
Correlation between Antimicrobial Resistance and the Hospital-Wide Diverse Use of Broad-Spectrum Antibiotics by the Antimicrobial Stewardship Program in Japan
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. AS Programs
2.2. Monitoring of Antibiotic Use
2.3. Monitoring of Antibiotic-Resistant Gram-Negative Rods
2.4. Statistical Analysis
3. Results
3.1. Intervention/Supervision of AS Programs
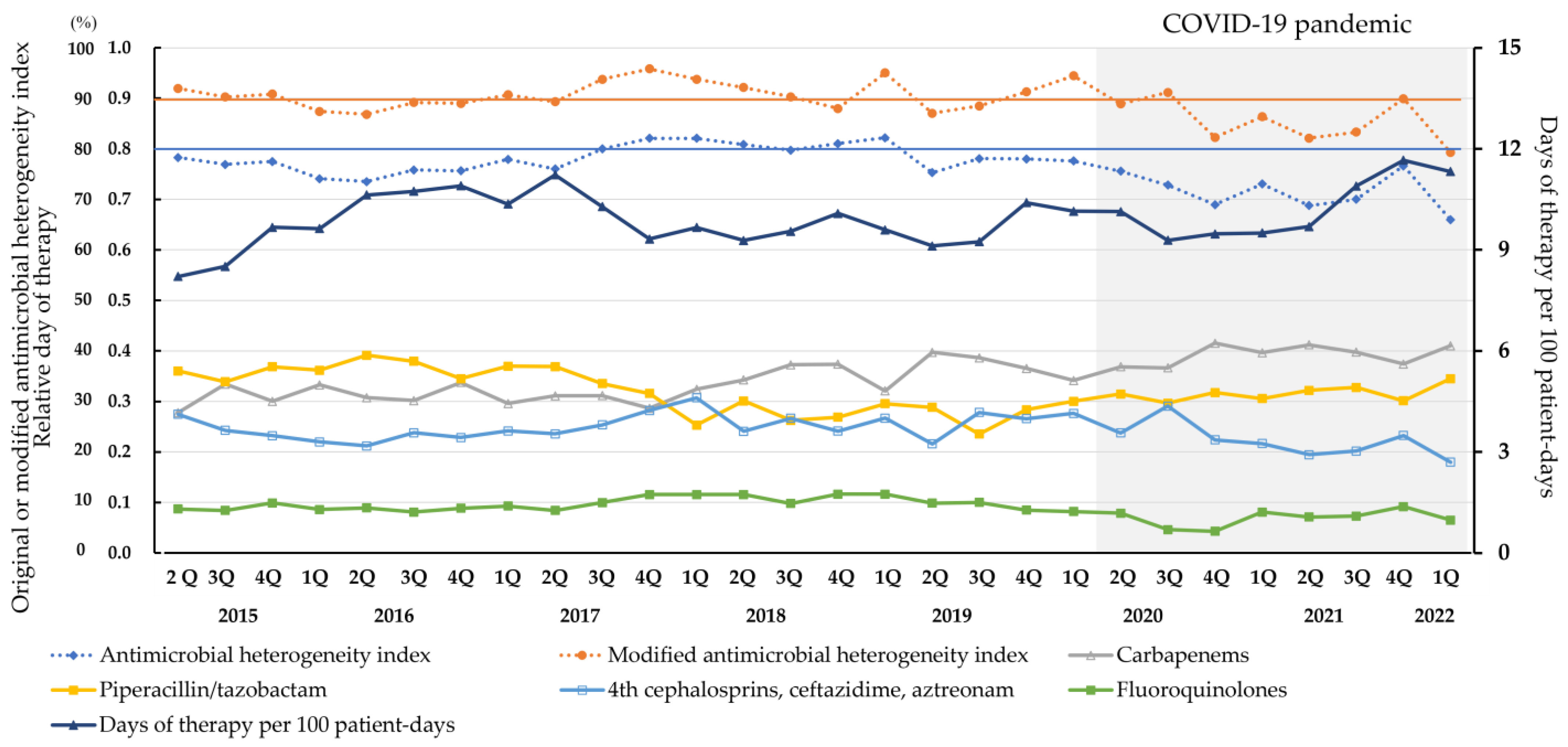
3.2. Antibiotic Use during the AS Programs
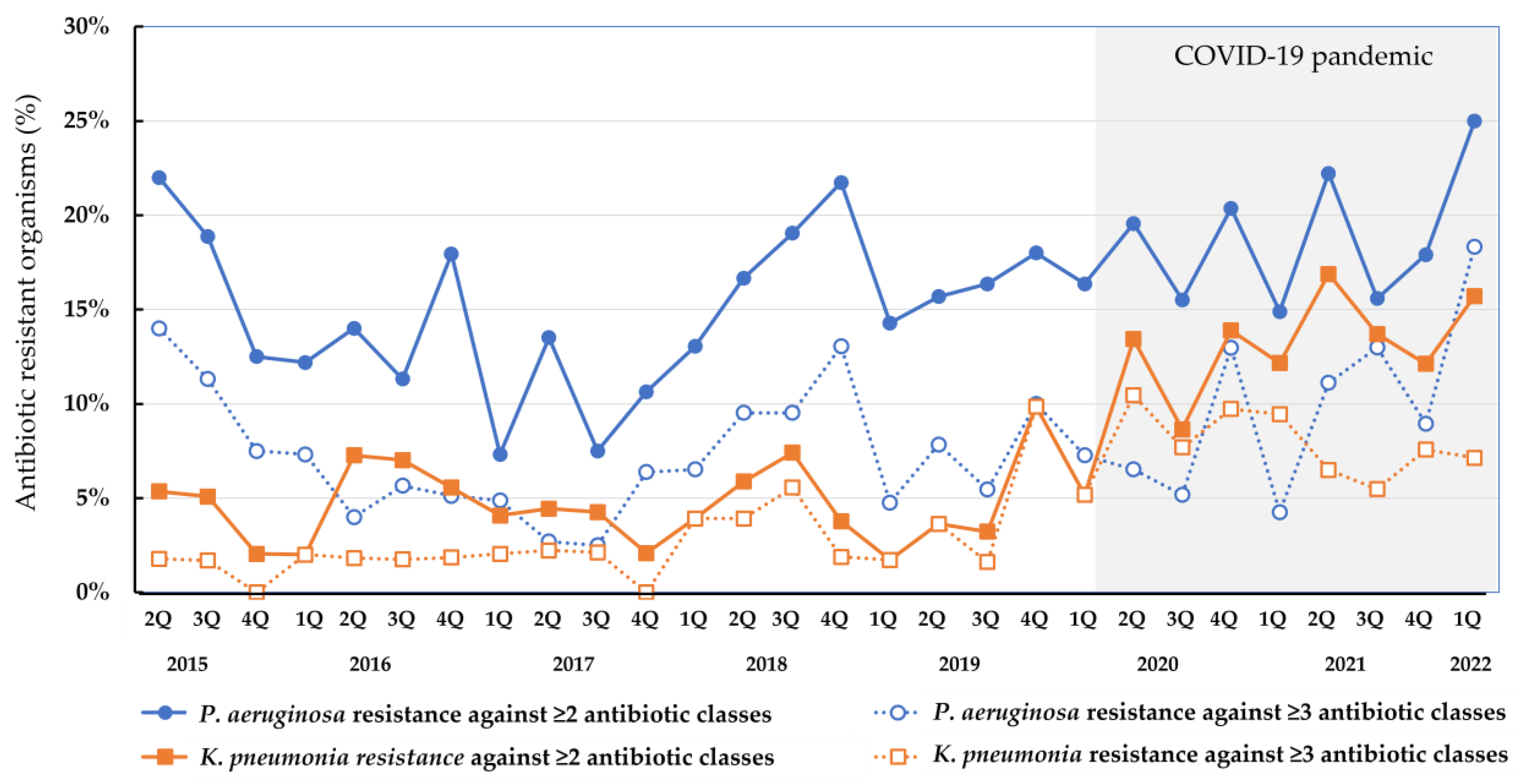
3.3. Isolation of Antibiotic-Resistant Gram-Negative Rods
