
Sonoporation of the Round Window Membrane on a Sheep Model: A Safety Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Animals and Housing
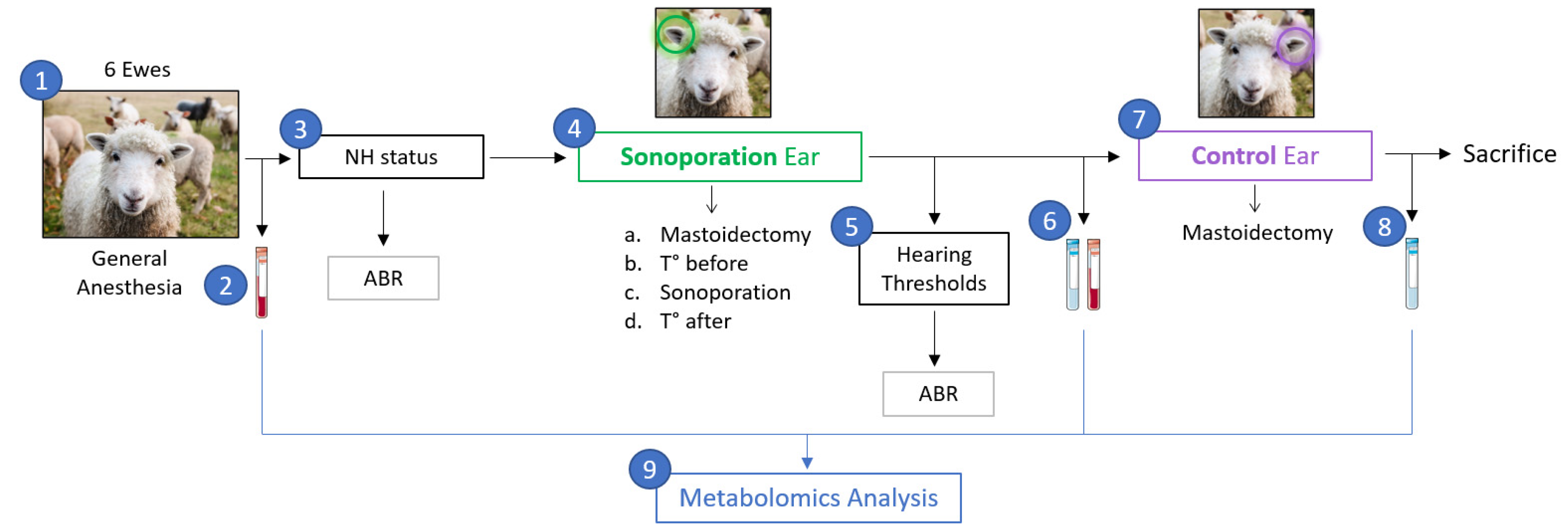
2.2. Sonoporation Protocol
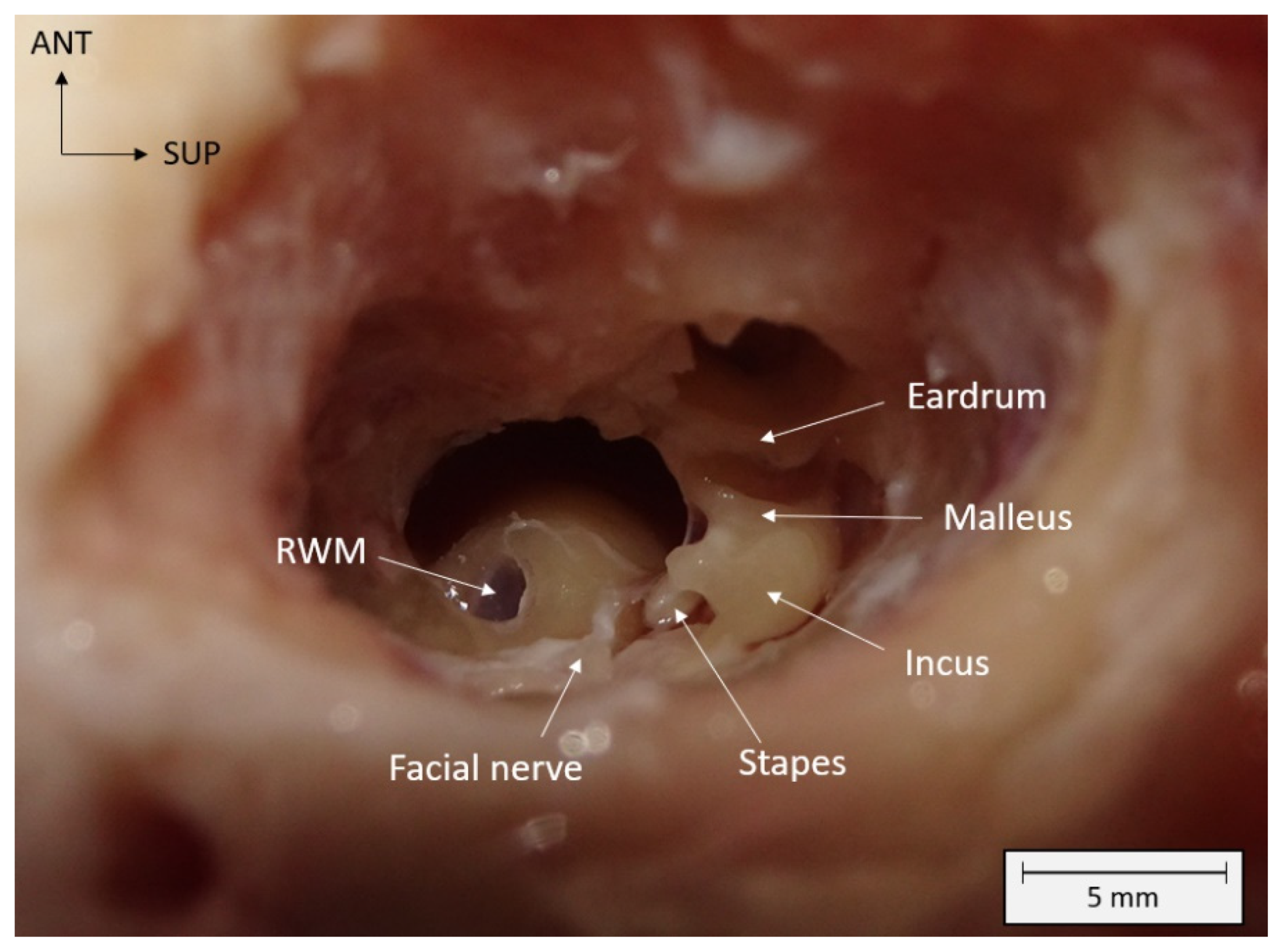
2.2.1. Surgery
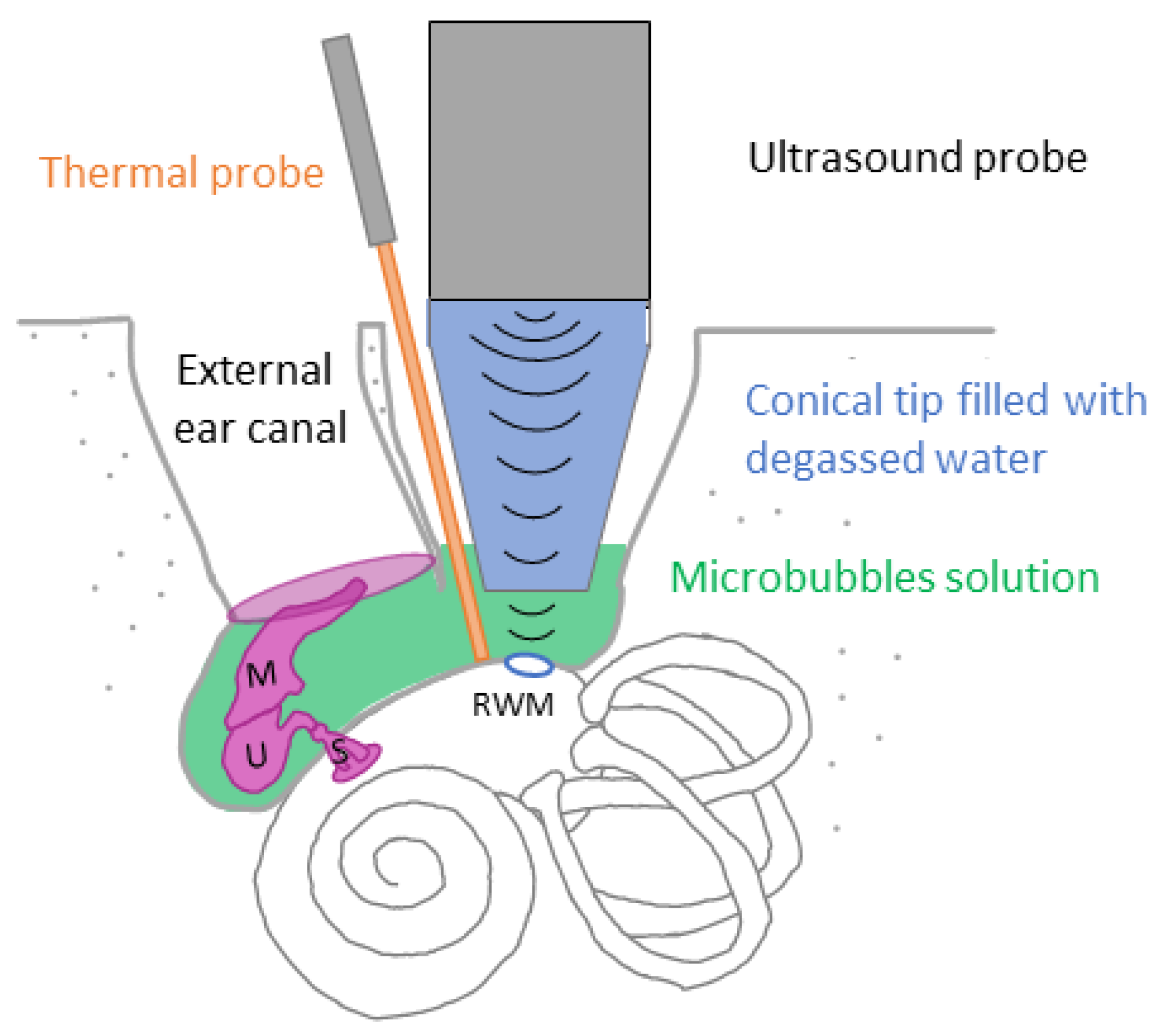
2.2.2. Ultrasound Treatment
2.3. Assessment of Auditory Function
2.4. Temperature Measurement
2.5. Metabolomic Analysis
2.5.1. Sample Collection
2.5.2. Sample Analysis
2.6. Statistical Analysis
2.6.1. Statistical Analysis of Auditory Function
2.6.2. Statistical Analysis of Temperature Measurements
2.6.3. Statistical Analysis of Metabolomics Samples
3. Results
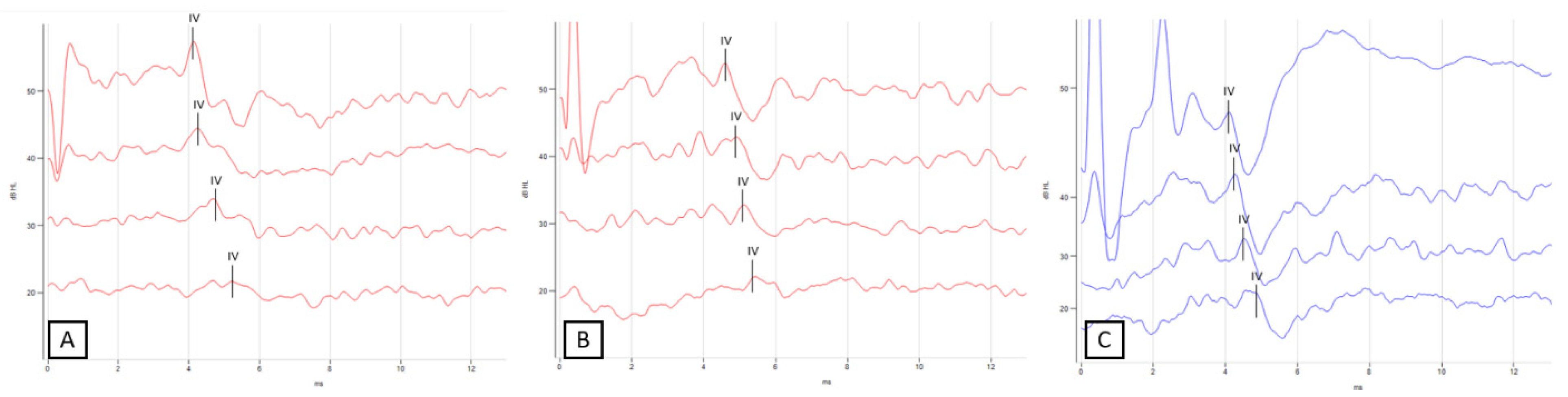
3.1. Evaluation of Auditory Thresholds
3.2. Temperature Measures
3.3. Metabolomics Analysis of Perilymph
3.3.1. Perilymph Composition
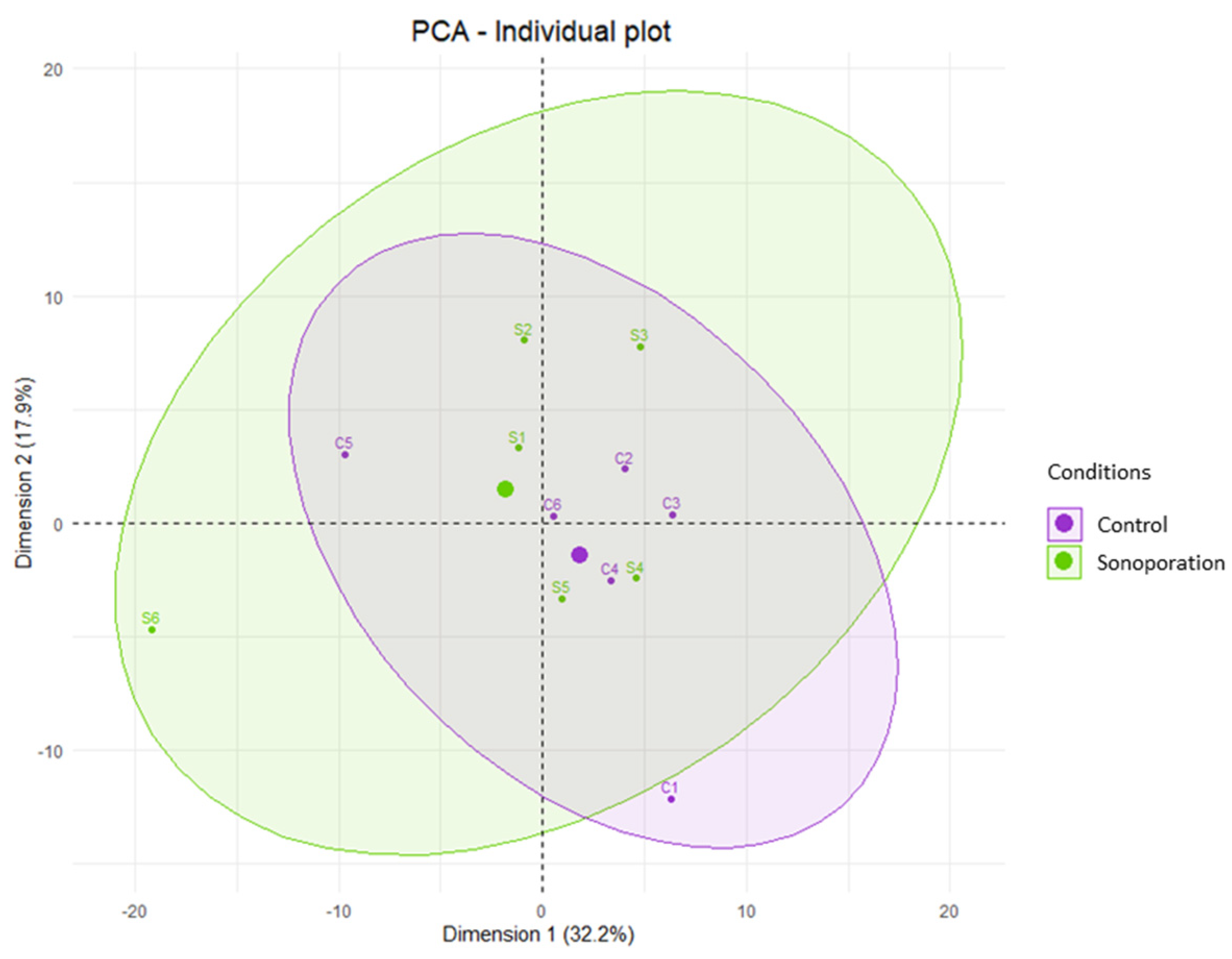
3.3.2. Perilymph Comparison by Multivariate Analysis
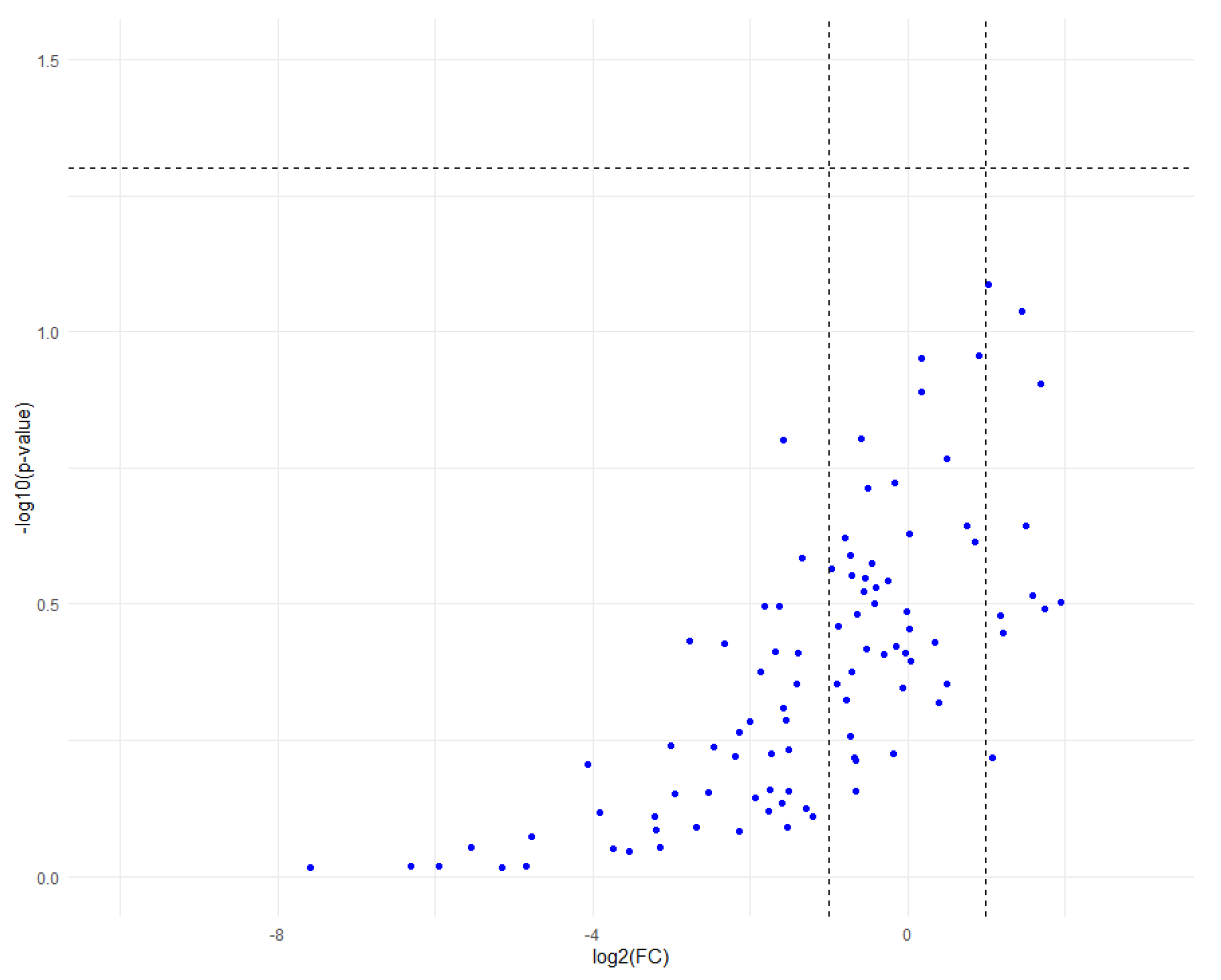
3.3.3. Perilymph Comparison by Univariate Analysis
3.4. Metabolomics Analysis of Plasma
3.4.1. Plasma Composition
3.4.2. Plasma Comparison before and after Sonoporation by Multivariate Analysis
3.4.3. Plasma Comparison by Univariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathers, C.D.; Stein, C.; Ma Fat, D.; Rao, C.; Inoue, M.; Tomijima, N.; Bernard, C.; Lopez, A.D.; Murray, C.J.L. Global Burden of Disease 2000: Version 2 Methods and Results; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Kanzaki, S.; Shibata, S.; Nakamura, M.; Ozaki, M.; Okano, H.; Ogawa, K. Comparison of inner ear drug availability of combined treatment with systemic or local drug injections alone. Neurosci. Res. 2020, 155, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Wu, H.; Zhang, P.; Hou, D.M.; Chen, J.; Zhang, S.G. The pharmacokinetic profiles of dexamethasone and methylprednisolone concentration in perilymph and plasma following systemic and local administration. Acta Otolaryngol. 2008, 128, 496–504. [Google Scholar] [CrossRef]
