
Pharmacodynamic and Pharmacokinetic Drug Interactions between Fexuprazan, a Novel Potassium-Competitive Inhibitor, and Aspirin, in Healthy Subjects
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Platelet Aggregation Assays
2.4. Determination of the Drug Concentrations
2.5. Pharmacodynamic and Pharmacokinetic Analyses
2.6. Safety Assessments
2.7. Statistical Analysis
3. Results
3.1. Study Population
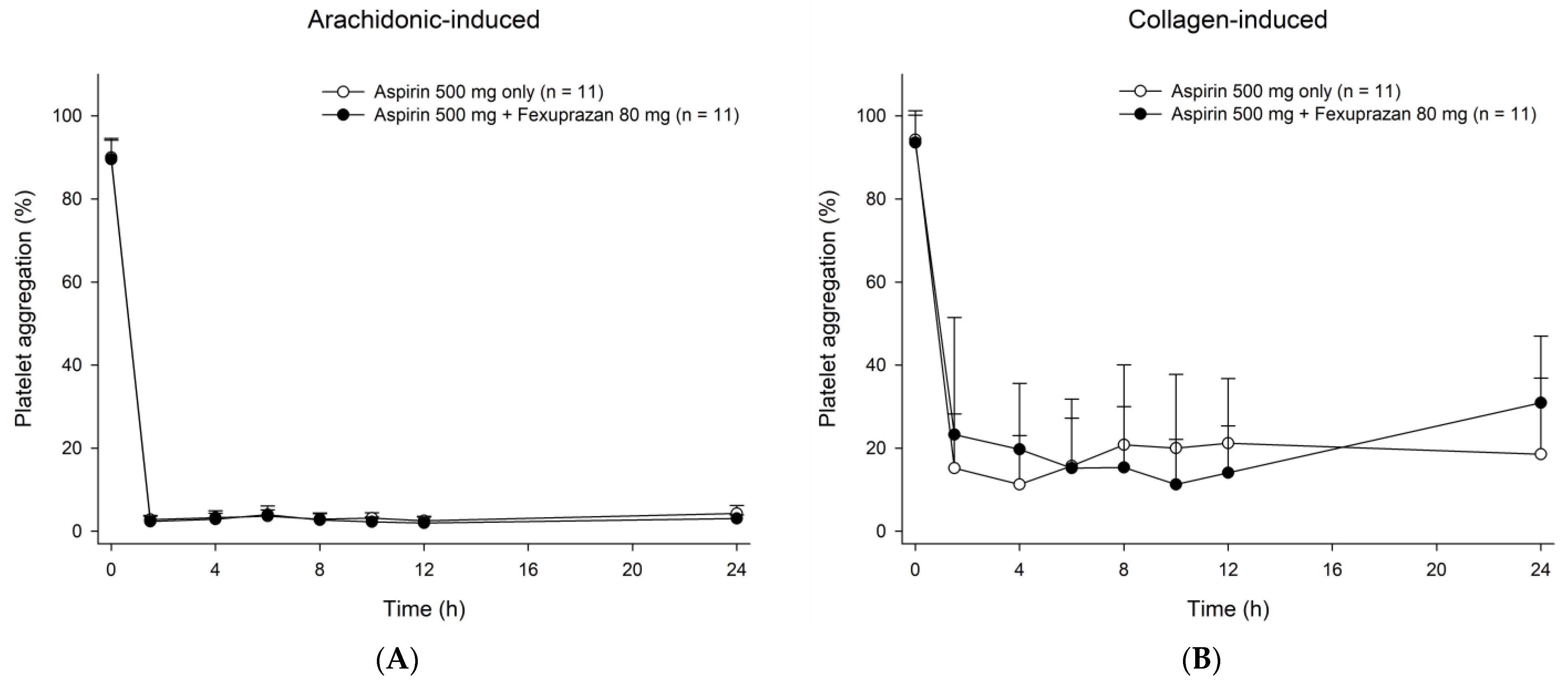
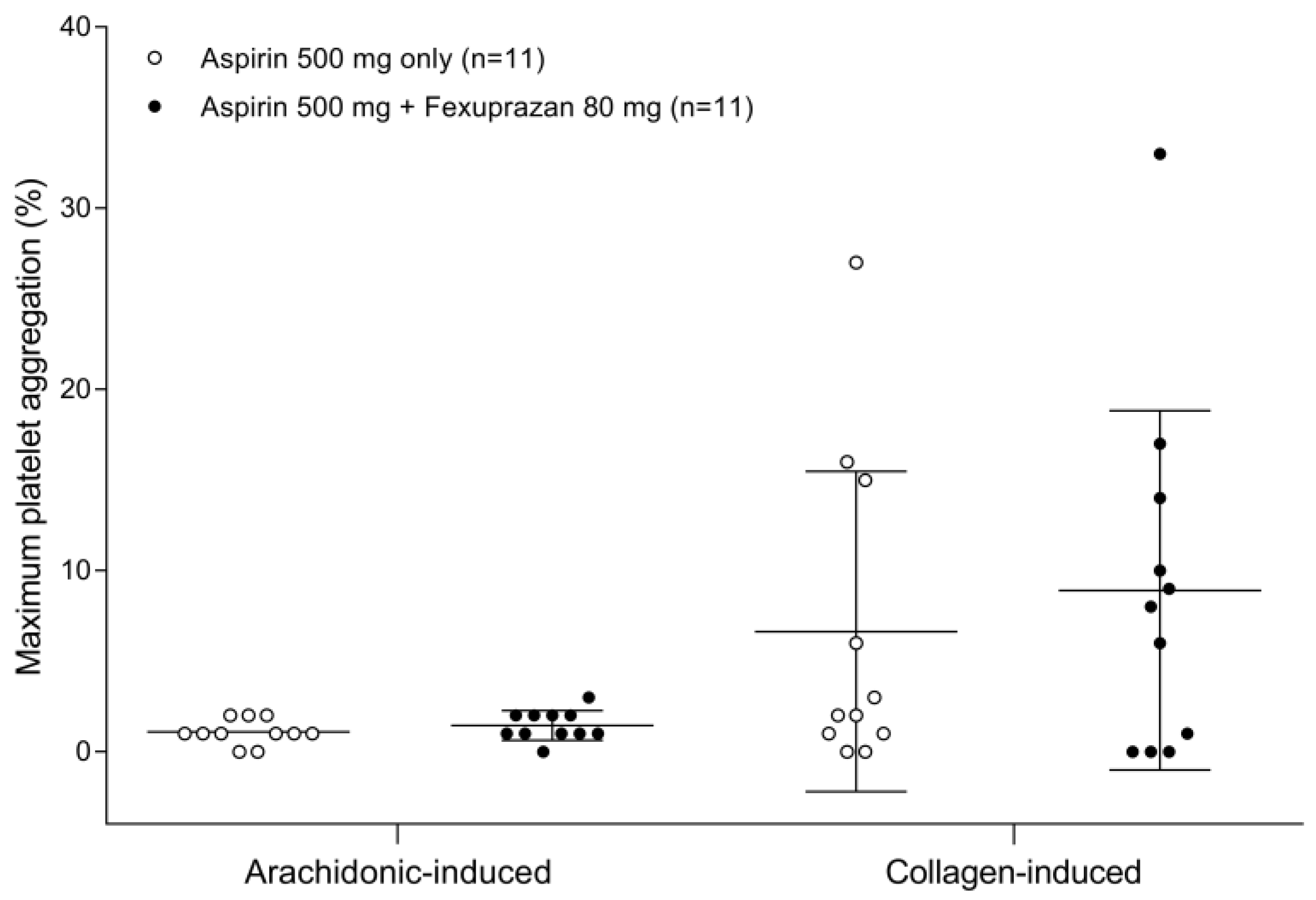
3.2. Effect of Fexuprazan on the Pharmacodynamics of Aspirin
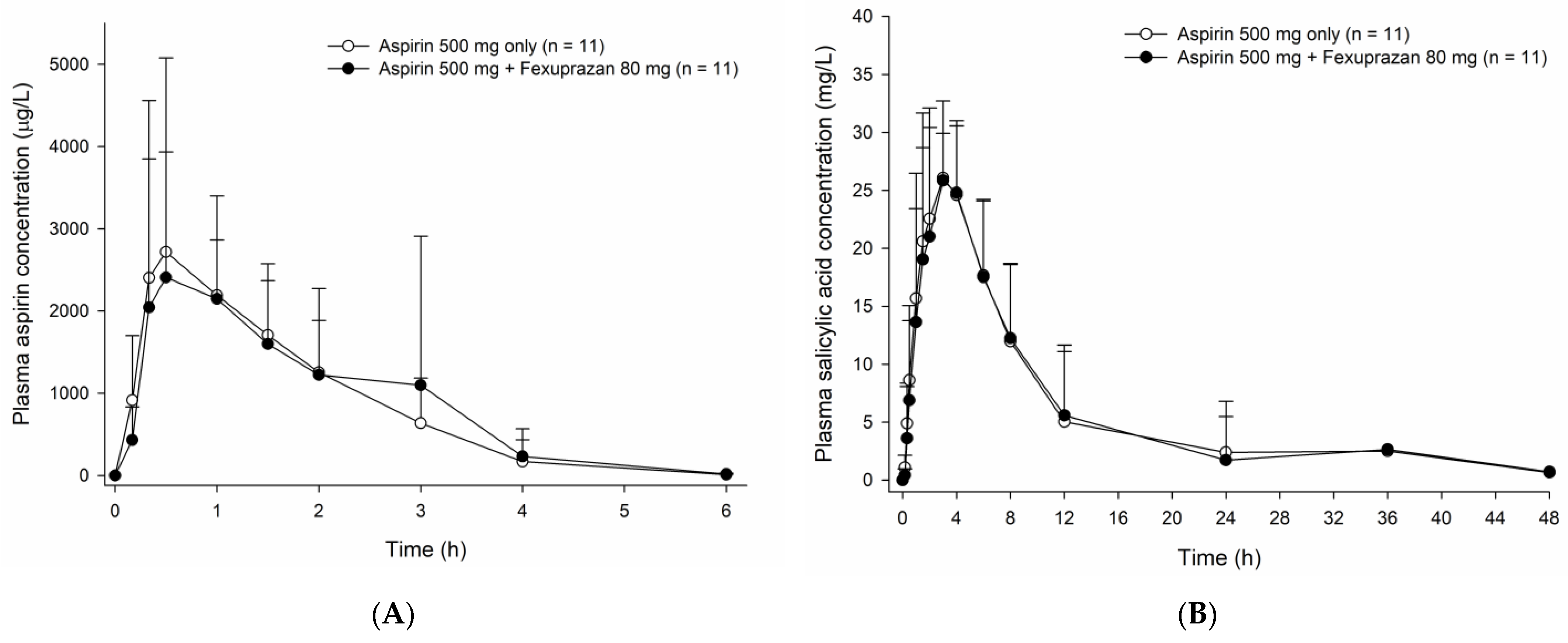
3.3. Effect of Fexuprazan Coadministration on the Pharmacokinetics of Aspirin
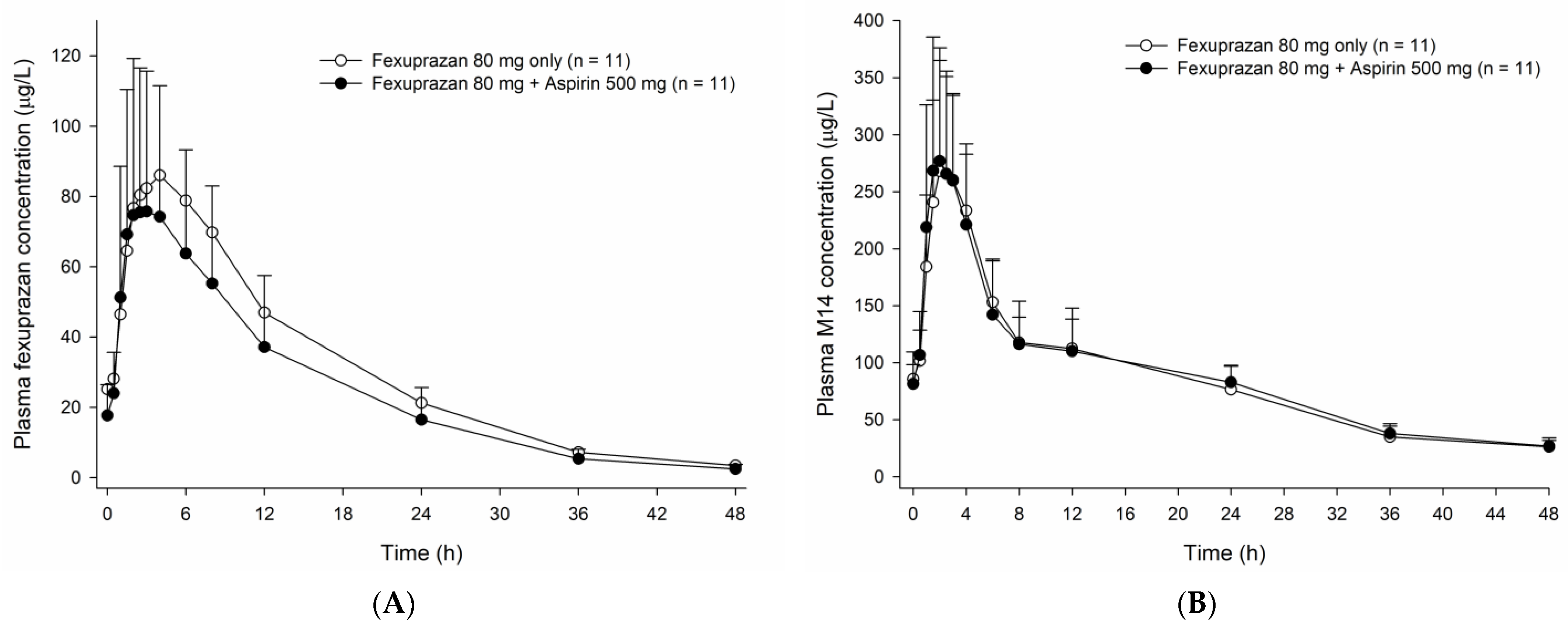
3.4. Effect of Aspirin on the Pharmacokinetics of Fexuprazan
3.5. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tran, H.; Anand, S.S. Oral antiplatelet therapy in cerebrovascular disease, coronary artery disease, and peripheral arterial disease. Jama 2004, 292, 1867–1874. [Google Scholar] [CrossRef] [PubMed]
- Collaboration, A.T. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002, 324, 71–86. [Google Scholar] [CrossRef]
- Soodi, D.; VanWormer, J.J.; Rezkalla, S.H. Aspirin in Primary Prevention of Cardiovascular Events. Clin. Med. Res. 2020, 18, 89–94. [Google Scholar] [CrossRef]