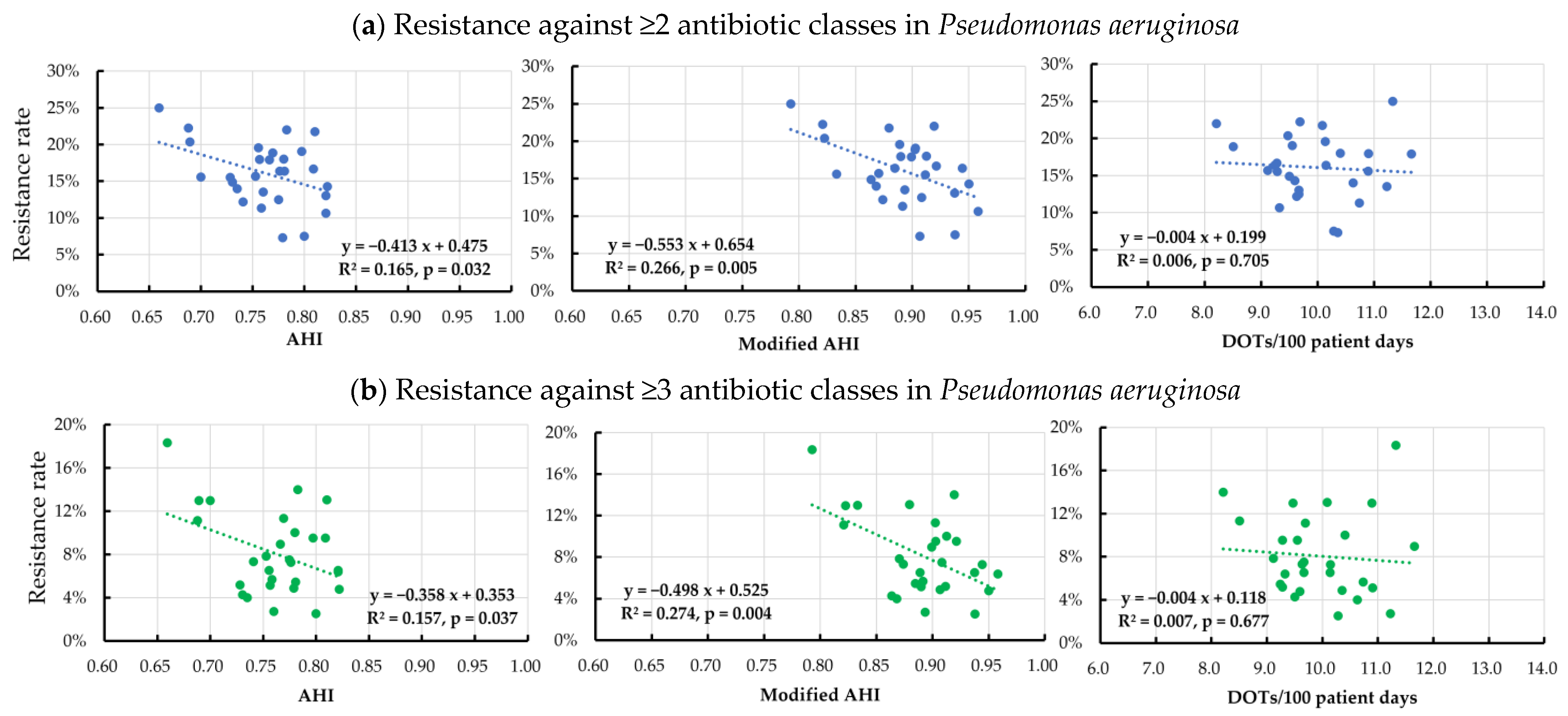
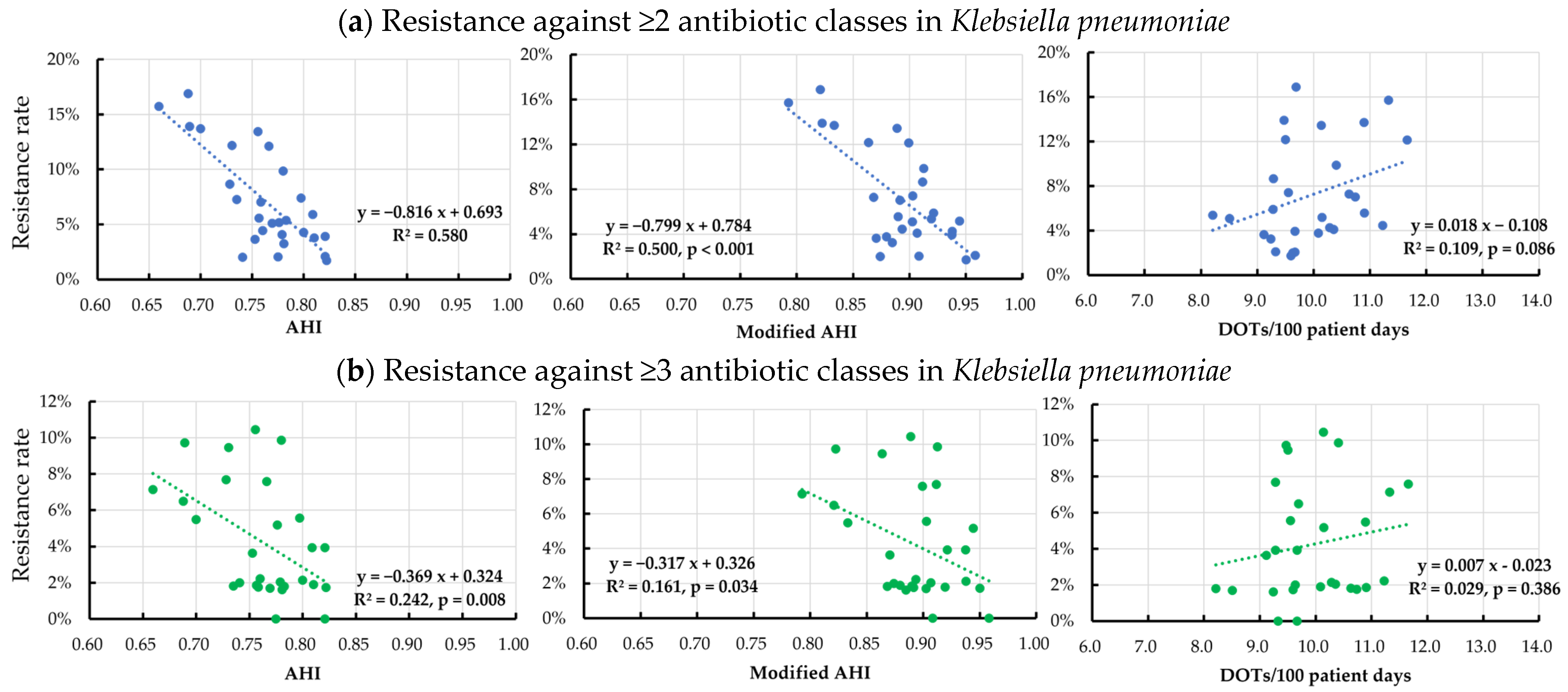
3.4. Correlation between the Isolation Rate of Antibiotic Resistant Organisms and Antibiotic Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cosgrove, S.E. The relationship between antimicrobial resistance and patient outcomes: Mortality, length of hospital stay, and health care costs. Clin. Infect. Dis. 2006, 42, S82–S89. [Google Scholar] [CrossRef]
- De Kraker, M.E.A.; Wolkewitz, M.; Davey, P.G.; Koller, W.; Berger, J.; Nagler, J.; Icket, C.; Kalenic, S.; Horvatic, J.; Seifert, H.; et al. Burden of antimicrobial resistance in European hospitals: Excess mortality and length of hospital stay associated with bloodstream infections due to Escherichia coli resistant to third-generation cephalosporins. J. Antimicrob. Chemother. 2011, 66, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- WHO Guidelines Approved by the Guidelines Review Committee. Guidelines for the Prevention and Control of Carbapenem-Resistant Enterobacteriaceae, Acinetobacter baumannii and Pseudomonas aeruginosa in Health Care Facilities. Available online: https://www.ncbi.nlm.nih.gov/books/NBK493061/ (accessed on 11 January 2023).
