
Microenvironmental pH Modification in Buccal/Sublingual Dosage Forms for Systemic Drug Delivery


Abstract
:1. Introduction
2. Concept of Microenvironmental pH (pHM) Modification in the Buccal/Sublingual Dosage Forms
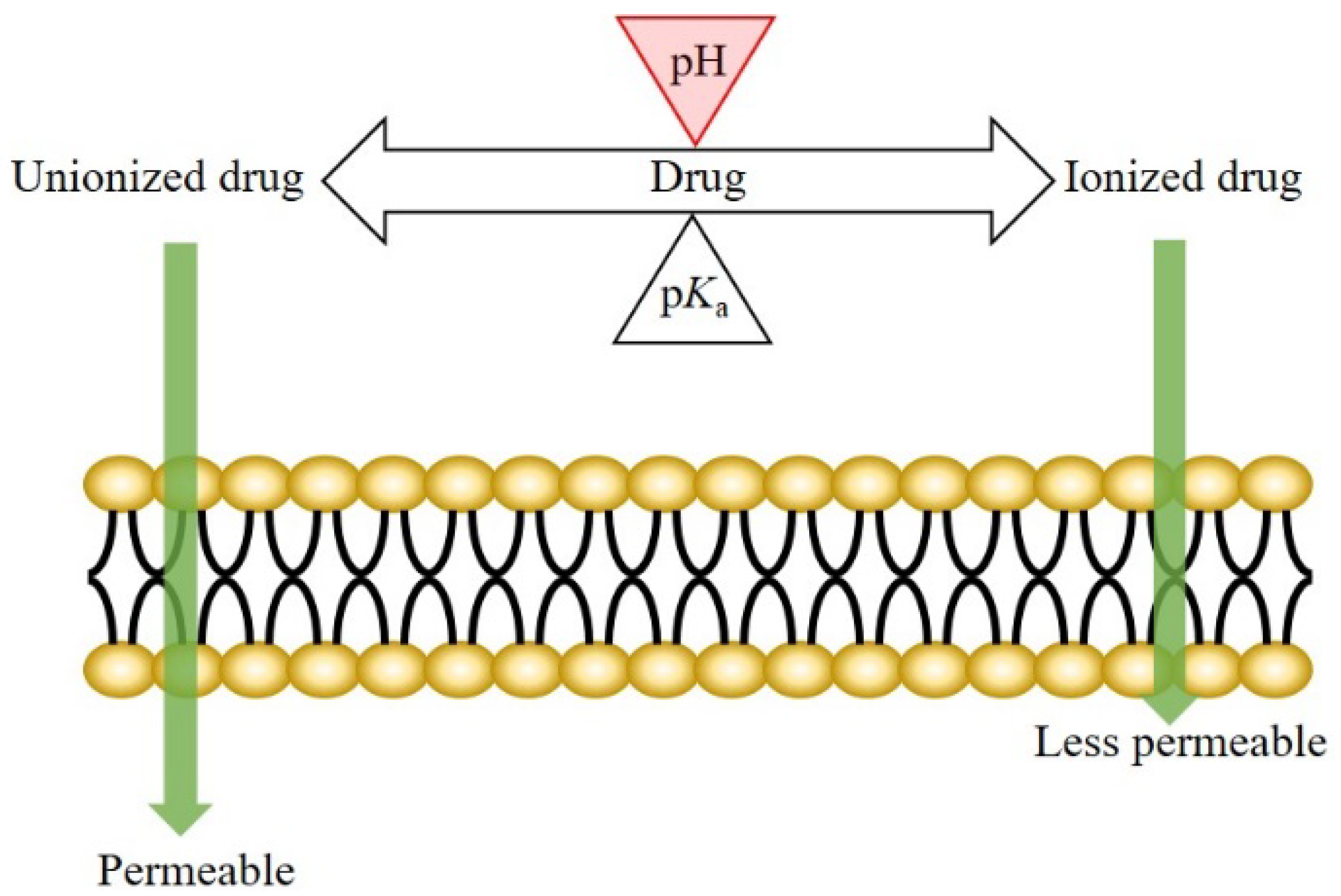
2.1. Theory: pH-Dependent Dissolution and Permeation
2.2. pHmax Concept
2.3. Microenvironmental pH Modification in Buccal/Sublingual Dosage Forms
3. Properties of Saliva Associated with pH Modification
3.1. pH and Buffer Capacity of Saliva
3.2. Secretion Rate of Saliva and Thickness of Salivary Film
4. Drug Candidate and pH Modifier for Buccal/Sublingual Dosage Forms
4.1. Drug Candidate
4.2. pH Modifier
5. Methods for Microenvironmental pH Measurement
5.1. pH Electrode Approach
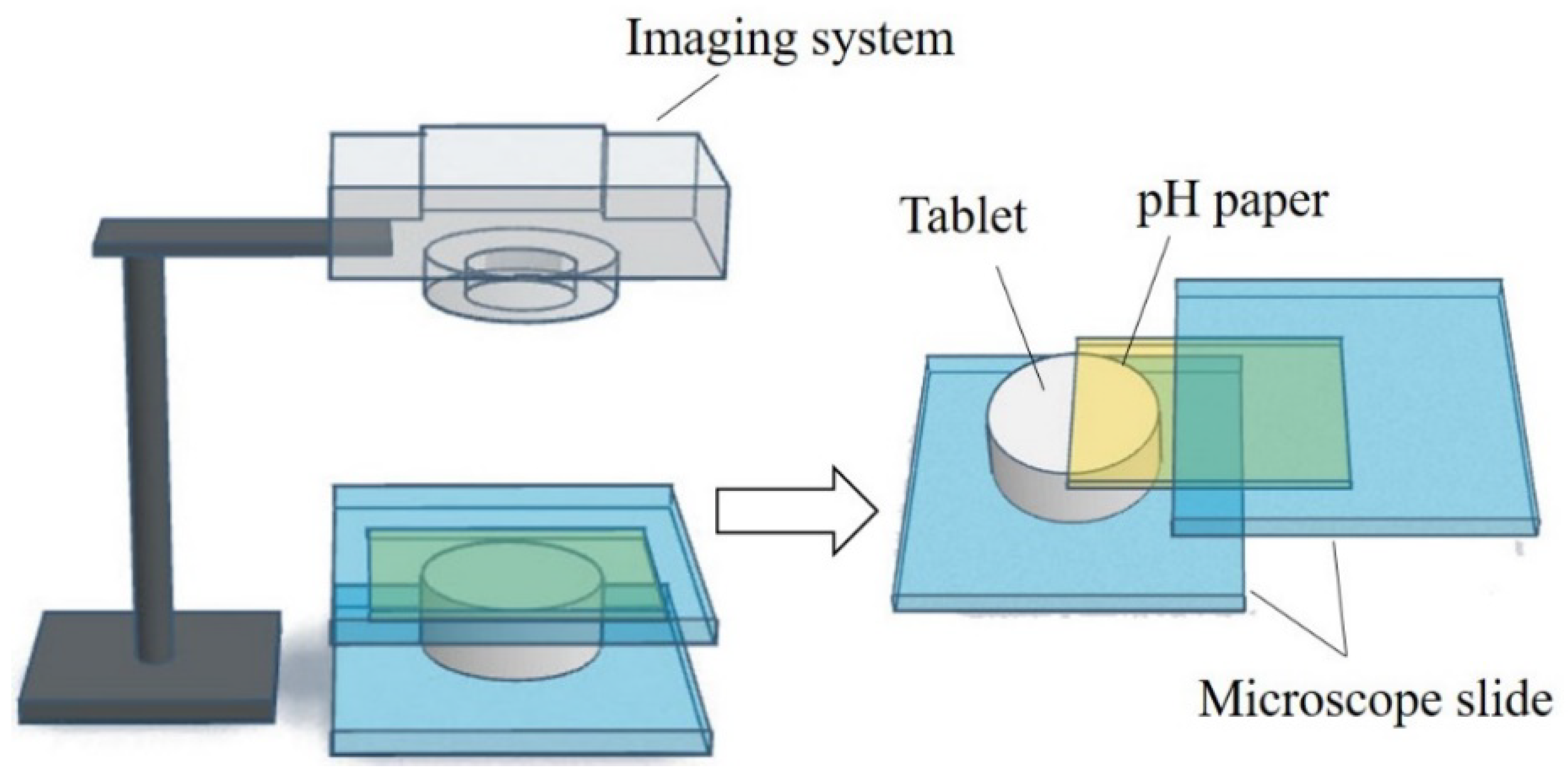
5.2. Computer-Enhanced Color Images Method
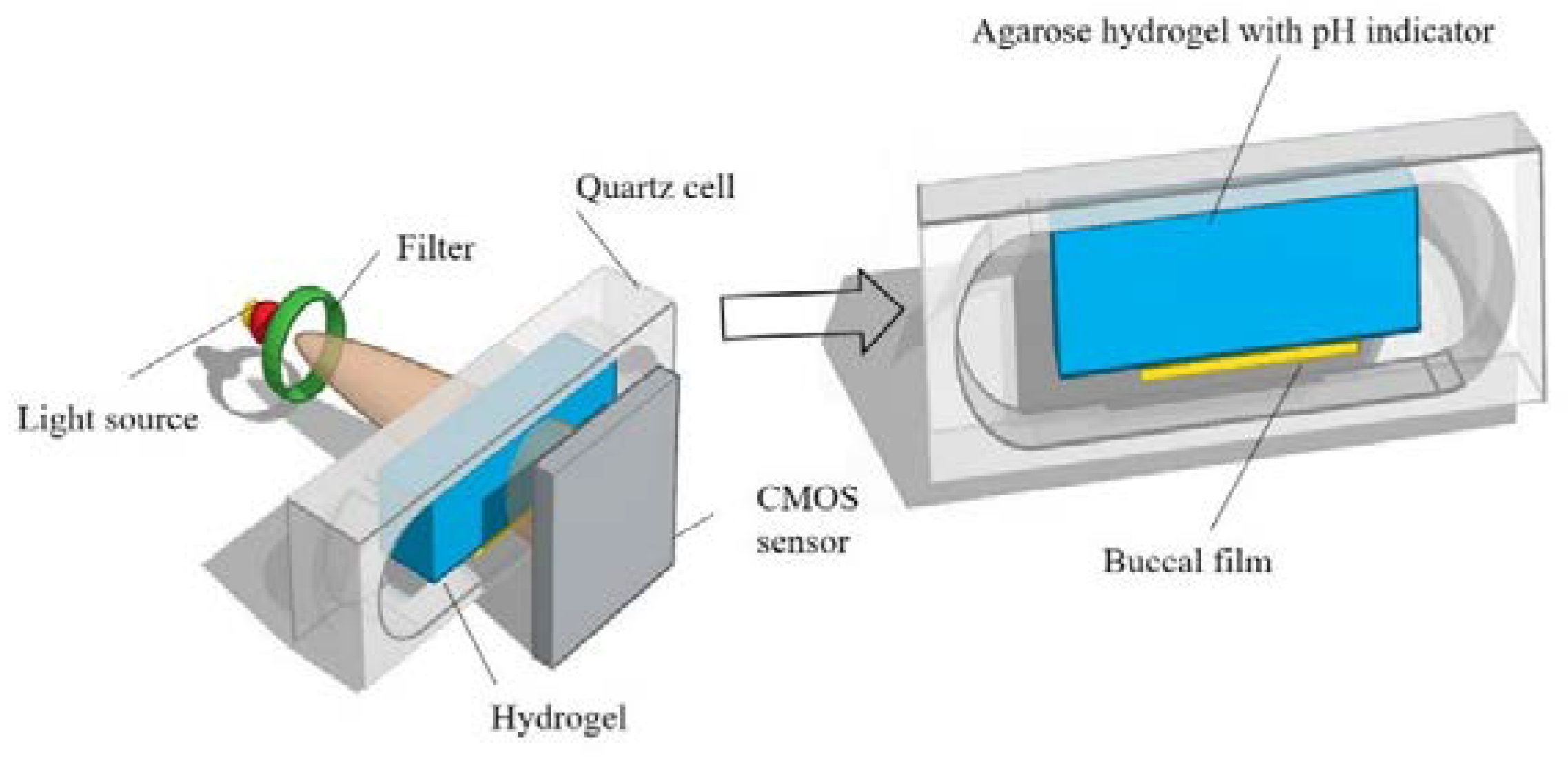
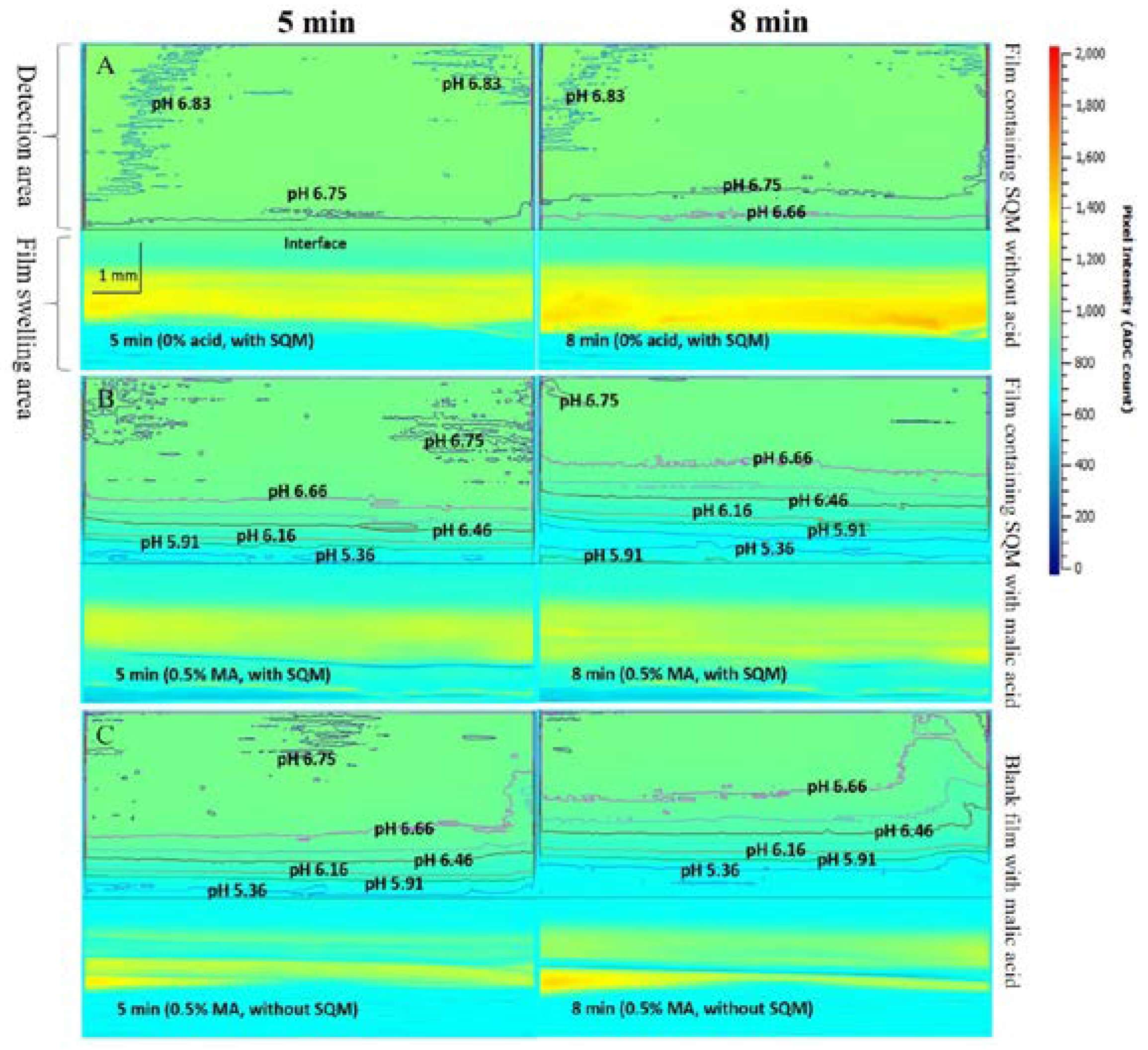
5.3. UV/Vis Imaging Method
6. Microenvironmental pH (pHM) Modification Methods
6.1. Microenvironmental pH Modification Using Acidifying/Alkalizing Agents
6.2. Microenvironmental pH Modification Using Buffering Agents
6.3. Microenvironmental pH Modification Using Effervescence
7. Challenges
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Macedo, A.S.; Castro, P.M.; Roque, L.; Thomé, N.G.; Reis, C.P.; Pintado, M.E.; Fonte, P. Novel and Revisited Approaches in Nanoparticle Systems for Buccal Drug Delivery. J. Control. Release 2020, 320, 125–141. [Google Scholar] [CrossRef]
- Madhav, N.V.S.; Shakya, A.K.; Shakya, P.; Singh, K. Orotransmucosal Drug Delivery Systems: A Review. J. Control. Release 2009, 140, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.K.W.; Xu, Y.; Worsley, A.; Wong, I.C.K. Oral Transmucosal Drug Delivery for Pediatric Use. Adv. Drug Deliv. Rev. 2014, 73, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, J.; Streisand, J.B. Oral Mucosal Drug Delivery. Clin. Pharmacokinet. 2002, 41, 661–680. [Google Scholar] [CrossRef]
- Loftsson, T.; Brewster, M.E. Pharmaceutical Applications of Cyclodextrins: Basic Science and Product Development. J. Pharm. Pharmacol. 2010, 62, 1607–1621. [Google Scholar] [CrossRef]
- Taniguchi, C.; Kawabata, Y.; Wada, K.; Yamada, S.; Onoue, S. Microenvironmental PH-Modification to Improve Dissolution Behavior and Oral Absorption for Drugs with PH-Dependent Solubility. Expert Opin. Drug Deliv. 2014, 11, 505–516. [Google Scholar] [CrossRef]
- Yang, M.; He, S.; Fan, Y.; Wang, Y.; Ge, Z.; Shan, L.; Gong, W.; Huang, X.; Tong, Y.; Gao, C. Microenvironmental PH-Modified Solid Dispersions to Enhance the Dissolution and Bioavailability of Poorly Water-Soluble Weakly Basic GT0918, a Developing Anti-Prostate Cancer Drug: Preparation, Characterization and Evaluation in Vivo. Int. J. Pharm. 2014, 475, 97–109. [Google Scholar] [CrossRef]
