
Adalimumab Serum Concentrations, Clinical and Endoscopic Disease Activity in Crohn’s Disease: A Cross-Sectional Multicentric Latin American Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Variables Analyzed
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Di Domenicantonio, R.; Trotta, F.; Cascini, S.; Agabiti, N.; Kohn, A.; Gasbarrini, A.; Davoli, M.; Addis, A. Population-based cohort study on comparative effectiveness and safety of biologics in inflammatory bowel disease. Clin. Epidemiol. 2018, 10, 203–213. [Google Scholar] [CrossRef]
- Karmiris, K.; Paintaud, G.; Noman, M.; Magdelaine–Beuzelin, C.; Ferrante, M.; Degenne, D.; Claes, K.; Coopman, T.; Van Schuerbeek, N.; Van Assche, G.; et al. Influence of Trough Serum Levels and Immunogenicity on Long-term Outcome of Adalimumab Therapy in Crohn’s Disease. Gastroenterology 2009, 137, 1628–1640. [Google Scholar] [CrossRef]
- Hanauer, S.B.; Sandborn, W.J.; Rutgeerts, P.; Fedorak, R.; Lukas, M.; MacIntosh, D.; Panaccione, R.; Wolf, D.; Pollack, P. Human anti tumor necrosis factor monoclonal antibody (adalimumab) in Crohn’s disease: The CLASSIC-I trial. Gastroenterology 2006, 130, 323–333. [Google Scholar]
- Sandborn, W.J.; Hanauer, S.B.; Rutgeerts, P.; Fedorak, R.; Lukas, M.; MacIntosh, D.G.; Panaccione, R.; Wolf, D.; Kent, J.D.; Bittle, B.; et al. Adalimumab for maintenance treatment of Crohn’s disease: Results of the CLASSIC II trial. Gut 2007, 56, 1232–1239. [Google Scholar]
- Colombel, J.; Sandborn, W.J.; Rutgeerts, P.; Enns, R.; Hanauer, S.B.; Panaccione, R.; Schreiber, S.; Byczkowski, D.; Li, J.; Kent, J.D.; et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn’s disease: The CHARM trial. Gastroenterology 2007, 132, 52–65. [Google Scholar] [CrossRef]
- Panaccione, R.; Colombel, J.-F.; Sandborn, W.J.; Rutgeerts, P.; D’Haens, G.R.; Robinson, A.M.; Chao, J.; Mulani, P.M.; Pollack, P.F. Adalimumab sustains clinical remission and overall clinical benefit after 2 years of therapy for Crohn’s disease. Aliment Pharmacol. Ther. 2010, 31, 1296–1309. [Google Scholar]