- McDanel, J.; Schweizer, M.; Crabb, V.; Nelson, R.; Samore, M.; Khader, K.; Blevins, A.E.; Diekema, D.; Chiang, H.Y.; Nair, R.; et al. Incidence of Extended-Spectrum β-Lactamase (ESBL)-Producing Escherichia coli and Klebsiella Infections in the United States: A Systematic Literature Review. Infect. Control Hosp. Epidemiol. 2017, 38, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Raman, G.; Avendano, E.E.; Chan, J.; Merchant, S.; Puzniak, L. Risk factors for hospitalized patients with resistant or multidrug-resistant Pseudomonas aeruginosa infections: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2018, 7, 79. [Google Scholar] [CrossRef]
- Wang, H.; Wang, H.; Yu, X.; Zhou, H.; Li, B.; Chen, G.; Ye, Z.; Wang, Y.; Cui, X.; Zheng, Y.; et al. Impact of antimicrobial stewardship managed by clinical pharmacists on antibiotic use and drug resistance in a Chinese hospital, 2010–2016: A retrospective observational study. BMJ Open 2019, 9, e026072. [Google Scholar] [CrossRef] [PubMed]
- Razzaque, M.S. Implementation of antimicrobial stewardship to reduce antimicrobial drug resistance. Expert Rev. Anti-Infect. Ther. 2021, 19, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhou, M.; Liu, F. Effect of antibiotic stewardship programs on reduction of antimicrobial resistance in China. Am. J. Infect. Control 2020, 48, 233–234. [Google Scholar] [CrossRef]
- Schuts, E.C.; Hulscher, M.E.J.L.; Mouton, J.W.; Verduin, C.M.; Stuart, J.W.T.C.; Overdiek, H.W.P.M.; van der Linden, P.D.; Natsch, S.; Hertogh, C.M.P.M.; Wolfs, T.F.W.; et al. Current evidence on hospital antimicrobial stewardship objectives: A systematic review and meta-analysis. Lancet Infect. Dis. 2016, 16, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Plüss-Suard, C.; Pannatier, A.; Kronenberg, A.; Mühlemann, K.; Zanetti, G. Impact of antibiotic use on carbapenem resistance in Pseudomonas aeruginosa: Is there a role for antibiotic diversity? Antimicrob. Agents Chemother. 2013, 57, 1709–1713. [Google Scholar] [CrossRef] [Green Version]
- Bennett, K.M.; Scarborough, J.E.; Sharpe, M.; Dodds-Ashley, E.; Kaye, K.S.; Hayward, T.Z.; Vaslef, S.N. Implementation of antibiotic rotation protocol improves antibiotic susceptibility profile in a surgical intensive care unit. J. Trauma 2007, 63, 307–311. [Google Scholar] [CrossRef]
- Brown, E.M.; Nathwani, D. Antibiotic cycling or rotation: A systematic review of the evidence of efficacy. J. Antimicrob. Chemother. 2005, 55, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Sandiumenge, A.; Lisboa, T.; Gomez, F.; Hernandez, P.; Canadell, L.; Rello, J. Effect of antibiotic diversity on ventilator-associated pneumoniae caused by ESKAPE Organisms. Chest 2011, 140, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Goel, N.; Wattal, C.; Oberoi, J.K.; Raveendran, R.; Datta, S.; Prasad, K.J. Trend analysis of antimicrobial consumption and development of resistance in non-fermenters in a tertiary care hospital in Delhi, India. J. Antimicrob. Chemother. 2011, 66, 1625–1630. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, P.R.; Chen, W.H.; Luh, K.T. Relationships between antimicrobial use and antimicrobial resistance in Gram-negative bacteria causing nosocomial infections from 1991–2003 at a university hospital in Taiwan. Int. J. Antimicrob. Agents 2005, 26, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Bal, A.M.; Kumar, A.; Gould, I.M. Antibiotic heterogeneity: From concept to practice. Ann. N. Y. Acad. Sci. 2010, 1213, 81–91. [Google Scholar] [CrossRef]
- Chong, Y.; Shimoda, S.; Yakushiji, H.; Ito, Y.; Miyamoto, T.; Kamimura, T.; Shimono, N.; Akashi, K. Antibiotic rotation for febrile neutropenic patients with hematological malignancies: Clinical significance of antibiotic heterogeneity. PLoS ONE 2013, 8, e54190. [Google Scholar] [CrossRef]
