
Is a Lower Dose of Rivaroxaban Required for Asians? A Systematic Review of a Population Pharmacokinetics and Pharmacodynamics Analysis of Rivaroxaban

Abstract
:1. Introduction
2. Methods
2.1. Study Identification
2.2. Reporting Quality
2.3. Data Extraction
2.4. Comparison of Studies
3. Results
3.1. Study Identification
3.2. Reporting Quality
3.3. Study Characteristics
3.3.1. Basic Characteristics
3.3.2. Population Pharmacokinetic Models
3.3.3. Population Pharmacokinetic-Pharmacodynamic Models

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Study Type | Country/Race | Study Population | No. of Subjects (M/F) | No. of Samples (Per Person) | Age (Years) a | Body weight (kg) a | Lean body mass (kg) a | CrCl (or eGFR, mL/min) a | Dose Regimens |
|---|---|---|---|---|---|---|---|---|---|---|
| Mueck et al. (2007) [19] | Phase I | Caucasian | Healthy subjects | 43 (43/0) | PK: 1809 (42.1) PD markers in total: 6533 (151.9) b | 32.5 [20–45] | NA | NA | NA | 5 mg qd, 5–30 mg bid, 5 mg tid |
| Mueck et al. (2008a) [21] | Phase II | Europeans, Israeli | HRS | PK: 758 (302/456) PT: 1118 (NA) | PK: 5743 (7.6) PT: 10467 (8.9) | 66 [26–93] c | 75 [45–120] c | NA | 88.1 [18.8–208] | 2.5–30 mg bid, 5–40 mg qd |
| Mueck et al. (2008b) [22] | Phase II | Canadians, American, Europeans | HRS, KRS | 1013 (NA) | PK: 7660 (7.6) PD markers in total: >9100 (>9.0) d | HRS: 65 [26–87] KRS: 67 [39–92] | HRS: 76 [45–125] KRS: 86 [50–173] | HRS:51 [34–81] KRS: 51 [28–83] | HRS: 96 [33–218] KRS: 104 [35–259] | 2.5–30 mg bid |
| Mueck et al. (2011) [23] | Phase II | Most Caucasian | DVT | 870 (487/383) | PK: 4634 (5.3) | 61 [18–94] | NA | Male: 63 ± 8 Female: 47 ± 5 | 87.4 ± 1.5 | 10–30 mg bid, 20–40 mg qd |
| Xu et al. (2012) [24] | Phase III | White (95.8), Black (0.8%), Asian (1.7%), Others (1.7%) | ACS | 2290 (1784/506) | PK: NA PT: 6644 (4.9) e | 57 [24–87] | 84 [36–181] | 60.7 [30.4–90.4] | 96.9 [22.4–298] | 2.5–10 mg bid, 5–20 mg qd |
| Tanigawa et al. (2013) [26] | Phase II | Japanese | NVAF | 182 (148/34) | PK: 842 (4.6) FXa activity: 985 (5.4) PT: 987 (5.4) aPTT: 986 (5.4) Heptest: 987 (5.4) | 65.6 ± 10.0 [30–92] | 67.2 ± 10.4 [45–103] | 51.4 ± 7.2 [34.7–67.9] | Baseline: 79.7 ± 25.2 [29.0–175.8] Day 28: 80.7 ± 26.6 [29.0–198.8] | 10–20 mg qd, 2.5–20 mg bid |
| Kaneko et al. (2013) [25] | Phase III | Japanese | NVAF | 597 (NA) | PK: 1834 (3.1) PT: 1869 (3.1) | 70.98 ± 8.31 72 [34–89] | 64.45 ± 10.65 63.9 [35–104] | 49.69 ± 7.14 50.24 [30.18–70.48] | 67.41 ± 22.89 64 [26–172] | 15 mg qd (10 mg qd in patients with CrCl < 50 mL/min) |
| Girgis et al. (2014) [27] | Phase III | Most Caucasian | NVAF | 161 (NA) | PK: 801 (5.0) FXa activity: 799 (5.0) PT: 796 (5.0) PiCT: 742 (4.6) | 65 ± 9.5 | NA | 57.5 ± 9.9 | NA | 20 mg qd (15 mg qd for patients with CrCl 30–49 mL/min) |
| Zhang et al. (2017) [29] | Phase II, III | Most Caucasian | DVT, NVAF | 285 (NA) | NA | NVAF: 65 [51–81] f DVT: 59 [31–83] f | NA | NVAF: 56.6 [42.5–73.6] f DVT: 54.1 [40.1–72.7] f | NA | 20 mg qd (15 mg for NVAF patients with CrCl 30–49 mL/min) |
| Barsam et al. (2017) [28] | Post- marketing study | Caucasian (74%), Afro-Caribbean (21%), Other (5%) | Acute VTE treatment, VTE prevention | 101 (59/42) | PK: 193 (1.9) g | 52 [20–86] h | 88 ± 23.4 | 57.0 ± 11.3 | 67%: > 80 mL/min 25%: 50–79 mL/min 7.8%: 30–49 mL/min 0.2%: < 30 mL/min | 10–20 mg qd, 15 mg bid |
| Suzuki et al. (2018) [30] | Post- marketing study | Japanese | NVAF | 96 (81/15) | PK: 192 (2) PT: 192 (2) | 68.0 ± 9.5 | 69.1 ± 11.4 | NA | Baseline: 76.2 ± 21.3 2–4 h after drug intake: 77.6 ± 21.8 | 15 mg qd (10 mg in patients with CrCl < 50 mL/min) |
| Willmann et al. (2018a) [31] | Phase II, III | Multinational | HRS, KRS, DVT, ACS, NVAF | 4918 (2985/1933) | PK: 22843 (4.6) | 60.53 ± 11.82 | 82.48 ± 16.87 | 57.05 ± 10.00 | 97.74 ± 33.97 i | 2.5–30 mg bid, 2.5–40 mg qd |
| Willmann et al. (2018b) [39] | Phase I | White (74.6%), Black (1.7%), Asian (3.4%), Hispanic (11.9%), Missing (6.8%) | Children with VTE | 59 (33/26) | PK: 206 (3.5) | 6.8 ± 4.9 6.0 [0.5–17] | 29.5 ± 18.3 27.7 [6.2–77.8] | NA | NA | 10, 20 mg |
| Zdovc et al. (2019) [32] | Post- marketing study | Slovenia | HRS, KRS | 17 (8/9) | PK: 82 (4.8) g PT: NA aPTT: NA | 64 [49–82] | 84 [54–125] | 53 [38–81] | 82 [57–150] j | 10 mg qd |
| Goto et al. (2020) [18] | Post- marketing study | Japanese | NVAF | 119 (85/34) | PK: 162 (1.3) g | 10 mg: 73.1 ± 10.0 15 mg: 66.7 ± 10.0 | 10 mg: 60.3 ± 15.5 15 mg: 67.3 ± 13.8 | NA | 10 mg: 64.0 ± 21.2 15 mg: 84.4 ± 27.7 | 10, 15 mg qd |