- Mitrev, N.; Casteele, N.V.; Seow, C.H.; Andrews, J.M.; Connor, S.J.; Moore, G.T.; Barclay, M.; Begun, J.; Bryant, R.; Chan, W.; et al. Review article: Consensus statements on therapeutic drug monitoring of anti-tumour necrosis factor therapy in inflammatory bowel diseases. Aliment Pharmacol. Ther. 2017, 46, 1037–1053. [Google Scholar] [CrossRef]
- Bodini, G.; Giannini, E.; Savarino, V.; Del Nero, L.; Pellegatta, G.; De Maria, C.; Baldissarro, I.; Savarino, E. Adalimumab trough serum levels and anti-adalimumab antibodies in the long-term clinical outcome of patients with Crohn’s disease. Scand. J. Gastroenterol. 2016, 51, 1081–1086. [Google Scholar] [PubMed]
- Ribaldone, D.G.; Manetta, T.; Mengozzi, G.; Saracco, G.M.; Pellicano, R.; Astegiano, M. Adalimumab trough levels predict Crohn’s disease clinical course. Dig. Liver Dis. 2018, 50, 204–206. [Google Scholar]
- Van Hoeve, K.; Hoffman, I.; Vermeire, S. Therapeutic drug monitoring of anti-TNF therapy in children with inflammatory bowel disease. Expert Opin. Drug. Saf. 2018, 17, 185–196. [Google Scholar] [CrossRef]
- Yoshihara, T.; Shinzaki, S.; Kawai, S.; Fujii, H.; Iwatani, S.; Yamaguchi, T.; Araki, M.; Hiyama, S.; Inoue, T.; Hayashi, Y.; et al. Tissue Drug Concentrations of Anti-tumor Necrosis Factor Agents Are Associated with the Long-term Outcome of Patients with Crohn’s Disease. Inflamm. Bowel Dis. 2017, 23, 2172–2179. [Google Scholar]
- Mazor, Y.; Almog, R.; Kopylov, U.; Ben Hur, D.; Blatt, A.; Dahan, A.; Waterman, M.; Ben-Horin, S.; Chowers, Y. Adalimumab drug and antibody levels as predictors of clinical and laboratory response in patients with Crohn’s disease. Aliment Pharmacol. Ther. 2014, 40, 620–628. [Google Scholar]
- Roblin, X.; Marotte, H.; Rinaudo, M.; Del Tedesco, E.; Moreau, A.; Phelip, J.M.; Genin, C.; Peyrin–Biroulet, L.; Paul, S. Association Between Pharmacokinetics of Adalimumab and Mucosal Healing in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2014, 12, 80–84.e2. [Google Scholar] [CrossRef]
- Ungar, B.; Levy, I.; Yavne, Y.; Yavzori, M.; Picard, O.; Fudim, E.; Loebstein, R.; Chowers, Y.; Eliakim, R.; Kopylov, U.; et al. Optimizing Anti-TNF-α Therapy: Serum Levels of Infliximab and Adalimumab Are Associated with Mucosal Healing in Patients With Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2016, 14, 550–557.e2. [Google Scholar]