- Gandra, S.; Trett, A.; Klein, E.Y.; Laxminarayan, R. Is antimicrobial resistance a bigger problem in tertiary care hospitals than in small community hospitals in the United States? Clin. Infect. Dis. 2017, 65, 860–863. [Google Scholar] [CrossRef]
- Van Santen, K.L.; Edwards, J.R.; Webb, A.K.; Pollack, L.A.; O’Leary, E.; Neuhauser, M.M.; Srinivasan, A.; Pollock, D.A. The standardized antimicrobial administration ratio: A new metric for measuring and comparing antibiotic use. Clin. Infect. Dis. 2018, 67, 179–185. [Google Scholar] [CrossRef]
- Van Duijn, P.J.; Bonten, M.J. Antibiotic rotation strategies to reduce antimicrobial resistance in Gram-negative bacteria in European intensive care units: Study protocol for a cluster-randomized crossover controlled trial. Trials 2014, 15, 277. [Google Scholar] [CrossRef] [Green Version]
- Beardmore, R.E.; Peña-Miller, R.; Gori, F.; Iredell, J. Antibiotic cycling and antibiotic mixing: Which one best mitigates antibiotic resistance? Mol. Biol. Evol. 2017, 34, 802–817. [Google Scholar] [CrossRef] [PubMed]
- Jayashree, M.; Singhi, S.; Ray, P.; Gautam, V.; Ratol, S.; Bharti, S. Longitudinal comparative trial of antibiotic cycling and mixing on emergence of gram negative bacterial resistance in a pediatric medical intensive care unit. J. Crit. Care 2020, 56, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Van Duijn, P.J.; Verbrugghe, W.; Jorens, P.G.; Spöhr, F.; Schedler, D.; Deja, M.; Rothbart, A.; Annane, D.; Lawrence, C.; Nguyen Van, J.C.; et al. The effects of antibiotic cycling and mixing on antibiotic resistance in intensive care units: A cluster-randomised crossover trial. Lancet Infect. Dis. 2018, 18, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Takesue, Y.; Nakajima, K.; Ichiki, K.; Ishihara, M.; Wada, Y.; Takahashi, Y.; Tsuchida, T.; Ikeuchi, H. Impact of a hospital-wide programme of heterogeneous antibiotic use on the development of antibiotic-resistant Gram-negative bacteria. J. Hosp. Infect. 2010, 75, 28–32. [Google Scholar] [CrossRef]
- Yoon, Y.K.; Kwon, K.T.; Jeong, S.J.; Moon, C.; Kim, B.; Kiem, S.; Kim, H.-s.; Heo, E.; Kim, S.-W. Guidelines on Implementing Antimicrobial Stewardship Programs in Korea. Infect. Chemother. 2021, 53, 617–659. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, E.N.; Edwards, J.R.; Srinivasan, A.; Neuhauser, M.M.; Webb, A.K.; Soe, M.M.; Hicks, L.A.; Wise, W.; Wu, H.; Pollock, D.A. National Healthcare Safety Network Standardized Antimicrobial Administration Ratios (SAARs): A progress report and risk modeling update using 2017 data. Clin. Infect. Dis. 2020, 71, e702–e709. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. A Guide the SAAR. Available online: https://www.cdc.gov/nhsn/pdfs/ps-analysis-resources/aur/au-saar-guide-508.pdf (accessed on 10 October 2022).
- Clinical and Laboratory Standards Institute. M100: Performance Standards for Antimicrobial Susceptibility Testing, 30th ed.; Clinical and Laboratory Standards Institute: Berwin, PA, USA, 2020. [Google Scholar]
- Sasaki, T.; Hirai, I.; Niki, M.; Nakamura, T.; Komalamisra, C.; Maipanich, W.; Kusolsuk, T.; Sa-Nguankiat, S.; Pubampen, S.; Yamamoto, Y. High prevalence of CTX-M beta-lactamase-producing Enterobacteriaceae in stool specimens obtained from healthy individuals in Thailand. J. Antimicrob. Chemother. 2010, 65, 666–668. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. M100: Performance Standards for Antimicrobial Susceptibility Testing, 28th ed.; Clinical and Laboratory Standards Institute: Berwin, PA, USA, 2018; Available online: https://file.qums.ac.ir/repository/mmrc/CLSI-2018-M100-S28.pdf (accessed on 24 November 2022).