- Li, Y.; Kanzaki, S.; Shibata, S.; Nakamura, M.; Ozaki, M.; Okano, H.; Ogawa, K. Comparison of Drug Availability in the Inner Ear After Oral, Transtympanic, and Combined Administration. Front. Neurol. 2021, 12, 641593. [Google Scholar] [CrossRef] [PubMed]
- King, E.B.; Salt, A.N.; Eastwood, H.T.; O’Leary, S.J. Direct entry of gadolinium into the vestibule following intratympanic applications in Guinea pigs and the influence of cochlear implantation. J. Assoc. Res. Otolaryngol. 2011, 12, 741–751. [Google Scholar] [CrossRef] [Green Version]
- Salt, A.N.; King, E.B.; Hartsock, J.J.; Gill, R.M.; O’Leary, S.J. Marker entry into vestibular perilymph via the stapes following applications to the round window niche of guinea pigs. Hear. Res. 2012, 283, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Lange, G. Gentamicin and other ototoxic antibiotics for the transtympanic treatment of Menière’s disease. Arch. Otorhinolaryngol. 1989, 246, 269–270. [Google Scholar] [CrossRef]
- Patel, M.; Agarwal, K.; Arshad, Q.; Hariri, M.; Rea, P.; Seemungal, B.M.; Golding, J.F.; Harcourt, J.P.; Bronstein, A.M. Intratympanic methylprednisolone versus gentamicin in patients with unilateral Ménière;s disease: A randomised, double-blind, comparative effectiveness trial. Lancet 2016, 388, 2753–2762. [Google Scholar] [CrossRef] [Green Version]
- Ahmadzai, N.; Cheng, W.; Kilty, S.; Esmaeilisaraji, L.; Wolfe, D.; Bonaparte, J.; Schramm, D.; Fitzpatrick, E.; Lin, V.; Skidmore, B.; et al. Pharmacologic and surgical therapies for patients with Meniere’s disease: A systematic review and network meta-analysis. PLoS ONE 2020, 15, e0237523. [Google Scholar] [CrossRef]
- Lim, H.J.; Kim, Y.T.; Choi, S.J.; Lee, J.B.; Park, H.Y.; Park, K.; Choung, Y.H. Efficacy of 3 different steroid treatments for sudden sensorineural hearing loss: A prospective, randomized trial. Otolaryngol. Head Neck Surg. 2013, 148, 121–127. [Google Scholar] [CrossRef]