- Badawy, S.I.F.; Hussain, M.A. Microenvironmental PH Modulation in Solid Dosage Forms. J. Pharm. Sci. 2007, 96, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Doherty, C.; York, P. Microenvironmental PH Control of Drug Dissolution. Int. J. Pharm. 1989, 50, 223–232. [Google Scholar] [CrossRef]
- Younes, N.F.; El Assasy, A.E.-H.I.; Makhlouf, A.I.A. Microenvironmental PH-Modified Amisulpride-Labrasol Matrix Tablets: Development, Optimization and in Vivo Pharmacokinetic Study. Drug Deliv. Transl. Res. 2020, 11, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Onoue, S.; Inoue, R.; Taniguchi, C.; Kawabata, Y.; Yamashita, K.; Wada, K.; Yamauchi, Y.; Yamada, S. Improved Dissolution and Pharmacokinetic Behavior of Dipyridamole Formulation with Microenvironmental PH-Modifier under Hypochlorhydria. Int. J. Pharm. 2012, 426, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Mitra, A.; Kesisoglou, F.; Beauchamp, M.; Zhu, W.; Chiti, F.; Wu, Y. Using Absorption Simulation and Gastric PH Modulated Dog Model for Formulation Development To Overcome Achlorhydria Effect. Mol. Pharm. 2011, 8, 2216–2223. [Google Scholar] [CrossRef] [PubMed]
- Koziolek, M.; Grimm, M.; Becker, D.; Iordanov, V.; Zou, H.; Shimizu, J.; Wanke, C.; Garbacz, G.; Weitschies, W. Investigation of PH and Temperature Profiles in the GI Tract of Fasted Human Subjects Using the Intellicap® System. J. Pharm. Sci. 2015, 104, 2855–2863. [Google Scholar] [CrossRef] [PubMed]
- Baliga, S.; Muglikar, S.; Kale, R. Salivary PH: A Diagnostic Biomarker. J. Indian Soc. Periodontol. 2013, 17, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Ciolino, L.A.; McCauley, H.A.; Fraser, D.B.; Wolnik, K.A. The Relative Buffering Capacities of Saliva and Moist Snuff: Implications for Nicotine Absorption. J. Anal. Toxicol. 2001, 25, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Proctor, G.B. The Physiology of Salivary Secretion. Periodontology 2000 2016, 70, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Dawes, C. Physiological Factors Affecting Salivary Flow Rate, Oral Sugar Clearance, and the Sensation of Dry Mouth in Man. J. Dent. Res. 1987, 66, 648–653. [Google Scholar] [CrossRef]
- Dokoumetzidis, A.; Macheras, P. A Century of Dissolution Research: From Noyes and Whitney to the Biopharmaceutics Classification System. Int. J. Pharm. 2006, 321, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Avdeef, A. Solubility of Sparingly-Soluble Ionizable Drugs. Adv. Drug Deliv. Rev. 2007, 59, 568–590. [Google Scholar] [CrossRef] [PubMed]
- Bassi, P.; Kaur, G. PH Modulation: A Mechanism to Obtain PH-Independent Drug Release. Expert Opin. Drug Deliv. 2010, 7, 845–857. [Google Scholar] [CrossRef] [PubMed]
- Pather, S.I.; Rathbone, M.J.; Şenel, S. Current Status and the Future of Buccal Drug Delivery Systems. Expert Opin. Drug Deliv. 2008, 5, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Mashru, R.; Sutariya, V.; Sankalia, M.; Sankalia, J. Transbuccal Delivery of Lamotrigine across Porcine Buccal Mucosa: In Vitro Determination of Routes of Buccal Transport. J. Pharm. Pharm. Sci. 2005, 8, 54–62. [Google Scholar]