| Speed et al. (2020) [33] | Post- marketing study | The United Kingdom | VTE, NVAF, other | 913 (522/391) | PK: 1108 (1.2) g | 67.03 ± 15.00 [19–96] | 85.75 ± 23.07 [39–172] | 55.8 ± 13.1 | 91.47 ± 43.81 [16–259] | 10–30 mg qd, 10–15 mg bid |
| Willmann et al. (2021) [40] | Phase III | Most Caucasian | Children with VTE, post- Fontan surgery | 524 (NA) | PK: 1988 (3.8) | Not defined (16% <2 years) | <6 months: 4.1 ± 1.3 [2.7–7.9] 6 months–2 years: 9.5 ± 2.3 [5.4–15.1] 2–6 years: 16.4 ± 4.2 [10.1–39.1] 6–12 years: 32.4 ± 10.8 [17–71] 12–18 years: 67.9 ± 21.1 [20–194] | NA | <6 months: 111 ± 45.6 [50.6–220] 6 month–2 years: 156 ± 52.4 [74.4–456] 2–6 years: 168 ± 49.4 [43.8–287] 6–12 years: 178 ± 43.5 [76.7–330] 12–18 years: 144 ± 38.3 [73.8–354] | 0.4–20 mg qd |
| Esmaeili et al. (2022) [38] | Post- marketing study | Iranian | NVAF, DVT, PE | 69 (33/36) | PK: 126 (1.8) | 64 [36–86] | 70 [46–112] | 49.6 [34.8–72.0] | 63.8 [23.5–128.5] | 20 mg bid, 10–20 mg qd |
| Liu et al. (2022) [34] | Post- marketing study | Chinese | NVAF | 195 (111/84) | PK: 256 (1.3) PT: 244 (1.3) | 66.7 ± 11.7 68 [28–96] | 68.9 ± 12.9 68 [36.5–119] | 51.5 ± 8.9 51.8 [29.0–73.3] | 77.8 ± 21.2 79.7 [21.9–127.7] | 5–20 mg qd |
| Singkham et al. (2022) [35] | Post- marketing study | Thai | NVAF | 60 (38/22) | PK: 240 (4) g | 69.4 ± 9.2 | 64.0 ± 14.1 | NA | 59.0 ± 22.8 | 10–20 mg qd |
| Willmann et al. (2022) [41] | Phase III | Multinational | Children with congenital heart disease and undergone the Fontan procedure | NA | NA | NA | NA | NA | NA | NA |
| Zhang et al. (2022) [37] | Post- marketing study | Chinese | NVAF | 150 (95/55) | PK: 263 (1.8) | 68.0 ± 12.6 69 [23–90] | 67.4 ± 20.8 66.1 [38.0–110.0] | NA | 72.1 ± 33.5 71.1 [13.3–146.7] | 10,15, 20 mg, others |
| Zhao et al. (2022) [20] | Post- marketing study | Chinese | Healthy subjects, NVAF | Healthy subjects: 304 (202/102) NVAF: 223 (118/105) | PK: 4726 (15.5) k PT: 1624 (3.1) Anti-Xa: 1253 (2.4) | Healthy subjects: 30 [18–62] NVAF: 70 [34–91] | Healthy subjects: 62.8 [47.0–83.0] NVAF: 68.2 [38–112] | NA | Healthy subjects: 103 [71.5–568] NVAF: 76.3 [26.1–178] | Healthy subjects: 10–20 mg (single dose) NVAF: 5–30 mg qd |
| Zhang et al. (2023) [36] | Post- marketing study | Chinese | NVAF | 180 (96/84) | PK: 360 (2) | 81.8 ± 4.3 81 (75–95) | 67.3 ± 12.4 70 (40–100) | NA | 71.7 ± 22.1 73.3 (20.4–113.7) | 5–20 mg qd |
| Study (Year) | Estimation Method | Fixed Effect Parameters | Between-Subject Variability | Residual Unexplained Variability | Model Evaluation | Model Application | |
|---|---|---|---|---|---|---|---|
| Mueck et al. (2007) [19] | FOCE | ka (/h) | 0.97 | 52.9% (BSV) 93.8% (IOV) | 25.4% | GOF, OFV | Determination of sampling window in phase II |
| ALAG (h) | 0.25 | 102.5% (IOV) | |||||
| CL/F (L/h) | 9.17 | 17.4% | |||||
| Vc/F (L) | 55.3 (dose < 30 mg) 79.2 (dose = 30 mg) | 30.7% | |||||
| Vp/F (L) | 12.6 (dose < 30 mg) 23.5 (dose = 30 mg) | 38.6% | |||||
| Q/F (L/h) | 1.35 | / | |||||
| Mueck et al. (2008a) [21] | FOCE-I | ka (/h) | 0.047 (day 2 for mixed population 1) 0.222 (day 3–4 for mixed population 1) 1.07 (≤ 4 days for mixed population 2) 1.49 (> 4 days for all patients) | / | 52.6% | GOF, OFV | NA |
| CL (L/h) | 5.46 (day 2) 6.91 (day 3–4) 7.51 × [1 − 0.01 × (age − 66) + 0.003 × (CrCl − 88.1) + 0.22 × (ALB − 3.4) − 0.012 × (HCT − 37.3)] (day > 4) | 38.2% | |||||
| V (L) | 58.2 × [1 + 0.64 × (BSA − 1.84)] | 32.4% | |||||
| F | 0.877 (5, 10 mg, compared to 2.5 mg) 0.791 (20 mg, compared to 2.5 mg) | / | |||||
| Mueck et al. (2008b) [22] | FOCE-I | ka (/h) | 0.092 (≤ 3 days for population 1, HRS) 1.81 (≤ 3 days for population 2 and > 3 days for the total population, HRS) 1.20 (> 3 days, KRS) | / | 37.1% (HRS) 34% (KRS) | GOF, OFV | NA |
| CL (L/h) | 6.4 (≤ 3 days, HRS) 7.3 × [1 − 0.015 × (age − 65) − 0.21 × (SCr − 0.78)] (> 3 days, HRS) 6.13 × [1 + 0.002 × (CrCl − 103)] × 0.85 (if female) (> 3 days, KRS) a | 70.1% (HRS, ≤ 3 days) 38.6% (HRS, > 3 days) b | |||||
| V (L) | 49.1 × [1 + 0.018 × (LBM − 51)] (HRS) 55.7 × [1 + 0.67 × (BSA − 1.95)] (KRS) | / | |||||
| F | 1 (2.5 mg bid) 0.847 (HRS, 5, 10 mg bid) 0.74 (KRS, 5, 10 mg bid) 0.609 (HRS, 20, 30 mg bid) 0.53 (KRS, 20, 30 mg bid) | / | |||||
| Mueck et al. (2011) [23] | FOCE-I | ka (/h) | 1.23 | / | 40.7% | GOF, bootstrap, VPC | The effect of identified factor on PK, and factors influencing PK in NVAF patients |
| CL (L/h) | 5.67 × [1 − 0.007 × (age − 61) − 0.269 × (SCr − 0.94)] | 39.9% | |||||
| V (L) | 54.4 × [1 + 0.008 × (LBM − 56) − 0.005 × (age − 61)] | 28.8% | |||||
| F | 0.79 (20 mg compared to 10 mg) 0.63 (30, 40 mg compared to 10 mg) | / | |||||
| Xu et al. (2012) [24] | FOCE | ka (/h) | 1.24 | 139% | 35.2 % | GOF, VPC | The effect of identified factors on PK |