- Serrano, P.; Lanas, A.; Arroyo, M.T.; Ferreira, I.J. Risk of upper gastrointestinal bleeding in patients taking low-dose aspirin for the prevention of cardiovascular diseases. Aliment. Pharmacol. Ther. 2002, 16, 1945–1953. [Google Scholar] [CrossRef] [PubMed]
- Lanas, A.; Ferrández, A. Treatment and prevention of aspirin-induced gastroduodenal ulcers and gastrointestinal bleeding. Expert. Opin. Drug. Saf. 2002, 1, 245–252. [Google Scholar] [CrossRef] [PubMed]
- McCarberg, B.H.; Cryer, B. Evolving therapeutic strategies to improve nonsteroidal anti-inflammatory drug safety. Am. J. Ther. 2015, 22, e167–e178. [Google Scholar] [CrossRef]
- Hsiao, F.Y.; Tsai, Y.W.; Huang, W.F.; Wen, Y.W.; Chen, P.F.; Chang, P.Y.; Kuo, K.N. A comparison of aspirin and clopidogrel with or without proton pump inhibitors for the secondary prevention of cardiovascular events in patients at high risk for gastrointestinal bleeding. Clin. Ther. 2009, 31, 2038–2047. [Google Scholar] [CrossRef] [PubMed]
- Scheiman, J.M.; Herlitz, J.; Veldhuyzen van Zanten, S.J.; Lanas, A.; Agewall, S.; Nauclér, E.C.; Svedberg, L.E.; Nagy, P. Esomeprazole for prevention and resolution of upper gastrointestinal symptoms in patients treated with low-dose acetylsalicylic acid for cardiovascular protection: The OBERON trial. J. Cardiovasc. Pharmacol. 