- Birudaraj, R.a.j.; Berner, B.; Shen, S.; Li, X. Buccal Permeation of Buspirone: Mechanistic Studies on Transport Pathways. J. Pharm. Sci. 2005, 94, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, H.M.; Rassing, M.R. Nicotine Permeability across the Buccal TR146 Cell Culture Model and Porcine Buccal Mucosa in Vitro: Effect of PH and Concentration. Eur. J. Pharm. Sci. 2002, 16, 151–157. [Google Scholar] [CrossRef]
- Thomae, A.V.; Wunderli-Allenspach, H.; Krämer, S.D. Permeation of Aromatic Carboxylic Acids across Lipid Bilayers: The PH-Partition Hypothesis Revisited. Biophys. J. 2005, 89, 1802–1811. [Google Scholar] [CrossRef] [PubMed]
- Shore, P.A.; Brodie, B.B.; Hogben, C.A.M. The Gastric Secretion of Drugs: A Ph Partition Hypothesis. J. Pharmacol. Exp. Ther. 1957, 119, 361–369. [Google Scholar] [PubMed]
- Wang, Y.; Zuo, Z.; Chen, X.; Tomlinson, B.; Chow, M.S.S. Improving Sublingual Delivery of Weak Base Compounds Using PHmax Concept: Application to Propranolol. Eur. J. Pharm. Sci. 2010, 39, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Meng-Lund, E.; Jacobsen, J.; Andersen, M.B.; Jespersen, M.L.; Karlsson, J.-J.; Garmer, M.; Jørgensen, E.B.; Holm, R. Conscious and Anaesthetised Göttingen Mini-Pigs as an in-Vivo Model for Buccal Absorption—PH-Dependent Absorption of Metoprolol from Bioadhesive Tablets. Drug Dev. Ind. Pharm. 2014, 40, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Holm, R.; Meng-Lund, E.; Andersen, M.B.; Jespersen, M.L.; Karlsson, J.-J.; Garmer, M.; Jørgensen, E.B.; Jacobsen, J. In Vitro, Ex Vivo and in Vivo Examination of Buccal Absorption of Metoprolol with Varying PH in TR146 Cell Culture, Porcine Buccal Mucosa and Göttingen Minipigs. Eur. J. Pharm. Sci. 2013, 49, 117–124. [Google Scholar] [CrossRef]
- Dodds, M.; Roland, S.; Edgar, M.; Thornhill, M. Saliva A Review of Its Role in Maintaining Oral Health and Preventing Dental Disease. BDJ Team 2015, 2, 15123. [Google Scholar] [CrossRef]
- de Almeida, P.D.V.; Grégio, A.M.T.; Machado, M.A.; de Lima, A.A.S.; Azevedo, L.R. Saliva Composition and Functions: A Comprehensive Review. J. Contemp. Dent. Pract. 2008, 9, 72–80. [Google Scholar] [PubMed]
- Patel, V.F.; Liu, F.; Brown, M.B. Advances in Oral Transmucosal Drug Delivery. J. Control. Release 2011, 153, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Aframian, D.; Davidowitz, T.; Benoliel, R. The Distribution of Oral Mucosal PH Values in Healthy Saliva Secretors. Oral Dis. 2006, 12, 420–423. [Google Scholar] [CrossRef]
- Tenovuo, J. Salivary Parameters of Relevance for Assessing Caries Activity in Individuals and Populations. Community Dent. Oral Epidemiol. 1997, 25, 82–86. [Google Scholar] [CrossRef]
