avouac, J.; Birchler, M.; et al. Clinicogenomic Factors of Biotherapy Immunogenicity in Autoimmune Disease: A Prospective Multicohort Study of the ABIRISK Consortium. PLoS Med. 2020, 17, e1003348. [Google Scholar] [CrossRef]
- Bartelds, G.M.; Wijbrandts, C.A.; Nurmohamed, M.T.; Wolbink, G.J.; de Vries, N.; Tak, P.P.; Dijkmans, B.A.C.; Crusius, J.B.A.; vand der Horst-Bruinsma, I.E. Anti-Adalimumab Antibodies in Rheumatoid Arthritis Patients Are Associated with Interleukin-10 Gene Polymorphisms. Arthritis Rheum. 2009, 60, 2541–2542. [Google Scholar] [CrossRef]
- Pratesi, S.; Nencini, F.; Grosso, F.; Dies, L.; Bormioli, S.; Cammelli, D.; Maggi, E.; Matucci, A.; Vultaggio, A. ABIRISK Consortium T Cell Response to Infliximab in Exposed Patients: A Longitudinal Analysis. Front. Immunol. 2019, 9, 3113. [Google Scholar] [CrossRef]
- Sazonovs, A.; Kennedy, N.A.; Moutsianas, L.; Heap, G.A.; Rice, D.L.; Reppell, M.; Bewshea, C.M.; Chanchlani, N.; Walker, G.J.; Perry, M.H.; et al. HLA-DQA1*05 Carriage Associated with Development of Anti-Drug Antibodies to Infliximab and Adalimumab in Patients with Crohn’s Disease. Gastroenterology 2020, 158, 189–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andre, F.; Ismaila, N.; Allison, K.H.; Barlow, W.E.; Collyar, D.E.; Damodaran, S.; Henry, N.L.; Jhaveri, K.; Kalinsky, K.; Kuderer, N.M.; et al. Biomarkers for Adjuvant Endocrine and Chemotherapy in Early-Stage Breast Cancer: ASCO Guideline Update. J. Clin. Oncol. 2022, 40, 1816–1837. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Busto-Iglesias, M.; Rodríguez-Martínez, L.; Rodríguez-Fernández, C.A.; González-López, J.; González-Barcia, M.; de Domingo, B.; Rodríguez-Rodríguez, L.; Fernández-Ferreiro, A.; Mondelo-García, C. Perspectives of Therapeutic Drug Monitoring of Biological Agents in Non-Infectious Uveitis Treatment: A Review. Pharmaceutics 2023, 15, 766. https://doi.org/10.3390/pharmaceutics15030766
Busto-Iglesias M, Rodríguez-Martínez L, Rodríguez-Fernández CA, González-López J, González-Barcia M, de Domingo B, Rodríguez-Rodríguez L, Fernández-Ferreiro A, Mondelo-García C. Perspectives of Therapeutic Drug Monitoring of Biological Agents in Non-Infectious Uveitis Treatment: A Review. Pharmaceutics. 2023; 15(3):766. https://doi.org/10.3390/pharmaceutics15030766
Chicago/Turabian StyleBusto-Iglesias, Manuel, Lorena Rodríguez-Martínez, Carmen Antía Rodríguez-Fernández, Jaime González-López, Miguel González-Barcia, Begoña de Domingo, Luis Rodríguez-Rodríguez, Anxo Fernández-Ferreiro, and Cristina Mondelo-García. 2023. "Perspectives of Therapeutic Drug Monitoring of Biological Agents in Non-Infectious Uveitis Treatment: A Review" Pharmaceutics 15, no. 3: 766. https://doi.org/10.3390/pharmaceutics15030766