- Arakawa, Y.; Shibata, N.; Shibayama, K.; Kurokawa, H.; Yagi, T.; Fujiwara, H.; Goto, M. Convenient test for screening metallo-beta-lactamase-producing gram-negative bacteria by using thiol compounds. J. Clin. Microbiol. 2000, 38, 40–43. [Google Scholar] [CrossRef]
- Veličković-Radovanović, R.; Stefanović, N.; Damnjanović, I.; Kocić, B.; Mladenović-Antić, S.; Dinić, M.; Petrović, J.; Mitić, R.; Catić-Đorđević, A. Antibiotic utility and susceptibility changes of multidrug-resistant Escherichia coli and Klebsiella spp: 5-year experience in a tertiary healthcare centre. Eur. J. Hosp. Pharm. 2022, 29, 84–89. [Google Scholar] [CrossRef]
- Troughton, J.A.; Millar, G.; Smyth, E.T.M.; Doherty, L.; McMullan, R. Ciprofloxacin use and susceptibility of Gram-negative organisms to quinolone and non-quinolone antibiotics. J. Antimicrob. Chemother. 2011, 66, 2152–2158. [Google Scholar] [CrossRef]
- Ortiz-Brizuela, E.; Caro-Vega, Y.; Bobadilla-Del-Valle, M.; Leal-Vega, F.; Criollo-Mora, E.; López Luis, B.A.; Esteban-Kenel, V.; Torres-Veintimilla, E.; Galindo-Fraga, A.; Olivas-Martínez, A.; et al. The influence of hospital antimicrobial use on carbapenem-non-susceptible Enterobacterales incidence rates according to their mechanism of resistance: A time-series analysis. J. Hosp. Infect. 2020, 105, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Sandiumenge, A.; Diaz, E.; Rodriguez, A.; Vidaur, L.; Canadell, L.; Olona, M.; Rue, M.; Rello, J. Impact of diversity of antibiotic use on the development of antimicrobial resistance. J. Antimicrob. Chemother. 2006, 57, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Dijkshoorn, L.; Nemec, A.; Seifert, H. An increasing threat in hospitals: Multidrug-resistant Acinetobacter baumannii. Nat. Rev. Microbiol. 2007, 5, 939–951. [Google Scholar] [CrossRef] [PubMed]
- Tseng, S.H.; Lee, C.M.; Lin, T.Y.; Chang, S.C.; Chuang, Y.C.; Yen, M.Y.; Hwang, K.P.; Leu, H.S.; Yen, C.C.; Chang, F.Y. Combating antimicrobial resistance: Antimicrobial stewardship program in Taiwan. J. Microbiol. Immunol. Infect. 2012, 45, 79–89. [Google Scholar] [CrossRef]
- Toombs-Ruane, L.J.; Benschop, J.; Burgess, S.; Priest, P.; Murdoch, D.R.; French, N.P. Multidrug resistant Enterobacteriaceae in New Zealand: A current perspective. N. Z. Vet. J. 2017, 65, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Akeda, Y. Current Situation of carbapenem-resistant Enterobacteriaceae and Acinetobacter in Japan and Southeast Asia. Microbiol. Immunol. 2021, 65, 229–237. [Google Scholar] [CrossRef]
- Yanagihara, K.; Matsumoto, T.; Tokimatsu, I.; Tsukada, H.; Fujikura, Y.; Miki, M.; Morinaga, Y.; Sato, J.; Wakamura, T.; Kiyota, H.; et al. Nationwide surveillance of bacterial respiratory pathogens conducted by the Surveillance Committee of Japanese Society of Chemotherapy, the Japanese Association for Infectious Diseases, and the Japanese Society for Clinical Microbiology in 2016: General view of the pathogens’ antibacterial susceptibility. J. Infect. Chemother. 2020, 26, 873–881. [Google Scholar] [CrossRef]
- Takesue, Y.; Kusachi, S.; Mikamo, H.; Sato, J.; Watanabe, A.; Kiyota, H.; Iwata, S.; Kaku, M.; Hanaki, H.; Sumiyama, Y.; et al. Antimicrobial susceptibility of common pathogens isolated from postoperative intra-abdominal infections in Japan. J. Infect. Chemother. 2018, 24, 330–340. [Google Scholar] [CrossRef]
- Pierce, J.; Stevens, M.P. COVID-19 and antimicrobial stewardship: Lessons learned, best practices, and future implications. Int. J. Infect. Dis. 2021, 113, 103–108. [Google Scholar] [CrossRef]