- Lazarchik, D.A.; Filler, S.J. Effects of Gastroesophageal Reflux on the Oral Cavity. Am. J. Med. 1997, 103, 107S–113S. [Google Scholar] [CrossRef] [PubMed]
- Bardow, A.; Moe, D.; Nyvad, B.; Nauntofte, B. The Buffer Capacity and Buffer Systems of Human Whole Saliva Measured without Loss of CO2. Arch. Oral Biol. 2000, 45, 1–12. [Google Scholar] [CrossRef]
- Pedersen, A.M.L.; Sørensen, C.E.; Proctor, G.B.; Carpenter, G.H.; Ekström, J. Salivary Secretion in Health and Disease. J. Oral Rehabil. 2018, 45, 730–746. [Google Scholar] [CrossRef]
- Pijpe, J.; Kalk, W.W.I.; Bootsma, H.; Spijkervet, F.K.L.; Kallenberg, C.G.M.; Vissink, A. Progression of Salivary Gland Dysfunction in Patients with Sjögren’s Syndrome. Ann. Rheum. Dis. 2007, 66, 107–112. [Google Scholar] [CrossRef]
- Heintze, U.; Birkhed, D.; Björn, H. Secretion Rate and Buffer Effect of Resting and Stimulated Whole Saliva as a Function of Age and Sex. Swed. Dent. J. 1983, 7, 227–238. [Google Scholar]
- Collins, L.M.C.; Dawes, C. The Surface Area of the Adult Human Mouth and Thickness of the Salivary Film Covering the Teeth and Oral Mucosa. J. Dent. Res. 1987, 66, 1300–1302. [Google Scholar] [CrossRef]
- Derrien, M.; van Passel, M.W.J.; van de Bovenkamp, J.H.B.; Schipper, R.; de Vos, W.; Dekker, J. Mucin-Bacterial Interactions in the Human Oral Cavity and Digestive Tract. Gut Microbes 2010, 1, 254–268. [Google Scholar] [CrossRef] [PubMed]
- Osailan, S.; Pramanik, R.; Shirodaria, S.; Challacombe, S.; Proctor, G. Investigating the Relationship between Hyposalivation and Mucosal Wetness. Oral Dis. 2011, 17, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Fang, X.; Li, X. Transbuccal Delivery of 2′,3′-Dideoxycytidine: In Vitro Permeation Study and Histological Investigation. Int. J. Pharm. 2002, 231, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Deneer, V.H.M.; Drese, G.B.; Roemelé, P.E.H.; Verhoef, J.C.; Lie-A-Huen, L.; Kingma, J.H.; Brouwers, J.R.B.J.; Junginger, H.E. Buccal Transport of Flecainide and Sotalol: Effect of a Bile Salt and Ionization State. Int. J. Pharm. 2002, 241, 127–134. [Google Scholar] [CrossRef]
- Easa, N.; Alany, R.G.; Carew, M.; Vangala, A. A Review of Non-Invasive Insulin Delivery Systems for Diabetes Therapy in Clinical Trials over the Past Decade. Drug Discov. Today 2019, 24, 440–451. [Google Scholar] [CrossRef]
- Morales, J.O.; Brayden, D.J. Buccal Delivery of Small Molecules and Biologics: Of Mucoadhesive Polymers, Films, and Nanoparticles. Curr. Opin. Pharmacol. 2017, 36, 22–28. [Google Scholar] [CrossRef]
- Heinemann, L.; Jacques, Y. Oral Insulin and Buccal Insulin: A Critical Reappraisal. J. Diabetes Sci. Technol. 2009, 3, 568–584. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA-Approved Drugs Database. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm (accessed on 1 October 2022).