- Feuerstein, J.D.; Nguyen, G.C.; Kupfer, S.S.; Falck-Ytter, Y.; Singh, S.; Gerson, L.; Hirano, I.; Rubenstein, J.H.; Smalley, W.E.; Stollman, N.; et al. American Gastroenterological Association Institute Guideline on Therapeutic Drug Monitoring in Inflammatory Bowel Disease. Gastroenterology 2017, 153, 827–834. [Google Scholar]
- Bian, S.; Lu, J.; Delport, F.; Vermeire, S.; Spasic, D.; Lammertyn, J.; Gils, A. Development and validation of an optical biosensor for rapid monitoring of adalimumab in serum of patients with Crohn’s disease. Drug Test Anal. 2017, 10, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, M.S.; Satsangi, J.; Ahmad, T.; Arnott, I.D.R.; Bernstein, C.N.; Brant, S.R.; Caprilli, R.; Colombel, J.-F.; Gasche, C.; Geboes, K.; et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: Report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can. J. Gastroenterol. 2005, 19 (Suppl. A), 5A–36A. [Google Scholar]
- Harvey, R.F.; Bradshaw, J.M. A simple index of Crohn’s-disease activity. Lancet Lond. Engl. 1980, 1, 514. [Google Scholar]
- Daperno, M.; D’Haens, G.; Van Assche, G.; Baert, F.; Bulois, P.; Maunoury, V.; Sostegni, R.; Rocca, R.; Pera, A.; Gevers, A.; et al. Development and validation of a new, simplified endoscopic activity score for Crohn’s disease: The SES-CD. Gastrointest. Endosc. 2004, 60, 505–512. [Google Scholar]
- Freire, P.; Portela, F.; Sofia, C. Scores Endoscópicos na Doença de Crohn: Artigo de Revisão. Rev. Port. Coloproct. 2010, 7, 126–134. [Google Scholar]
- Dhaliwal, J.; Leach, S.; Katz, T.; Nahidi, L.; Pang, T.; Lee, J.M.; Strachan, R.; Day, A.S.; Jaffe, A.; Ooi, C.Y. Intestinal Inflammation and Impact on Growth in Children with Cystic Fibrosis. J. Pediatr. Gastroenterol. Nutr. 2015, 6, 21–526. [Google Scholar]
- Paul, S.; Moreau, A.C.; Del Tedesco, E.; Rinaudo, M.; Phelip, J.M.; Genin, C.; Peurin-Biroulet, L.; Roblin, X. Pharmacokinetics of adalimumab in inflammatory bowel diseases: A systematic review and meta-analyses. Inflamm. Bowel Dis. 2014, 20, 1288–1295. [Google Scholar]
- Chiu, Y.L.; Rubin, D.T.; Vermeire, S.; Louis, E.; Robinson, A.M.; Lomax, K.G.; Pollack, P.F.; Paulson, S.K. Serum adalimumab concentratios and clinical remission in patients wih Crohn’s Disease. Inflamm. Bowel Dis. 2013, 19, 1112–1122. [Google Scholar] [CrossRef]