2013, 61, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Niazi, M.; Andersson, T.; Nauclér, E.; Sundin, M.; Naesdal, J. Evaluation of the pharmacokinetic interaction between esomeprazole (40 mg) and acetylsalicylic acid (325 mg) in healthy volunteers. Int. J. Clin. Pharmacol. Ther. 2009, 47, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Andersson, T.; Morrison, D.; Nagy, P.; Pisupati, J.; Schettler, J.; Warner, T.D. Evaluation of the pharmacodynamics of acetylsalicylic acid 81 mg with or without esomeprazole 20 mg in healthy volunteers. Am. J. Cardiovasc. Drugs 2012, 12, 217–224. [Google Scholar] [CrossRef]
- Adamopoulos, A.B.; Sakizlis, G.N.; Nasothimiou, E.G.; Anastasopoulou, I.; Anastasakou, E.; Kotsi, P.; Karafoulidou, A.; Stergiou, G.S. Do proton pump inhibitors attenuate the effect of aspirin on platelet aggregation? A randomized crossover study. J. Cardiovasc. Pharmacol. 2009, 54, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ren, X.; Fang, Z. Systematic Review and Meta-analysis: The Effects of Prophylactic Proton Pump Inhibitor Treatment in Patients With Coronary Heart Disease Receiving Dual Antiplatelet Therapy. J. Cardiovasc. Pharmacol. 2021, 77, 835–861. [Google Scholar] [CrossRef] [PubMed]