- Zamora, W.J.; Curutchet, C.; Campanera, J.M.; Luque, F.J. Prediction of PH-Dependent Hydrophobic Profiles of Small Molecules from Miertus–Scrocco–Tomasi Continuum Solvation Calculations. J. Phys. Chem. B 2017, 121, 9868–9880. [Google Scholar] [CrossRef]
- Zamora, W.J.; Campanera, J.M.; Luque, F.J. Development of a Structure-Based, PH-Dependent Lipophilicity Scale of Amino Acids from Continuum Solvation Calculations. J. Phys. Chem. Lett. 2019, 10, 883–889. [Google Scholar] [CrossRef]
- Xing, L.; Glen, R.C. Novel Methods for the Prediction of LogP, PKa, and LogD. J. Chem. Inf. Comput. Sci. 2002, 42, 796–805. [Google Scholar] [CrossRef]
- Iwanaga, K.; Kato, S.; Miyazaki, M.; Kakemi, M. Enhancing the Intestinal Absorption of Poorly Water-Soluble Weak-Acidic Compound by Controlling Local PH. Drug Dev. Ind. Pharm. 2013, 39, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- Henderson—Hasselbalch Equation. In Manual of Pharmacologic Calculations: With Computer Programs; Tallarida, R.J.; Murray, R.B. (Eds.) Springer: New York, NY, USA, 1987; pp. 74–75. ISBN 978-1-4612-4974-0. [Google Scholar]
- Durfee, S.; Messina, J.; Khankari, R. Fentanyl Effervescent Buccal Tablets. Am. J. Drug Deliv. 2006, 4, 1–5. [Google Scholar] [CrossRef]
- Darwish, M.; Hamed, E.; Messina, J. Fentanyl Buccal Tablet for the Treatment of Breakthrough Pain: Pharmacokinetics of Buccal Mucosa Delivery and Clinical Efficacy. Perspect. Med. Chem. 2010, 4, 11–21. [Google Scholar] [CrossRef]
- Darwish, M.; Tempero, K.; Jiang, J.G.; Simonson, P.G. Relative Bioavailability of Fentanyl Following Various Dosing Regimens of Fentanyl Buccal Tablet in Healthy Japanese Volunteers. Arch. Drug Inf. 2008, 1, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Elagamy, H.I.; Essa, E.A.; Nouh, A.; El Maghraby, G.M. Development and Evaluation of Rapidly Dissolving Buccal Films of Naftopidil: In Vitro and in Vivo Evaluation. Drug Dev. Ind. Pharm. 2019, 45, 1695–1706. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Østergaard, J.; Ashna, M.; Nielsen, C.U.; Jacobsen, J.; Mu, H. Microenvironmental PH Modifying Films for Buccal Delivery of Saquinavir: Effects of Organic Acids on PH and Drug Release in Vitro. Int. J. Pharm. 2020, 585, 119567. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Jacobsen, J.; Nielsen, C.U.; Genina, N.; Østergaard, J.; Mu, H. Exploration of in Vitro Drug Release Testing Methods for Saquinavir Microenvironmental PH Modifying Buccal Films. Eur. J. Pharm. Sci. 2021, 163, 105867. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Radeke, C.; Jacobsen, J.; Lind, J.U.; Mu, H. Multi-Material 3D Printing of Programmable and Stretchable Oromucosal Patches for Delivery of Saquinavir. Int. J. Pharm. 2021, 610, 121236. [Google Scholar] [CrossRef]
- He, S.; Nielsen, C.U.; Mu, H.; Jacobsen, J. In Vitro and Ex Vivo Evaluation of Bilayered Effervescent Microenvironmental PH Modifying Buccal Films with Saquinavir. J. Drug Deliv. Sci. Technol. 2022, 78, 103954. [Google Scholar] [CrossRef]
- Fouad, S.A.; Shamma, R.N.; Basalious, E.B.; El-Nabarawi, M.A.; Tayel, S.A. Novel Instantly-Soluble Transmucosal Matrix (ISTM) Using Dual Mechanism Solubilizer for Sublingual and Nasal Delivery of Dapoxetine Hydrochloride: In-Vitro/in-Vivo Evaluation. Int. J. Pharm. 2016, 505, 212–222. [Google Scholar] [CrossRef]
- Aldawsari, H.M.; Badr-Eldin, S.M. Enhanced Pharmacokinetic Performance of Dapoxetine Hydrochloride via the Formulation of Instantly-Dissolving Buccal Films with Acidic PH Modifier and Hydrophilic Cyclodextrin: Factorial Analysis, in Vitro and in Vivo Assessment. J. Adv. Res. 2020, 24, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Pongjanyakul, T.; Kanjanabat, S. Influence of PH Modifiers and HPMC Viscosity Grades on Nicotine–Magnesium Aluminum Silicate Complex-Loaded Buccal Matrix Tablets. AAPS PharmSciTech 2012, 13, 674–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, M.K.; Chetty, D.J.; Chien, Y.W.; Ho, H. Biomembrane Permeation of Nicotine: Mechanistic Studies with Porcine Mucosae and Skin. J. Pharm. Sci. 1997, 86, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-L.H.; Chetty, D.J.; Chien, Y.W. A Mechanistic Analysis to Characterize Oramucosal Permeation Properties. Int. J. Pharm. 1999, 184, 63–72. [Google Scholar] [CrossRef]
- The United States. Pharmacopeial Convention Excipients: USP and NF Excipients, Listed by Functional Category. In United States Pharmacopeia and National Formulary; The United States Pharmacopeial Convention: North Bethesda, MD, USA, 2016; p. 7490. [Google Scholar]
- Food and Drug Administration. FDA-Inactive Ingredient Search for Approved Drug Products Search. Available online: https://www.accessdata.fda.gov/scripts/cder/iig/index.cfm (accessed on 1 October 2022).