| CL (L/h) | 6.48 × [1 − 0.0112 × (age − 57) − 0.151 × (SCr − 0.95)] | 31.3% (BSV) 32.4% (IOV) | |||||
| V (L) | 57.9 × [1 + 0.00833 × (LBM − 60.7) − 0.00707 × (age-57)] | 10.0% | |||||
| F | 1 (2.5 mg) 0.851 (< 10 mg) 0.705 (≥ 10 mg) | / | |||||
| Tanigawa et al. (2013) [26] | FOCE-I | ka (/h) | 0.6 | 68% | 40.2% | GOF, VPC, bootstrap | Comparison of PK parameters in Japanese and Caucasian patients |
| CL (L/h) | 4.72 × [1 − 0.0165 × (BUN − 16.73)] | 21.3% | |||||
| V (L) | 42.9 | / | |||||
| F | 1 | 24.4% | |||||
| Kaneko et al. (2013) [25] | FOCE-I | ka (/h) | 0.617 | 58.2% | 13.1% | GOF, VPC, bootstrap | Comparison of the posthoc estimated PK parameters between Japanese and non-Japanese patients |
| CL (L/h) c | 4.73 × (CrCl/67.11)0.159 × [1 − 0.0132 × (HCT − 42.14)] | 41.0% | |||||
| V (L) | 43.8 | 63.6% | |||||
| F | 1 | 37.7% (IOV) | |||||
| Girgis et al. (2014) [27] | FOCE-I | ka (/h) | 1.16 | / | 47.9% | PE%, GOF, pc-VPC | Dose modification for patients with renal impairment |
| CL/F (L/h) | 6.1 × [1 − 0.011 × (age − 65) − 0.194 × (SCr − 1.09)] | 35.2% | |||||
| V/F (L) | 79.7 × [1 − 0.00133 × (age − 65) + 0.0118 × (LBM − 57.5)] | 17.6% | |||||
| Zhang et al. (2017) [29] | FOCE-I | ka (/h) | 0.982 | / | 47.5% | GOF, VPC | Cross-study PK comparison |
| CL/F (L/h) | 6.31 × [1 − 0.011 × (age − 65) − 0.244 × (SCr − 1.05)]/1.12 (if DVT) | 34.6% | |||||
| V/F (L) | 70.3 × [1 − 0.00347 × (age − 65) − 0.109 × (LBM − 56.62)]/1.12 (if DVT) | 15.5% | |||||
| Barsam et al. (2017) [28] | FOCE | ka (/h) | 1.21 | / | 31% 0.016 ng/mL | VPC | NA |
| CL/F (L/h) | 8.86 × (CrCl/79)0.434 | 48% | |||||
| V/F (L) | 101 | 60% | |||||
| Suzuki et al. (2018) [30] | FOCE | ka (/h) | 1.37 | 44.6% | 41.8% | GOF | NA |
| CL/F (L/h) | 4.40 × (CrCl/75)0.324 × (ALT/22)−0.225 × (1 − 0.319 × INH) | 20.6% | |||||
| V/F (L) | 38.2 | 63.6% | |||||
| Willmann et al. (2018a) [31] | FOCE-I | ka (/h) | 0.821 | 79.25% | 45.06% | GOF, pc-VPC | The effect of identified factors on PK |
| CL (L/h) | 6.58 × (CrCl/93)0.406 × (BW/81) −0.278 × 0.966 (if co-medication with P-pg inhibitor) × 0.978 (if co-medication with strong CYP3A4 inhibitors) × 0.863 (if co-medication with moderate CYP3A4 inhibitors) × 0.939 (if co-medication with weak CYP3A4 inhibitors) × 1.30 (if co-medication with CYP3A4 inducers) × 1 (if venous thromboembolism treatment) × 0.849 (if non-valvular atrial fibrillation) × 1.14 (if acute coronary syndromes) × 1.04 (if venous thromboembolism prevention, < 72 h) × 1.29 (if venous thromboembolism prevention, ≥ 72 h) | 40.87% | |||||
| V (L) | 62.5 × (BW/81) 0.216 × (age/61) −0.189 × 0.889 (if female) | 19.77% | |||||
| F | 0.59 + 0.66 × e− 0.048 × dose | / | |||||
| Willmann et al. (2018b) [39] | FOCE-I | ka (/h) | 0.717 (for tablet or diluted suspension) 0.208 (for undiluted suspension) | 39.7% | 46.6% | Compare PK parameters with that derived from non-compartmental analysis | Comparison of PK parameters with PBPK model predictions |
| CL (L/h) | 7.26 × (BW/70)0.323 | 26.2% | |||||
| Vc (L) | 50.9 × (BW/70) | / | |||||
| Vp (L) | 13.5 | / | |||||
| Q (L/h) | 0.928 | / | |||||
| F | 0.648 | / | |||||
| Zdovc et al. (2019) [32] | Laplacian method with interaction | ka (/h) | 0.147 | 794% | 59.5% | GOF, VPC, bootstrap | The effect of identified factors on PK |
| CL/F (L/h) | 6.12 × (ABCB1 expression/1.25)0.817 | 80.8% | |||||
| V/F (L) | 96.8 | / | |||||
| Goto et al. (2020) [18] | NA | ka (/h) | 0.617 d | 58.2% d | 13.1 % d | GOF, VPC | NA |
| CL (L/h) | 5.59 × (CrCl/67.11)0.159 | 41.0% d | |||||
| V (L) | 50.9 | 63.6% d | |||||
| F | 1 | 37.7% d | |||||
| Speed et al. (2020) [33] | FOCE-1 | ka (/h) | 0.707 | / | 46.37% | VPC, bootstrap | The effect of identified factors on PK |
| CL/F (L/h) | 5.57 × (CrCl_LBM/55)0.446 | 23.02% e | |||||
| V/F | 59.4 × (LBM/55)0.519 | / | |||||
| Willmann et al. (2021) [40] | NA | ka (/h) | 0.799 (for tablet and diluted suspension) 0.226 (for undiluted suspension) | / | NA | Comparison of PK parameters with PBPK model predictions | |
| CL (L/h) | 8.02 × (BW/82.48)0.481 | 27.0% | 46.9% | ||||
| Vc (L) | 53.2 × (BW/82.48)0.821 | / | |||||
| Vp (L) | 13.5 × (BW/82.48)0.821 | / | |||||
| Q (L/h) | 2.5 × (BW/82.48)0.761 | / | |||||
| F | 0.59 + 0.66 × e− dose/BW × 3.97 | 25.1% | |||||
| Esmaeili et al. (2022) [38] | SAEM | ka (/h) | 0.821 f | / | 38% | GOF, bootstrap | NA |
| CL/F (L/h) | 3.7 × (CrCl/62.3)0.89 × (CTP/5.7)−1.76 | 61% | |||||
| V/F (L) | 59 | 21% | |||||
| Liu et al. (2022) [34] | FOCE-I | ka (/h) | 0.617 d | / | 33.6% | GOF, VPC, bootstrap | The effect of identified factors on PK and PD, and dose modification |