- Ahmadzai, N.; Kilty, S.; Cheng, W.; Esmaeilisaraji, L.; Wolfe, D.; Bonaparte, J.P.; Schramm, D.; Fitzpatrick, E.; Lin, V.; Skidmore, B.; et al. A systematic review and network meta-analysis of existing pharmacologic therapies in patients with idiopathic sudden sensorineural hearing loss. PLoS ONE 2019, 14, e0221713. [Google Scholar] [CrossRef] [PubMed]
- Parnes, L.S.; Sun, A.H.; Freeman, D.J. Corticosteroid pharmacokinetics in the inner ear fluids: An animal study followed by clinical application. Laryngoscope 1999, 109 Pt 2, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, H.; Choo, D.; Rosenberg, S.I.; Kuhn, J.; Seidman, M.; Stein, I. Intratympanic steroid treatment of inner ear disease and tinnitus (preliminary report). Ear. Nose Throat J. 1996, 75, 468–488. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Wang, S.; Shu, Y.; Zhang, H. Nanoparticle-based inner ear delivery systems for the treatment of hearing loss. Smart Mater. Med. 2021, 2, 350–353. [Google Scholar] [CrossRef]
- Wise, A.K.; Tan, J.; Wang, Y.; Caruso, F.; Shepherd, R.K. Improved Auditory Nerve Survival with Nanoengineered Supraparticles for Neurotrophin Delivery into the Deafened Cochlea. PLoS ONE 2016, 11, e0164867. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.; Wang, Y.; Yip, X.; Glynn, F.; Shepherd, R.K.; Caruso, F. Nanoporous peptide particles for encapsulating and releasing neurotrophic factors in an animal model of neurodegeneration. Adv. Mater. 2012, 24, 3362–3366. [Google Scholar] [CrossRef] [Green Version]
- Jaudoin, C.; Carré, F.; Gehrke, M.; Sogaldi, A.; Steinmetz, V.; Hue, N.; Cailleau, C.; Tourrel, G.; Nguyen, Y.; Ferrary, E.; et al. Transtympanic injection of a liposomal gel loaded with N-acetyl-L-cysteine: A relevant strategy to prevent damage induced by cochlear implantation in guinea pigs? Int. J. Pharm. 2021, 604, 120757. [Google Scholar] [CrossRef]
- Warnecke, A.; Prenzler, N.; Harre, J.; Köhl, U.; Gärtner, L.; Lenarz, T.; Laner-Plamberger, S.; Wietzorrek, G.; Staecker, H.; Lassacher, T.; et al. First-in-human intracochlear application of human stromal cell-derived extracellular vesicles. J. Extracell. Vesicles 2021, 10, e12094. [Google Scholar] [CrossRef]