- Sunwoo, J.; Oh, J.; Moon, S.J.; Ji, S.C.; Lee, S.H.; Yu, K.S.; Kim, H.S.; Lee, A.; Jang, I.J. Safety, tolerability, pharmacodynamics and pharmacokinetics of DWP14012, a novel potassium-competitive acid blocker, in healthy male subjects. Aliment. Pharmacol. Ther. 2018, 48, 206–218. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.S.; Kim, M.S.; Lee, N.; Lee, A.; Chae, Y.J.; Chung, S.J.; Lee, K.R. Development of Physiologically Based Pharmacokinetic Model for Orally Administered Fexuprazan in Humans. Pharmaceutics 2021, 13, 813. [Google Scholar] [CrossRef] [PubMed]
- Gurbel, P.A.; Bliden, K.P.; DiChiara, J.; Newcomer, J.; Weng, W.; Neerchal, N.K.; Gesheff, T.; Chaganti, S.K.; Etherington, A.; Tantry, U.S. Evaluation of dose-related effects of aspirin on platelet function: Results from the Aspirin-Induced Platelet Effect (ASPECT) study. Circulation 2007, 115, 3156–3164. [Google Scholar] [CrossRef]
- Sakurai, Y.; Shiino, M.; Horii, S.; Okamoto, H.; Nakamura, K.; Nishimura, A.; Sakata, Y. Pharmacokinetic Drug-Drug Interactions Between Vonoprazan and Low-Dose Aspirin or Nonsteroidal Anti-inflammatory Drugs: A Phase 2, Open-Label, Study in Healthy Japanese Men. Clin. Drug. Investig. 2017, 37, 39–49. [Google Scholar] [CrossRef]