| CL/F (L/h) | 5.03 × (eGFR/80)0.53 | 35.4% | |||||
| V/F (L) | 40.3 | / | |||||
| Singkham et al. (2022) [35] | FOCE-I | ka (/h) | 0.697 | 75.91% | 0.092 mg/L | GOF, VPC, bootstrap | The effect of identified factors on PK, and dose modification |
| CL/F (L/h) | 4.19 × (CrCl/57.5)0.277 | 21.94% | |||||
| V/F (L) | 37.5 × (BW/63)0.412 | / | |||||
| Willmann et al. (2022) [41] | NA | ka (/h) | 0.799 | / | 51.9% | GOF | Comparison of PK parameters with PBPK model predictions, and simulation for dose-exposure relationship |
| CL (L/h) | 6.07 × (BW/82.48)0.481 | 31.8% | |||||
| Vc (L) | 53.2 × (BW/82.48)0.821 | / | |||||
| Vp (L) | 59.1 × (BW/82.48)0.821 | / | |||||
| Q (L/h) | 2.5 × (BW/82.48)0.761 | / | |||||
| F | 0.752 (≥5 years) 1.2 (<5 years) | 40.1% | |||||
| Zhang et al. (2022) [37] | FOCE-I | ka (/h) | 0.821 f | / | 36.6% 2.51 μg/L | GOF, VPC, bootstrap | The effect of identified factors on PK, and dose modification |
| CL/F (L/h) | 5.79 × e(CRCl − 76.1) × 0.00586 × e-(TBIL − 14) × 0.0144 × 1.476 (if ABCB1 rs4728709 AA/GA) | 38.3% | |||||
| V/F (L) | 51.5 × e(BW−66) × 0.00873 | 18.5% | |||||
| Zhao et al. (2022) [20] | FOCE-I | ka (/h) | 0.406 × 0.830 (if postprandial status) g | / | 21.0% 1.95 μg/L | GOF, bootstrap | The effect of identified factors on PD |
| D (h) | 0.101 × 4.9 (if postprandial status) g | 183% g | |||||
| ALAG (h) | 0.164 g | / | |||||
| CL/F (L/h) | 7.39 × (CrCl/95)0.61003 | 47.1% | |||||
| Vc/F (L) | 10.9 × (BMI/22.85)1.364 g | 53.8% g | |||||
| Vp/F (L) | 50.9 g | 68.1% g | |||||
| Q/F (L/h) | 4.4 g | 77.9% g | |||||
| F | 0.867 (15 mg, compared to 10 mg) g 0.608 (20 mg, compared to 10 mg) g × 1.244 (if postprandial status) g | 15.5% g | |||||
| Zhang et al. (2023) [36] | FOCE-I | ka (/h) | 0.821 f | / | 20 % 0.193 μg/L | GOF, VPC, bootstrap | The effect of identified factors on PK, and dose modification |
| CL/F (L/h) | 3.68 × (eGFR/73.275)0.528 × (TBIL/13.63)−0.246 × 1.257 (if ABCB1 rs1045642 CT/TT) | / | |||||
| V/F (L) | 42.9 | / | |||||
3.3.4. Model Evaluation
3.3.5. Model Application
3.4. Comparison of Studies
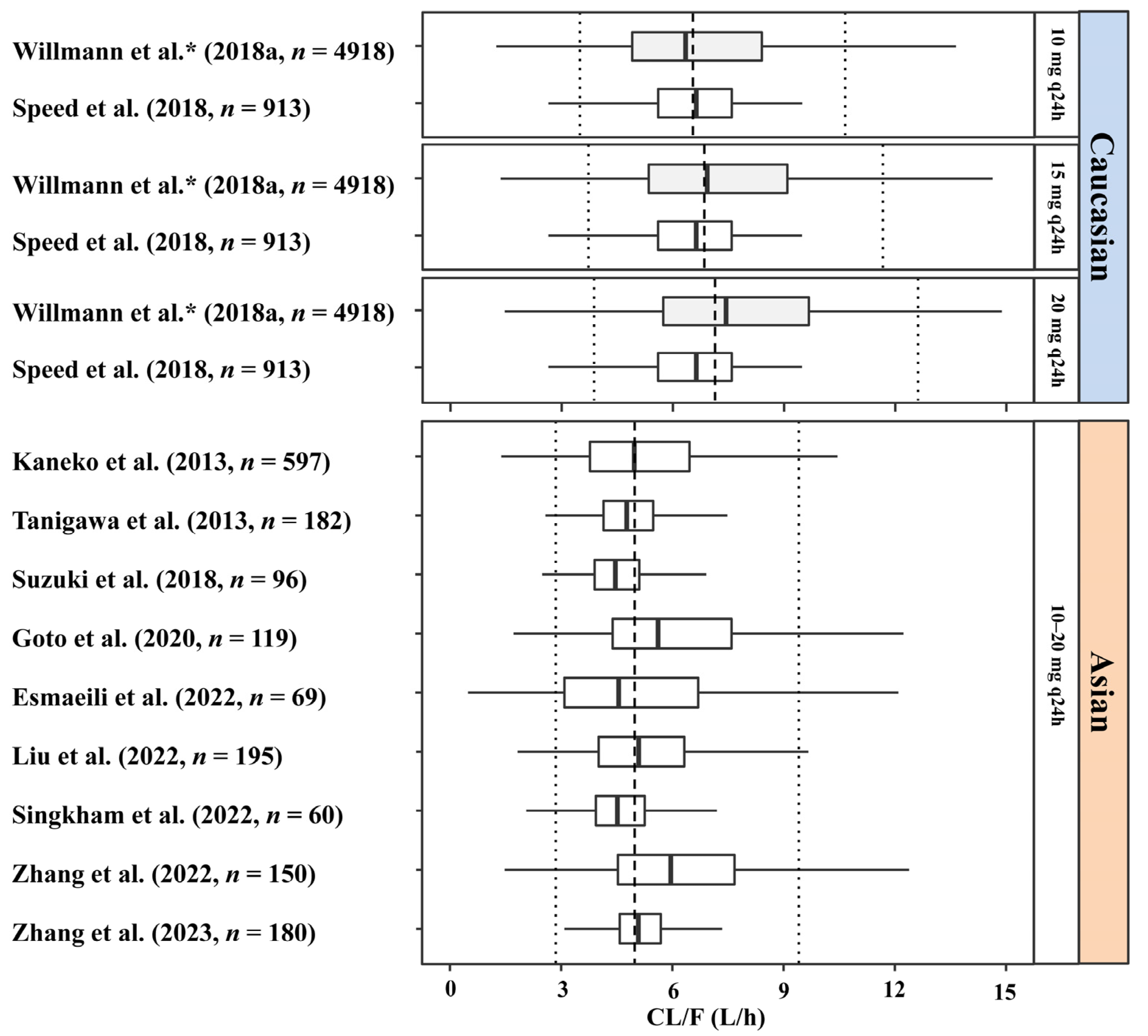
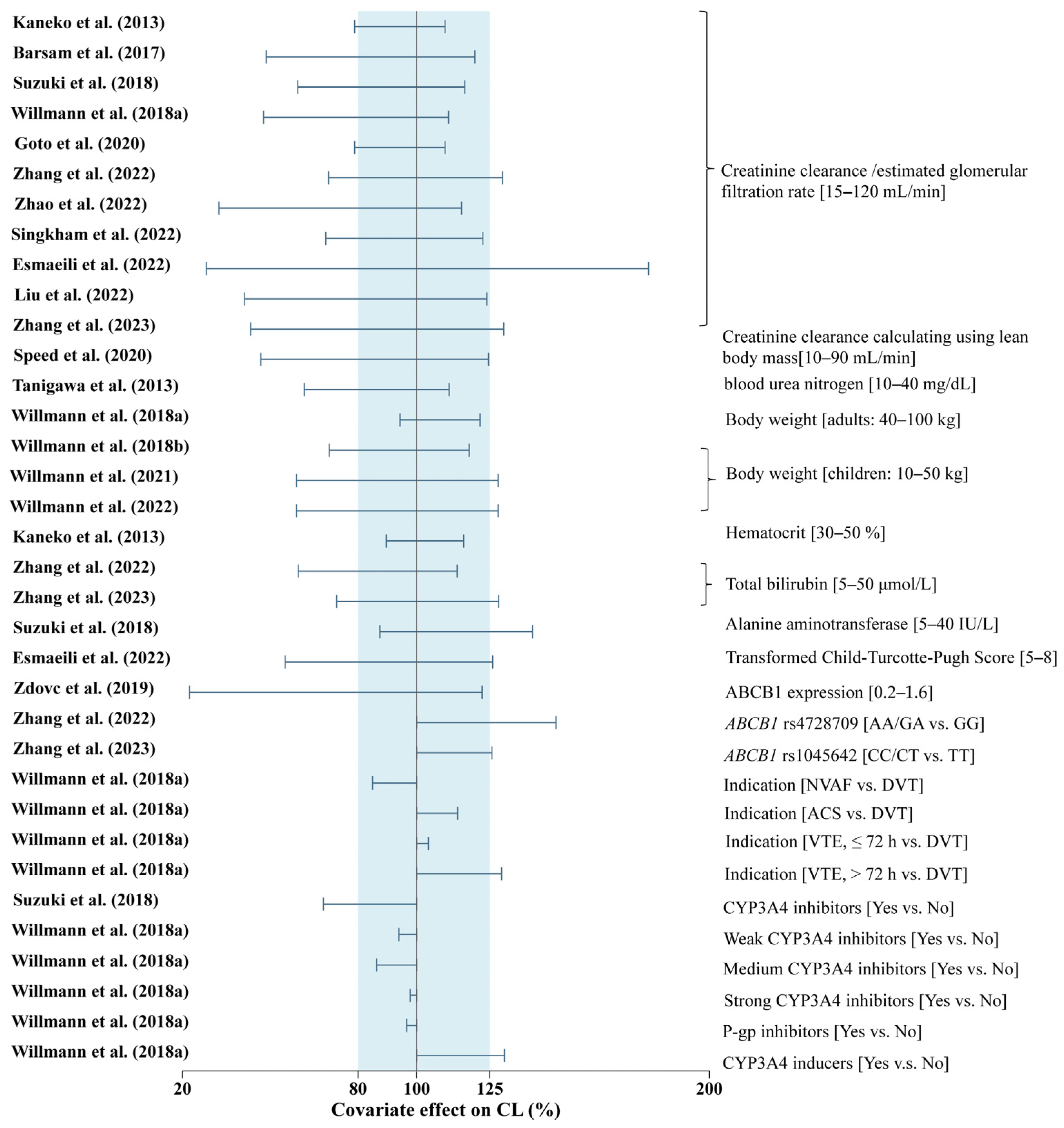
3.4.1. Pharmacokinetic Analysis
| Study (Year) | Analytical Method/ Regent | Formula | Fixed Effect Parameters | Between-Subject Variability | Residual Unexplained Variability | |
|---|---|---|---|---|---|---|
| Prothrombin time | ||||||
| Mueck et al. (2007) [19] | Neoplastin Plus® | PT = PT0 + slope × Cp | PT0 (s) | 12.7 | 3.7% | 1.58 s |
| slope (s/(μg/L)) | 0.0458 | 12.3% | ||||
| Mueck et al. (2008b) [22] a | STA® Neoplastine® | PT = PT0 + slope × Cp | PT0 (s) | 13.1 × [1 + 0.034 × (ALB − 3.3)] × [1–0.0045 × (CrCl − 96)] (HRS) 13.4 × [1 + 0.05 × (ALB − 3.6)] × [1–0.008 × (CrCl − 104)] (KRS) | 5.8% (HRS) 7.4% (KRS) | 8.6% (HRS) 10.9% (KRS) |
| slope (s/(μg/L)) | 0.032 (HRS) 0.042 (KRS) | 43.2% | ||||
| Mueck et al. (2011) [23] | STA® Neoplastine® | PT = PT0 + slope × Cp1-Hill × Cp | PT0 (s) | 12.5 × [1–0.0004 × (CrCl − 87.4)] | 9.7% | 10.3% |
| slope (s/(μg/L)) | 0.036 | / | ||||
| Hill | 0.0000996 × [1 + 0.0046 × (CrCl − 87.4)] | 4.3% | ||||
| Xu et al. (2012) [24] | STA Neoplastin CI Plus® | PT = PT0 + slope × Cp1-Hill × Cp | PT0 (s) | 13.9 × [1–0.0003 × (CrCl − 96.9)] | 9.32% | 7.6% |
| slope (s/(μg/L)) | 0.032 | / | ||||
| Hill | 0.0000593 × [1 + 0.0233 × (CrCl − 96.9)] | 6.61% | ||||
| Kaneko et al. (2013) [25] | Neoplastin Plus® | PT = PT0 + slope × Cp1-Hill × Cp | PT0 (s) | 11.4 × [1 + 0.0035 × (age − 70.98) + 0.00242 × (LBM − 49.69) − 0.065 × (ALB − 4.22) − 0.015 × (HGB − 14.06)] | 9.6% | 7.1% |
| slope (s/(μg/L)) | 0.0467 | / | ||||
| Hill | 0.000155 × (TBIL/14.02)−1.11 | 7.3% | ||||
| Tanigawa et al. (2013) [26] | Neoplastin Plus® | PT = PT0 + slope × CpHill | PT0 (s) | 13.7 | 8.0% | 9.4% |
| slope (s/(μg/L)) | 0.0227 | 27.0% | ||||
| Hill | 1.1 | / | ||||
| Girgis et al. (2014) [27] | STA Neoplastin CI Plus® | PT = PT0 + slope × Cp1-Hill × Cp | PT0 (s) | 11.4 × [1–0.000192 × (CrCl − 76)] | 22.6% | 12.9% |
| slope (s/(μg/L)) | 0.0426 | 4.42% | ||||
| Hill | 0.0000551 × [1 + 0.0174 × (CrCl − 76)] | / | ||||
| Suzuki et al. (2018) [30] | Neoplastin Plus® | PT = PT0 + slope × Cp | PT0 (s) | 14 | / | 0.87 s |
| slope (s/(μg/L)) | 0.0335 × (HCT/42)−1.10 | 11.7% | ||||
| Thromborel® S | PT = PT0 + slope × Cp | PT0 (s) | 12.5 | / | 0.71 s | |
| slope (s/(μg/L)) | 0.0158 × (HCT/42)−1.38 × (ALB/4.2)−2.31 | 8.7% | ||||
| ThromboCheck PT® | PT = PT0 + slope × Cp | PT0 (s) | 11.8 | / | 0.61 s | |
| slope (s/(μg/L)) | 0.0220 × (HCT/42)−1.30 | 9.5% | ||||
| RecombiPlasTin 2G® | PT = PT0 + slope × Cp | PT0 (s) | 12.1 | / | 0.75 s | |