- Dinh, C.; Hoang, K.; Haake, S.; Chen, S.; Angeli, S.; Nong, E.; Eshraghi, A.A.; Balkany, T.J.; Van De Water, T.R. Biopolymer-released dexamethasone prevents tumor necrosis factor alpha-induced loss of auditory hair cells in vitro: Implications toward the development of a drug-eluting cochlear implant electrode array. Otol. Neurotol. 2008, 29, 1012–1019. [Google Scholar] [CrossRef]
- Paasche, G.; Bögel, L.; Leinung, M.; Lenarz, T.; Stöver, T. Substance distribution in a cochlea model using different pump rates for cochlear implant drug delivery electrode prototypes. Hear. Res. 2006, 212, 74–82. [Google Scholar] [CrossRef]
- Scheper, V.; Hessler, R.; Hütten, M.; Wilk, M.; Jolly, C.; Lenarz, T.; Paasche, G. Local inner ear application of dexamethasone in cochlear implant models is safe for auditory neurons and increases the neuroprotective effect of chronic electrical stimulation. PLoS ONE 2017, 12, e0183820. [Google Scholar] [CrossRef] [Green Version]
- Hakuba, N.; Watabe, K.; Hyodo, J.; Ohashi, T.; Eto, Y.; Taniguchi, M.; Yang, L.; Tanaka, J.; Hata, R.; Gyo, K. Adenovirus-mediated overexpression of a gene prevents hearing loss and progressive inner hair cell loss after transient cochlear ischemia in gerbils. Gene Ther. 2003, 10, 426–433. [Google Scholar] [CrossRef]
- Escoffre, J.M.; Bouakaz, A. Minireview: Biophysical Mechanisms of Cell Membrane Sonopermeabilization. Knowns and Unknowns. Langmuir 2019, 35, 10151–10165. [Google Scholar] [CrossRef]
- Presset, A.; Bonneau, C.; Kazuyoshi, S.; Nadal-Desbarats, L.; Mitsuyoshi, T.; Bouakaz, A.; Kudo, N.; Escoffre, J.M.; Sasaki, N. Endothelial Cells, First Target of Drug Delivery Using Microbubble-Assisted Ultrasound. Ultrasound Med. Biol. 2020, 46, 1565–1583. [Google Scholar] [CrossRef]
- Shih, C.P.; Chen, H.C.; Chen, H.K.; Chiang, M.C.; Sytwu, H.K.; Lin, Y.C.; Li, S.L.; Shih, Y.F.; Liao, A.H.; Wang, C.H. Ultrasound-aided microbubbles facilitate the delivery of drugs to the inner ear via the round window membrane. J. Control. Release 2013, 167, 167–174. [Google Scholar] [CrossRef]