- Rawson, T.M.; Ming, D.; Ahmad, R.; Moore, L.S.P.; Holmes, A.H. Antimicrobial use, drug-resistant infections and COVID-19. Nat. Rev. Microbiol. 2020, 18, 409–410. [Google Scholar] [CrossRef]
- Lai, C.C.; Chen, S.Y.; Ko, W.C.; Hsueh, P.R. Increased antimicrobial resistance during the COVID-19 pandemic. Int. J. Antimicrob. Agents 2021, 57, 106324. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Castro-Sanchez, E.; Charani, E.; Davies, F.; Satta, G.; Ellington, M.J.; Holmes, A.H. COVID-19 and the potential long-term impact on antimicrobial resistance. J. Antimicrob. Chemother. 2020, 75, 1681–1684. [Google Scholar] [CrossRef] [PubMed]
- Fattouh, R.; Tijet, N.; McGeer, A.; Poutanen, S.M.; Melano, R.G.; Patel, S.N. What is the appropriate meropenem MIC for screening of carbapenemase-producing Enterobacteriaceae in low-prevalence settings? Antimicrob. Agents Chemother. 2015, 60, 1556–1559. [Google Scholar] [CrossRef] [PubMed]
- Yonekawa, S.; Mizuno, T.; Nakano, R.; Nakano, A.; Suzuki, Y.; Asada, T.; Ishii, A.; Kakuta, N.; Tsubaki, K.; Mizuno, S.; et al. Molecular and epidemiological characteristics of carbapenemase-producing Klebsiella pneumoniae clinical isolates in Japan. mSphere 2020, 5, e00490-20. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reasons for the Initial Intervention/Supervision | 2015 April–2016 March | 2016 April–2017 March | 2017 April–2018 March | 2018 April–2019 March | 2019 April–2020 March | 2020 April–2021 March | 2021 April–2022 March | Total |
|---|---|---|---|---|---|---|---|---|
| Infectious disease consultation service | 684 (69.2%) | 657 (65.0%) | 613 (54.9%) | 602 (51.7%) | 659 (56.2%) | 552 (48.6%) | 668 (54.6%) | 4435 (56.9%) |
| Suggestion of antimicrobial selection and dosing for patients admitted to the intensive care unit | 152 (15.4%) | 158 (15.9%) | 179 (16.0%) | 164 (14.1%) | 165 (14.1%) | 172 (15.2%) | 166 (13.6%) | 1156 (14.8%) |
| Isolation of organisms from the aseptic specimen | 92 (9.3%) | 97 (9.8%) | 97 (8.7%) | 94 (8.1%) | 95 (8.1%) | 143 (12.6%) | 135 (11.0%) | 753 (9.7%) |
| Isolation of antimicrobial-resistant organisms | 9 (0.9%) | 18 (1.9%) | 31 (2.8%) | 51 (4.4%) | 51 (4.4%) | 52 (4.6%) | 51 (4.2%) | 263 (3.4%) |
| Diagnosis of Clostridioides difficile infection | 42 (4.2%) | 31 (3.1%) | 37 (3.3%) | 33 (2.8%) | 34 (2.9%) | 47 (4.1%) | 30 (2.5%) | 254 (3.3%) |
| Prescription for carbapenems or piperacillin/tazobactam * | – | – | 87 (7.8%) | 144 (12.4%) | 92 (7.8%) | 121 (10.7%) | 104 (8.5%) | 548 (7.0%) |
| Prolonged use of designated antimicrobial agents | 10 (1.0%) | 35 (3.6%) | 73 (6.5%) | 76 (6.5%) | 76 (6.5%) | 48 (4.2%) | 69 (5.6%) | 387 (5.0%) |
| Total | 989 | 996 | 1117 | 1164 | 1172 | 1135 | 1223 | 7796 |
| Organisms | No. of Strains | No. of Resistant Organisms (Rate) | Extended-Spectrum β-Lactamase-producing Organisms | Carbapenemase-Producing Organisms | |
|---|---|---|---|---|---|
| ≥2 Classes | ≥3 Classes | ||||
| Glucose non-fermenting Gram-negative rod | 1713 | 248 (14.5%) | 123 (7.2%) | – | 8 (0.5%) |
| Pseudomonas aeruginosa | 1392 | 228 (16.4%) | 117 (8.4%) | – | 8 (0.6%) |
| Acinetobacter baumannii | 321 | 20 (6.2%) | 6 (1.9%) | – | 0 (0.0%) |
| Enterobacteriaceae sp. | 7838 | 1102 (14.1%) | 297 (3.8%) | 897 (11.4%) | 23 (0.3%) |
| Escherichia coli | 2863 | 765 (26.7%) | 190 (6.6%) | 702 (24.3%) | 3 (0.1%) |
| Klebsiella pneumoniae | 1685 | 131 (7.8%) | 79 (4.7%) | 155 (8.8%) | 7 (0.4%) |
| Klebsiella oxytoca | 670 | 26 (3.9%) | 7 (1.0%) | 11 (1.5%) | 0 (0.0%) |
| Klebsiella aerogenes | 339 | 16 (4.7%) | 5 (1.5%) | 2 (0.6%) | 0 (0.0%) |
| Enterobacter cloacae | 960 | 123 (12.8%) | 10 (1.0%) | 9 (0.8%) | 9 (0.9%) |