| slope (s/(μg/L)) | 0.0323 | 11.2% | ||||
| Suzuki et al. (2018) [30] | Thrombocheck PT Plus® | PT = PT0 + slope × Cp | PT0 (s) | 13.2 | / | 0.82 s |
| slope (s/(μg/L)) | 0.0266 × (HCT/42)−1.07 × (age/69)0.680 | 10.6% | ||||
| Zdovc et al. (2019) [32] | Thromborel® S | PT = PT0 + slope × log(Cp) | PT0 (s) | 12.8 | 11.4% | 1.85 s |
| slope (s/(μg/L)) | 0.215 | 109% | ||||
| Liu et al. (2022) [34] | Thromborel® S | PT = PT0 + slope × Cp | PT0 (s) | 13.9 × e0.00574 × (TBIL − 12) × (1 − 0.0872 × eGFR/80) | 5.6 % | 9.4% |
| slope (s/(μg/L)) | 0.0133 | 61.8 % | ||||
| Esmaeili et al. (2022) [38] | FisherbrandTM | PT = PT0 + slope × Cp | PT0 (s) | 12.6 | 2% | 12% |
| slope (s/(μg/L)) | 0.018 | 54% | ||||
| Zhao et al. (2022) [20] | Thromborel® S | PT = PT0 + slope × CpHill | PT0 (s) | 11.4 × (BW/68.2)−0.159 × (TCHO/3.96)−0.0794 b | 6.9% b | 0.372 s |
| slope (s/(μg/L)) | 0.0018 b | 24.9% b | ||||
| Hill | 1.37 b | / | ||||
| Factor Xa activity | ||||||
| Mueck et al. (2007) [19] | Two-step photometric assay | FXa = FXa0 × (1 − ) | FXa0 (U/mL) | 0.87 | 10.09% | 0.0027 U/mL |
| Emax (U/mL) | 0.86 | 9.9% | ||||
| EC50 (μg/L) | 220 | / | ||||
| Mueck et al. (2008b) [22] | Two-step photometric assays | FXa = FXa0 × (1 − ) | FXa0 (U/mL) | 1 | 13.9% (HRS) 14.5% (KRS) | 8.4% (HRS) 9.7% (KRS) |
| Emax (U/mL) | 0.881 (day 1, HRS) 0.942 (steady state, HRS) 0.837 (KRS) | / | ||||
| EC50 (μg/L) | 296 (HRS) 243(day 1, KRS) 172 (steady state, KRS) | 36.6% (HRS) 50.2% (KRS) | ||||
| Tanigawa et al. (2013) [26] | Two-step photometric assays | FXa = FXa0 × | FXa0 (U/mL) | 0.803 × [1 − 0.00656 × (age − 65.59)] | 4.8% | 6.9% |
| Emax (U/mL) | 0.928 | / | ||||
| EC50 (μg/L) | 221 | 10.6% | ||||
| Hill | 1.16 | / | ||||
| Girgis et al. (2014) [27] | Two-step photometric assays | FXa = FXa0 × | FXa0 | 104% c | 16.61% | 10.05% |
| Emax | 107% c | / | ||||
| EC50 (μg/L) | 760 | 5.97% | ||||
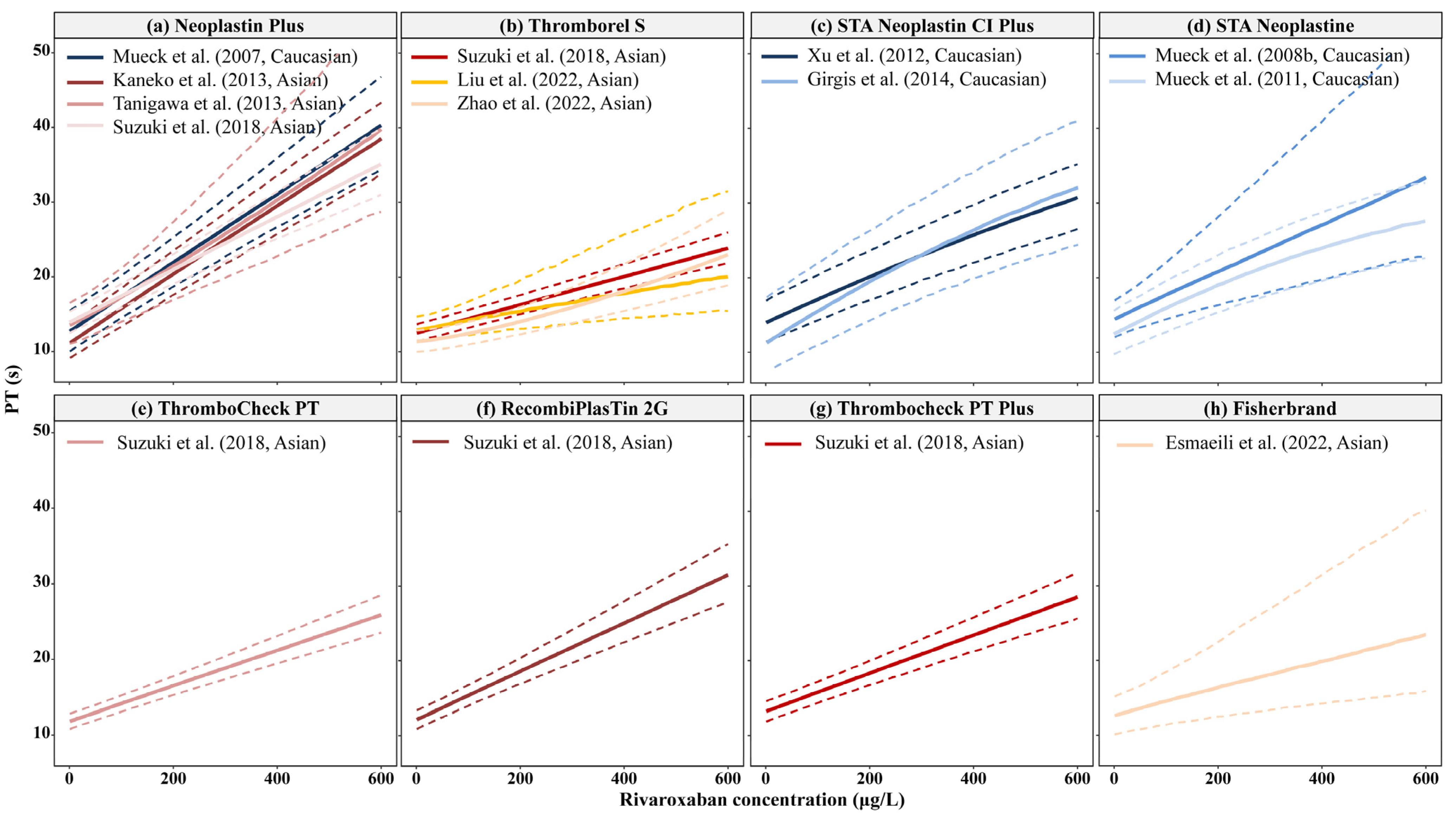
3.4.2. Pharmacodynamics Analysis: PT
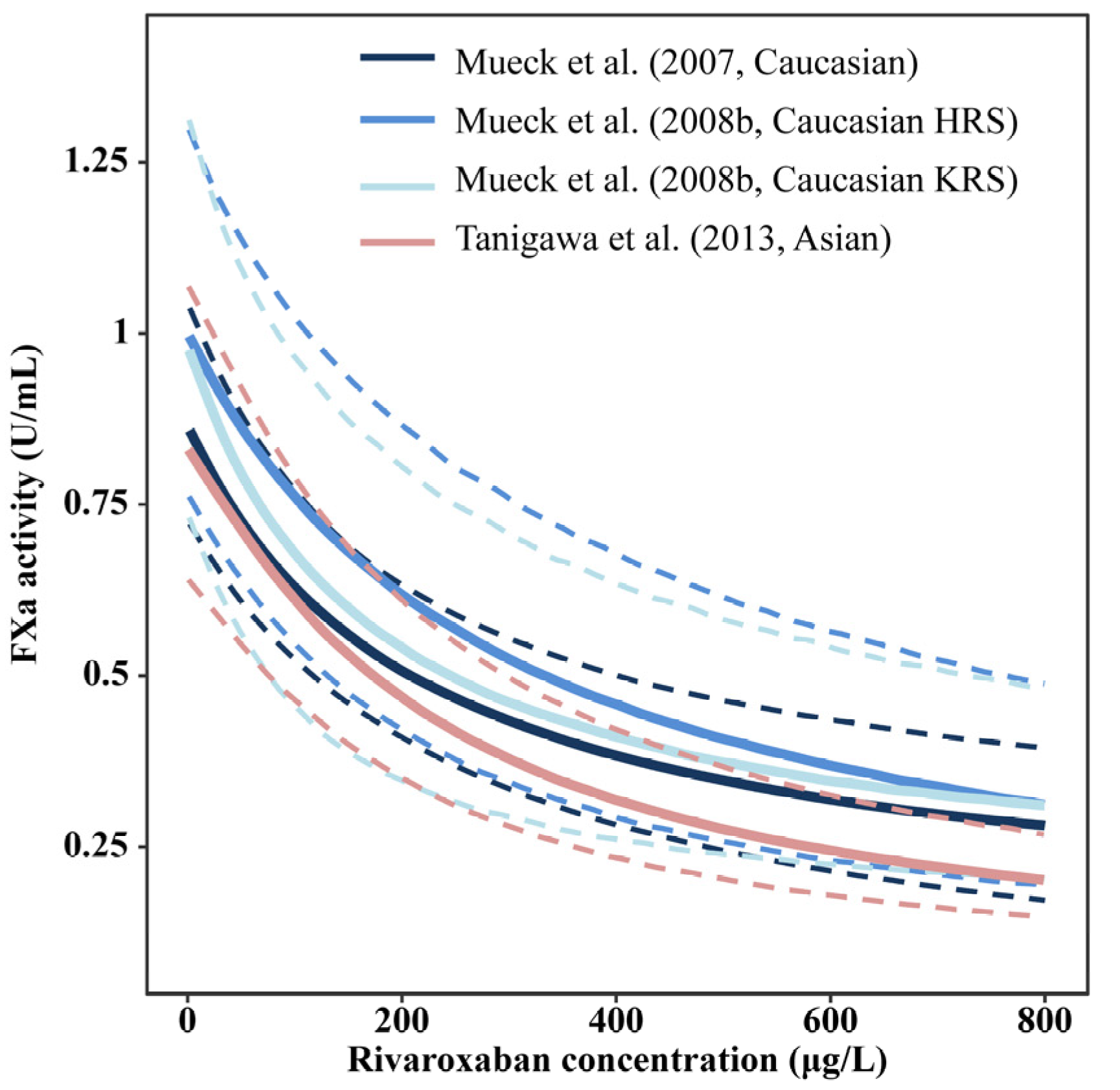
3.4.3. Pharmacodynamics Analysis: FXa Activity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trujillo, T.; Dobesh, P.P. Clinical use of rivaroxaban: Pharmacokinetic and pharmacodynamic rationale for dosing regimens in different indications. Drugs 2014, 74, 1587–1603. [Google Scholar] [CrossRef] [PubMed]
- Young, G.; Lensing, A.W.A.; Monagle, P.; Male, C.; Thelen, K.; Willmann, S.; Palumbo, J.S.; Kumar, R.; Nurmeev, I.; Hege, K.; et al. Rivaroxaban for treatment of pediatric venous thromboembolism. An Einstein-Jr phase 3 dose-exposure-response evaluation. J. Thromb. Haemost. 2020, 18, 1672–1685. [Google Scholar] [CrossRef] [PubMed]
- Male, C.; Lensing, A.W.A.; Palumbo, J.S.; Kumar, R.; Nurmeev, I.; Hege, K.; Bonnet, D.; Connor, P.; Hooimeijer, H.L.; Torres, M.; et al. Rivaroxaban compared with standard anticoagulants for the treatment of acute venous thromboembolism in children: A randomised, controlled, phase 3 trial. Lancet Haematol. 2020, 7, e18–e27. [Google Scholar] [CrossRef] [PubMed]
- Mueck, W.; Stampfuss, J.; Kubitza, D.; Becka, M. Clinical pharmacokinetic and pharmacodynamic profile of rivaroxaban. Clin. Pharmacokinet. 2014, 53, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Stampfuss, J.; Kubitza, D.; Becka, M.; Mueck, W. The effect of food on the absorption and pharmacokinetics of rivaroxaban. Int. J. Clin. Pharmacol. Ther. 2013, 51, 549–561. [Google Scholar] [CrossRef]
- Mueck, W.; Kubitza, D.; Becka, M. Co-administration of rivaroxaban with drugs that share its elimination pathways: Pharmacokinetic effects in healthy subjects. Br. J. Clin. Pharmacol. 2013, 76, 455–466. [Google Scholar] [CrossRef]
- Kvasnicka, T.; Malikova, I.; Zenahlikova, Z.; Kettnerova, K.; Brzezkova, R.; Zima, T.; Ulrych, J.; Briza, J.; Netuka, I.; Kvasnicka, J. Rivaroxaban—Metabolism, pharmacologic properties and drug interactions. Curr. Drug Metab. 2017, 18, 636–642. [Google Scholar] [CrossRef]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef]
- Hori, M.; Matsumoto, M.; Tanahashi, N.; Momomura, S.-I.; Uchiyama, S.; Goto, S.; Izumi, T.; Koretsune, Y.; Kajikawa, M.; Kato, M.; et al. Rivaroxaban vs. warfarin in Japanese patients with atrial fibrillation—The J-ROCKET AF study. Circ. J. 2012, 76, 2104–2111. [Google Scholar] [CrossRef]
- Chan, Y.H.; Lee, H.F.; Wang, C.L.; Chang, S.H.; Yeh, C.H.; Chao, T.F.; Yeh, Y.H.; Chen, S.A.; Kuo, C.T. Comparisons of rivaroxaban following different dosage criteria (ROCKET AF or J-ROCKET AF trials) in Asian patients with atrial fibrillation. J. Am. Heart Assoc. 2019, 8, e013053. [Google Scholar] [CrossRef]