- Adhikary, A.; Vavia, P.R. Bioadhesive Ranitidine Hydrochloride for Gastroretention with Controlled Microenvironmental PH. Drug Dev. Ind. Pharm. 2008, 34, 860–869. [Google Scholar] [CrossRef]
- Ching, A.L.; Liew, C.V.; Chan, L.W.; Heng, P.W.S. Modifying Matrix Micro-Environmental PH to Achieve Sustained Drug Release from Highly Laminating Alginate Matrices. Eur. J. Pharm. Sci. 2008, 33, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Pudipeddi, M.; Zannou, E.A.; Vasanthavada, M.; Dontabhaktuni, A.; Royce, A.E.; Joshi, Y.M.; Serajuddin, A.T.M. Measurement of Surface PH of Pharmaceutical Solids: A Critical Evaluation of Indicator Dye-sorption Method and Its Comparison with Slurry PH Method. J. Pharm. Sci. 2008, 97, 1831–1842. [Google Scholar] [CrossRef]
- Siepe, S.; Lueckel, B.; Kramer, A.; Ries, A.; Gurny, R. Assessment of Tailor-Made HPMC-Based Matrix Minitablets Comprising a Weakly Basic Drug Compound. Drug Dev. Ind. Pharm. 2008, 34, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Eisenächer, F.; Schädlich, A.; Mäder, K. Monitoring of Internal PH Gradients within Multi-Layer Tablets by Optical Methods and EPR Imaging. Int. J. Pharm. 2011, 417, 204–215. [Google Scholar] [CrossRef]
- Cope, S.J.; Hibberd, S.; Whetstone, J.; MacRae, R.J.; Melia, C.D. Measurement and Mapping of PH in Hydrating Pharmaceutical Pellets Using Confocal Laser Scanning Microscopy. Pharm. Res. 2002, 19, 1554–1563. [Google Scholar] [CrossRef]
- Østergaard, J.; Jensen, H.; Larsen, S.W.; Larsen, C.; Lenke, J. Microenvironmental PH Measurement during Sodium Naproxenate Dissolution in Acidic Medium by UV/Vis Imaging. J. Pharm. Biomed. Anal. 2014, 100, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.S.; Jensen, H.; Cornett, C.; Møller, E.H.; Østergaard, J. Real-Time UV Imaging Identifies the Role of PH in Insulin Dissolution Behavior in Hydrogel-Based Subcutaneous Tissue Surrogate. Eur. J. Pharm. Sci. 2015, 69, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Liu, Y.; Li, W.; Gao, P.; Xiang, D.; Ren, X.; Liu, D. Mucoadhesive Buccal Film Containing Ornidazole and Dexamethasone for Oral Ulcers: In Vitro and in Vivo Studies. Pharm. Dev. Technol. 2019, 24, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Nafee, N.A.; Ismail, F.A.; Boraie, N.A.; Mortada, L.M. Mucoadhesive Delivery Systems. I. Evaluation of Mucoadhesive Polymers for Buccal Tablet Formulation. Drug Dev. Ind. Pharm. 2004, 30, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.M.; Prajapati, B.G.; Patel, H.V.; Patel, K.M. Mucoadhesive Bilayer Tablets of Propranolol Hydrochloride. AAPS PharmSciTech 2007, 8, E203–E208. [Google Scholar] [CrossRef] [PubMed]
- Mohamad, S.A.; Abdelkader, H.; Elrehany, M.; Mansour, H.F. Vitamin B12 Buccoadhesive Tablets: Auspicious Non-Invasive Substitute for Intra Muscular Injection: Formulation, in Vitro and in Vivo Appraisal. Drug Dev. Ind. Pharm. 2019, 45, 244–251. [Google Scholar] [CrossRef]
- Nafee, N.A.; Ismail, F.A.; Boraie, N.A.; Mortada, L.M. Mucoadhesive Buccal Patches of Miconazole Nitrate: In Vitro/in Vivo Performance and Effect of Ageing. Int. J. Pharm. 2003, 264, 1–14. [Google Scholar] [CrossRef]
- Chen, G.; Bunt, C.; Wen, J. Mucoadhesive Polymers-Based Film as a Carrier System for Sublingual Delivery of Glutathione. J. Pharm. Pharmacol. 2015, 67, 26–34. [Google Scholar] [CrossRef]
- Koirala, S.; Nepal, P.; Ghimire, G.; Basnet, R.; Rawat, I.; Dahal, A.; Pandey, J.; Parajuli-Baral, K. Formulation and Evaluation of Mucoadhesive Buccal Tablets of Aceclofenac. Heliyon 2021, 7, e06439. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Shirwaikar, A.; Nair, A. Preparation and Evaluation of Fast-Disintegrating Effervescent Tablets of Glibenclamide. Drug Dev. Ind. Pharm. 2009, 35, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Avdeef, A.; Berger, C.M. PH-Metric Solubility.: 3. Dissolution Titration Template Method for Solubility Determination. Eur. J. Pharm. Sci. 2001, 14, 281–291. [Google Scholar] [CrossRef]
- Zur, M.; Gasparini, M.; Wolk, O.; Amidon, G.L.; Dahan, A. The Low/High BCS Permeability Class Boundary: Physicochemical Comparison of Metoprolol and Labetalol. Mol. Pharm. 2014, 11, 1707–1714. [Google Scholar] [CrossRef] [PubMed]
- Advankar, A.; Maheshwari, R.; Tambe, V.; Todke, P.; Raval, N.; Kapoor, D.; Tekade, R.K. Chapter 13—Specialized Tablets: Ancient History to Modern Developments. In Drug Delivery Systems; Tekade, R.K., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 615–664. ISBN 978-0-12-814487-9. [Google Scholar]
- Freye, E. A New Transmucosal Drug Delivery System for Patients with Breakthrough Cancer Pain: The Fentanyl Effervescent Buccal Tablet. Available online: https://www.dovepress.com/a-new-transmucosal-drug-delivery-system-for-patients-with-breakthrough-peer-reviewed-article-JPR (accessed on 30 September 2020).
- Eichman, J.D.; Robinson, J.R. Mechanistic Studies on Effervescent-Induced Permeability Enhancement. Pharm. Res. 1998, 15, 925–930. [Google Scholar] [CrossRef]
- Pather, I.; Kolli, C.S. Chemical Methods for Enhancing Oral Mucosal Delivery. In Oral Mucosal Drug Delivery and Therapy; Rathbone, M.J., Senel, S., Pather, I., Eds.; Springer: Boston, MA, USA, 2015; pp. 31–52. ISBN 978-1-4899-7558-4. [Google Scholar]
- Jaipal, A.; Pandey, M.M.; Charde, S.Y.; Sadhu, N.; Srinivas, A.; Prasad, R.G. Controlled Release Effervescent Buccal Discs of Buspirone Hydrochloride: In Vitro and in Vivo Evaluation Studies. Drug Deliv. 2016, 23, 452–458. [Google Scholar] [CrossRef]
- Hans, R.; Thomas, S.; Garla, B.; Dagli, R.J.; Hans, M.K. Effect of Various Sugary Beverages on Salivary PH, Flow Rate, and Oral Clearance Rate amongst Adults. Scientifica 2016, 2016, 5027283. [Google Scholar] [CrossRef]
- West, N.X.; Hughes, J.A.; Addy, M. The Effect of PH on the Erosion of Dentine and Enamel by Dietary Acids in Vitro. J. Oral Rehabil. 2001, 28, 860–864. [Google Scholar] [CrossRef] [PubMed]
- Martelli, B.K.L.; de Melo, D.M.; Nai, G.A.; Parizi, J.L.S. Influence of Water PH in Oral Changes Caused by Cadmium Poisoning: An Experimental Study in Rats. Rev. Odontol. UNESP 2014, 43, 180–184. [Google Scholar] [CrossRef]
- Committee on Toxicity, Food Standard Agency Home Page. Available online: https://webarchive.nationalarchives.gov.uk/ukgwa/20200803134618/https://cot.food.gov.uk/cotstatements/cotstatementsyrs/cotstatements2004/acidsweets (accessed on 12 February 2023).