- Renda, G.; Zurro, M.; Malatesta, G.; Ruggieri, B.; De Caterina, R. Inconsistency of different methods for assessing ex vivo platelet function: Relevance for the detection of aspirin resistance. Haematologica 2010, 95, 2095–2101. [Google Scholar] [CrossRef]
- Li, J.P.; Guo, J.M.; Shang, E.X.; Zhu, Z.H.; Liu, Y.; Zhao, B.C.; Zhao, J.; Tang, Z.S.; Duan, J.A. Quantitative determination of five metabolites of aspirin by UHPLC-MS/MS coupled with enzymatic reaction and its application to evaluate the effects of aspirin dosage on the metabolic profile. J. Pharm. Biomed. Anal. 2017, 138, 109–117. [Google Scholar] [CrossRef]
- Rocca, B.; Petrucci, G. Variability in the responsiveness to low-dose aspirin: Pharmacological and disease-related mechanisms. Thrombosis 2012, 2012, 376721. [Google Scholar] [CrossRef]
- Hawkey, C.J. Review article: Aspirin and gastrointestinal bleeding. Aliment. Pharmacol. Ther. 1994, 8, 141–146. [Google Scholar] [CrossRef]
- Guidance for Industry: Clinical Drug Interaction Studies—Cytochrome P450 Enzyme- and Transporter—Mediated Drug Interactions. 2020. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-drug-interaction-studies-cytochrome-p450-enzyme-and-transporter-mediated-drug-interactions (accessed on 1 October 2022).