- Yarur, A.J.; Jain, A.; Hauenstein, S.I.; Quintero, M.A.; Barkin, J.S.; Deshpande, A.R.; Sussman, D.A.; Singh, S.; Abreu, M.T. Higher Adalimuman Levels Are Associated with Histologic and Endoscopic Remission in Patients with Crohn’s Disease and Ulcerative Colitis. Inflamm. Bowel Dis. 2016, 22, 409–415. [Google Scholar] [CrossRef] [Green Version]
- Aguas Peris, M.; Bosó, V.; Navarro, B.; Marqués-Miñana, M.R.; Bastida, G.; Beltrán, B.; Iborra, M.; Sáez-González, E.; Monte-Boquet, E.; Poveda-Andrés, J.L.; et al. Serum Adalimumab Levels Predict Successful Remission and Safe Deintensification in Inflammatory Bowel Disease Patients in Clinical Practice. Inflamm. Bowel Dis. 2017, 23, 1454–1460. [Google Scholar] [PubMed]
- Papamichael, K.; Afif, W.; Drobne, D.; Dubinsky, M.C.; Ferrante, M.; Irving, P.M.; Kamperidis, N.; Kobayashi, T.; Kotze, P.G.; Lambert, J.; et al. Therapeutic drug monitoring of biologics in inflammatory bowel disease: Unmet needs and future perspectives. Lancet Gastroenterol. Hepatol. 2022, 7, 171–185. [Google Scholar]
- D’Haens, G.R.; Sandborn, W.J.; Loftus, E.V., Jr.; Hanauer, S.B.; Schreiber, S.; Peyrin-Biroulet, L.; Panaccione, R.; Panés, J.; Baert, F.; Colombel, J.-F.; et al. Higher vs. Standard Adalimumab Induction Dosing Regimens and Two Maintenance Strategies: Randomized SERENE CD Trial Results. Gastroenterology 2022, 162, 1876–1890. [Google Scholar]
- Rocha, C.; Afonso, J.; Lago, P.; Arroja, B.; Vieira, A.I.; Dias, C.C.; Magro, F. Accuracy of the new rapid test for monitoring adalimumab levels. Ther. Adv. Gastroenterol. 2019, 12, 1756284819828238. [Google Scholar] [CrossRef]
- Laserna-Mendieta, E.J.; Salvador-Martín, S.; Arias-González, L.; Ruiz-Ponce, M.; Menchén, L.A.; Sánchez, C.; López-Fernández, L.A.; Lucendo, A.J. Comparison of a new rapid method for the determination of adalimumab serum levels with two established ELISA kits. Clin. Chem. Lab. Med. 2019, 57, 1906–1914. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Active Disease (n = 27) | Clinical Remission (n = 62) | p-Value | |||
|---|---|---|---|---|---|
| Patients (N = 89) | |||||