| Other Enterobacteriaceae sp. | 1321 | 41 (3.1%) | 6 (0.5%) | 18 (1.2%) | 4 (0.3%) |
| Serratia marcescens | 382 | 4 (1.0%) | 1 (0.3%) | 0 (0.0%) | 0 (0.0%) |
| Citrobacter freundii | 300 | 12 (4.0%) | 4 (1.3%) | 6 (1.7%) | 3 (1.0%) |
| Proteus mirabilis | 204 | 14 (6.9%) | 0 (0.0%) | 12 (5.1%) | 0 (0.0%) |
| Proteus vulgaris | 140 | 4 (2.9%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Morganella morganii | 295 | 7 (2.4%) | 1 (0.3%) | 0 (0.0%) | 1 (0.3%) |
| Resistant Organisms | Antimicrobial Heterogeneity Index | Modified Antimicrobial Heterogeneity Index | Days of Therapy per 100 Patient Days | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gradient | R2 | p-Value | 95% CI | Gradient | R2 | p Value | 95% CI | Gradient | R2 | p-Value | 95% CI | |
| Pseudomonas aeruginosa | ||||||||||||
| ≥ 2 class | −0.413 | 0.165 | 0.032 | −0.676 to −0.039 | −0.553 | 0.266 | 0.005 | −0.746 to −0.177 | −0.004 | 0.006 | 0.705 | −0.436 to 0.307 |
| ≥ 3 class | −0.358 | 0.157 | 0.037 | −0.670 to −0.027 | −0.498 | 0.274 | 0.004 | −0.750 to −0.186 | −0.004 | 0.007 | 0.677 | −0.442 to 0.300 |
| Acinetobacter baumannii | ||||||||||||
| ≥ 2 class | −0.077 | 0.002 | 0.810 | −0.413 to 0.331 | −0.097 | 0.003 | 0.774 | −0.421 to 0.323 | 0.020 | 0.061 | 0.204 | −0.139 to 0.568 |
| ≥ 3 class | 0.024 | 0.001 | 0.899 | −0.351 to 0.395 | 0.044 | 0.002 | 0.824 | −0.335 to 0.410 | 0.007 | 0.022 | 0.447 | −0.236 to 0.495 |
| Escherichia coli | ||||||||||||
| ≥ 2 class | −0.079 | 0.006 | 0.697 | −0.438 to −0.305 | −0.199 | 0.034 | 0.350 | −0.521 to 0.204 | −0.009 | 0.032 | 0.363 | −0.517 to 0.208 |
| ≥ 3 class | 0.153 | 0.055 | 0.231 | −0.152 to 0.558 | 0.087 | 0.016 | 0.521 | −0.259 to 0.477 | −0.005 | 0.024 | 0.432 | −0.499 to 0.232 |
| Klebsiella pneumoniae | ||||||||||||
| ≥ 2 class | −0.816 | 0.580 | <0.001 | −0.894 to −0.576 | −0.799 | 0.500 | <0.001 | −0.855 to−0.454 | 0.018 | 0.109 | 0.086 | −0.048 to 0.626 |
| ≥ 3 class | −0.369 | 0.242 | 0.008 | −0.765 to −0.219 | −0.317 | 0.161 | 0.034 | −0.673 to−0.033 | 0.007 | 0.029 | 0.386 | −0.217 to 0.511 |
| Enterobacter cloacae | ||||||||||||
| ≥ 2 class | −0.338 | 0.047 | 0.268 | −0.546 to 0.170 | −0.188 | 0.013 | 0.562 | −0.468 to 0.270 | −0.014 | 0.032 | 0.364 | −0.517 to 0.209 |
| ≥ 3 class | −0.084 | 0.038 | 0.320 | −0.530 to 0.192 | −0.087 | 0.037 | 0.330 | −0.527 to 0.196 | −0.002 | 0.007 | 0.676 | −0.442 to 0.300 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ueda, T.; Takesue, Y.; Nakajima, K.; Ichiki, K.; Ishikawa, K.; Yamada, K.; Tsuchida, T.; Otani, N.; Takahashi, Y.; Ishihara, M.; et al. Correlation between Antimicrobial Resistance and the Hospital-Wide Diverse Use of Broad-Spectrum Antibiotics by the Antimicrobial Stewardship Program in Japan. Pharmaceutics 2023, 15, 518. https://doi.org/10.3390/pharmaceutics15020518
Ueda T, Takesue Y, Nakajima K, Ichiki K, Ishikawa K, Yamada K, Tsuchida T, Otani N, Takahashi Y, Ishihara M, et al. Correlation between Antimicrobial Resistance and the Hospital-Wide Diverse Use of Broad-Spectrum Antibiotics by the Antimicrobial Stewardship Program in Japan. Pharmaceutics. 2023; 15(2):518. https://doi.org/10.3390/pharmaceutics15020518
Chicago/Turabian StyleUeda, Takashi, Yoshio Takesue, Kazuhiko Nakajima, Kaoru Ichiki, Kaori Ishikawa, Kumiko Yamada, Toshie Tsuchida, Naruhito Otani, Yoshiko Takahashi, Mika Ishihara, and et al. 2023. "Correlation between Antimicrobial Resistance and the Hospital-Wide Diverse Use of Broad-Spectrum Antibiotics by the Antimicrobial Stewardship Program in Japan" Pharmaceutics 15, no. 2: 518. https://doi.org/10.3390/pharmaceutics15020518