- Benedek, I.H.; Joshi, A.S.; Pieniaszek, H.J.; King, S.Y.; Kornhauser, D.M. Variability in the pharmacokinetics and pharmacodynamics of low dose aspirin in healthy male volunteers. J. Clin. Pharmacol. 1995, 35, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Schrör, K.; Huber, K.; Hohlfeld, T. Functional testing methods for the antiplatelet effects of aspirin. Biomark. Med. 2011, 5, 31–42. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Aspirin 500 mg + Fexuprazan 80 mg (N = 11) | Aspirin 500 mg Only (N = 11) | Geometric Mean Ratio a (90% Confidence Interval) |
|---|---|---|---|
| Tmax (h) | 1.0 [0.3–3.0] | 0.5 [0.3–1.5] | NA |
| AUClast (h·μg/L) | 5033.04 ± 979.17 | 4965.96 ± 1244.60 | 1.0679 (0.9963–1.1448) |
| AUCinf (h·μg/L) | 5049.74 ± 978.89 | 4981.70 ± 1248.07 | 1.0678 (0.9953–1.1457) |
| Cmax (μg/L) | 4094.55 ± 2179.78 | 3056.36 ± 1132.98 | 1.2618 (0.9511–1.6738) |
| t1/2 (h) | 0.41 ± 0.05 | 0.41 ± 0.04 | NA |
| Parameters | Fexuprazan 80 mg + Aspirin 500 mg (N = 11) | Fexuprazan 80 mg Only (N = 11) | Geometric Mean Ratio a (90% Confidence Interval) |
|---|---|---|---|
| Tmax,ss (h) | 3.0 [1.5–6.0] | 4.0 [2.0–6.0] | NA |
| AUCτ,ss (h·μg/L) | 983.32 ± 507.09 | 1190.82 ± 511.52 | 0.7980 (0.7504–0.8486) |
| Cmax,ss (μg/L) | 85.19 ± 42.44 | 91.30 ± 37.18 | 0.8931 (0.8155–0.9780) |
| t1/2,ss (h) | 9.03 ± 1.18 | 9.06 ± 1.03 | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, J.; Yang, E.; Jang, I.-J.; Lee, H.; Yoo, H.; Chung, J.-Y.; Lee, S.; Oh, J. Pharmacodynamic and Pharmacokinetic Drug Interactions between Fexuprazan, a Novel Potassium-Competitive Inhibitor, and Aspirin, in Healthy Subjects. Pharmaceutics 2023, 15, 549. https://doi.org/10.3390/pharmaceutics15020549
Oh J, Yang E, Jang I-J, Lee H, Yoo H, Chung J-Y, Lee S, Oh J. Pharmacodynamic and Pharmacokinetic Drug Interactions between Fexuprazan, a Novel Potassium-Competitive Inhibitor, and Aspirin, in Healthy Subjects. Pharmaceutics. 2023; 15(2):549. https://doi.org/10.3390/pharmaceutics15020549
Chicago/Turabian StyleOh, JungJin, Eunsol Yang, In-Jin Jang, Hyejung Lee, Hokyun Yoo, Jae-Yong Chung, SeungHwan Lee, and Jaeseong Oh. 2023. "Pharmacodynamic and Pharmacokinetic Drug Interactions between Fexuprazan, a Novel Potassium-Competitive Inhibitor, and Aspirin, in Healthy Subjects" Pharmaceutics 15, no. 2: 549. https://doi.org/10.3390/pharmaceutics15020549