- Liao, A.H.; Hsieh, Y.L.; Ho, H.C.; Chen, H.K.; Lin, Y.C.; Shih, C.P.; Chen, H.C.; Kuo, C.Y.; Lu, Y.J.; Wang, C.H. Effects of microbubble size on ultrasound-mediated gene transfection in auditory cells. Biomed. Res. Int. 2014, 2014, 840852. [Google Scholar] [CrossRef] [Green Version]
- Shih, C.P.; Chen, H.C.; Lin, Y.C.; Chen, H.K.; Wang, H.; Kuo, C.Y.; Lin, Y.Y.; Wang, C.H. Middle-ear dexamethasone delivery via ultrasound microbubbles attenuates noise-induced hearing loss. Laryngoscope 2019, 129, 1907–1914. [Google Scholar] [CrossRef]
- Liao, A.H.; Wang, C.H.; Weng, P.Y.; Lin, Y.C.; Wang, H.; Chen, H.K.; Liu, H.L.; Chuang, H.C.; Shih, C.P. Ultrasound-induced microbubble cavitation via a transcanal or transcranial approach facilitates inner ear drug delivery. JCI Insight 2020, 5, e132880. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.C.; Chen, H.C.; Chen, H.K.; Lin, Y.Y.; Kuo, C.Y.; Wang, H.; Hung, C.L.; Shih, C.P.; Wang, C.H. Ultrastructural Changes Associated with the Enhanced Permeability of the Round Window Membrane Mediated by Ultrasound Microbubbles. Front. Pharmacol. 2020, 10, 1580. [Google Scholar] [CrossRef]
- Liao, A.H.; Shih, C.P.; Li, M.W.; Lin, Y.C.; Chuang, H.C.; Wang, C.H. Development of thermosensitive poloxamer 407-based microbubble gel with ultrasound mediation for inner ear drug delivery. Drug Deliv. 2021, 28, 1256–1271. [Google Scholar] [CrossRef]
- Lin, Y.C.; Lin, Y.Y.; Chen, H.C.; Kuo, C.Y.; Liao, A.H.; Chou, Y.L.; Hung, C.L.; Shih, C.P.; Wang, C.H. Ultrasound Microbubbles Enhance the Efficacy of Insulin-Like Growth Factor-1 Therapy for the Treatment of Noise-Induced Hearing Loss. Molecules 2021, 26, 3626. [Google Scholar] [CrossRef] [PubMed]
- Ter Haar, G. Ultrasonic imaging: Safety considerations. Interface Focus 2011, 1, 686–697. [Google Scholar] [CrossRef]
- Nordang, L.; Linder, B.; Anniko, M. Morphologic changes in round window membrane after topical hydrocortisone and dexamethasone treatment. Otol. Neurotol. 2003, 24, 339–343. [Google Scholar] [CrossRef]