- Lee, H.F.; Chan, Y.H.; Tu, H.T.; Kuo, C.T.; Yeh, Y.H.; Chang, S.H.; Wu, L.S.; See, L.C. The effectiveness and safety of low-dose rivaroxaban in Asians with non-valvular atrial fibrillation. Int. J. Cardiol. 2018, 261, 78–83. [Google Scholar] [CrossRef]
- Yu, H.T.; Yang, P.S.; Jang, E.; Kim, T.H.; Uhm, J.S.; Kim, J.Y.; Pak, H.N.; Lee, M.H.; Lip, G.Y.H.; Joung, B. Label Adherence of Direct Oral Anticoagulants Dosing and Clinical Outcomes in Patients with Atrial Fibrillation. J. Am. Heart Assoc. 2020, 9, e014177. [Google Scholar] [CrossRef]
- Hori, M.; Kajikawa, M. The J-ROCKET AF Study: A matter of ethnicity or a matter of weight? Reply. Circ. J. 2013, 77, 2637. [Google Scholar] [CrossRef]
- Terrier, J.; Gaspar, F.; Guidi, M.; Fontana, P.; Daali, Y.; Csajka, C.; Reny, J.L. Population Pharmacokinetic Models for Direct Oral Anticoagulants: A Systematic Review and Clinical Appraisal Using Exposure Simulation. Clin. Pharmacol. Ther. 2022, 112, 353–363. [Google Scholar] [CrossRef]
- Kanji, S.; Hayes, M.; Ling, A.; Shamseer, L.; Chant, C.; Edwards, D.J.; Edwards, S.; Ensom, M.H.; Foster, D.R.; Hardy, B.; et al. Reporting Guidelines for Clinical Pharmacokinetic Studies: The ClinPK Statement. Clin. Pharmacokinet. 2015, 54, 783–795. [Google Scholar] [CrossRef]
- Jamsen, K.M.; McLeay, S.C.; Barras, M.A.; Green, B. Reporting a population pharmacokinetic-pharmacodynamic study: A journal’s perspective. Clin. Pharmacokinet. 2014, 53, 111–122. [Google Scholar] [CrossRef]
- Duffull, S.B.; Wright, D.F. What do we learn from repeated population analyses? Br. J. Clin. Pharmacol. 2015, 79, 40–47. [Google Scholar] [CrossRef]
- Goto, E.; Horinaka, S.; Ishimitsu, T.; Kato, T. Factor Xa inhibitors in clinical practice: Comparison of pharmacokinetic profiles. Drug Metab. Pharmacokinet. 2020, 35, 151–159. [Google Scholar] [CrossRef]
- Mueck, W.; Becka, M.; Kubitza, D.; Voith, B.; Zuehlsdorf, M. Population model of the pharmacokinetics and pharmacodynamics of rivaroxaban—An oral, direct Factor Xa inhibitor—In healthy subjects. Int. J. Clin. Pharmacol. Ther. 2007, 45, 335–344. [Google Scholar] [CrossRef]
- Zhao, N.; Liu, Z.; Xie, Q.; Wang, Z.; Sun, Z.; Xiang, Q.; Cui, Y. A Combined Pharmacometrics Analysis of Biomarker Distribution Under Treatment with Standard- or Low-Dose Rivaroxaban in Real-World Chinese Patients With Nonvalvular Atrial Fibrillation. Front. Pharmacol. 2022, 13, 814724. [Google Scholar] [CrossRef]
- Mueck, W.; Borris, L.C.; Dahl, O.E.; Haas, S.; Huisman, M.V.; Kakkar, A.K.; Kälebo, P.; Muelhofer, E.; Misselwitz, F.; Eriksson, B.I. Population pharmacokinetics and pharmacodynamics of once-and twice-daily rivaroxaban for the prevention of venous thromboembolism in patients undergoing total hip replacement. Thromb. Haemost. 2008, 100, 453–461. [Google Scholar] [PubMed]
- Mueck, W.; Eriksson, B.I.; Bauer, K.A.; Borris, L.; Dahl, O.E.; Fisher, W.D.; Gent, M.; Haas, S.; Huisman, M.V.; Kakkar, A.K.; et al. Population pharmacokinetics and pharmacodynamics of rivaroxaban--an oral, direct factor Xa inhibitor—In patients undergoing major orthopaedic surgery. Clin. Pharmacokinet. 2008, 47, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Mueck, W.; Lensing, A.W.; Agnelli, G.; Decousus, H.; Prandoni, P.; Misselwitz, F. Rivaroxaban: Population pharmacokinetic analyses in patients treated for acute deep-vein thrombosis and exposure simulations in patients with atrial fibrillation treated for stroke prevention. Clin. Pharmacokinet. 2011, 50, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.S.; Moore, K.; Burton, P.; Stuyckens, K.; Mueck, W.; Rossenu, S.; Plotnikov, A.; Gibson, M.; Vermeulen, A. Population pharmacokinetics and pharmacodynamics of rivaroxaban in patients with acute coronary syndromes. Br. J. Clin. Pharmacol. 2012, 74, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, M.; Tanigawa, T.; Hashizume, K.; Kajikawa, M.; Tajiri, M.; Mueck, W. Confirmation of model-based dose selection for a Japanese phase III study of rivaroxaban in non-valvular atrial fibrillation patients. Drug Metab. Pharmacokinet. 2013, 28, 321–331. [Google Scholar] [CrossRef]
- Tanigawa, T.; Kaneko, M.; Hashizume, K.; Kajikawa, M.; Ueda, H.; Tajiri, M.; Paolini, J.F.; Mueck, W. Model-based dose selection for phase III rivaroxaban study in Japanese patients with non-valvular atrial fibrillation. Drug Metab. Pharmacokinet. 2013, 28, 59–70. [Google Scholar] [CrossRef]
- Girgis, I.G.; Patel, M.R.; Peters, G.R.; Moore, K.T.; Mahaffey, K.W.; Nessel, C.C.; Halperin, J.L.; Califf, R.M.; Fox, K.A.; Becker, R.C. Population pharmacokinetics and pharmacodynamics of rivaroxaban in patients with non-valvular atrial fibrillation: Results from ROCKET AF. J. Clin. Pharmacol. 2014, 54, 917–927. [Google Scholar] [CrossRef]