- Ahuja, A.; Khar, R.K.; Ali, J. Mucoadhesive Drug Delivery Systems. Drug Dev. Ind. Pharm. 1997, 23, 489–515. [Google Scholar] [CrossRef]
- Asane, G.S.; Nirmal, S.A.; Rasal, K.B.; Naik, A.A.; Mahadik, M.S.; Rao, Y.M. Polymers for Mucoadhesive Drug Delivery System: A Current Status. Drug Dev. Ind. Pharm. 2008, 34, 1246–1266. [Google Scholar] [CrossRef]
- Pham, Q.D.; Nöjd, S.; Edman, M.; Lindell, K.; Topgaard, D.; Wahlgren, M. Mucoadhesion: Mucin-Polymer Molecular Interactions. Int. J. Pharm. 2021, 610, 121245. [Google Scholar] [CrossRef]
- da Bassi Silva, J.; de Ferreira, S.B.S.; Reis, A.V.; Cook, M.T.; Bruschi, M.L. Assessing Mucoadhesion in Polymer Gels: The Effect of Method Type and Instrument Variables. Polymers 2018, 10, 254. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Cardoso, V.M.; Gremião, M.P.D.; Cury, B.S.F. Mucin-Polysaccharide Interactions: A Rheological Approach to Evaluate the Effect of PH on the Mucoadhesive Properties. Int. J. Biol. Macromol. 2020, 149, 234–245. [Google Scholar] [CrossRef] [PubMed]
- Surendranath, M.; Ramesan, R.M.; Parameswaran, R. Recent Advances in Functionally Modified Polymers for Mucoadhesive Drug Delivery. J. Mater. Chem. B 2022, 10, 5913–5924. [Google Scholar] [CrossRef] [PubMed]
- Waterman, K.C.; Adami, R.C.; Alsante, K.M.; Antipas, A.S.; Arenson, D.R.; Carrier, R.; Hong, J.; Landis, M.S.; Lombardo, F.; Shah, J.C.; et al. Hydrolysis in Pharmaceutical Formulations. Pharm. Dev. Technol. 2002, 7, 113–146. [Google Scholar] [CrossRef] [PubMed]
- Brandl, M.; Magill, A.; Rudraraju, V.; Gordon, M.S. Approaches for Improving the Stability of Ketorolac in Powder Blends. J. Pharm. Sci. 1995, 84, 1151–1153. [Google Scholar] [CrossRef]
- Tabatar, T.; Makino, T.; Kashihara, T.; Hirai, S.; Kitamori, N.; Toguchi, H. Stabilization of a New Antiulcer Drug (Lansoprazole) in the Solid Dosage Forms. Drug Dev. Ind. Pharm. 1992, 18, 1437–1447. [Google Scholar] [CrossRef]
- Chen, J.-G.; Chen, J.-G.; Markovitz, D.A.; Yang, A.Y.; Rabel, S.R.; Pang, J.; Dolinsky, O.; Wu, L.-S.; Alasandro, M. Degradation of a Fluoropyridinyl Drug in Capsule Formulation: Degradant Identification, Proposed Degradation Mechanism, and Formulation Optimization. Pharm. Dev. Technol. 2000, 5, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Oliyai, C.; Patel, J.P.; Carr, L.; Borchardt, R.T. Chemical Pathways of Peptide Degradation. VII. Solid State Chemical Instability of an Aspartyl Residue in a Model Hexapeptide. Pharm. Res. 1994, 11, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Strickley, R.G.; Anderson, B.D. Solid-State Stability of Human Insulin I. Mechanism and the Effect of Water on the Kinetics of Degradation in Lyophiles from PH 2–5 Solutions. Pharm. Res. 1996, 13, 1142–1153. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, C.; Inoue, R.; Kawabata, Y.; Yamashita, K.; Wada, K.; Yamauchi, Y.; Yamada, S.; Onoue, S. Novel Formulations of Dipyridamole with Microenvironmental PH-Modifiers for Improved Dissolution and Bioavailability under Hypochlorhydria. Int. J. Pharm. 2012, 434, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Adeleke, O.A.; Choonara, Y.E.; Du Toit, L.C.; Pillay, V. In Vivo and Ex Vivo Evaluation of a Multi-Particulate Composite Construct for Sustained Transbuccal Delivery of Carbamazepine. J. Pharm. Sci. 2014, 103, 1157–1169. [Google Scholar] [CrossRef] [PubMed]
- El-Mahrouk, G.M.; El-Gazayerly, O.N.; Aboelwafa, A.A.; Taha, M.S. Chitosan Lactate Wafer as a Platform for the Buccal Delivery of Tizanidine HCl: In Vitro and in Vivo Performance. Int. J. Pharm. 2014, 467, 100–112. [Google Scholar] [CrossRef] [PubMed]
- Kassem, M.A.A.; ElMeshad, A.N.; Fares, A.R. Enhanced Bioavailability of Buspirone Hydrochloride via Cup and Core Buccal Tablets: Formulation and in Vitro/in Vivo Evaluation. Int. J. Pharm. 2014, 463, 68–80. [Google Scholar] [CrossRef]
- Urbanova, M.; Gajdosova, M.; Steinhart, M.; Vetchy, D.; Brus, J. Molecular-Level Control of Ciclopirox Olamine Release from Poly(Ethylene Oxide)-Based Mucoadhesive Buccal Films: Exploration of Structure–Property Relationships with Solid-State NMR. Mol. Pharm. 2016, 13, 1551–1563. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Name | Active Ingredients | Molecular Weight (g/mol) | Dosage Form | Administration Route | Company | Approval Date |
|---|---|---|---|---|---|---|
| Metandren® | Methyltestosterone | 302.5 | Tablet | Buccal, Sublingual | Novartis, Basel, Switzerland | - |
| Sorbitrate® | Isosorbide dinitrate | 236.1 | Tablet | Sublingual | Astrazeneca, Cambridge, UK | - |
| Isuprel® | Isoproterenol hydrochloride | 247.7 | Tablet | Sublingual, Rectal | Sanofi-Aventis US, Bridgewater (NJ), U.S. | 1948 |
| Hydergine® | Ergoloid mesylates | - | Tablet | Sublingual | Novartis, Basel, Switzerland | 1953 |
| Isordil® | Isosorbide dinitrate | 236.1 | Tablet | Sublingual | Biovail, Ontario, Canada | 1961 |
| Dentipatch® | Lidocaine | 234.3 | Film | Buccal | Noven, Miami (FL), U.S. | 1996 |
| Nitrostat® | Nitroglycerin | 227.1 | Tablet | Sublingual | Upjohn, Hastings (MI), U.S. | 2000 |