- Schachern, P.A.; Paparella, M.M.; Duvall, A.J., 3rd; Choo, Y.B. The human round window membrane. An electron microscopic study. Arch. Otolaryngol. 1984, 110, 15–21. [Google Scholar] [CrossRef]
- Trinh, T.T.; Cohen, C.; Boullaud, L.; Cottier, J.P.; Bakhos, D. Sheep as a large animal model for cochlear implantation. Braz. J. Otorhinolaryngol. 2023, 88, 24–32. [Google Scholar] [CrossRef]
- Seibel, V.A.; Lavinsky, L.; Irion, K. CT-Scan sheep and human inner ear morphometric comparison. Braz. J. Otorhinolaryngol. 2006, 72, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Seibel, V.A.; Lavinsky, L.; De Oliveira, J.A. Morphometric study of the external and middle ear anatomy in sheep: A possible model for ear experiments. Clin. Anat. 2006, 19, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Péus, D.; Dobrev, I.; Pfiffner, F.; Sim, J.H. Comparison of sheep and human middle-ear ossicles: Anatomy and inertial properties. J. Comp. Physiol. A Neuroethol. Sens. Neural Behav. Physiol. 2020, 206, 683–700. [Google Scholar] [CrossRef]
- Soares, H.B.; Lavinsky, L. Histology of sheep temporal bone. Braz. J. Otorhinolaryngol. 2011, 77, 285–292. [Google Scholar] [CrossRef] [Green Version]
- Han, S.; Suzuki-Kerr, H.; Suwantika, M.; Telang, R.S.; Gerneke, D.A.; Anekal, P.V.; Bird, P.; Vlajkovic, S.M.; Thorne, P.R. Characterization of the Sheep Round Window Membrane. J. Assoc. Res. Otolaryngol. 2021, 22, 1–17. [Google Scholar] [CrossRef]
- Hill, M.W.; Heavens, R.P.; Baldwin, B.A. Auditory evoked potentials recorded from conscious sheep. Brain Res. Bull. 1985, 15, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Trinh, T.T.; Blasco, H.; Emond, P.; Andres, C.; Lefevre, A.; Lescanne, E.; Bakhos, D. Relationship between Metabolomics Profile of Perilymph in Cochlear-Implanted Patients and Duration of Hearing Loss. Metabolites 2019, 9, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boullaud, L.; Blasco, H.; Caillaud, E.; Emond, P.; Bakhos, D. Immediate-Early Modifications to the Metabolomic Profile of the Perilymph Following an Acoustic Trauma in a Sheep Model. J. Clin. Med. 2022, 11, 4668. [Google Scholar] [CrossRef] [PubMed]