- Barsam, S.J.; Patel, J.P.; Roberts, L.N.; Kavarthapu, V.; Patel, R.K.; Green, B.; Arya, R. The impact of body weight on rivaroxaban pharmacokinetics. Res. Pract. Thromb. Haemost. 2017, 1, 180–187. [Google Scholar] [CrossRef]
- Zhang, L.; Peters, G.; Haskell, L.; Patel, P.; Nandy, P.; Moore, K.T. A Cross-Study Analysis Evaluating the Effects of Food on the Pharmacokinetics of Rivaroxaban in Clinical Studies. J. Clin. Pharmacol. 2017, 57, 1607–1615. [Google Scholar] [CrossRef]
- Suzuki, S.; Yamashita, T.; Kasai, H.; Otsuka, T.; Sagara, K. An analysis on distribution and inter-relationships of biomarkers under rivaroxaban in Japanese patients with non-valvular atrial fibrillation (CVI ARO 1). Drug Metab. Pharmacokinet. 2018, 33, 188–193. [Google Scholar] [CrossRef]
- Willmann, S.; Zhang, L.; Frede, M.; Kubitza, D.; Mueck, W.; Schmidt, S.; Solms, A.; Yan, X.; Garmann, D. Integrated population pharmacokinetic analysis of rivaroxaban across multiple patient populations. CPT Pharmacomet. Syst. Pharmacol. 2018, 7, 309–320. [Google Scholar] [CrossRef]
- Zdovc, J.; Petre, M.; Pišlar, M.; Repnik, K.; Mrhar, A.; Vogrin, M.; Potočnik, U.; Grabnar, I. Downregulation of ABCB1 gene in patients with total hip or knee arthroplasty influences pharmacokinetics of rivaroxaban: A population pharmacokinetic-pharmacodynamic study. Eur. J. Clin. Pharmacol. 2019, 75, 817–824. [Google Scholar] [CrossRef]
- Speed, V.; Green, B.; Roberts, L.N.; Woolcombe, S.; Bartoli-Abdou, J.; Barsam, S.; Byrne, R.; Gee, E.; Czuprynska, J.; Brown, A.; et al. Fixed dose rivaroxaban can be used in extremes of bodyweight: A population pharmacokinetic analysis. J. Thromb. Haemost. 2020, 18, 2296–2307. [Google Scholar] [CrossRef]
- Liu, X.Q.; Zhang, Y.F.; Ding, H.Y.; Yan, M.M.; Jiao, Z.; Zhong, M.K.; Ma, C.L. Population pharmacokinetic and pharmacodynamic analysis of rivaroxaban in Chinese patients with non-valvular atrial fibrillation. Acta Pharmacol. Sin. 2022, 43, 2723–2734. [Google Scholar] [CrossRef]
- Singkham, N.; Phrommintikul, A.; Pacharasupa, P.; Norasetthada, L.; Gunaparn, S.; Prasertwitayakij, N.; Wongcharoen, W.; Punyawudho, B. Population Pharmacokinetics and Dose Optimization Based on Renal Function of Rivaroxaban in Thai Patients with Non-Valvular Atrial Fibrillation. Pharmaceutics 2022, 14, 1744. [Google Scholar] [CrossRef]
- Zhang, D.; Chen, W.; Qin, W.; Du, W.; Wang, X.; Zuo, X.; Li, P. Population Pharmacokinetics and Hemorrhagic Risk Analysis of Rivaroxaban in Elderly Chinese Patients with Nonvalvular Atrial Fibrillation. J. Clin. Pharmacol. 2023, 53, 66–76. [Google Scholar] [CrossRef]
- Zhang, F.; Chen, X.; Wu, T.; Huang, N.; Li, L.; Yuan, D.; Xiang, J.; Wang, N.; Chen, W.; Zhang, J. Population Pharmacokinetics of Rivaroxaban in Chinese Patients with Non-Valvular Atrial Fibrillation: A Prospective Multicenter Study. Clin. Pharmacokinet. 2022, 61, 881–893. [Google Scholar] [CrossRef]
- Esmaeili, T.; Rezaee, M.; Abdar Esfahani, M.; Davoudian, A.; Omidfar, D.; Rezaee, S. Rivaroxaban population pharmacokinetic and pharmacodynamic modeling in Iranian patients. J. Clin. Pharm. Ther. 2022, 47, 1284–1292. [Google Scholar] [CrossRef]
- Willmann, S.; Thelen, K.; Kubitza, D.; Lensing, A.W.A.; Frede, M.; Coboeken, K.; Stampfuss, J.; Burghaus, R.; Mück, W.; Lippert, J. Pharmacokinetics of rivaroxaban in children using physiologically based and population pharmacokinetic modelling: An EINSTEIN-Jr phase I study. Thromb. J. 2018, 16, 32. [Google Scholar] [CrossRef]
- Willmann, S.; Coboeken, K.; Zhang, Y.; Mayer, H.; Ince, I.; Mesic, E.; Thelen, K.; Kubitza, D.; Lensing, A.W.A.; Yang, H.; et al. Population pharmacokinetic analysis of rivaroxaban in children and comparison to prospective physiologically-based pharmacokinetic predictions. CPT Pharmacomet. Syst. Pharmacol. 2021, 10, 1195–1207. [Google Scholar] [CrossRef]
- Willmann, S.; Ince, I.; Ahsman, M.; Coboeken, K.; Zhang, Y.; Thelen, K.; Kubitza, D.; Zannikos, P.; Zhou, W.; Pina, L.M.; et al. Model-informed bridging of rivaroxaban doses for thromboprophylaxis in pediatric patients aged 9 years and older with congenital heart disease. CPT Pharmacomet. Syst. Pharmacol. 2022, 11, 1111–1121. [Google Scholar] [CrossRef] [PubMed]
- Holford, N.; Yim, D.S. Clearance. Trans. Clin. Pharmacol. 2015, 23, 42–45. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, M.; Chen, H.; Wang, F. Influence of ABCB1 gene polymorphism on rivaroxaban blood concentration and hemorrhagic events in patients with atrial fibrillation. Front. Pharmacol. 2021, 12, 639854. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/xarelto-epar-product-information_en.pdf (accessed on 13 January 2023).