| Suboxone® | Buprenorphine hydrochloride; Naloxone hydrochloride | 504.1, 363.8 | Tablet | Sublingual | Indivior, Richmond (VA), U.S. | 2002 |
| Subutex® | Buprenorphine hydrochloride | 504.1 | Tablet | Sublingual | Indivior, Richmond (VA), U.S. | 2002 |
| Striant® | Testosterone | 288.4 | Tablet | Buccal | Auxilium Pharms, Centerbrook (CT), U.S. | 2003 |
| Fentora® | Fentanyl citrate | 528.6 | Tablet | Buccal, Sublingual | Cephalon, Frazer (PA), U.S. | 2006 |
| Edluar® | Zolpidem tartrate | 764.9 | Tablet | Sublingual | Mylan Speciality Lp, Basking Ridge (NJ), U.S. | 2009 |
| Saphris® | Asenapine maleate | 401.8 | Tablet | Sublingual | Allergan, Dublin, Ireland | 2009 |
| Onsolis® | Fentanyl citrate | 528.6 | Film | Buccal | BioDelivery Sciences International, Raleigh (NC), U.S. | 2009 |
| Suboxone® | Buprenorphine hydrochloride; Naloxone hydrochloride | 504.1, 363.8 | Film | Buccal, Sublingual | Indivior, Richmond (VA), U.S. | 2010 |
| Intermezzo® | Zolpidem tartrate | 764.9 | Tablet | Sublingual | Purdue Pharma, Stamford (CT), U.S. | 2011 |
| Abstral® | Fentanyl citrate | 528.6 | Tablet | Sublingual | Sentynl Theraps, Solana Beach (CA), U.S. | 2011 |
| Zubsolv® | Buprenorphine hydrochloride; Naloxone hydrochloride | 504.1, 363.8 | Tablet | Sublingual | Orexo US Inc., Morristown (NJ), U.S. | 2013 |
| Bunavail® | Buprenorphine hydrochloride; Naloxone hydrochloride | 504.1, 363.8 | Film | Buccal | BioDelivery Sciences International, Raleigh (NC), U.S. | 2014 |
| Belbuca® | Buprenorphine hydrochloride | 504.1 | Film | Buccal | BioDelivery Sciences International, Raleigh (NC), U.S. | 2015 |
| Dsuvia® | Sufentanil citrate | 578.7 | Tablet | Sublingual | Acelrx Pharmaceuticals, Hayward (CA), U.S. | 2018 |
| Nocdurna® | Desmopressin acetate | 1129.3 | Tablet | Sublingual | Ferring Pharmaceuticals, Saint-Prex, Switzerland | 2018 |
| Cassipa® | Buprenorphine hydrochloride; Naloxone hydrochloride | 504.1, 363.8 | Film | Sublingual | Teva Pharmaceuticals, Tel Aviv, Isreal | 2018 |
| Kynmobi® | Apomorphine hydrochloride | 303.8 | Film | Sublingual | Sunovion Pharmaceuticals, Marlborough (MA), U.S. | 2020 |
| Igalmi® | Dexmedetomidine | 200.28 | Film | Sublingual | BioXcel Therapeutics, New Haven (CT), U.S. | 2022 |
| Drug | Molecular Weight (g/mol) | pKa * | Log P | Water Solubility (mg/mL) | Relevant Literature |
|---|---|---|---|---|---|
| Fentanyl | 336.47 | 8.99 | 4.05 | 0.74 | [54,55,56] |
| Naftopidil | 392.50 | 7.35 | 3.65 | 0.07 | [57] |
| Saquinavir | 670.84 | 8.47 | 3.80 | 0.00247 | [58,59,60,61] |
| Dapoxetine hydrochloride | 305.41 | 8.96 | 4.75 | 0.00084 | [62,63] |
| Nicotine | 162.23 | 8.58 | 1.17 | 93.3 | [64,65,66] |
| Metoprolol | 267.36 | 9.67 | 2.15 | 0.402 | [29] |
| Propranolol | 259.34 | 9.42 | 3.48 | 61.7 | [27] |
| pH Modifiers | Maximum Potency Per Unit Dose (mg/Unit) | |
|---|---|---|
| Oral Tablet/Capsule/Podwer | Buccal or Sublingual Tablet/Film | |
| Acetic Acid | 0.36 | - |
| Adipic Acid | - | - |
| Ammonia | 6.03 | - |
| Ammonium Carbonate | - | - |
| Ammonium Chloride | 10.67 | - |
| Diammonium Phosphate | 0.4 | 0.2 |
| Boric Acid | - | - |
| Calcium Carbonate | 550 | 145.7 |
| Calcium Hydroxide | 35 | - |
| Calcium Lactate | - | - |
| Calcium Phosphate, Tribasic | 333.3 | 99.2 |
| Citric Acid Monohydrate | 914 | 30 |
| Citric Acid, Anhydrous | 839 | 30 |
| Diethanolamine | - | - |
| Fumaric Acid | 150 | - |
| Glycine | 200 | - |
| Hydrochloric Acid | 1.72 | - |
| Alpha-Lactalbumin | - | - |
| Lactic Acid | 44 | - |
| Lysine Hydrochloride | - | - |
| Maleic Acid | 4 | - |
| Malic Acid | 315 | - |
| Methionine | NA | - |
| Monoethanolamine | 1 | - |
| Monosodium Glutamate | - | - |
| Nitric Acid | - | - |
| Phosphoric Acid | 1 | - |
| Potassium Bicarbonate | 500 | 8 |
| Potassium Citrate | NA | - |
| Potassium Hydroxide | 25.6 | - |
| Potassium Metaphosphate | NA | - |
| Potassium Phosphate, Dibasic | 30 | - |
| Potassium Phosphate, Monobasic | 25 | - |
| Propionic Acid | - | - |
| Racemethionine | - | - |
| Sodium Acetate | - | - |
| Sodium Bicarbonate | 1600 | 42 |
| Sodium Borate | - | - |
| Sodium Carbonate | 430 | 30 |
| Sodium Citrate | 1900 | 19.5 |
| Sodium Hydroxide | 60 | 1.18 |
| Sodium Lactate Solution | - | - |
| Sodium Phosphate, Dibasic | 600 | 4.07 |
| Succinic Acid | 125.3 | - |
| Sulfuric Acid | - | - |
| Tartaric Acid | 96 | 1.5 |
| Trolamine | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, S.; Mu, H. Microenvironmental pH Modification in Buccal/Sublingual Dosage Forms for Systemic Drug Delivery. Pharmaceutics 2023, 15, 637. https://doi.org/10.3390/pharmaceutics15020637
He S, Mu H. Microenvironmental pH Modification in Buccal/Sublingual Dosage Forms for Systemic Drug Delivery. Pharmaceutics. 2023; 15(2):637. https://doi.org/10.3390/pharmaceutics15020637
Chicago/Turabian StyleHe, Shaolong, and Huiling Mu. 2023. "Microenvironmental pH Modification in Buccal/Sublingual Dosage Forms for Systemic Drug Delivery" Pharmaceutics 15, no. 2: 637. https://doi.org/10.3390/pharmaceutics15020637