- Presset, A.; Bodard, S.; Lefèvre, A.; Millet, A.; Oujagir, E.; Dupuy, C.; Iazourène, T.; Bouakaz, A.; Emond, P.; Escoffre, J.M.; et al. First Metabolomic Signature of Blood-Brain Barrier Opening Induced by Microbubble-Assisted Ultrasound. Front. Mol. Neurosci. 2022, 15, 888318. [Google Scholar] [CrossRef]
- Mavel, S.; Lefèvre, A.; Bakhos, D.; Dufour-Rainfray, D.; Blasco, H.; Emond, P. Validation of metabolomics analysis of human perilymph fluid using liquid chromatography-mass spectroscopy. Hear. Res. 2018, 367, 129–136. [Google Scholar] [CrossRef]
- Diémé, B.; Mavel, S.; Blasco, H.; Tripi, G.; Bonnet-Brilhault, F.; Malvy, J.; Bocca, C.; Andres, C.R.; Nadal-Desbarats, L.; Emond, P. Metabolomics Study of Urine in Autism Spectrum Disorders Using a Multiplatform Analytical Methodology. J. Proteome Res. 2015, 4, 5273–5282. [Google Scholar] [CrossRef] [Green Version]
- Bressand, D.; Novell, A.; Girault, A.; Raoul, W.; Fromont-Hankard, G.; Escoffre, J.M.; Lecomte, T.; Bouakaz, A. Enhancing Nab-Paclitaxel Delivery Using Microbubble-Assisted Ultrasound in a Pancreatic Cancer Model. Mol. Pharm. 2019, 16, 3814–3822. [Google Scholar] [CrossRef]
- Escoffre, J.M.; Novell, A.; Piron, J.; Zeghimi, A.; Doinikov, A.; Bouakaz, A. Microbubble attenuation and destruction: Are they involved in sonoporation efficiency? IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2013, 60, 46–52. [Google Scholar] [CrossRef]
- Escoffre, J.M.; Piron, J.; Novell, A.; Bouakaz, A. Doxorubicin delivery into tumor cells with ultrasound and microbubbles. Mol. Pharm. 2011, 8, 799–806. [Google Scholar] [CrossRef]
- Fujita, T.; Yamashita, D.; Irino, Y.; Kitamoto, J.; Fukuda, Y.; Inokuchi, G.; Hasegawa, S.; Otsuki, N.; Yoshida, M.; Nibu, K. Metabolomic profiling in inner ear fluid by gas chromatography/mass spectrometry in guinea pig cochlea. Neurosci. Lett. 2015, 606, 188–193. [Google Scholar] [CrossRef]
- Ji, L.; Lee, H.J.; Wan, G.; Wang, G.P.; Zhang, L.; Sajjakulnukit, P.; Schacht, J.; Lyssiotis, C.A.; Corfas, G. Auditory metabolomics, an approach to identify acute molecular effects of noise trauma. Sci. Rep. 2019, 9, 9273. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Thresholds (dB) | |||