| Age (years) (N = 89) | 39 ± 14.8 | 45 ± 13.7 | 0.518 | ||
| Duration of the disease (months) (N = 89) | 112.6 ± 100.7 | 132.5 ± 104.5 | 0.874 | ||
| Optimization time (months) (N = 31) | 12.2 ± 9.1 | 17.9 ± 13.9 | 0.194 | ||
| CRP (N = 77) | 8.2 ± 8.2 | 1.8 ± 3.4 | <0.05 | ||
| ESR (N = 49) | 35.6 ± 17.1 | 17.3 ± 20.8 | 0.705 | ||
| Albumin (N = 50) | 4.1 ± 0.46 | 4.1 ± 0.30 | 0.208 | ||
| Hemoglobin (N = 76) | 12.9 ± 1.9 | 13.2 ± 1.8 | 0.977 | ||
| Hematocrit (N = 76) | 38.7 ± 4.9 | 39.9 ± 4.6 | 0.624 | ||
| Calprotectin (N = 63) | 516 ± 397.9 | 231.9 ± 378.3 | 0.304 | ||
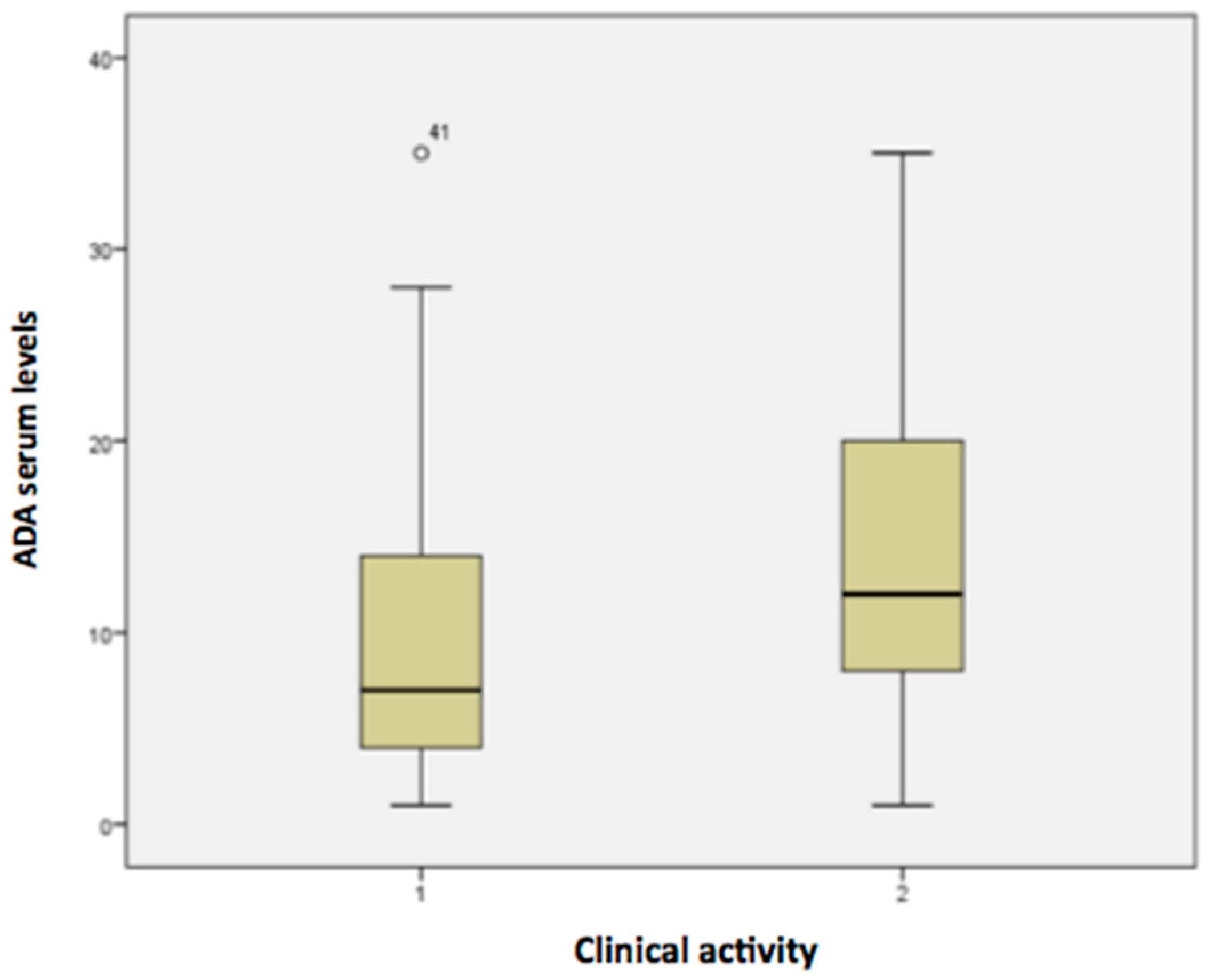
| ADA serum level (N = 89) | 10.2 ± 8.5 | 14.3 ± 9.4 | 0.395 | ||
| ADA levels in optimized (Md ± SD) | 10.5 ± 9.5 | p = 0.501 | 18.6 ± 8.9 | p = 0.894 | |
| ADA levels in non-optimized (Md ± SD) | 9.6 ± 6.8 | 13 ± 9.2 | |||
| BMI (N = 89) | 24.1 ± 4.9 | 25.9 ± 5.2 | 0.854 | ||
| HBI (N = 89) | 8.6 ± 3 | 1.6 ± 1.5 | <0.05 | ||
| Female (%) (N = 89) | 16 (17.9) | 37 (41.6) | 0.971 | ||
| Caucasian (%) (N = 89) | 22 (24.7) | 50 (56.2) | 0.472 | ||
| Non-smokers (%) (N = 89) | 21(23.6) | 46 (51.7) | 0.821 | ||
| Montreal Classification | |||||
| Age at onset—N (%) (N = 89) | 0.134 | ||||
| A1: ≤16 years | 4 (4.5) | 2 (2.2) | |||
| A2: 16–40 years | 17 (19.1) | 44 (49.4) | |||
| A3: >40 years | 6 (6.7) | 16 (17.9) | |||
| Disease location—N (%) (N = 89) | 0.703 | ||||
| L1: terminal ileum | 7 (1.1) | 16 (17.9) | |||
| L2: colonic | 3 (3.4) | 10 (11.2) | |||
| L3: ileocolonic | 17 (19.1) | 34 (38.2) | |||
| L4: isolated upper GI disease | 0 | 2 (2.2) | |||
| Disease behaviour—N (%) (N = 89) | 0.145 | ||||
| B1: nonstricturing, nonpenetrating | 13 (14.6) | 17 (19.1) | |||
| B2: stricturing | 8 (8.9) | 22 (24.7) | |||
| B3: penetrating | 6 (6.7) | 23 (25.8) | |||
| Perianal disease (%) (N = 89) | 16 (17.9) | 19 (21.3) | 0.011 | ||
| Use of imunossupressants | |||||
| AZA (%) (N = 89) | 16 (17.9) | 25 (28) | 0.099 | ||
| MTX (%) (N = 89) | 1 (1.1) | 0 | 0.128 | ||
| Corticosteroids (%) (N = 89) | 13 (14.6) | 18 (20.2) | 0.082 | ||
| Previous use of biologicals (%) (N = 89) | 10 (11.2) | 16 (17.9) | 0.284 | ||
| Previous surgery (%) (N = 89) | 16 (17.9) | 38 (42.7) | 0.857 | ||