- Food and Drug Administration. XARELTO® (Insert Package). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/215859s000lbl.pdf (accessed on 1 November 2022).
- Zhao, X.; Sun, P.; Zhou, Y.; Liu, Y.; Zhang, H.; Mueck, W.; Kubitza, D.; Bauer, R.J.; Zhang, H.; Cui, Y. Safety, pharmacokinetics and pharmacodynamics of single/multiple doses of the oral, direct Factor Xa inhibitor rivaroxaban in healthy Chinese subjects. Br. J. Clin. Pharmacol. 2009, 68, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Kubitza, D.; Becka, M.; Wensing, G.; Voith, B.; Zuehlsdorf, M. Safety, pharmacodynamics, and pharmacokinetics of BAY 59-7939—An oral, direct Factor Xa inhibitor—After multiple dosing in healthy male subjects. Eur. J. Clin. Pharmacol. 2005, 61, 873–880. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, X.; Fox, K.A.A.; Willmann, S.; Nandy, P.; Berkowitz, S.D.; Hermanowski-Vosatka, A.; Weitz, J.I.; Solms, A.; Schmidt, S.; et al. Associations between model-predicted rivaroxaban exposure and patient characteristics and efficacy and safety outcomes in patients with non-valvular atrial fibrillation. J. Thromb. Thrombolysis 2020, 50, 20–29. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, X.; Nandy, P.; Willmann, S.; Fox, K.A.A.; Berkowitz, S.D.; Sharma, A.; Hermanowski-Vosatka, A.; Schmidt, S.; Weitz, J.I.; et al. Influence of model-predicted rivaroxaban exposure and patient characteristics on efficacy and safety outcomes in patients with acute coronary syndrome. Ther. Adv. Cardiovasc. Dis. 2019, 13, 1753944719863641. [Google Scholar] [CrossRef]
- Reinecke, I.; Solms, A.; Willmann, S.; Spiro, T.E.; Peters, G.; Weitz, J.I.; Mueck, W.; Garmann, D.; Schmidt, S.; Zhang, L.; et al. Associations between model-predicted rivaroxaban exposure and patient characteristics and efficacy and safety outcomes in the prevention of venous thromboembolism. J. Thromb. Thrombolysis 2020, 50, 12–19. [Google Scholar] [CrossRef]
- Kampouraki, E.; Abohelaika, S.; Avery, P.; Biss, T.; Murphy, P.; Wynne, H.; Kamali, F. Elderly people are inherently sensitive to the pharmacological activity of rivaroxaban: Implications for DOAC prescribing. J. Thromb. Thrombolysis 2021, 52, 170–178. [Google Scholar] [CrossRef]
- Batchelor, H.K.; Marriott, J.F. Paediatric pharmacokinetics: Key considerations. Br. J. Clin. Pharmacol. 2015, 79, 395–404. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, T.; Ogawa, S.; Kitazono, T.; Nakagawara, J.; Minematsu, K.; Miyamoto, S.; Murakawa, Y.; Iwashiro, S.; Okayama, Y.; Sunaya, T.; et al. Real-world safety and effectiveness of rivaroxaban using Japan-specific dosage during long-term follow-up in patients with atrial fibrillation: XAPASS. PLoS ONE 2021, 16, e0251325. [Google Scholar] [CrossRef]
- Chan, Y.H.; Chao, T.F.; Chen, S.W.; Lee, H.F.; Yeh, Y.H.; Huang, Y.C.; Chang, S.H.; Kuo, C.T.; Lip, G.Y.H.; Chen, S.A. Off-label dosing of non-vitamin K antagonist oral anticoagulants and clinical outcomes in Asian patients with atrial fibrillation. Heart Rhythm 2020, 17, 2102–2110. [Google Scholar] [CrossRef]
- Lee, S.R.; Lee, Y.S.; Park, J.S.; Cha, M.J.; Kim, T.H.; Park, J.; Park, J.K.; Lee, J.M.; Kang, K.W.; Shim, J.; et al. Label Adherence for Non-Vitamin K Antagonist Oral Anticoagulants in a Prospective Cohort of Asian Patients with Atrial Fibrillation. Yonsei Med. J. 2019, 60, 277–284. [Google Scholar] [CrossRef]
- Amarenco, P.; Haas, S.; Hess, S.; Kirchhof, P.; Lambelet, M.; Bach, M.; Turpie, A.G.G.; Camm, A.J. Outcomes associated with non-recommended dosing of rivaroxaban: Results from the XANTUS study. Eur. Heart J. Cardiovasc. Pharmacother. 2019, 5, 70–79. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.-Q.; Li, Z.-R.; Wang, C.-Y.; Chen, Y.-T.; Jiao, Z. Is a Lower Dose of Rivaroxaban Required for Asians? A Systematic Review of a Population Pharmacokinetics and Pharmacodynamics Analysis of Rivaroxaban. Pharmaceutics 2023, 15, 588. https://doi.org/10.3390/pharmaceutics15020588
Liu X-Q, Li Z-R, Wang C-Y, Chen Y-T, Jiao Z. Is a Lower Dose of Rivaroxaban Required for Asians? A Systematic Review of a Population Pharmacokinetics and Pharmacodynamics Analysis of Rivaroxaban. Pharmaceutics. 2023; 15(2):588. https://doi.org/10.3390/pharmaceutics15020588
Chicago/Turabian StyleLiu, Xiao-Qin, Zi-Ran Li, Chen-Yu Wang, Yue-Ting Chen, and Zheng Jiao. 2023. "Is a Lower Dose of Rivaroxaban Required for Asians? A Systematic Review of a Population Pharmacokinetics and Pharmacodynamics Analysis of Rivaroxaban" Pharmaceutics 15, no. 2: 588. https://doi.org/10.3390/pharmaceutics15020588