|---|---|---|---|
| Sheep | Before Sonoporation | After Sonoporation | Control |
| #1 | 30 | 30 | 30 |
| #2 | 30 | 30 | 30 |
| #3 | 20 | 30 | 20 |
| #4 | 20 | 20 | 20 |
| #5 | 20 | 20 | 20 |
| #6 | 20 | 20 | 20 |
| Sheep | Measurement | 30 dB | 20 dB |
|---|---|---|---|
| #1 | Before sonoporation | 4.49 | # |
| After sonoporation | 5.22 | # | |
| Control side | 5.24 | # | |
| #2 | Before sonoporation | 4.9 | # |
| After sonoporation | 4.75 | # | |
| Control side | 4.82 | # | |
| #3 | Before sonoporation | 4.74 | 5.10 |
| After sonoporation | 4.75 | # | |
| Control side | 4.61 | 5.10 | |
| #4 | Before sonoporation | 4.36 | 4.59 |
| After sonoporation | 4.35 | 4.85 | |
| Control side | 4.77 | 4.88 | |
| #5 | Before sonoporation | 4.69 | 5.15 |
| After sonoporation | 5.10 | 5.40 | |
| Control side | 4.49 | 4.84 | |
| #6 | Before sonoporation | 4.83 | 5.08 |
| After sonoporation | 4.93 | 5.50 | |
| Control side | 5.03 | 5.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kerneis, S.; Escoffre, J.-M.; Galvin, J.J., III; Bouakaz, A.; Presset, A.; Alix, C.; Oujagir, E.; Lefèvre, A.; Emond, P.; Blasco, H.; et al. Sonoporation of the Round Window Membrane on a Sheep Model: A Safety Study. Pharmaceutics 2023, 15, 442. https://doi.org/10.3390/pharmaceutics15020442
Kerneis S, Escoffre J-M, Galvin JJ III, Bouakaz A, Presset A, Alix C, Oujagir E, Lefèvre A, Emond P, Blasco H, et al. Sonoporation of the Round Window Membrane on a Sheep Model: A Safety Study. Pharmaceutics. 2023; 15(2):442. https://doi.org/10.3390/pharmaceutics15020442
Chicago/Turabian StyleKerneis, Sandrine, Jean-Michel Escoffre, John J. Galvin, III, Ayache Bouakaz, Antoine Presset, Corentin Alix, Edward Oujagir, Antoine Lefèvre, Patrick Emond, Hélène Blasco, and et al. 2023. "Sonoporation of the Round Window Membrane on a Sheep Model: A Safety Study" Pharmaceutics 15, no. 2: 442. https://doi.org/10.3390/pharmaceutics15020442