| Endoscopic Activity (n = 40) | Endoscopic Remission (n = 49) | p-Value | |||
|---|---|---|---|---|---|
| Patients (N = 89) | |||||
| Age (years) (N = 89) | 39 ± 16.1 | 46 ± 11.7 | 0.029 | ||
| Disease duration (months) (N = 89) | 83.1 ± 78.2 | 161.9 ± 108.3 | 0.072 | ||
| Optimization time (months) (N = 31) | 14.4 ± 9.4 | 15.7 ± 15.9 | 0.178 | ||
| CRP (N = 77) | 7.4 ± 7.7 | 1.1 ± 2.1 | <0.05 | ||
| ESR (N = 49) | 28.7 ± 21.2 | 18.3 ± 20.6 | 0.358 | ||
| Albumin (N = 50) | 4 ± 0.36 | 4.2 ± 0.36 | 0.299 | ||
| Hemoglobin (N = 77) | 12.7 ± 1.8 | 13.4 ± 1.7 | 0.942 | ||
| Hematocrit (N = 77) | 38.4 ± 4.7 | 40.4 ± 4.5 | 0.466 | ||
| Calprotectin (N = 63) | 397.1 ± 373 | 245.24 ± 421.2 | 0.601 | ||
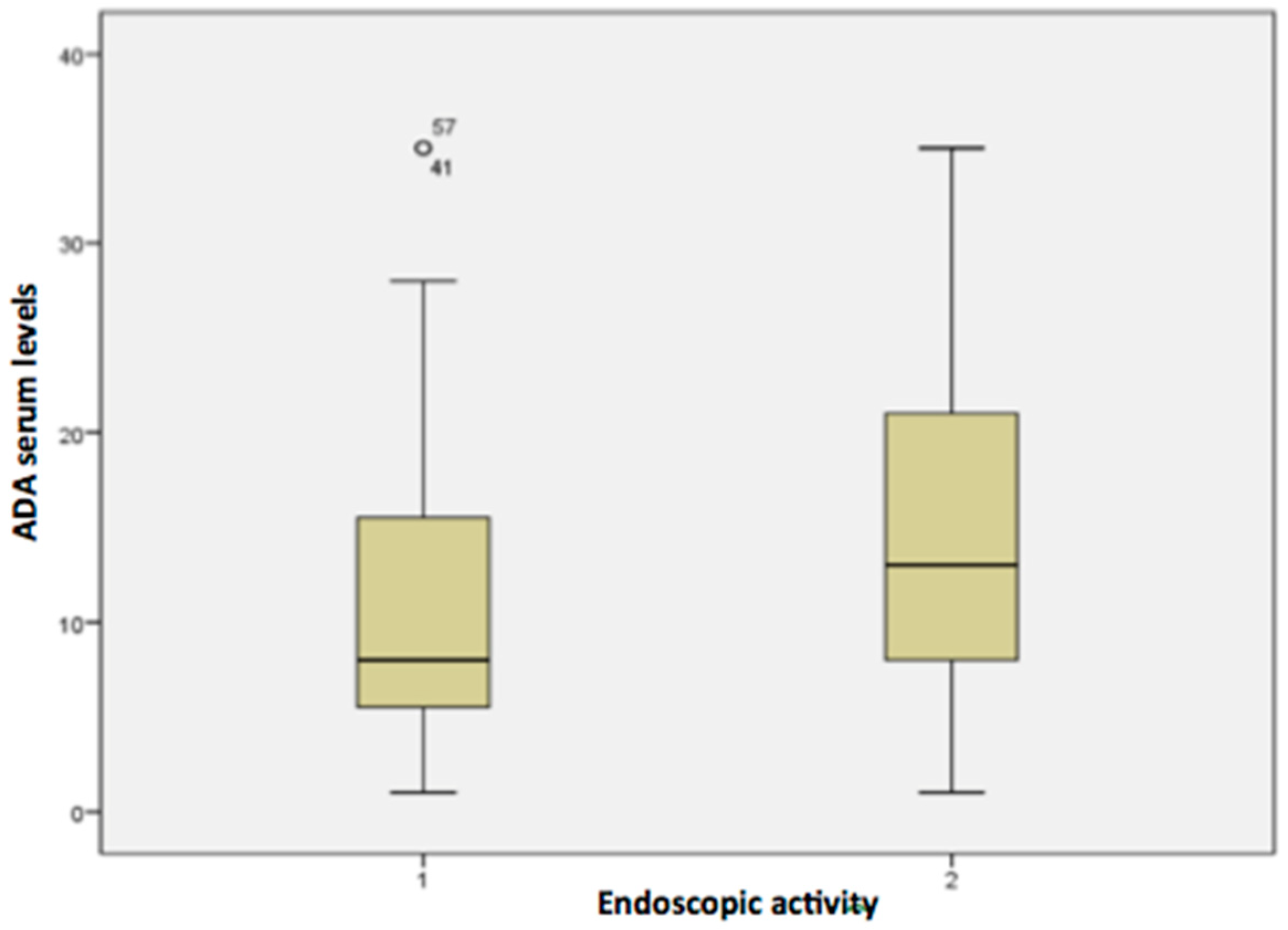
| ADA serum levels (N = 89) | 11.3 ± 8.8 | 14.5 ± 9.5 | 0.566 | ||
| ADA levels in optimized (Md ± SD) | 11.4 ± 9.4 | p = 0.386 | 19.9 ± 9.1 | p = 0.918 | |
| ADA levels in non optimized (Md ± SD) | 11.2 ± 8.3 | 13.1 ± 9.2 | |||
| BMI (N = 89) | 24.5 ± 4.9 | 26.2 ± 5.3 | 0.513 | ||
| HBI (N = 89) | 5.8 ± 4.3 | 2 ± 2.4 | <0.05 | ||
| ADA time of use (months) (N = 89) | 46.1 ± 32.7 | 55.6 ± 34.9 | 0.777 | ||
| Female (%) (N = 89) | 24 (26.9) | 29 (32.6) | 0.938 | ||
| Caucasian (%) (N = 89) | 34 (38.2) | 38 (42.7) | 0.269 | ||
| Non-smokers (%) (N = 89) | 31 (34.8) | 36 (40.4) | 0.874 | ||
| Montreal Classification | |||||
| Age at onset—N (%) (N = 89) | 0.102 | ||||
| A1: ≤16 years | 5 (5.6) | 1 (1.1) | |||
| A2: 16–40 years | 24 (26.9) | 37 (41.6) | |||
| A3: >40 years | 11 (12.4) | 11 (12.4) | |||
| Disease location—N (%) (N = 89) | 0.619 | ||||
| L1: terminal ileum | 13 (14.6) | 10 (11.2) | |||
| L2: colonic | 5 (5.6) | 8 (8.9) | |||
| L3: ileocolonic | 21 (23.6) | 30 (33.7) | |||
| L4: isolated upper disease | 1 (1.1) | 1 (1.1) | |||
| Disease behaviour—N (%) (N = 89) | 0.017 | ||||
| B1: nonstricturing, nonpenetrating | 19 (21.3) | 11 (12.4) | |||
| B2: stricturing | 8 (8.9) | 22 (24.7) | |||
| B3: penetrating | 13 (14.6) | 16 (17.9) | |||
| Perianal disease (%) (N = 89) | 21 (23.6) | 14 (15.7) | 0.022 | ||
| Use of imunossupressants | |||||
| AZA (%) (N = 89) | 22 (24.7) | 19 (21.3) | 0.127 | ||
| MTX (%) (N = 89) | 1 (1.1) | 0 | 0.266 | ||
| Corticosteroids (%) (N = 89) | 18 (20.2) | 13 (14.6) | 0.069 | ||
| Previous use of biologicals (%) (N = 89) | 14 (15.7) | 12 (13.5) | 0.278 | ||
| Previous surgery (%) (N = 89) | 23 (25.8) | 31 (34.8) | 0.58 | ||
| Cut-Off of Serum ADA Concentrations (µg/mL) | ||||||
|---|---|---|---|---|---|---|
| Cut-Off 5.0 µg/mL | Cut-Off 7.5 µg/mL | Cut-Off 12 µg/mL | ||||
| <5 | ≥5 | <7.5 | ≥7.5 | <12 | ≥12 | |
| Clinical disease activity, n (%) | ||||||
| Yes | 9 (50) | 19 (25) | 15 (50) | 12 (20.3) | 17 (37.0) | 10 (23.3) |
| No | 9 (50) | 57 (75) | 15 (50) | 47 (79.7) | 29 (63.0) | 33 (76.7) |
| p-value | 0.573 | 0.0001 | 1.000 | 0.0001 | 0.109 | 0.001 |
| Endoscopic disease activity, n (%) | ||||||
| Yes | 8 (61.5) | 31 (40.8) | 18 (60) | 22 (37.3) | 25 (54.3) | 15 (34.9) |
| No | 5 (38.5) | 45 (59.2) | 12 (40) | 37 (62.7) | 21 (45.6) | 28 (65.1) |
| p-value | 0.255 | 0.139 | 0.362 | 0.067 | 0.662 | 0.069 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Souza, L.R.; Magro, D.O.; Teixeira, F.V.; Parra, R.S.; Miranda, E.F.; Féres, O.; Saad-Hossne, R.; Soares Prates Herrerias, G.; Nisihara, R.M.; Coy, C.S.R.; et al. Adalimumab Serum Concentrations, Clinical and Endoscopic Disease Activity in Crohn’s Disease: A Cross-Sectional Multicentric Latin American Study. Pharmaceutics 2023, 15, 586. https://doi.org/10.3390/pharmaceutics15020586
de Souza LR, Magro DO, Teixeira FV, Parra RS, Miranda EF, Féres O, Saad-Hossne R, Soares Prates Herrerias G, Nisihara RM, Coy CSR, et al. Adalimumab Serum Concentrations, Clinical and Endoscopic Disease Activity in Crohn’s Disease: A Cross-Sectional Multicentric Latin American Study. Pharmaceutics. 2023; 15(2):586. https://doi.org/10.3390/pharmaceutics15020586
Chicago/Turabian Stylede Souza, Letícia Rodrigues, Daniela Oliveira Magro, Fábio Vieira Teixeira, Rogério Serafim Parra, Eron Fábio Miranda, Omar Féres, Rogério Saad-Hossne, Giedre Soares Prates Herrerias, Renato Mitsunori Nisihara, Claudio Saddy Rodrigues Coy, and et al. 2023. "Adalimumab Serum Concentrations, Clinical and Endoscopic Disease Activity in Crohn’s Disease: A Cross-Sectional Multicentric Latin American Study" Pharmaceutics 15, no. 2: 586. https://doi.org/10.3390/pharmaceutics15020586